
Abstract
The NICE Guidelines published in 2015 state that testosterone supplementation can be considered for menopausal women with low sexual desire if hormone replacement therapy alone is not effective. There is however, no detail on what to prescribe, how much to prescribe or whether monitoring is required. At the time of conception of this project, there was no national guideline or official advice from the British Menopause Society. We decided to ask menopause experts from around the UK to see if a consensus could be reached about good prescribing practice. The method and results as discussed below may be helpful in future recommendations and guidance.
Introduction
The NICE Guidelines state that testosterone supplementation can be considered for menopausal women with low sexual desire if hormone replacement therapy (HRT) alone is not effective. 1 The British Menopause Society (BMS) 2020 recommendations advise that this indication could be extended to include menopausal women with low sexual desire and tiredness. 2 However, although testosterone replacement therapy (TRT) is recognised as an appropriate adjunct to menopause care, there is no detail on how to prescribe, appropriate products and their doses or advice on whether monitoring is required stated in the NICE Guidelines. 1 At the time of conception of this project, there was an absence of any national guideline or official advice from the BMS and so it was decided to collate information from menopause experts around the UK to see if a consensus could be reached about good prescribing practice. Half-way through the data collection for this project, the BMS did release some guidance on testosterone prescribing 3 and a Global Consensus Position Statement on the Use of Testosterone Therapy for Women 4 was then published later in the year. However, it is the authors’ opinion that the results of the project demonstrate an interesting insight into prescribing practice of testosterone in the UK and may be helpful in determining future recommendations.
Aim
To collate information on prescribing practice of testosterone from BMS Menopause Specialists.
Methods
The project was registered with the Kings College London Research Ethics Office (Number MRA-18/19-10399). A link to a Google forms® questionnaire was emailed from an administrator of the BMS to the 124 registered BMS menopause specialists in the UK who were registered on the BMS specialist register at that time. As defined by the BMS, these are healthcare professionals who have obtained the Faculty of Sexual & Reproductive Healthcare (FSRH)/BMS advanced certificate in menopause care, or completed the Royal College of Obstetricians & Gynaecologists (RCOG)/BMS advanced training skills module (ATSM) in menopause care (or equivalent, e.g. the menopause and premature ovarian insufficiency module of the subspecialty training programme in reproductive medicine) and who: is a member of the British Menopause Society, attends a national (BMS) or international menopause society (e.g. International Menopause Society, European Menopause and Andropause Society) scientific conference at least once every three years, provides a minimum of 100 menopause-related consultations per year, of which at least 50 are new and is responsible for ensuring that the specialism is documented in their job plan and is discussed and recorded at their annual appraisal in the UK or Ireland. 5
Data collection took place between 8 February 2019 and 8 March 2019. No personal details were obtained during the data collection, so the answers to the questionnaires were anonymous. Some of the questions were multiple choice and some were free text boxes. The data was then collated using an Excel spread sheet and percentages used to analyse the responses.
Testosterone prescribing questionnaire (Research Ethics Number MRA-18/19-10399) (online Appendix 1).
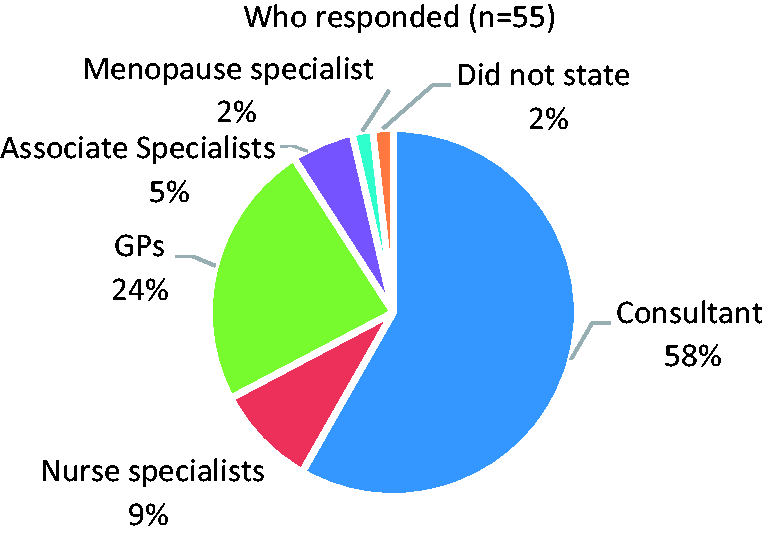
Job titles of survey participants.
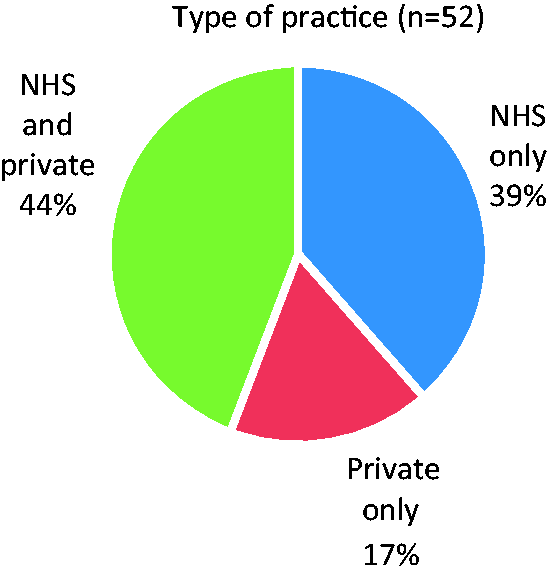
Type of practice that survey participants undertake.
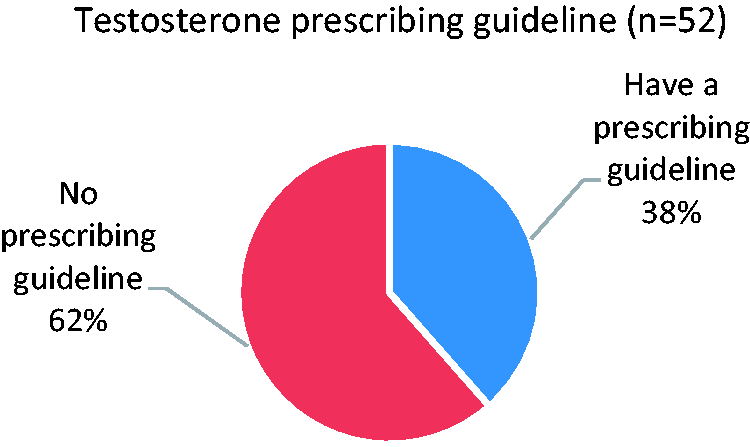
Existence of a departmental testosterone prescribing guideline.
