
Abstract
The menopausal transition is associated with increasing sleep disorders including sleep apnoea and restless leg syndrome. Insomnia is the most common and is recognised as a core symptom of the menopause. Guidelines to support decision making for women with sleep problems during the menopausal transition are lacking. Sleep problems are associated with negative impacts on healthcare utilisation, quality of life and work productivity. Sleep deprivation is a risk factor for cardiovascular disease, diabetes, obesity and neurobehavioral dysfunction. Declining oestrogen is implicated as a cause of menopausal sleep disruption. Vasomotor symptoms (VMS) and menopausal mood disturbance are also factors in the complex aetiology. VMS commonly precipitate insomnia and, due to their prolonged duration, they often perpetuate the condition. Insomnia in the general population is most effectively treated with cognitive behavioural therapy (CBT) (also effective in the menopausal transition.) The associations of menopausal sleep disturbance with VMS and depression mean that other treatment options must be considered. Existing guidelines outline effectiveness of hormone replacement therapy (HRT), CBT and antidepressants. HRT may indirectly help with sleep disturbance by treating VMS and also via beneficial effect on mood symptoms. The evidence base underpinning menopausal insomnia often references risks associated with HRT that are not in line with current international menopause guidelines. This may influence clinicians managing sleep disorders, leading to hesitation in offering HRT, despite evidence of effectiveness. Viewing sleep symptoms on an axis of menopausal symptoms – towards vasomotor symptoms or towards mood symptoms may help tailor treatment options towards the symptom profile.
Introduction
Sleep disturbances are among the most common symptoms of the menopause. 1 Despite a growing evidence base, there are few clinical guidelines to support decision making for women presenting with sleep problems during the menopausal transition. The evidence base is heterogeneous due to the multi-symptom profile of the menopause, and the multifactorial aetiology of sleep problems. 2
This article reviews the context of sleep problems associated with menopause and what the evidence tells us about management. It identifies factors in clinical presentation that should be understood to support women in achieving the best outcomes in line with their preferences, values, demographics, symptoms and risk profiles.
Sleep and the menopause
Prior to the menopause, women have been found to sleep objectively better than men with higher total sleep time, lower percentage of stage 1 (light) and higher percentage of slow wave (deep) sleep. 3 Healthy young women experience less sleep disturbance due to external stressors than men. This gender dimorphism in sleep regulation may have arisen to protect women from the demands of infant and childcare. This changes as women enter the perimenopause, when they are more likely to experience sleep disturbance, peaking in late perimenopause and continuing into post menopause. 4 The most common symptom is difficulty maintaining sleep, reported by 40–60% of peri- and postmenopausal women, as well as increased difficulty falling asleep. 5 50% of postmenopausal women with difficulties sleeping obtain < 6 h of sleep. 6
The aetiology of sleep problems in the menopause is uncertain. Possible reasons include a decline in oestrogen,
7
disruption due to vasomotor symptoms (VMS) or relationship to co-existing psychiatric disorders. Symptoms may be related to another sleep disorder.
8
There is an increased incidence of sleep-disordered breathing (SDB) during the menopause, although the mechanism is not clear.
9
Restless leg syndrome (RLS) is a condition more prevalent in women than men, and it increases in severity after menopause regardless of the use of HRT.
