
Abstract
Menopause is a state of estrogen deficiency that affects numerous estrogen-dependent tissues in the female body. Skin is one of the most affected organs. Many consider menopausal skin changes to be merely an aesthetic problem; however, they can significantly affect women’s quality of life. Currently, there are no approved effective treatments to prevent or alleviate skin changes associated with estrogen deficiency. Standard systemic hormone replacement therapy used to treat menopausal symptoms may be effective to some degree for skin treatment. In addition, compounded bioidentical hormone replacement therapy, selective estrogen receptor modulators, and phytoestrogens could also be used for skin treatment, although this is only hypothetical due to lack of data. Many questions therefore remain unanswered. On the other hand, topical, low-dose estrogen that would act only on the skin without systemic effects could be a possible option, as could be skin-only acting topical phytoestrogens. Such topical products without systemic effects could play a role in the treatment of menopausal skin. However, they are not currently approved because there is insufficient data on their safety and efficacy. A healthy lifestyle could have a positive effect on the menopausal skin. In this review, we provide an overview of the characteristics of menopausal skin, an outlook on the future treatment of menopausal skin with estrogens and other approaches, and the associated controversies and speculations. Overall, the importance of menopausal skin changes should not be neglected, and high-quality research is needed to gain new insights into the treatment of menopausal skin.
Introduction
Estrogen is a hormone that plays an important role in numerous physiological functions, including the regulation of the immune system, glucose and lipid metabolism, bone metabolism, brain function, reproduction, cardiovascular system, and skin.1–3 Three types of estrogen are found in the human body: 17β-estradiol, estrone, and estriol. 4 Although estrogen deficiency affects different tissues differently, skin changes, such as increased wrinkling and dryness, decreased elasticity, and impaired wound healing, are undoubtedly the most visible.5–7 In addition to estrogen deficiency, endogenous and exogenous skin aging also promote the progression of menopausal skin changes.6,8 Estrogen deficiency is associated with the decreased expression of estrogen receptors in skin cells. 8 Importantly, complete estrogen deficiency and the associated substantial reduction in estrogen receptors in the skin have deleterious effects that appear irreversible.5,8 Therefore, it can be assumed that appropriate timing and dosage of estrogen replacement could prevent significant depletion of estrogen receptors in the skin. Whether HRT treatment as early as perimenopause would prevent significant depletion of estrogen receptors in the skin remains to be thoroughly investigated. Undoubtedly, studies are needed to clarify this interesting question.
Characteristic skin changes associated with estrogen deficiency include thinner atrophic skin with less collagen, decreased elasticity with fewer elastin fibres, increased dryness due to decreased hyaluronic acid content, loss of water-binding mucopolysaccharides, wrinkling, pigmentary changes, impaired skin barrier, impaired wound healing, and decreased vascularity. 8 Taken together, these changes may be an important reason for lower self-esteem and significant reduction in the quality of life of postmenopausal women. This may contribute to psychological problems, such as depression and an unhealthy lifestyle, which in turn promotes the development of cardiovascular and metabolic disorders and other complications of menopause. 9 Therefore, the treatment of menopausal women requires a holistic approach that considers all potentially affected organs and focuses also on the skin.
Menopause
Menopause is defined as 1 year without menstrual bleeding in women aged 45 to 55 years, 4 although menopause may occur abruptly and earlier after ovariectomy. Due to increased life expectancy, the period of time during which women are menopausal has lengthened considerably so that menopause is receiving increasing attention in various respects. Menopause is caused by ovarian follicles that do not produce sufficient estrogen to stimulate endometrial growth due to minimal ovarian biosynthesis of estrogen. 5 After menopause, the main source of estrogen is the peripheral conversion of androgens secreted by the ovarian stroma and adrenal glands.10,11 Menopause is associated with several health problems including increased cardiovascular morbidity, metabolic disorders, osteoporosis, and decreased cognitive function.12,13 Menopausal skin lesions are often neglected in the face of these important health problems, 13 although they can substantially decrease the quality of life of postmenopausal women.
