
Abstract
Objectives
Menopause is a natural part of women’s lives and is associated with a series of complications that can impair their quality of life. This study was conducted to determine the effect of specific educational interventions on the quality of life among postmenopausal women.
Methods
This randomized controlled trial was conducted on 80 menopausal women who met the inclusion and exclusion criteria and were selected through the multi-stage stratified random sampling method. The participants were randomly allocated to either the control or intervention group (40 per group). The intervention comprised 5 × 45-min educational sessions based on the Multi-Theory Model on the predetermined days of the week. The scores of the quality of life level were collected at baseline, immediately, and 3 months after the intervention using the Menopause-Specific Quality of Life questionnaire (MENQOL). The control group received a health advice.
Results
Analysis of variance of repeated measures showed a significant interaction between time and intervention. The comparison between the mean score of quality of life of the “before,” “immediately after intervention,” and “3 months after the intervention” showed a significant difference between the two groups. The intervention group quality of life improved significantly as the intervention went on compared to the control group.
Conclusion
Structured simple educational programs based on the Multi-Theory Model could be used as a simple and noninvasive intervention that help menopausal women improve their quality of life through menopausal symptoms relief. Further interventions with larger trials may be required to confirm these findings.
Keywords
Introduction
Menopause is determined by the permanent cessation of menstruation and occurs due to a decline in the production of ovarian sex steroid hormones, estrogen, and progesterone. 1 Generally, the median age at natural menopause is 51 years; however, it varies based on race, ethnicity, and other factors. 2 In Iran, the median age for menopause is estimated at 47.8 years. 3 Women are one of the most important pillars of society, accounting for about half of the population. They are more vulnerable than men due to exposure to different stages of development, one of which is menopause where women spend a third of their lives dealing with hormonal and physiological changes.4,5 Headaches, sleep disorders, mood swings, vasomotor symptoms (e.g., hot flash and night sweats), somatic symptoms (e.g., vaginal dryness, or atrophy and dyspareunia), as well as psychological symptoms (e.g., anxiety, difficulty in concentrating, overreacting to minor upsets, quickly being irritated, and forgetfulness) are all symptoms of menopause that affect various aspects of quality of life for those afflicted.6,7
Many studies have highlighted the negative effects of menopausal symptoms on the quality of life.8–10 However, healthy lifestyle behaviors may positively influence the severity of menopausal complaints. In relevant studies, it has been shown that healthy lifestyle behaviors have remarkable effects on reducing menopausal symptoms, thereby improving the quality of life.11,12 Quality of life has been defined by the World Health Organization as the "individual’s perceptions of their position in life in the context of the cultural and value systems in which they live and in relation to their goals, expectations, standards, and concerns." 13 Quality of life is a multidimensional concept that includes the physical, emotional, and social dimensions of illness and treatment. 14 Moreover, menopausal symptoms can affect the quality of life of women physically, mentally, and socially. Alternative non-pharmacological strategies to promote health and help women to better cope with menopausal symptoms are health education interventions. 4
Various studies have shown the positive effect of educational programs on improving the quality of life.15–17 In health education and health promotion, more coherent and effective planning can be developed using models and theories. 18 One of the practical and effective models is the Multi-Theory Model (MTM) which is cost-effective with flexible constructs that can be used for a variety of behaviors (repetitive and long-term behaviors as well as one-time behavior), and it is applicable in different cultures. 19 The MTM has two important parts, namely, the initiation of behavior change and maintenance of behavior.
The main constructs that influence the initiation of behavior change include "participatory dialogue," "behavioral confidence," and "changes in the physical environment." Furthermore, "emotional transformation," "practice for change," and "change in the social environment" are three main constructs that influence the sustenance of health behavior change. 19 The application of the MTM in predicting behaviors, such as physical activity, fruit and vegetable consumption, 20 water consumption instead of carbonated and sweet drinks, 21 and consumption of small meals 22 has been confirmed in several studies.