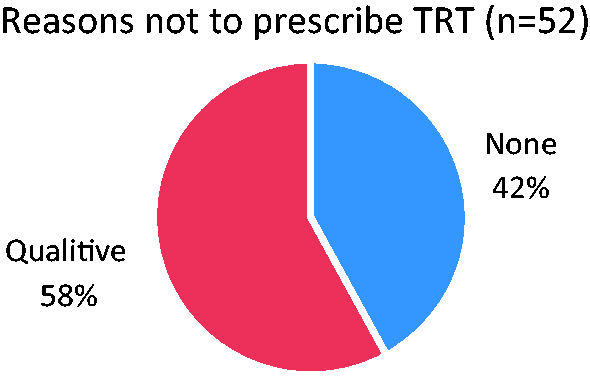
Some participants consider there are reasons when testosterone should not be prescribed.
Reasons listed for situations in which the participants consider testosterone should not be prescribed.

FAI: free androgen index.
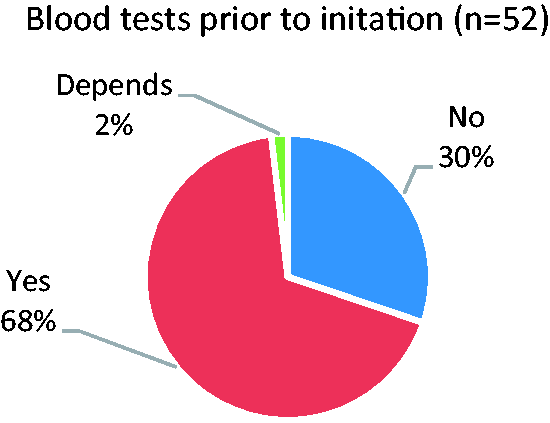
Some participants arrange initial blood tests prior to initiating testosterone.
Different blood tests requested prior to initiation of testosterone.

SHBG: sex hormone-binding globulin; LH: luteinising hormone; FSH: Follicle-stimulating hormone.
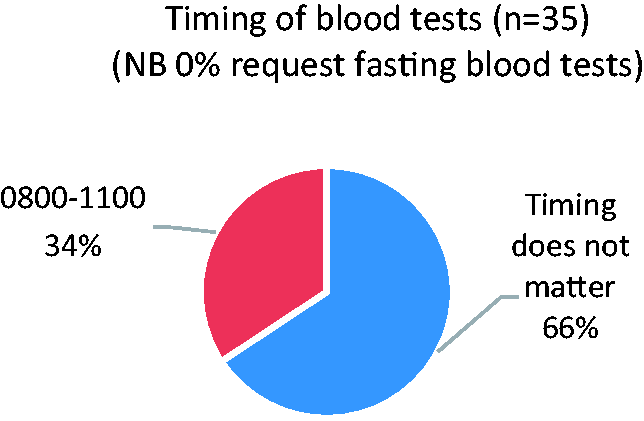
Some participants arrange the initial blood tests at specific times of the day.
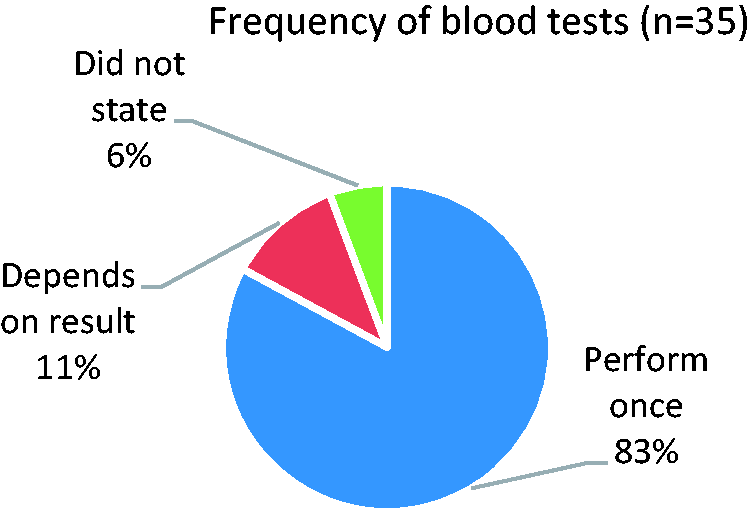
Whether blood tests are repeated prior to initiation of testosterone.
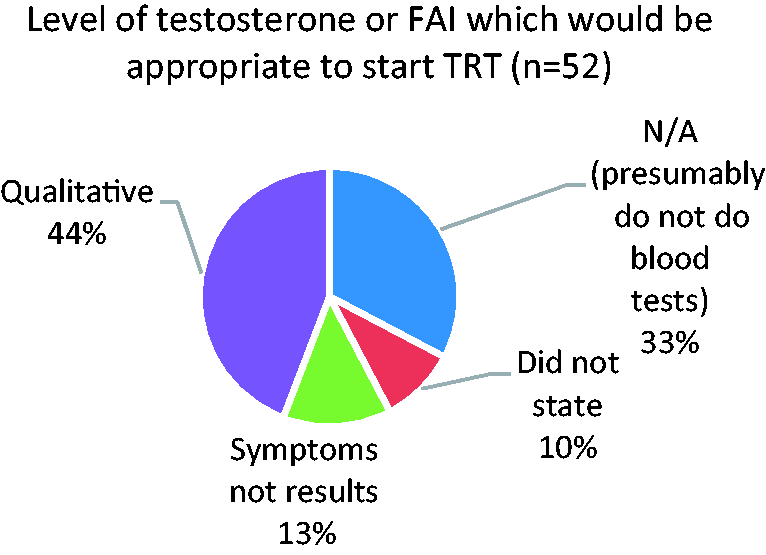
Whether there is a specific testosterone or FAI blood level at which it is appropriate to start testosterone.
The different levels of testosterone or FAI at which participants consider it would be appropriate to start testosterone.

FAI: free androgen index.
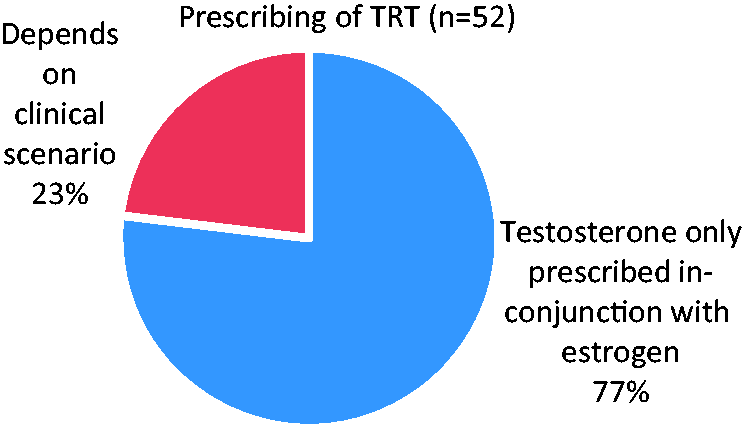
The prescribing of testosterone alone or only in conjunction with estrogen.