Estrogen and skin
Estrogen plays an important role in regulating skin morphology and function. Estrogen receptors in the skin have been found in keratinocytes, melanocytes, fibroblasts, Langerhans cells, hair follicles, and sebaceous glands. 14 In addition, keratinocytes, melanocytes, and fibroblasts can synthesize estrogen.15–17 Estrogen indirectly increases the levels of collagen types I and III, elastin, glycosaminoglycans, and the structural protein ezrin, which is involved in maintaining skin barrier integrity.4,18 Thus, estrogen in the skin affects skin thickness, elasticity, hydration, smoothness, barrier function, wound healing, and vascularization. 19
There are two types of estrogen receptors (ER), ERα and ERβ, which belong to the nuclear receptor superfamily. 20 They differ in their expression in various tissues. ERβ are highly expressed in the skin and dermal structures,15,17,20 whereas ERα are highly expressed in the female reproductive organs.20,21 ERα activation play an important role in breast and prostate cancer.5,22
Activation of ERβ is responsible for the beneficial effects of estrogen on skin structure and function. 23 Therefore, ERβ are a potential therapeutic target for the treatment of menopausal skin; moreover, ERβ represent a potential target for the prevention and treatment of photoaging, which is common and worsens during menopause. 24 Thus, the maintenance and activation of ERβ during menopause appear to be an effective and safe approach for the treatment of estrogen-deficient skin. The molecular pathways downstream of ER have not been extensively studied but may reveal new treatment options for menopausal skin in the future.
Estrogen deficient skin
There are three underlying causes of menopausal skin changes, which are distinct but also overlap to some extent: (i) decreased expression of estrogen receptors in the skin, (ii) decreased estrogen levels due to decreased synthesis by the ovaries, and (iii) decreased estrogen synthesis locally in the skin.20,25,26
Interestingly, a decrease in skin thickness and collagen content during menopause has been shown to be accompanied by a decrease in bone mineral density, highlighting the complexity and interrelatedness of menopausal changes in different tissues. This relationship is particularly evident in the early menopausal phase. 14 During the first 4 years of menopause, collagen synthesis decreases by 30%. 27 Thereafter, the loss of skin collagen and decrease in skin thickness are almost linear, with annual rates of 2.1% and 1.13%, respectively. 27 Immunohistochemical staining of skin biopsy specimens and computerized image analysis revealed lower amounts of collagen type I and III and a lower ratio of type III/I collagen compared to premenopausal women. 28
Other features of estrogen-deficient skin include decreased elastin and hyaluronic acid levels. This results in thinner skin, decreased elasticity, reduced tone, decreased resilience, volume loss, wrinkles, dryness, pigmentary changes, and impaired wound healing.8,20 Therefore, dermal fillers containing collagen and hyaluronic acid are commonly used to correct volume loss in altered facial contours. 19 However, an approach that preserves endogenous collagen, elastin, and hyaluronic acid would be a more psychological approach, with more favourable aesthetic and functional outcomes. Such an approach would lead to more natural and physiological results, and skin structures could be preserved over the long term.