Hot flashes are among the most common complications during menopause and the most frequent reason to visit a doctor due to their influence on the quality of life. 23 In previous studies, proper nutritional behaviors (soy consumption, decreasing sugar intake, caffeinated substances, spices, high-fat foods and alcohol, food consumption at specific times, and consumption of fruits and vegetables) have been shown to have a significant impact on menopause symptoms, particularly hot flashes. 24 Studies have also revealed that women who follow regular physical activity have a higher bone density 25 and better sleep quality. 26 Several other studies have reported positive impacts of physical activity on the improvement of vasomotor symptoms.27–30
The MTM has individual, social, and environmental applications in developing plans for educational intervention, and to our knowledge, it has not been previously implemented in the population of postmenopausal women. Furthermore, since various interventions were performed on the Iranian women sporadically and without careful scientific planning, there is a necessity to design an appropriate intervention for this group. Therefore, the framework of this model was used to plan an intervention to improve the quality of life of postmenopausal women, in Yazd, Iran. This study aimed to investigate the effect of an educational intervention based on the MTM on the quality of life of postmenopausal women.
Materials and methods
Sample and study design
This randomized control trial was conducted on 80 menopausal women who were randomly assigned into two groups of intervention and control between February and May 2020 in Yazd, Iran. Based on the values obtained from the descriptive-analytical and pilot phase of the intervention, the first type error of 5%, test power of 80%, and the following formula, the sample size was calculated to be 40 cases per group.
On the other hand, the women who were not willing to participate and continue the training programs, and those who missed more than one session of the training programs and developed a debilitating illness during the research procedures were excluded from the study. After obtaining the required permission from the Yazd Deputy of Health, the health care centers were selected using multi-stage random stratified sampling. In the first stage, based on the socio-economic status, the health care centers of Yazd were divided into three categories of poor, moderate, and good areas in terms of socio-economic status. Subsequently, two centers were randomly selected from each category, and the total centers (n = 6) were divided randomly into the intervention (n = 3) and control groups (n = 3). The educational intervention was designed with an emphasis on effective and statistically significant constructs of the MTM. The designed interventions were pre-tested in the presence of health and educational technology experts, as well as a number of the target population and their families.
Lesson plan of the training program.