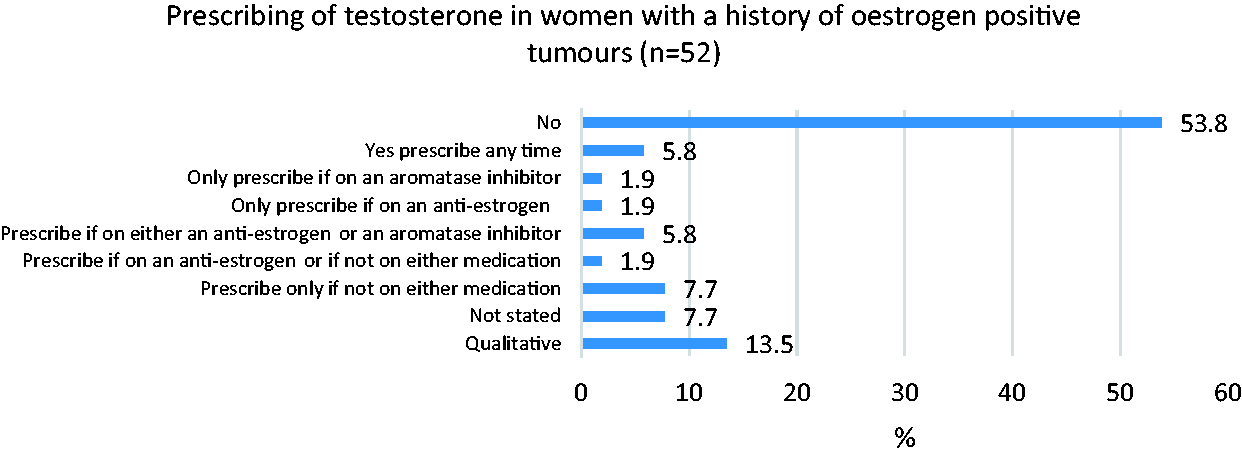
The prescribing of testosterone in women with a history of estrogen-positive tumours.
The qualitative reasons given for prescribing testosterone in women with a history of estrogen-positive tumours.

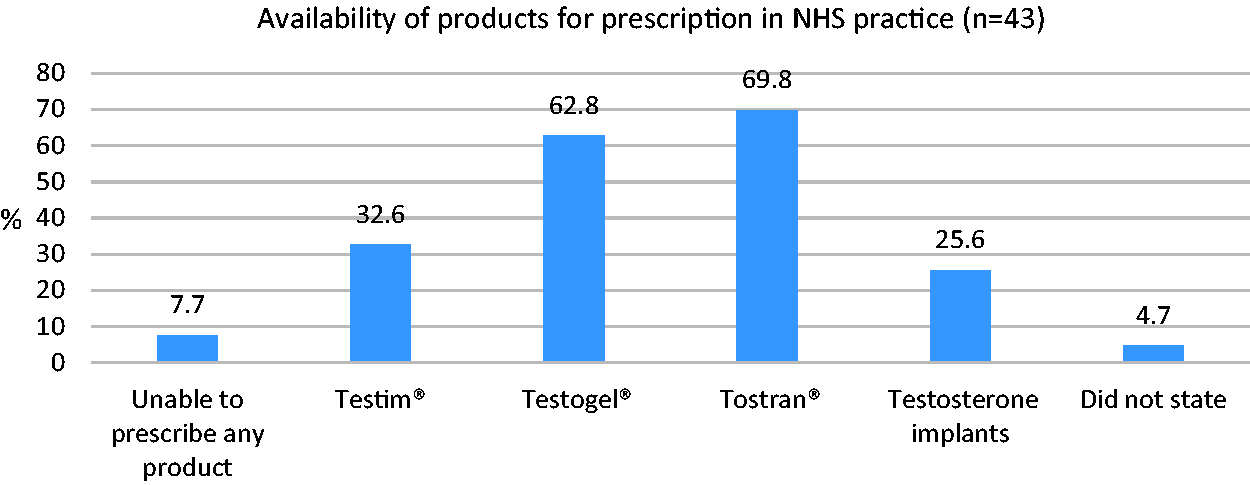
Testosterone preparations available to prescribe in NHS practice.
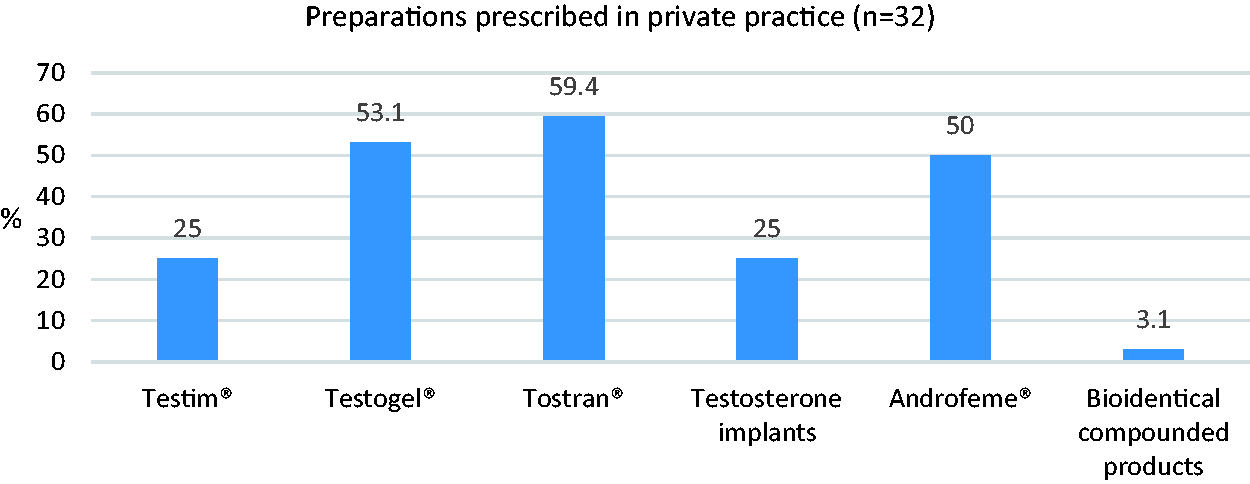
Testosterone products available to prescribe in private practice.