Interplay between estrogen deficiency and skin aging
Skin aging occurs at different rates due to genetic, environmental, and hormonal factors. Skin aging involves both intrinsic and extrinsic components. The skin serves as a protective barrier and is influenced by numerous exogenous and endogenous factors. 29 Exogenous factors include environmental factors such as air pollution, sun exposure, and smoking. Endogenous factors include cellular aging, mitochondrial DNA mutations, oxidative stress, telomere shortening, genetic mutations, and decreased levels of various hormones including estrogen. 30 Both intrinsic and extrinsic factors lead to the dysfunction of keratinocytes, fibroblasts, melanocytes, and other skin structures such as hair follicles. 29 Intrinsic skin aging is thought to result in fine lines, whereas extrinsic skin aging results in deep wrinkles and hyperpigmentation due to sun exposure. 31 Skin aging also leads to decreased and impaired microcirculation, which in turn leads to decreased vascularization of the skin. 32
Thus, there is a functional overlap between the aging process and estrogen deficiency, affecting the same cells. It appears that both processes may accelerate each other, leading to an estrogen deficiency-aging loop (Figure 1). As mentioned earlier, aging is accelerated by extrinsic and intrinsic factors in addition to estrogen deficiency. However, a healthy lifestyle and preventive measures, such as sun protection and regular skin care, can help mitigate the effects of aging, while hormone replacement therapy can correct estrogen deficiency. All factors described in Figure 1 contribute to the individually varying rates of skin aging observed during menopause. Estrogen deficiency-aging loop with accelerators (extrinsic and intrinsic factors) and possible interventions (hormone replacement therapy and healthy lifestyle).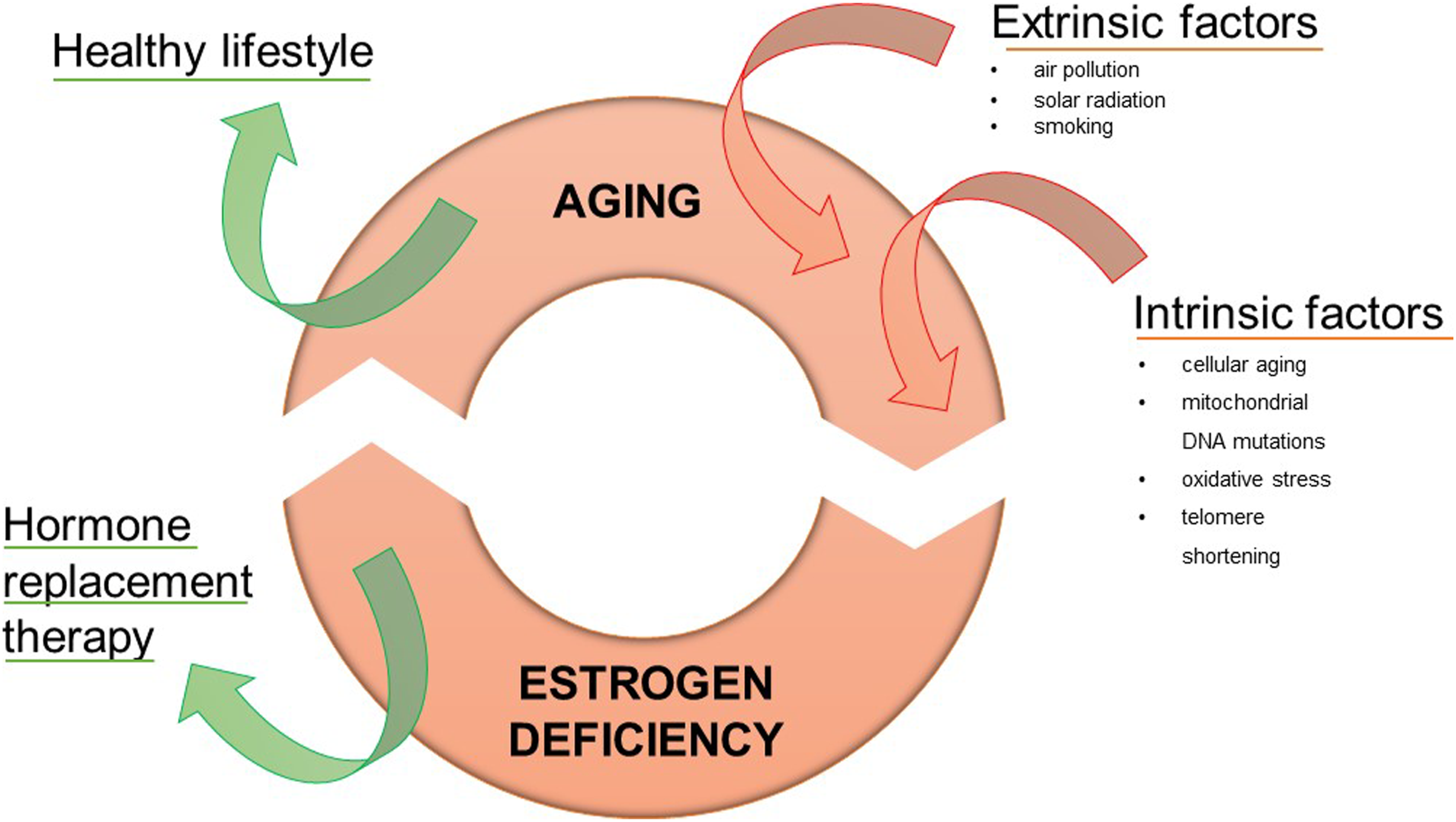