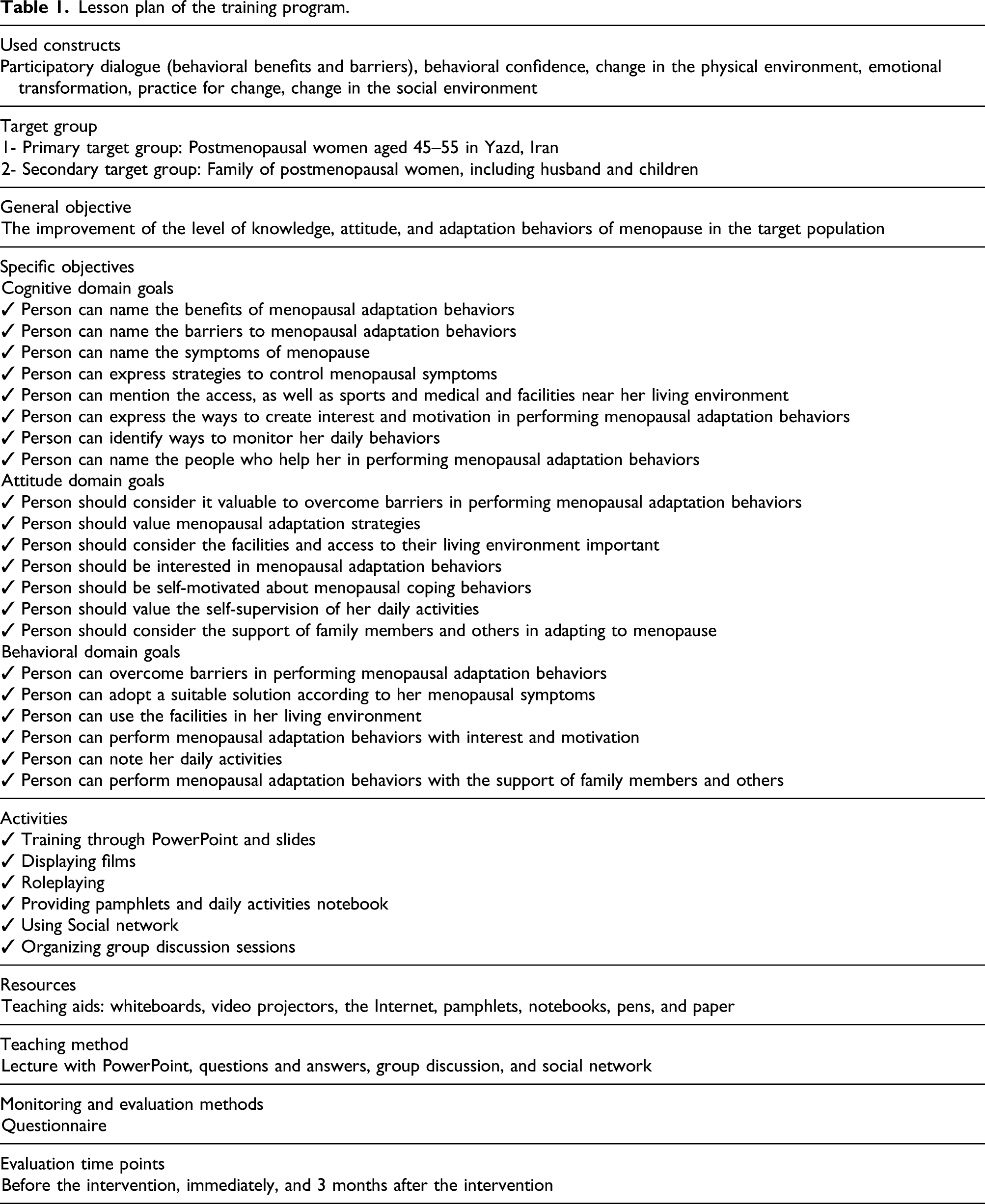
The intervention group received the educational program based on the MTM, whereas the control group received only the routine care.
According to the "participatory dialogue" construct, small group discussion sessions (two 45-min sessions) were held, and the women in these groups discussed the benefits and barriers to healthy behaviors. Following that, a representative of each group announced the result of her group discussion to the other groups. Finally, the session expert presented the strategies for overcoming barriers and emphasizing the benefits of healthy behaviors and their role in improving menopausal symptoms (Table 1).
For the "behavioral confidence" construct, materials on coping with menopausal problems and complications (in PowerPoint format) were provided by a reproductive health professional (a 30-min session). Furthermore, motivational speeches (2 × 25-min sessions) and ways to increase behavioral confidence were provided by a health psychologist. The women were also provided with solutions, such as breaking complex behaviors into simple steps, presenting pamphlets to people, and assigning exercises and homework (start walking 15 min a day in the backyard and gradually continue to 30–40 min a day and plan to reach local green spaces and parks).
Regarding the "changes in the physical environment" construct, brochures containing a list of swimming pools, parks, and green spaces in Yazd (prepared by the Parks and Green Spaces Organization of the Municipality and the Sports and Youth Organization), as well as menopausal care service centers (prepared by the Deputy Minister of Health) were given to the participants in the intervention group. In addition, they were asked to share the recipes for cooking different foods with soy in the social group (WhatsApp Application).
Considering the "emotional transformation construct," a motivational movie (a film about a postmenopausal woman who was able to have a good menopausal period with regular exercise) was displayed (a 20-min session). Moreover, the individuals were asked to interact with each other in the social group, and if they had improved their menopausal symptoms according to the training, they were asked to share their experience via the WhatsApp group so that others could be motivated.
With regard to the construct of "practice for change," a diary notebook of daily activities (monitoring daily behaviors for 1 month) containing healthy behaviors to better adapt to menopause was designed by the research team. This diary notebook was distributed among women in the intervention group with an explanation of how to complete it (a 20-min session). Afterward, if individuals had any questions, they were asked to raise them in the WhatsApp group. They were also asked to report their weekly scores in the group. At the end of the fourth week, the participants would announce their total score, and the three women who scored the highest points were awarded.