10
Figure 1 lists some questions that may help to determine the presence of a sleep disorder. Questions to help determine a sleep disorder.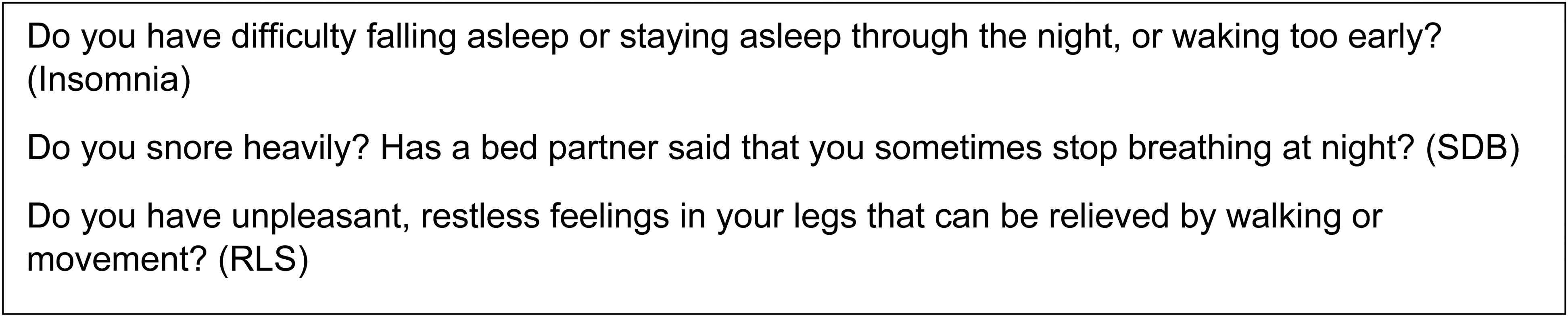
Sleep problems are associated with significant negative impact on healthcare utilisation and costs, health-related quality of life, work productivity, and can have long-term effects on health and wellbeing. 11 Sleep deprivation is a risk factor for cardiovascular disease, diabetes, obesity and neurobehavioral dysfunction. 12 Both disturbed sleep and menopause are linked to impaired female sexual health and satisfaction.13,14
Insomnia
Insomnia disorder is defined as dissatisfaction with sleep quantity or quality, associated with one (or more) of the following symptoms: difficulty initiating sleep, difficulty maintaining sleep, frequent awakenings or problems returning to sleep. The sleep difficulty occurs at least three nights per week and is present for at least 3 months. 15 The prevalence increases as women approach and pass through the menopause. 5 At a State-of-the-Science Conference in 2005, 16 insomnia was described as one of the core four symptoms of the menopause.
Spielman’s three-factor model (1987) describes the chronicity of insomnia using the ‘3 Ps’ predisposing factors (such as genetics and personality type), precipitating factors (such as illness, stress and vasomotor symptoms) and perpetuating factors (unhelpful cognitions and behaviours).9,17 Menopause symptoms can be both a precipitating and a perpetuating factor for insomnia. Insomnia treatment is based in managing the perpetuating factors. Cognitive behavioural therapy for insomnia, CBT-I, is recommended first line and is efficacious. 18
Menopause, insomnia and vasomotor symptoms
Vasomotor symptoms (VMS) affect most women during the menopausal transition and are strongly associated with sleep disturbances. 1 Hot flushes are reported by up to 85% of menopausal women, 19 and average duration of hot flushes is about 5.2 years. 20 The Study of Women’s Health Across the Nation (SWAN) found that women with moderate-to-severe hot flushes are almost three times more likely to suffer from frequent nocturnal awakenings compared to women without hot flushes. 21
Menopause, insomnia and depression
Affective symptoms are independently associated with both menopause and with insomnia. SWAN data show 16.5% women in menopausal transition reported depressed mood. 22 The relationship between sleep and depression is bidirectional: sleep disturbance can be both a consequence of depressed mood as well as a cause of depression. 23 Numerous studies show that treating sleep disturbance can improve symptoms of depression 24 and the importance of identifying and managing insomnia during this transition should be emphasised.
Existing guidelines
The Italian Association of Sleep Medicine (2019) carried out a systematic review of evidence informing a position statement on the management of postmenopausal sleep disorders. 25 This emphasises the co-occurrence of insomnia, vasomotor symptoms and depression. It states that overall hormone replacement therapy (HRT) improves vasomotor symptoms, insomnia and mood, and that postmenopausal insomnia is best managed with HRT and CBT-I. It also suggests antidepressants can improve insomnia, alone or in association with HRT.