The link between menopausal estrogen deficiency and skin aging is further supported by the discovery of ER expression in mitochondria. Estrogen plays an important role in regulating cellular bioenergetics and counteracts oxidative stress, which are both negatively affected by menopause and are one of the culprit molecular mechanisms of aging.33–35 In addition, estrogen has been shown to possess potent antioxidant properties, as supported by animal and in vitro studies.36,37 By counteracting oxidative stress, estrogen protects dermal fibroblasts and keratinocytes from oxidative damage in vivo and maintains normal collagen synthesis and cell proliferation. 37
Furthermore, estrogen deficiency is associated with cellular senescence, one of the basic mechanisms in skin aging. 38 In aging skin, senescent cells accumulate throughout the epidermis and dermis, where they severely damage the extracellular matrix, cellular DNA, proteins, and lipids, reduce collagen production, and alter the skin architecture. 37 In vitro and in vivo studies have shown that estrogen replacement has a direct anti-senescent effect. 39 Estrogen deficiency appears to contribute significantly to the complex process of aging, including skin aging. 8
Overall, estrogen deficiency and menopausal aging are closely linked, setting a downward spiral in motion that leads to irreversible skin changes. However, several in vitro and animal studies have shown that these deleterious mechanisms can be partially prevented or even reversed by estrogen replacement therapy.40,41
Treatment of estrogen deficient skin
There are several options for the treatment of estrogen-deficient skin, with either systemically or locally acting treatments, or other estrogen-independent approaches (Figure 2). Importantly, there are currently few well-designed studies on the efficacy of these approaches. In addition, the appropriate approach may be individualized and not applicable to everyone. Schematic presentation of possible therapeutic options for menopausal skin. The options can be combined. HRT – hormone replacement therapy, cBHRT – compounded bioidentical hormone replacement therapy, SERMs – selective estrogen receptor modulators.