Considering the construct of "change in the social environment," a session was held in the presence of the husband or one of the children of the postmenopausal women who were provided with information about the problems, symptoms, and strategies to reduce the symptoms of menopause and support women during this period. People were asked to connect and collaborate to do some activities in groups (Ms. A met and became friends with Ms. B after attending training sessions, and from that point on, they started walking together).
Measures
A structured questionnaire was administered through face-to-face interviews in the health care centers. The questionnaire consisted of two sections, the first of which assessed the socio-demographic variables and reproductive characteristics. The demographic characteristics questionnaire comprised 26 questions which included age, age at the last menstruation, age at the first menstruation, age at the first pregnancy, age at the last pregnancy, marriage age, age at the menopause of mother or sister, regular or irregular menstrual cycles, education, occupation, income, weight, and height.
The second section measured MENQOL, which was designed and standardized by Hilditch et al. 32 at the University of Toronto, Canada. This part consisted of 29 items evaluating vasomotor (n = 3), psychosocial (n = 7), physical (n = 16), and sexual conditions (n = 3). The items were rated based on a 6-point Likert scale of 1 " I do not have symptoms," 2 "very low," 3 "low," 4 "average," 5 "severe," and 6 "very severe." The questionnaire’s total score is between 29 and 174 with a lower score indicating a better quality of life.32,33 In this study, Fallahzadeh et al. tested this questionnaire’s reliability with a Cronbach’s alpha coefficient of 0.85. 34
Statistical analysis
The collected data were analyzed using SPSS software package (version 22). In addition to descriptive statistics indices (central and dispersion indices), parametric or non-parametric analytical statistics tests were utilized after examining the normality or abnormality of the data by the Smirnov–Kolmogorov test. Furthermore, the independent t-test was used to compare demographic variables in the control and intervention groups. Moreover, analysis of variance on repeated measures and Bonferroni’s pairwise comparison test was employed to investigate the changes in the scores of quality of life at pretest, posttest, and follow-up in both intervention and control groups. An analysis of covariance was also used to compare the mean scores of quality of life change in the intervention and control groups, as well as compare the intervention in the two groups with the pretest results.