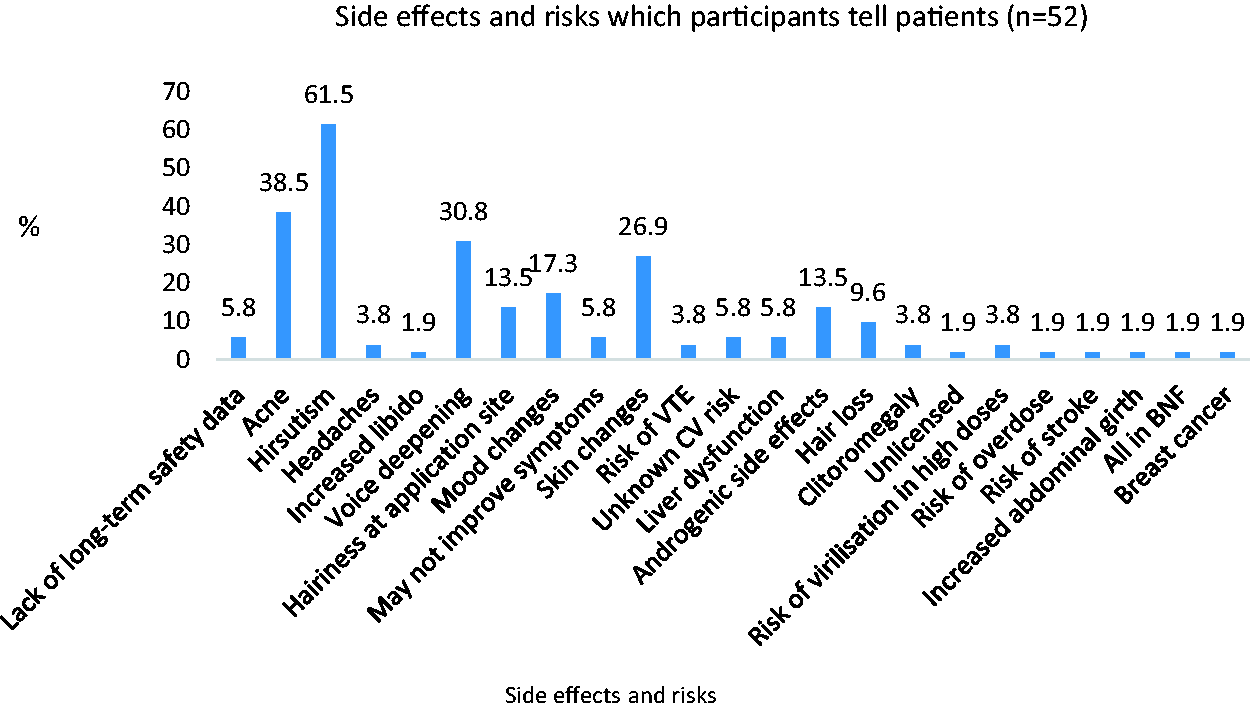
The specific risks/side effects that patients are informed of when starting testosterone.
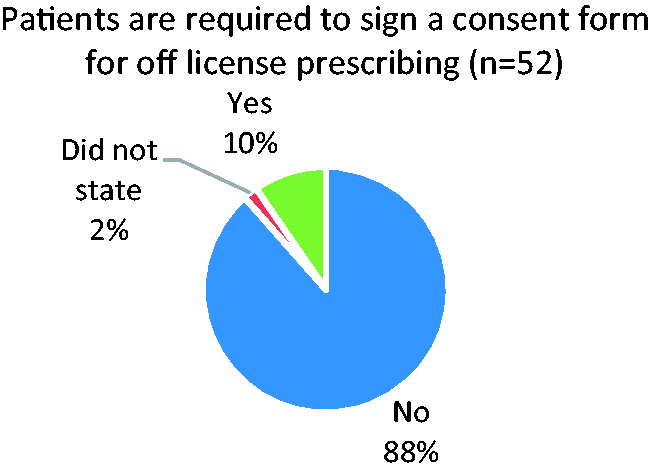
Whether the patient is asked to sign a consent form for off-license prescribing.
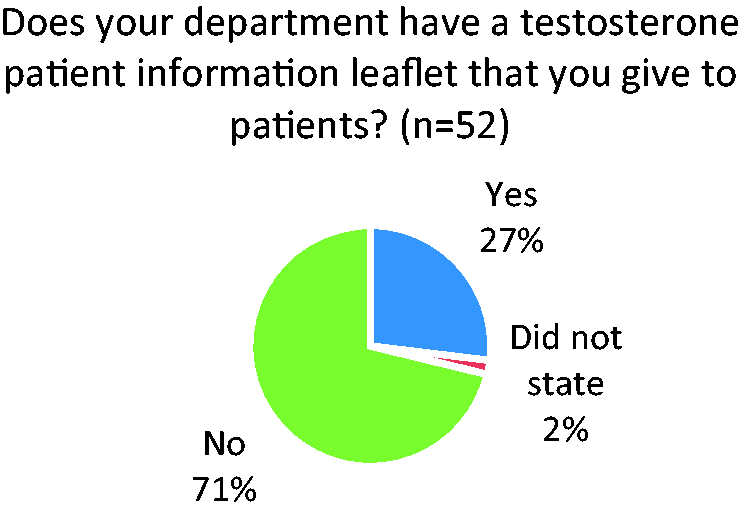
Whether patients are given a departmental testosterone patient information leaflet.
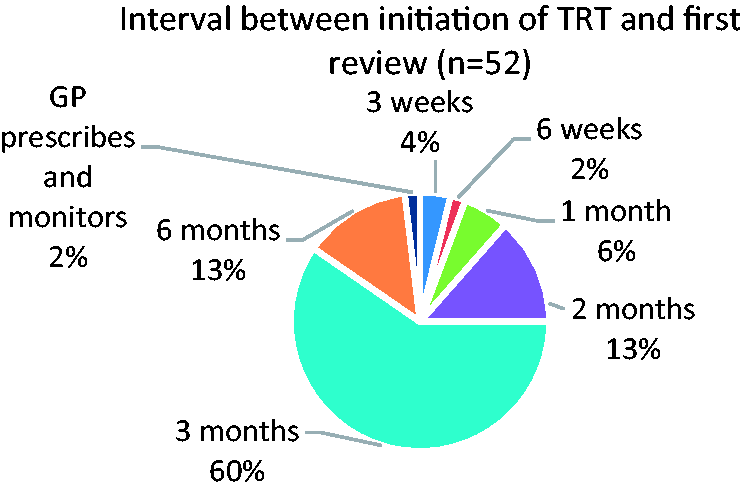
The first review of treatment with the patient after initiation of testosterone.
