
Abstract

Introduction
Managing menopausal symptoms involves many different options, including both hormonal and non-hormonal interventions. Hormone replacement therapy (HRT) is the most effective treatment option available for women experiencing classical menopausal symptoms, such as vasomotor symptoms and sleep disturbance. If HRT is to be considered, this should be based on an individualised risk assessment. Decision-making around HRT prescribing can be challenging in women who have a complex medical history, including women with a history of a hormone-dependent cancer. An ever-increasing number of cancer survivors now live long enough to reach the natural age of menopause or they may experience menopausal symptoms earlier as a side effect of treatment (surgery, chemotherapy or radiotherapy).
When considering treatment options for menopausal symptoms, the oncologic risk of HRT – the potential to cause cancer recurrence and progression – is difficult to assess. Individualised decision-making is needed, but the evidence on which this should be based is not always clear. Collaboration with oncologists and surgeons is needed to ensure that long-term patient safety is not compromised for short-term symptom control.
Guidance published recently in a joint statement from the Royal College of Obstetricians and Gynaecologists (RCOG), the British Menopause Society (BMS) and the Society for Endocrinology provides an evidence base to help clinicians advising women experiencing symptoms of menopause. It is important that women have the right information and are supported by appropriate clinicians when making decisions about their treatment and care. 1 Alongside this, the National Institute for Health and Clinical Excellence (NICE) published helpful guidance that provides a framework for shared decision-making and advocates the use of clinical decision aids to support a collaborative approach between the clinician and the patient. 2
In these tales, two cases are presented, relating to women with a history of pelvic cancer (endometrial and bladder cancer). Both women presented for advice in relation to managing menopausal symptoms.
Case 1
A 59-year-old woman with a history of endometrial cancer, presented with symptoms of sleep disturbance, fatigue, hot flushes and joint pain. In addition, she described memory problems and low libido. She was otherwise fit and well with normal blood pressure but a slightly raised BMI, despite having a healthy lifestyle.
FIGO Staging of uterine corpus carcinoma and carcinosarcoma.
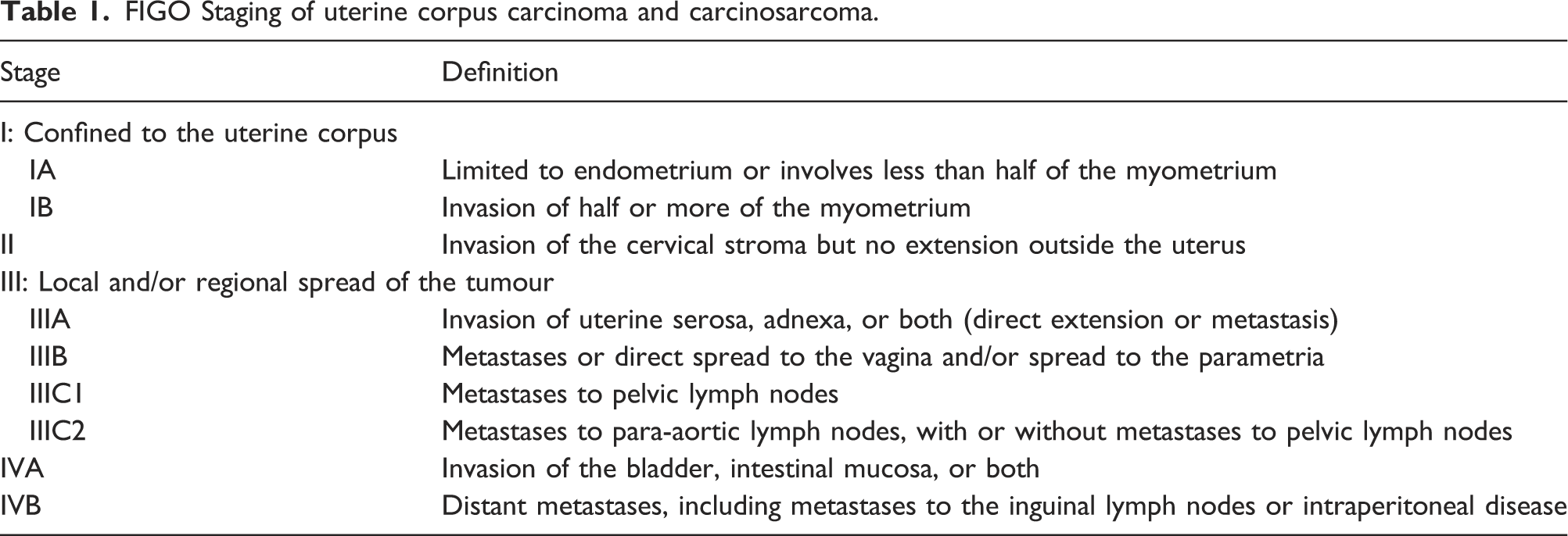
Having been disease-free for 5 years following surgery for a stage 1 endometrial cancer, the risk of recurrence for this patient was considered low and to manage her menopausal symptoms, including low libido, she was commenced on tibolone, a low dose gonadomimetic compound. This was used in preference to estrogen-only HRT to protect against stimulation of any potential endometrial tissue left in the peritoneal cavity following surgery and for the possible beneficial effect on sex drive without considering the use of estrogen transdermally and the possible addition of testosterone, out of product licence, in an NHS setting.