Hormone replacement therapy (HRT)
HRT is the most effective treatment for menopausal symptoms. 42 HRT consists of estrogen (17β-estradiol in Europe or conjugated equine estrogen (CEE) in the United States) and progestogen in patients with an intact uterus, whereas it consists of estrogen alone in women who have undergone hysterectomy. 42 HRT is used not only to relieve menopausal symptoms, such as vasomotor symptoms, depression, mood swings, lower sexual desire and libido, vulvovaginal atrophy, and musculoskeletal effects, but also to prevent age-related diseases such as osteoporosis and cardiovascular disease.42,43 However, some possible side effects, such as increased incidence of venous thromboembolism (not associated with transdermal HRT), coronary heart disease (possible if started in women over 60 years of age or with pre-existing coronary heart disease), breast cancer, and stroke (possible if oral HRT is started in women over 60 years of age), have also been associated with HRT.42,43 Evidence from large observational studies confirms the safety of HRT when used appropriately, and the benefits and risks are carefully weighed in each patient. Therefore, the guidelines recommend starting HRT before age 60 or within 10 years of menopause.42,43
The use of HRT has been shown to improve skin thickness, dermal collagen, 44 elastin fibres, 45 and dermal hyaluronic acid content. 46 Undoubtedly, there is a lack of studies, especially those with appropriate designs; therefore, there are no firm evidence-based data. In a randomized, double-blind, placebo-controlled trial, 1 year of oral estrogen therapy in menopausal women was shown to increase skin thickness by 30%, 47 whereas 6 months of treatment with oral estrogen increased skin collagen by 6.5%. 48 Increase of skin collagen was also confirmed by others. 49 Interestingly, another study found no difference in skin thickness or collagen content after oral estrogen therapy. 50 Importantly, this may be due to only a short period of estrogen deprivation (median time after menopause 12 months). Some authors believe that the increase in collagen content of the skin in response to estrogen therapy is related to the initial collagen content. 51 HRT has also been shown to improve skin hydration when estrogen is administered systemically or topically. 52 In addition, hyaluronic acid and mucopolysaccharide content in the skin is increased by HRT. 53
Hormone replacement therapy and others
Topical, low-dose estrogen that acts only on the skin without systemic effects could also increase skin collagen content. 8 The weakness of topical, low-dose estrogen that would act only on the skin would be its limited effect, restricted only to the area to which the estrogen would be directly applied. However, to date, topical estrogen is only approved to be used as HRT. The effect of topical, low-dose estrogen on menopausal skin has been investigated in several studies summarized by Rzepecki et al. 5 They identified 23 studies that examined the effect of topical estrogen. The large heterogeneity of the studies does not allow any clear conclusions to be drawn. The studies differed in terms of study design, method of topical estrogen application, concentration of topical estrogen product, concurrent administration of systemic therapy, skin region studied, study duration, and the presence and type of a control group. In addition, the different studies examined different and not always similar skin characteristics. 5 Although most of the studies reviewed reported that there were no systemic effects after topical skin application of low dose estrogen, some studies reported also systemic effects. Because it is not yet clear whether topical application of low dose estrogen can potentially lead to adverse systemic effects, topical low-dose estrogens are still not approved for treatment of menopausal skin. 5 In addition, although positive results have been reported, the criteria for adequate evidence-based studies have not been met. Therefore, many questions remain unanswered that will need to be addressed in future studies.
However, there are also studies showing no effects of estrogen on menopausal skin. Oral and transdermal estrogen were compared in a randomized, placebo-controlled trial that found no effects on skin wrinkles or stiffness in most facial areas. 54 The incidence of adverse systemic effects was low and comparable to that in the control group. 54 Treatment lasted 4 years, and the study enrolled women aged 42 to 58 years who were enrolled in the study within 36 months of their last menstrual period. Patient selection and treatment duration may influence results. 54 In addition, various skin characteristics, such as thickness, elasticity, wrinkles, firmness, hydration, and vascularization, may be differentially affected by systemic or local estrogen replacement. Overall, numerous issues related to systemically or locally acting estrogen treatment of menopausal skin should be clarified to provide reliable information to physicians and menopausal women.
Compounded bioidentical hormone replacement therapy
Compounded bioidentical hormone replacement therapy (cBHRT) consists of chemical substances with the same molecular structure as human hormones. cBHRT refers to individually formulated hormone preparations that are specifically tailored to the individual. These formulations may contain different doses of estrogen, progesterone, and testosterone.55, 42 cBHRT are not recommended by menopausal and endocrine societies because they are not properly regulated and have not been adequately tested for efficacy and safety.42,55,56 Regarding menopausal skin treatment, although some small studies have found that cBHRT can increase skin hydration and reduce skin atrophy, 57 no large appropriately designed studies have yet been conducted.