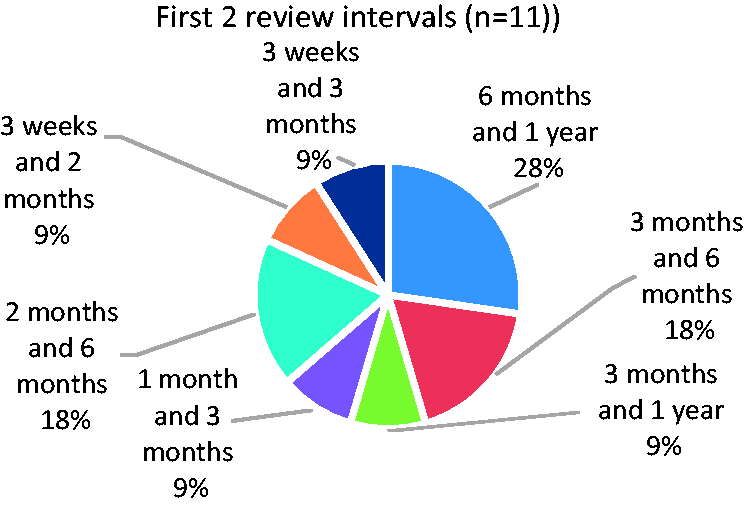
The first and second review intervals after initiation of testosterone.
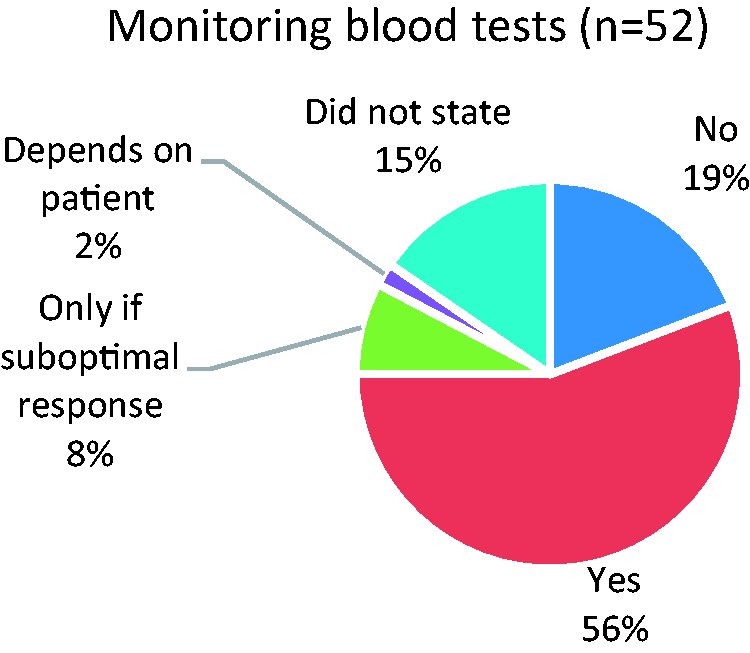
Some participants arrange monitoring blood tests whilst on testosterone treatment.
Different monitoring blood tests are requested.

SHBG: sex hormone-binding globulin; LFT: liver function test; FBC: full blood count.
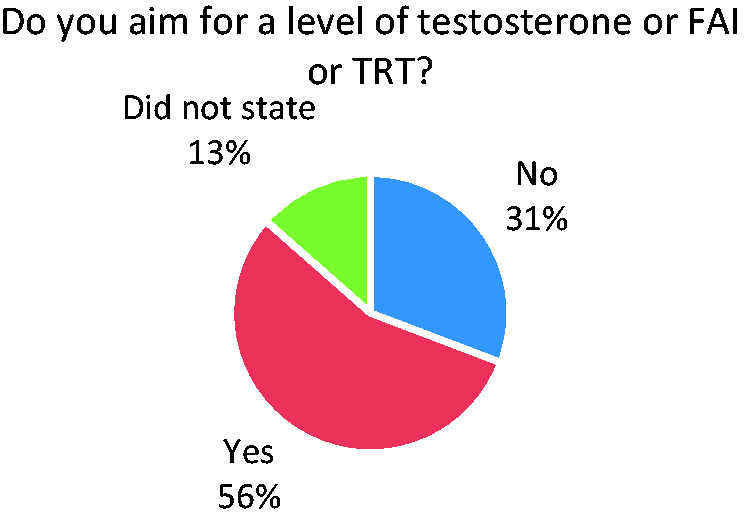
Some participants aim for a specific testosterone or FAI level when prescribing testosterone.
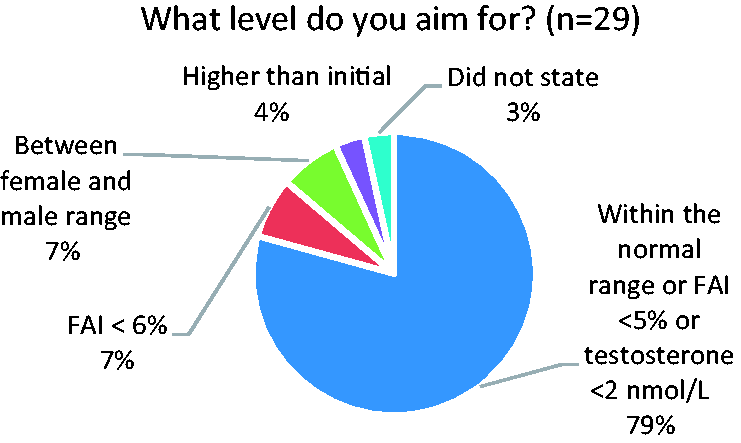
The level of testosterone or FAI that participants aim for when prescribing testosterone.
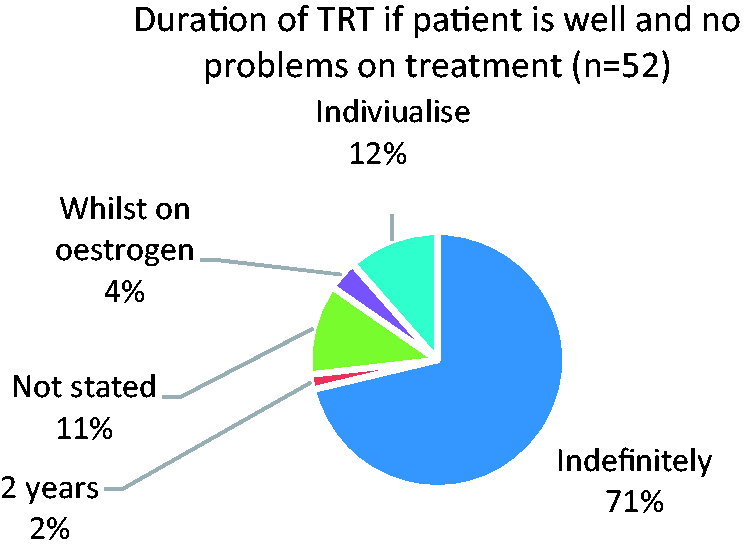
The length of time that participants are happy for the patient to stay on testosterone.