Endometrial cancer is the commonest gynaecological malignancy. It is the fourth most common cancer in females in the UK and the sixth most common female cancer worldwide, with more than 380,000 new cases diagnosed in 2018. 3 Incidence in the UK has increased by around 55% since the 1990s, with around 9400 women diagnosed per year in 2015–2017, leading to 2409 deaths in 2018. 4 The increase in incidence is thought to be due to rising obesity levels in the population. 5 Other risk factors are type II diabetes, hypertension and unopposed estrogen in conditions such as polycystic ovarian syndrome (PCOS) and estrogen-only HRT.
Endometrial cancer is estrogen-sensitive in 90% of cases (type I, endometrioid) and estrogen-independent in only 10% (type II, most commonly serous papillary carcinoma). The stage and grade and of the cancer are important when considering whether HRT is appropriate and safe. Although one could expect an increased recurrence rate after the initiation of HRT, the available evidence does not support this hypothesis. Studies mainly apply to early stage, low grade endometrioid endometrial cancer. There are no data to guide the use of HRT in advanced stage or high-grade endometrial cancers.
Several studies have found consistently that the recurrence rate and disease-free survival are not worse with HRT use, although studies were heterogeneous and various regimens were used. In most cases, survival rates were found to be better in HRT users compared to non-HRT users. The safety of exogenous estrogen-only HRT was not conclusively confirmed, but the absolute recurrence rates were very low. Continuous combined HRT does not appear to increase the risk of recurrence, but the marginal increased risk of breast cancer with the progestogen component, needs to be weighed against any benefit.
In most studies, HRT was initiated between one to 60 months following treatment and associated disease-free survival. No specific studies have been identified relating to HRT use in survivors of type II endometrial cancers, but as these are not sensitive to estrogen, it is reasonable to assume no increase in recurrence associated with HRT use.6–10
Case 2
A 58-year-old woman, with a history of radical treatment for bladder cancer 2 years earlier, presented with a 5-year history of symptoms of menopause. These included vasomotor symptoms, anxiety, palpitations, urogenital symptoms and low libido. She also complained of joint pain. Her symptoms had previously been well controlled on HRT, which was stopped at the time of her diagnosis.
She was prescribed Citalopram, 20 mg daily for anxiety and NSAIDs/Omeprazole for joint pain after stopping HRT. She was a lifelong non-smoker, with minimal alcohol consumption and was fit and well, despite having migraine, prior to her diagnosis of transitional carcinoma of the bladder in 2020. She was treated with chemotherapy and pelvic clearance with urostomy (her kidneys now drain urine through the ureters and into a small piece of ileum before draining out via a stoma). Histology confirmed high-grade carcinoma in situ (CIS). Further testing of the tissue demonstrated that it was estrogen-receptor positive with 1–2% potential increase in activity when exposed to estrogen, but not testosterone, in vitro.
She had a family history of endometrial cancer in her mother and stomach cancer in her father and a diagnosis of Lynch Syndrome was being explored.