Selective estrogen receptor modulators
Selective estrogen receptor modulators (SERMs) are compounds that bind to the ER and act as agonists or antagonists. They are used in the treatment of estrogen-responsive target tissues such as the breast, bone, vagina, endometrium, and brain. 58 SERMs are approved for the treatment of osteoporosis, vasomotor symptoms, genitourinary syndrome, infertility, and breast cancer. 59 However, their effects on the skin have not been fully elucidated. In vitro studies have shown that raloxifene increases skin collagen synthesis, 60 whereas in vivo studies have shown improved skin elasticity. 61 Current data suggest that the use of SERMs may preserve the beneficial effects of estrogen, while avoiding the potentially harmful effects of systemic hormone therapy.62,63
SERMs might be developed in the topical form for the menopausal skin in the future. 4 Nevertheless, further studies are needed to determine the specific effects of SERMs on the menopausal skin.
Phytoestrogens
Phytoestrogens are estrogen-like substances produced by plants. Phytoestrogens bind directly to the ER and exert mixed agonistic and antagonistic effects. They consist of three main groups: isoflavones, lignans, and coumestans. 62 Compared to estrogens, the effects of phytoestrogens are weaker, and they are not stored in tissues. 20 Because of this weak effect, the risk of hormone-related cancers is thought to be low or non-existent. 62 Phytoestrogens intended for the treatment of menopausal skin are available in oral or topical form.4,64,65 Studies have shown that topical isoflavones have positive effects on skin aging, including improved elasticity, wrinkling, and hydration.59,66 Therefore, they are already used in cosmetic products and could represent a promising option for the prevention of skin aging.4,64 However, in studies comparing topical isoflavones with topical estrogen, estrogen was superior, resulting in greater improvements in skin characteristics.66,67 Nevertheless, more research is needed to fully clarify and understand the role of phytoestrogens in the treatment of menopausal skin. 68
Non-hormonal options
Non-hormonal options for the treatment of menopausal skin aging include oral and topical products. Many menopausal women take oral supplements such as antioxidants (vitamins C, E, and B7 (biotin), coenzyme Q10, selenium, polyphenols, and flavonoids) to alleviate skin aging.66,67 Some of these agents are often formulated as topical cosmetic products that are said to have promising effects on skin aging. However, there is limited data on whether these agents improve skin aging and/or menopausal skin changes. Other agents, such as hyaluronic acid, retinol (or prescribed forms of retinoids), and alpha hydroxy acids, in topical form are also commonly used to affect skin aging. 69
Recently, a new target to prevent structural and functional deterioration of aging skin has become hallmark mechanism of aging. Senescent cells, which have lost their ability to divide, steadily accumulate in the aged skin. They have harmful effects, as they secrete inflammatory cytokines, immunomodulators, growth factors, and proteases. 68 Therefore, senotherapeutics, a class of agents that act on senescent cells, are of particular interest as potential therapeutic options. 70 Of particular interest are flavonoids with senolytic activity, such as fisetin and quercetin, and polyamines, such as spermidin, either in topical form or in combined topical and oral forms. Therefore, further studies are required. Accumulation of oxidative stress is another feature of skin aging. 71 Antioxidants from the thiol group, such as methionine and cysteine, have rarely been used to treat skin aging, although they may have a greater potential than standard antioxidants. 72 In any case, several antioxidants are of interest for topical or combined topical and systemic applications. Furthermore, sirtuins, proteins that play a key role in the cellular response to various age-related stressors such as oxidative and genotoxic stress and estrogen deficiency, 73 may also be attractive targets. Sirtuins are reduced in aged and estrogen-deficient skin. 74 Among the various compounds that activate sirtuins, resveratrol is most used. Numerous other sirtuin activators are currently being investigated. As for treatment targeting the aging mechanism described above, it is probably appropriate that treatment be individualized. The biomarkers that might guide treatment are currently unknown.
The next possible target could be impairment of skin vascularization during menopause. Estrogen regulates endothelial function through its receptors on the vascular wall and activates nitric oxide (NO).