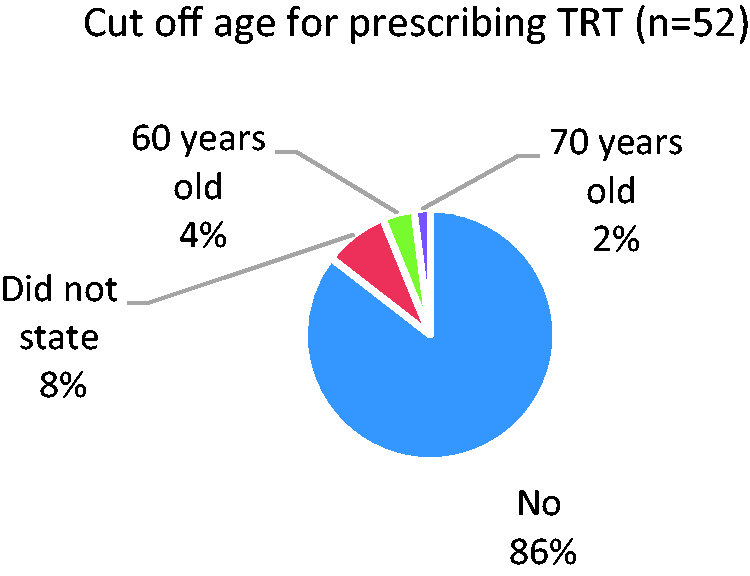
Some participants have a cut off age when they would stop prescribing testosterone.
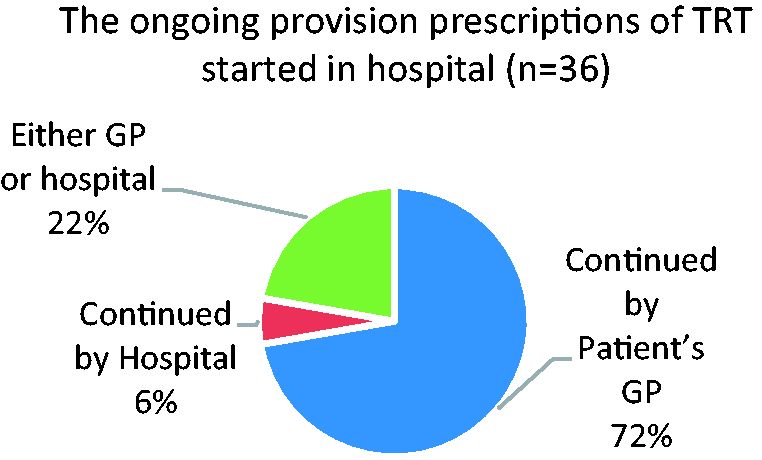
The provision of ongoing testosterone prescriptions after initiation in NHS practice.
Results
A total of 124 participants were surveyed, and there were 57 responses. Of these, two were errors in submission causing duplicates and were therefore discarded leaving a total of 55 participants, which was a 44% response rate. Three consultants said they did not prescribe testosterone at all and so they were therefore removed from further analysis leaving a remaining 52 responses which were analysed further.
The survey participants were from a spread of roles including Consultants, Menopause Specialists and Associate Specialists, Specialist Nurses and General Practitioners (Figure 1). They undertook a mixture of NHS and Private Practice (Figure 2). Most (62%) did not have a departmental prescribing guideline (Figure 3). Lots of different reasons were given for situations in which the participants consider testosterone should not be prescribed (Figure 4, Table 1).
There was variability in the requirements for blood tests and monitoring of TRT (Figures 5–8, 18–20 Table 2, 3, 5). Most participants (77%) only prescribed testosterone in conjunction with estrogen (Figure 9). The majority (53.8%) of participants did not prescribe testosterone in women with a history of estrogen positive tumours, some participants said they would prescribe if they were on an aromatase inhibitor or on an anti-estrogen (Figure 10) or in specific circumstances (Table 4).
Several products were available for prescription in both NHS (Figure 11) and private practice (Figure 12), with Androfeme® and Bioidentical compounded products being available privately, whereas they were not prescribed in NHS practice.
Several different side effects and risks were discussed with patients prior to initiation of TRT (figure 13). 10% of participants required their patients to sign a consent form for off-license prescribing (Figure 14). The majority (71%) did not have a patient information leaflet for TRT (Figure 15). Durations between initiation and review of patients varied (Figure 16, Figure 17). Participants had different views on how long patients could stay on TRT (Figure 21) and until what age (Figure 22). The provision of ongoing testosterone prescriptions after initiation in NHS practice varied, with some continued by the GP and others from hospital (Figure 23).
What is your role? Does your department have a testosterone prescribing guideline? Are there any reasons why you would not prescribe testosterone in a woman with symptoms of androgen deficiency? Do you arrange initial blood tests prior to starting testosterone? Are these blood tests fasting/non-fasting or at a particular time of day? Do you perform these tests once or do you repeat them prior to initiation? What level of testosterone or free androgen index (FAI) would you consider it appropriate to start testosterone? Do you prescribe testosterone alone or only in conjunction with estrogen? Do you prescribe testosterone in women with a history of estrogen-positive tumours? What products are available for you to prescribe in your NHS practice? What products do you prescribe in your private practice? Have you had any problems with supply of any products? 84.6% have had supply issues with product availability. When starting testosterone, what specific risks/side effects do you tell the patient? Do you request that the patient signs a consent form for off-license prescribing? Does your department have a testosterone patient information leaflet that you give to patients? After starting treatment, what is your usual reviewing pattern during the first year of treatment? Do you arrange any monitoring blood tests? Do you aim for a specific testosterone or FAI level? If the patient is feeling well and there are no problems on the treatment, is there a limit as to how long you are happy that they can stay on it? Do you have an age cut-off when you would stop prescribing? If you are an NHS hospital doctor, how are ongoing prescriptions issued?
For the participants who responded that either the GP or the hospital would continue the prescribing, many of these responses made the comment that it was only if the GP is unable/refuses that the hospital will do the prescribing.