Results
In total, 80 women (40 subjects per group) participated in and completed the study (Figure 1). Schematic flow chart of the study.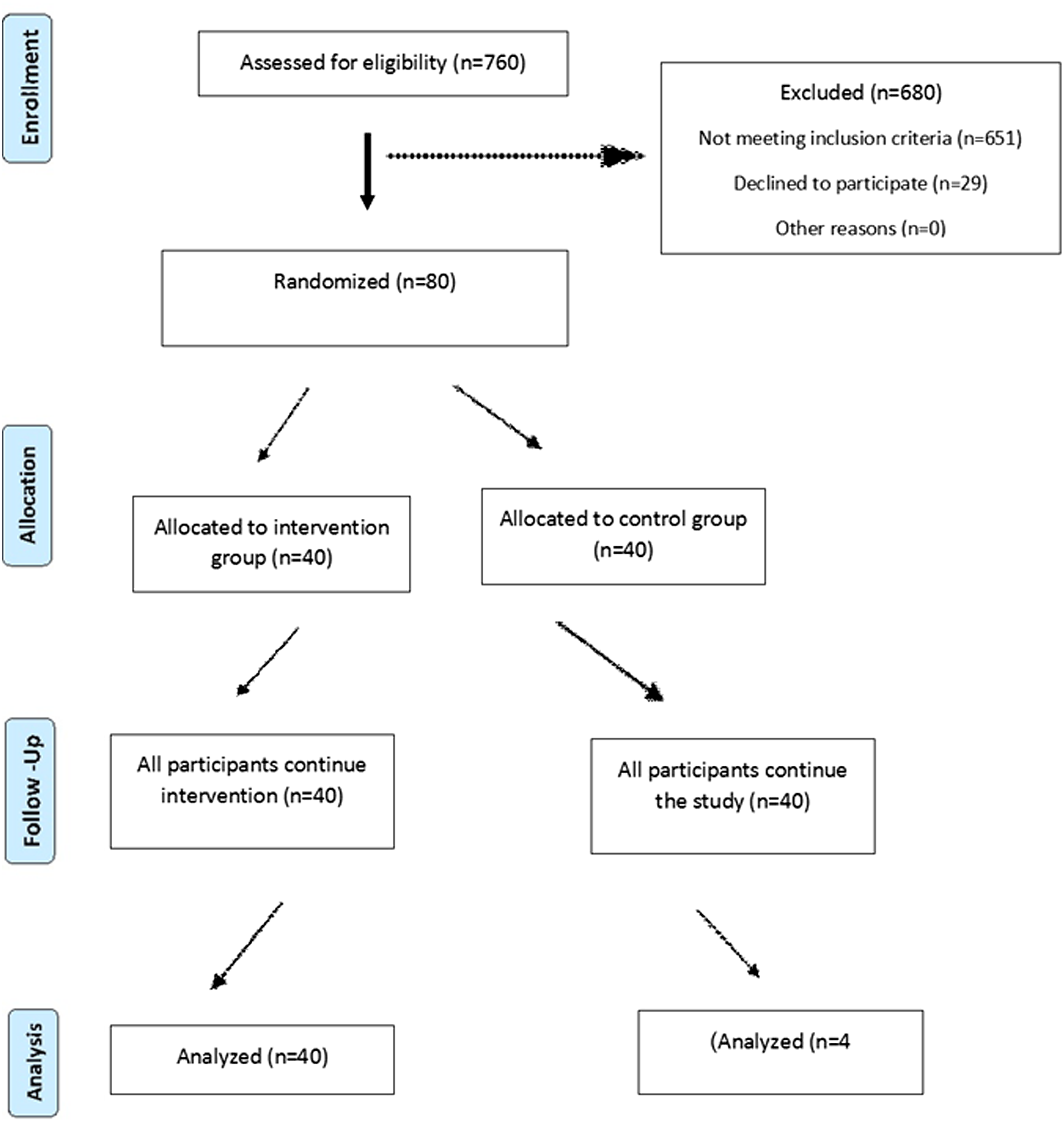
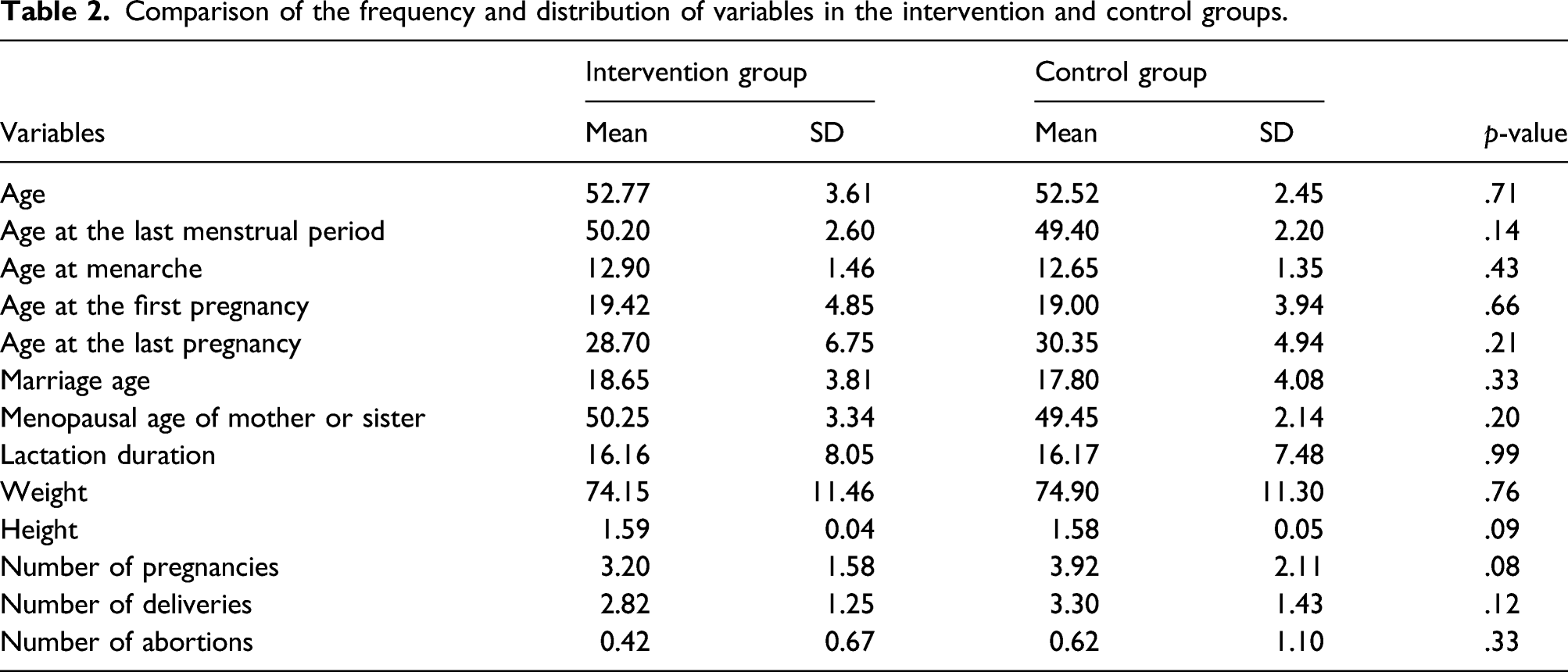
There were no significant differences between the two groups in demographic characteristics, such as education level, occupational status, income, marital status, place of residence, type of delivery, history of infertility, history of taking birth control pills, and history of menstrual cycles.
Comparison of the frequency and distribution of variables in the intervention and control groups.
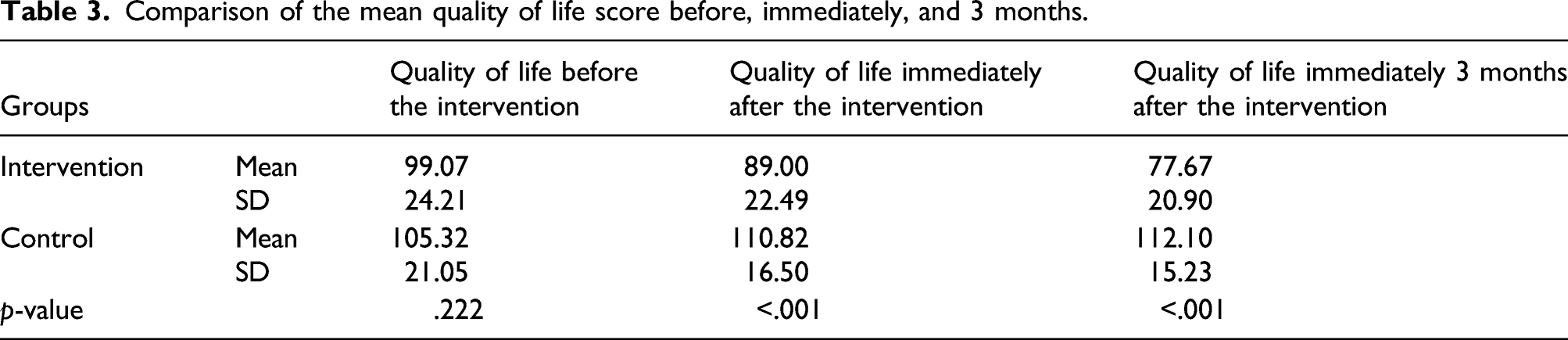
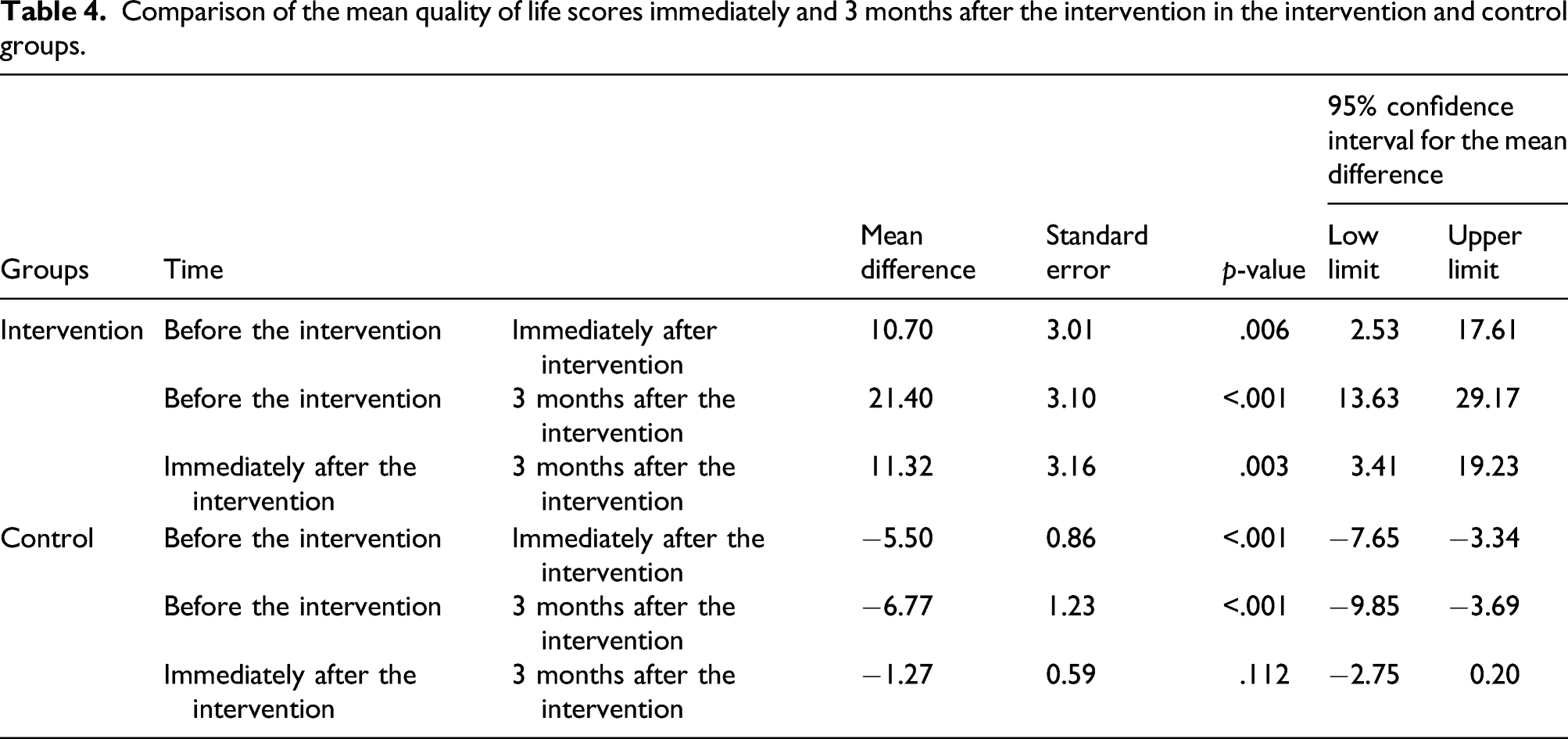
The effect of the intervention on the quality of life was investigated using the analysis of variance of repeated measures. The above-mentioned test showed a significant interaction between time and intervention (p < .001). Subsequently, the independent t-test was used to compare the mean score of quality of life before, immediately, and 3 months after the intervention in the intervention and control groups. Prior to the intervention, there was no significant difference between the two groups (p = .222). However, a significant difference was found between the two groups immediately (p < .001) and 3 months after the intervention (p < .001). Furthermore, Bonferroni’s pairwise comparison test was used to compare the mean score of quality of life before, immediately, and 3 months after the intervention. In the intervention group, a significant difference was found between the "before intervention" and "immediately after the intervention" measures (p = .006), while the "before" and 3 months after the intervention showed no significant differences.
Comparison of the mean quality of life score before, immediately, and 3 months.
Comparison of the mean quality of life scores immediately and 3 months after the intervention in the intervention and control groups.
The mean score of vasomotor, psychosocial, physical, and sexual domains of the women before the intervention was not significantly different in the intervention and control groups; however, after the intervention, a statistically significant difference was observed between the intervention and control groups regarding the mean score of all quality of life domains (p < .001).