The British Association for Psychopharmacology (BAP) consensus statement on evidence-based treatment of insomnia (2019) 26 highlights the increased incidence of insomnia (and sleep-disordered breathing) after the menopause and outlines treatment strategies that include HRT, CBT-I and antidepressant medication
Hormone replacement therapy
Oestrogen-based hormonal therapy is effective in treating menopause-related symptoms and improving quality of life for postmenopausal women. HRT is recommended in national and international guidelines including those of the National Institute of Clinical Excellence and the International Menopause Society.27,28
Oestrogen can improve sleep quality indirectly through a domino effect. 26 It is an effective treatment for vasomotor symptoms (75% reduction in the frequency of hot flushes relative to placebo.) 29 Reducing VMS decreases the frequency of night-time waking, improving sleep. Oestrogen HRT has also been found to improve depression symptoms, and NICE recommends HRT first line as treatment for low mood relating to the menopause. 28
Progesterone may also improve sleep. 30 It stimulates benzodiazepine receptors, causing the release of gamma-aminobutyric acid (GABA), a sedating neurotransmitter that can facilitate sleep cycles. 31
A 2015 systematic review of 23 articles looking at HRT treatment and chronic menopausal insomnia found significant, continuous improvement in sleep in 14 of the 23 studies. The other nine showed no difference. 32 A systematic review in 2017 reported that HRT improved sleep quality in women with vasomotor symptoms but that evidence for improved sleep in women without such symptoms was lacking. 2
Much of the literature regarding how to manage menopausal sleep problems refers to possible associated risks of HRT, often in reference to the Women’s Health Initiative (WHI) Report in 2002. 33 This report suggested worsening cardiovascular outcomes in women taking HRT and was followed by a sharp decline in HRT use. Despite many articles contradicting the initial analyses, the early findings are often referenced in more contemporary sleep and menopause research.34,35 In 2015, Tal et al. reviewed insomnia symptoms during the menopause, calling the WHI findings ‘undoubtedly concerning’. 9 A 2019 randomised control trial of non-pharmacological treatments for postmenopausal insomnia commented, ‘HRT has limited efficacy and carries serious health risks’. 36 This narrative may lead to concerns regarding HRT and could limit a possibly efficacious treatment option. 37 Interdisciplinary education regarding the management of menopause, and the utilisation of a multidisciplinary approach to management of sleep disorders in mid-life women may help reach a shared understanding of sleep disorders and dispel myths about HRT. 38
Cognitive behavioural therapy for insomnia
CBT-I is the first-line treatment for insomnia in adults and has been shown to be effective in insomnia with long-lasting benefits.18,27 It is a structured, skill-focused programme that consists of cognitive and behavioural techniques and sleep education. CBT-I has been shown to effectively treat menopause-related insomnia disorder. 36 It is not possible to compare the effect size of CBT-I and hormone replacement therapy in the current literature.
Instead of approaching the physical symptoms that may trigger insomnia, CBT-I focuses on the cognitive and behavioural factors that prolong insomnia. These include distress about poor sleep and dysfunctional efforts to induce sleep, causing conditioned arousal.
Understanding these factors helps explain why some women’s sleep disturbance does not improve following the cessation of vasomotor symptoms that were originally thought to be the cause. The provision of face-to-face CBT-I is limited, leading to development of digital offers which are effective in improving health and wellbeing in patients with insomnia symptoms. 39
Antidepressants
Several antidepressants have been shown to improve insomnia, 40 and some, selective serotonin reuptake inhibitors (SSRIs) and serotonin and noradrenaline reuptake inhibitors (SNRIs), are also indicated for treating vasomotor symptoms in postmenopausal women.26,27
Venlafaxine (an SNRI) has been shown to reduce VMS in healthy postmenopausal women and breast cancer survivors. 41
The BAP advises antidepressants should be considered when there is a co-existent mood disorder. 25 However, the side effect profile of commonly used SSRIs can lead to counter-productive sleep disruption and sexual dysfunction. 42 Sedating drugs (trazodone or mirtazapine) have been shown to reduce insomnia in people with depression. Tricyclic antidepressants are commonly used, though with little evidence of efficacy (and increased risks in overdose.)
Hypnotics
Sedative hypnotic medication can be effective in improving sleep, although few studies have focused on women in the menopausal transition. 26 National and international guidelines for insomnia recommend that hypnotics should not be used long-term due to safety concerns. Potential adverse effects include daytime sedation, poor coordination, cognitive impairment, increased risk of driving accidents, falls, development of tolerance, dependence and withdrawal, rebound insomnia, dementia and increased mortality. 43
Melatonin
Secretion of melatonin reduces with age, which may contribute to sleep disturbances during the menopausal transition and beyond. In the United Kingdom, one prolonged-release melatonin tablet is licensed for short-term use in adults aged 55 or over. Further research is needed to understand the potential benefit and when to recommend it in clinical practice. 44
Other options
Aerobic exercise, acupuncture, mindfulness, reflexology and yoga have shown some positive results in small groups, but more research is needed to understand the extent of their impact.26,33
Conclusions
Sleep is frequently disturbed during the menopausal transition, with sleep maintenance insomnia being the most common. Menopausal sleep problems are significantly associated with vasomotor symptoms and depression although the aetiology of menopausal sleep disorder is not fully understood.
It is important to treat menopausal sleep symptoms due to their significant impact on women’s quality of life and because sleep deprivation is a risk factor for chronic disease and increased morbidity and mortality.
Hormonal and non-hormonal pharmacological options as well as non-drug therapies should be discussed with women with menopausal insomnia in order to individualise treatment to a women’s needs and preferences. The research is heterogeneous, and it is not possible to compare effect sizes of different treatments.