22. If prescriptions are issued from the NHS hospital, what is the maximum duration that you are able to prescribe?
The duration of prescriptions issued from the NHS hospital ranged from two weeks to six months.
Discussion
Androgens are precursor hormones for estrogen production and also act directly via androgen receptors which are widespread throughout the body. Androgens are important for bone density and muscle mass; cognitive function, mood and a sense of well-being; sexual function and energy. 6
The Princeton Evaluation of peer-review literature and consensus conference of international experts, suggested guidelines for clinical assessment and diagnosis of female androgen insufficiency. 6 They recommended that androgen insufficiency could be diagnosed if clinical symptoms were present and not attributable to other disease processes (one example of many would be thyroid disease); the patient was adequately estrogenised; and free testosterone values were in the lowest quartile of the normal range. 6 The most described symptoms of androgen insufficiency include dysphoric mood; unexplained fatigue; change in sexual function including reduced libido; changes in cognition; vasomotor symptoms; bone loss and decreased muscle strength. 6
A Cochrane review looked at the use of testosterone as an add on to estrogen-only or estrogen plus progestogen HRT and found that testosterone has a positive effect on sexual function in postmenopausal women. 7 Testosterone has been shown to have additional benefits including the improvement of urogenital, psychological and somatic symptoms, 8 an increase in bone density when combined with estrogen 9 and enhancement of cognitive performance.10,11
Testosterone is produced by the ovaries and by peripheral conversion of the pre-androgens androstenedione and dehydroepiandrosterone which are synthesised in the ovaries and adrenal glands. Androgen levels fall with age, particularly in early reproductive years, flatten out in midlife and do not appear to reduce significantly at the time of menopause in contrast to the decline of estrogen. The postmenopausal ovary does continue to produce a small amount of testosterone.12,13 Testosterone levels reduce at an earlier age in women who have premature ovarian insufficiency (POI). 6 In women who have an oophorectomy, testosterone levels reduce abruptly and without the small amount of postmenopausal testosterone produced by the ovary, these women can become particularly symptomatic with symptoms of androgen insufficiency.
Determining the normal range of testosterone in women is difficult due to changes with age, menstrual cycle and circadian rhythm. Testosterone levels are at their highest mid-cycle and have a peak concentration in the early morning. 14 Most of the available tests do not provide the accuracy or precision required when testing the low serum concentrations in women. As most testosterone is protein bound to sex hormone-binding globulin (SHBG), there is only a small circulating free fraction which is difficult to measure reliably. Bioavailable testosterone is affected by SHBG, with higher levels of SHBG binding more testosterone and therefore being associated with lower bioavailable testosterone levels. The level of bioavailable testosterone can either be calculated using free testosterone concentration, measured by equilibrium dialysis, 6 or indirectly by calculation of the free androgen index (FAI = total testosterone/SHBG × 100). However, as testosterone is also made in peripheral tissues, serum levels may not accurately reflect tissue exposure. 15 There is also individual variation in androgen receptor sensitivity, 15 which may explain why symptoms of androgen deficiency do not always correlate with the serum level of bioavailable testosterone, with some women having low levels but being asymptomatic, and some women having troublesome symptoms and levels within the normal range.
Measuring testosterone levels in women when considering starting treatment can add weight to the diagnosis of androgen deficiency, justification of a trial of treatment and can be useful to demonstrate that levels have increased if tested after treatment has been initiated. 3 This will also exclude high baseline concentrations and ensure that supraphysiological concentrations do not occur during treatment. 4 Current BMS guidance suggests a low FAI of <1% in a symptomatic woman supports the use of testosterone, and that if monitoring treatment, the level of FAI should be maintained at <5% but that clinical improvement in symptoms is more important than aiming for a specific level on treatment. 3 The Endocrine Society Guidelines on Androgen Therapy in women suggests measuring testosterone levels at baseline, three to six weeks after treatment initiation and then six monthly, with cessation after six months if there has been no response to treatment, 16 and this position has also been endorsed by the recent Global Consensus Statement. 4
Giving testosterone via the transdermal route avoids first-pass metabolism in the liver and leads to more physiological and stable serum levels. 17 A systematic review and large meta-analysis of the safety of the transdermal patch showed that no changes in serum lipid profile, renal, liver function or blood cell indices were seen with transdermal testosterone. 18 Testosterone does not appear to stimulate the endometrium.17,19
Available data on the use of testosterone and cardiovascular risk appears to be reassuring, 19 but there is not much long-term data. A small study looking at the combination of HRT plus testosterone implants showed that they increased endothelium-dependent flow-mediated dilation in the brachial artery more than HRT only users. 20 This implies that testosterone may improve coronary endothelial function. Another small study assessed the effect of a six-month testosterone supplementation therapy, in the form of the transdermal patch, on functional capacity and insulin resistance in female patients in their 60s and 70s with chronic heart failure (CHF) and found that there were improvements in functional capacity, insulin resistance and muscle strength in women with advanced CHF treated with testosterone. 21 Improvements in insulin resistance may protect against cancer, cardiovascular disease and metabolic syndrome. 22 A study in the UK population of 2103 women using testosterone therapy compared to 6309 controls showed no statistically significant differences between the two groups in the rates of cerebrovascular disease, ischaemic heart disease, breast cancer, deep venous thrombosis/pulmonary embolism, diabetes mellitus or acute hepatitis. 23 A recent systematic review and meta-analysis of treatment in women has shown that transdermal testosterone is not associated with an increase in cardiovascular events, did not cause an increase in blood pressure, was not associated with an increased risk of venous thromboembolism (VTE) and has no adverse effect on lipid profile. 24
There is evidence that testosterone has an inhibitory effect on the breast and is breast protective. 25 A study looking at transdermal testosterone in combination with estrogen over a four-year period found no evidence of an increased risk of breast cancer. 26 Studies looking at women prescribed testosterone alone (without concomitant estrogen) were also reassuring that there was no significant increase in breast cancer, but the trials were of short duration and breast cancer was not the primary end point.27,28 A retrospective cohort study did not find any significant increased incidence of breast cancer in patients treated with testosterone. 29 The Dayton study began in 2008 and was a large 10-year observational, longitudinal study which looked at the incidence of breast cancer in a group of 1268 pre-menopausal and postmenopausal women with symptoms of androgen deficiency who were treated with testosterone implants. 30 Some of these women were treated with testosterone alone and some, who had either had symptoms of excess estrogen or an increased risk of breast cancer, were given testosterone and anastrozole in combination. At the five-year interim analysis, both groups had a lower rate of breast cancer compared to the background population risk. 30 The full 10-year analysis is awaited.