Discussion
Menopausal symptoms usually have adverse effects on women’s quality of life. Menopause affects all aspects of a person’s health (i.e., vasomotor, psychosocial, physical, and sexual domains). The lower and higher scores of QoL during menopause indicate better and lower quality of life, respectively. Before the intervention, there was no significant difference between the intervention and control groups in terms of the mean score of quality of life. After the intervention, the mean score of quality of life in both the second and third measurements showed a significant difference between the intervention and control groups. In the control group, the mean scores of the second and third measurements revealed a significant increase, compared to the first measurement. In the intervention group, the second and third measurements were significantly reduced, compared to the first measurement; moreover, the third measurement was significantly reduced, compared to the second measurement.
In the studies conducted by Yazdkhasti et al. 17 , Farrokhi et al. 35 , Moridi et al. 36 , and Rathnayake et al. 37 , it was reported that educational intervention has improved the quality of life of postmenopausal women. 38 In the explanation of this finding in the present study, it can be stated that educational intervention by considering effective behaviors in adapting women to menopause, along with providing solutions, increasing knowledge, providing environmental facilities, creating social support, motivating, and creating behavioral confidence can play an important role in improving the quality of life of postmenopausal women. In general, based on the evidence, it can be concluded that in the present study, an educational intervention based on the MTM was effective in improving the quality of life of postmenopausal women (early postmenopausal stage). Given that women are the core of the family, they should benefit from menopausal care and education. Organized training and providing the necessary care of natural menopause are the least that can be offered early on and prior to progression and exacerbation of menopausal complications.
This study was performed on the postmenopausal women aged 45–55 years (early postmenopausal stage) in Yazd, Iran. It should be noted that the results may not be generalizable to all postmenopausal women. Therefore, there is a need for more extensive studies. The data were collected in a self-report format that might have affected the accuracy of the study results. Lack of studies by other researchers in the field of menopause and the use of the MTM were other limitations of the present study; accordingly, there is a need for further developments in this regard. Due to the fact that the follow-up (completion of the questionnaire 3 months after the intervention) was during the Coronavirus Disease 2019 outbreak, and people did not have the necessary cooperation to come to the intended place, the questionnaires were delivered to them at home, and again the next day it was collected from the doors of houses. Furthermore, due to the impatience of the majority of the women and the fact that postmenopausal women are in a period when they usually have various responsibilities (caring for grandchildren and doing housework), the number of face-to-face training sessions was limited. In this study, motivations were created for people to participate in the intervention using incentives, and plans to provide additional training using pamphlets and WhatsApp virtual group were made.
Conclusion
Since menopause is associated with negative effects on the quality of life of postmenopausal women, interventions to increase knowledge and training in the management of menopausal symptoms play an important role in improving the quality of life during this period. Based on the current study, it can be said that educational intervention based on the MTM has been effective in improving the quality of life of postmenopausal women. Given the good access of most postmenopausal women to health centers, it seems that the most effective solution is to keep menopausal caregivers up to date. It is also recommended that policy makers and healthcare centers provide facilities and training sessions on menopause with a health promotion approach for postmenopausal women, particularly at early stages.
Footnotes
Acknowledgements
The authors would like to thank the other investigators, the staff, and the participants of the study for their valuable contributions. The authors also acknowledge the research office of Shahid Sadoughi University of Medical Sciences, which financially supported this research and all of the individuals who participated in this study because of their valuable help. Torrens University Australia is also appreciated for the time and publication fees upon acceptance of manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study has been obtained by the ethics committee affiliated with Shahid Sadoughi University of Medical Sciences, Yazd, Iran (reference number IR.SSU.SPH.REC.1397.137) and date (02/02/2019). Registration of this randomized control trial has been completed with the Iranian Registry of Clinical Trials, IRCT20190206042640N1.
Guarantor
FH
Contributorship
NY and MaMsh with the support from MSh and FH were involved in the conception and design of the study. NY, SJ, NB, and MaMsh were responsible for the data acquisition. SJ performed the data analysis and interpretation. NY drafted the initial manuscript, and NY and FH did the necessary modifications for making the manuscript acceptable for publication. All authors revised the manuscript critically for intellectual content and approved the submitted version.