The authors have suggested an algorithm to support assessment and management for women with disturbed sleep during the menopausal transition (Figure 2). This is based on the evidence discussed and our experience in clinical practice. It should be utilised in conjunction with a woman’s medical history and preferences. The algorithm will be refined by future research on outcomes, ease of use and patient acceptability. Management of sleep disturbance during the menopausal transition.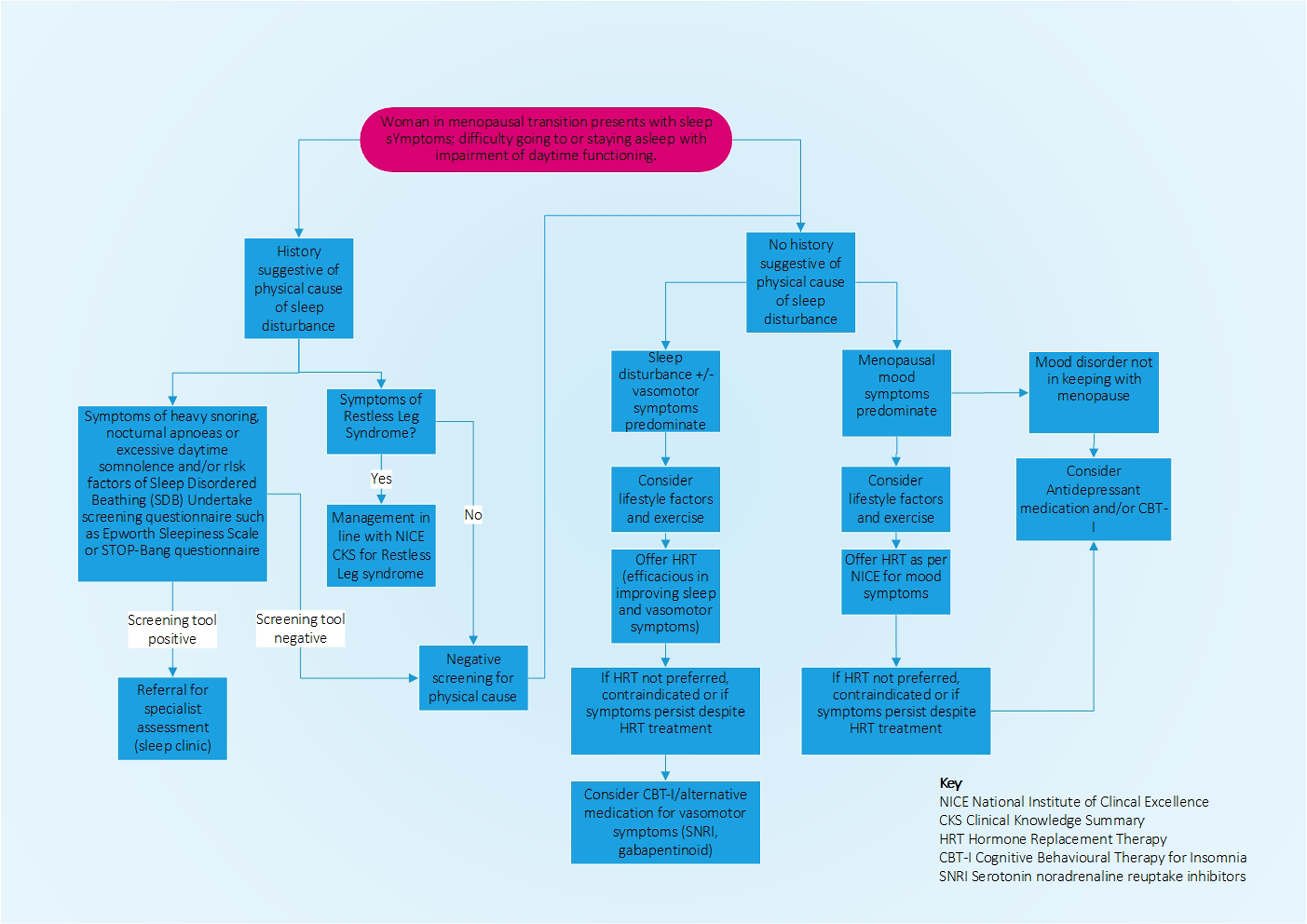
Footnotes
Author contributions
Zoe Schaedel and Janice Rymer conceived the research topic.Zoe Schaedel researched the literature and wrote the draft article.Janice Rymer, Debra Holloway and Deborah Bruce reviewed and edited the article.All authors reviewed and approved the final version of the article.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Zoe Schaedel is a director of The Good Sleep Clinic 2018 to date. The other authors declare no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
ZS