As testosterone is aromatised to estrogen, which may stimulate the breast, there has been concern about how safe it is to give testosterone to women with a history of hormone-dependent breast cancers. As third-generation aromatase inhibitors effectively inhibit the aromatisation of testosterone to estrogen, it has been postulated that testosterone may help improve menopausal symptoms in these women without increasing breast stimulation, and there is a small amount of evidence that it can be safely be used in women with hormone-sensitive breast cancer who are taking aromatase inhibitors. 31 A study has shown that the antiproliferative effects of anastrozole on human breast cancer cells which had been cultured in vitro was significantly enhanced by combined treatment with testosterone. 32 A case study of a 51-year-old postmenopausal woman, treated with testosterone implants for seven years prior to a diagnosis of hormone receptor-positive breast cancer, describes how after diagnosis she continued with subcutaneous testosterone implants and had additional high-dose letrozole implants. 33 There was a 43% reduction in tumour volume in six weeks and the tumour responded at an increased rate to neo-adjuvant chemotherapy. 33 The authors suggest that the higher dose letrozole allowed a greater inhibitory effect of testosterone at the breast therefore enhancing the response to further treatment. 33 Small trials have found that vaginal testosterone given to women on aromatase inhibitors was effective at treating vaginal atrophy and dryness and that estrogen levels remained suppressed. 34 , 35 There is also evidence that testosterone may be beneficial in women with metastatic breast cancer who become refractory to treatment with other endocrine therapy. 36 Current research in this area continues.
Side effects which may occur with testosterone replacement include acne and increased hair growth at the site of application and a small increase in weight, but increase in facial hair, alopecia or voice deepening does not occur if testosterone levels are kept within the female physiological range. 24
Conclusions
Our results demonstrate differing practices in the prescribing of TRT. The results suggested anxiety on the part of the participants in terms of the safety profile of testosterone with regard to cardiovascular disease, risk of VTE, effect on endometrium and hormone-dependent cancer. Participants can be reassured that with transdermal testosterone therapy there is no evidence of an increased risk of breast cancer, cardiovascular disease, VTE or stimulatory effect on the endometrium. Long-term safety data of TRT is lacking, the BioSante LibiGel Safety Study (BLISS) data37 looking at the rate of cardiovascular events and breast cancer in women on testosterone gel will hopefully be available soon. Numerous side effects and risks were discussed with patients prior to initiation of TRT but patients can be reassured that side effects are unlikely if levels are kept within the physiological range for women.
In terms of blood tests, as no changes in serum lipid profile, renal function, liver function or blood cell indices are seen with transdermal testosterone, it is unnecessary to monitor Liver Function Tests (LFTs), Full Blood Count (FBC) or lipids. In the new BMS guidance on testosterone prescribing,3 a further paragraph could be added making mention of this.
There is not much evidence surrounding the safety of prescribing testosterone in women with hormone-dependent cancers, but there is a small amount of evidence that testosterone in conjunction with an aromatase inhibitor may be safe; however, this would be a decision to be made in conjunction with the oncology team and further research are needed in this area.
A significant problem with prescribing testosterone is lack of available licensed preparations. ‘Unlicensed product’ was a reason given for not prescribing (Table 1) and it is likely that this may either cause apprehension for GPs in continuing prescriptions started in the hospital, or may mean that their medicines management teams will not allow them to prescribe. One possible solution is the development of a shared-care prescribing guideline to interface secondary and primary care and to aid GPs with continuation of the prescription and containing advice (and reassurance) about monitoring and safety of treatment. This could also include a consent form which the patient could sign to acknowledge that the treatment is unlicensed. It would also be helpful to have more information about testosterone prescribing included in the next version of the NICE guidelines, as it is absent from the current guidance. This would further reassure healthcare professionals about prescribing testosterone for women using unlicensed products. The best answer to this would be the development of licensed testosterone products for women in order to address the gender inequality of access to testosterone hormone therapy, but for now the General Medical Council guidance of the prescription of unlicensed medication should be consulted when prescribing.38 The Women's Health Concern has also developed a patient information leaflet about the use of testosterone which is a helpful adjunct for patients.39
Following this project, an article has been published in the British Journal of General Practice to raise the awareness of testosterone prescribing in perimenopausal and menopausal women and to increase GPs' knowledge of the subject.40
We have proposed some updates for our departmental guideline for prescribing of testosterone (online Appendix 2) which we hope to implement. We have suggested a shared-care prescribing guideline which we hope to utilise to send to our GP colleagues when we have initiated testosterone treatment in the hospital setting (online Appendix 3). We have also recommended some changes to our patient information leaflet (online Appendix 4).
Recommendations
Updated consensus BMS Guidance All departments should have a protocol for the prescribing of testosterone in women All departments should have an information leaflet for female patients The development of a BMS-endorsed proforma for shared-care prescribing guideline Inclusion of guidance on testosterone prescribing in next NICE guidance on the management of the menopause Repeat audit of prescribing amongst menopause specialists in the future.
Supplemental Material
sj-pdf-1-min-10.1177_2053369120985743 - Supplemental material for The testosterone prescribing practice of BMS menopause specialists
Supplemental material, sj-pdf-1-min-10.1177_2053369120985743 for The testosterone prescribing practice of BMS menopause specialists by A Scott, D Holloway J Rymer and D Bruce in Post Reproductive Health
Supplemental Material
sj-pdf-2-min-10.1177_2053369120985743 - Supplemental material for The testosterone prescribing practice of BMS menopause specialists
Supplemental material, sj-pdf-2-min-10.1177_2053369120985743 for The testosterone prescribing practice of BMS menopause specialists by D Holloway J Rymer and D Bruce in Post Reproductive Health
Supplemental Material
sj-pdf-3-min-10.1177_2053369120985743 - Supplemental material for The testosterone prescribing practice of BMS menopause specialists
Supplemental material, sj-pdf-3-min-10.1177_2053369120985743 for The testosterone prescribing practice of BMS menopause specialists D Holloway J Rymer and D Bruce in Post Reproductive Health
Supplemental Material
sj-pdf-4-min-10.1177_2053369120985743 - Supplemental material for The testosterone prescribing practice of BMS menopause specialists
Supplemental material, sj-pdf-4-min-10.1177_2053369120985743 for The testosterone prescribing practice of BMS menopause specialists by A Scott, D Holloway J Rymer and D Bruce in Post Reproductive Health
Footnotes
Acknowledgement
Henry Bruce assisted with data compilation.
Authors contribution
All authors conceived the manuscript. AS researched the literature, completed the data collection, and wrote the first draft of the manuscript. DB complied the data into tables and charts. All authors reviewed and approved the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.