She had started swimming again after her surgery, having built up confidence in managing her stoma. Despite this, she had a raised BMI at 38 and reported struggling with carbohydrate cravings. She monitored her blood pressure regularly and this remained within the normal range.
Some of the symptoms experienced were related to anxiety due to her cancer diagnosis and treatment, but others were thought to be related to the menopause as these had previously been relieved by HRT.
The patient’s primary concern was to manage the risk of recurrence of her cancer, and she was keen to avoid hormone therapy. She had already explored several non-hormonal treatment options. She was referred for cognitive behavioural therapy (CBT), which helped with her anxiety symptoms, and was taking an SSRI with a beneficial effect. She had tried gabapentin and pregabalin for night sweats but struggled with the side effects of both and was not keen to try them again. She came to the clinic to discuss whether there were any treatments which might relieve her symptoms.
Bladder cancer is a urothelial tumour and can affect any part of the urinary tract from the urethra to the renal pelvis. Five to ten percent of urothelial cancers occur in the upper urinary tract (ureters, renal pelvis and renal calyces). Bladder cancer is more common in men, but women tend to have more advanced disease at diagnosis and a poorer prognosis. The influence of hormones in relation to bladder cancer is generally not well recognised, although 12–18% of bladder cancers are estrogen-receptor (ER) positive and those ER-positive tumours tend to be more aggressive than ER-negative cancers. 11 Deli et al. (2020) 12 suggest that although no direct clinical evidence is available, extrapolation of available research findings suggests that HRT should be avoided in women with a history of bladder cancer
Treatment for bladder cancer includes local resection of low grade, non-invasive disease, Bacillus Calmette-Guerin (BCG) immunotherapy for higher grade disease and radical treatment in the form of cystectomy and urinary diversion for invasive disease and CIS carcinoma in situ. Women tend to be less sensitive to treatment with BCG immunotherapy compared to men. Women also have a poorer disease-free, cancer-specific overall survival after radical surgery. 14 Recurrent disease can occur in residual urothelial tissue in the ureters and renal pelvises/calyces, potentially requiring nephroureterectomy.
The available evidence in relation to bladder cancer and estrogen replacement therapy was discussed with the patient, including the potential benefits of treatment and the possible risks. The patient decided against hormone replacement therapy at the time of consultation, deciding that for her the possible increased risk of recurrence outweighed any potential benefits, due to the worry of a potential recurrence.
Discussion
The benefits associated with HRT for otherwise healthy symptomatic women outweigh any potential risk. However, for women with a history of cancer and other health issues, special consideration needs to be taken in relation to the oncologic safety of HRT and risk of recurrence.
Shared decision-making is defined by NICE as ‘a collaborative process that involves a person and their healthcare professional working together to reach a joint decision about care. It could be care the person needs straightaway or care in the future, for example, through advance care planning. It involves choosing tests and treatments based both on evidence and on the person’s individual preferences, beliefs and values. It means making sure the person understands the risks, benefits and possible consequences of different options through discussion and information sharing. This joint process empowers people to make decisions about the care that is right for them at that time (with the options of choosing to have no treatment or not changing what they are currently doing always included)’. 2
When sharing treatment options with women about management of menopausal symptoms, including the option of HRT, it is important to share the available evidence (or often lack of evidence) and to discuss this in the context of potential benefits, both in terms of symptom relief and in the potential to reduce the risk of osteoporosis and cardiovascular disease. Benefits need to be weighed carefully against the risks of new cancers and of disease recurrence in relation to existing cancers.
These tales highlight the diverse influence of hormones on cancer risk. Available evidence suggests that caution should be applied not only in breast cancer, but also in women with a history of bladder, liver, stomach cancer, meningiomas and gliomas. 13
For women who decide not to take HRT, symptom relief can be achieved with non-hormonal treatments, including CBT, SSRI’s, SNRIs, gabapentin and pregabalin. Newer medical therapies such as neurokinin 3 receptor antagonists offer options for the symptomatic relief of vasomotor symptoms and sleep disturbance in the future and are particularly relevant for women experiencing menopausal symptoms who have had a hormone-dependent cancer. 15
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.