75
The NO controls vascular tone, ensures the integrity of the endothelial barrier, and has important anti-inflammatory, antioxidant, and antiproliferative functions.
76
Therefore, endothelial dysfunction occurs during menopause and may be involved in skin changes in addition to atherosclerosis.
76
Approaches to improve endothelial dysfunction may be beneficial for menopausal skin. Topically applied
Healthy lifestyle
During menopause, a healthy lifestyle can help relieve symptoms and promote overall well-being. Regular physical activity, such as aerobic exercise and strength training, can help control weight and improve cardiovascular health. 78 A balanced diet rich in fruits, vegetables, whole grains, lean protein, and fibres can provide essential nutrients and support hormonal balance.78,79 In addition, abstaining from smoking and excessive alcohol consumption may help reduce the risk of certain health conditions associated with menopause, such as cardiovascular disease and osteoporosis. 80 Furthermore, social contact and engaging in stress-reducing activities such as yoga or meditation can help manage mood swings and promote mental well-being. 80 Healthy lifestyle habits incorporated during the premenopausal period can mitigate many of the harmful effects of menopause. 81 There are no specific data on skin changes during menopause, but it seems plausible that a healthy lifestyle, throughout life, and especially in the premenopausal and menopausal period, has beneficial effects on the skin. A healthy lifestyle in relation to the skin also includes regular skin care, including cleansing, rehydrating the skin, and protecting the skin from UV radiation. 82
Controversies and speculations
The first controversy is that skin problems are largely neglected by physicians compared with other symptoms and consequences of menopause. The reason for this is probably that menopausal skin problems are generally considered aesthetic rather than medical problem. The opposite is true. Therefore, we believe that there should be a call to action to address skin problems in a similar way to other menopause-related health problems.
The second unresolved issue that gives rise to controversy and speculation is related to the lack of data on the effects of estrogen on menopausal skin. The factors that influence the beneficial effects of estrogen in HRT have not yet been studied. It may be that the introduction of HRT at perimenopause is the best time to affect menopausal skin changes, but this assumption remains to be clarified. Overall, it is still unclear when is the best time to start HRT for potential skin benefits.
Moreover, which skin feature, apart from collagen content, is affected by estrogen is also not yet clear. Whether and to what extent late introduction of HRT after the onset of menopause is still effective is questionable. Topical low-dose, skin-only acting estrogen could be a good alternative to systemically acting estrogen. However, the data is sparse. It would be informative to know if systemic and topical low-dose, skin-only acting estrogen (especially in the facial skin) is more effective than either treatment alone. Therefore, well-designed studies are required.
Third, the possible dose-response relationship between estrogen and its effects on the skin has not yet been investigated. As with all biological processes, where there is a substance-activity relationship, this would be very informative. This is particularly important for the still insufficiently studied topical low-dose, skin-only acting estrogen that would act only on the skin, where, in addition to the possible beneficial effects on the skin, the potential adverse effects of possible systemic absorption of estrogen should also be considered. Treatment with topical low-dose skin-only acting estrogen is currently not yet approved due to insufficient data.
Fourth, the duration of systemically estrogen administration required to achieve skin improvement remains unclear. It would be informative to know the relationship between systemic treatment duration and skin effects. In addition, estrogen resistance may develop over time. Many drug treatments have been associated with the development of resistance over time. The similar might apply for topical low-dose, skin-only acting estrogen. If so, intermittent or cyclic treatment with topical low-dose, skin-only acting estrogen might be more effective and safer than continuous treatment. Cyclic treatment with locally acting estrogen might be likely to result in better adherence to therapy in menopausal women.
Fifth, it is not yet known whether and to what extent HRT would provide more skin benefits than cBHRT, SERMs, and phytoestrogens. In addition, it would be very informative to compare topical low-dose, skin-only acting estrogen and topical phytoestrogens. To date, no such study exists because such topical preparations are not approved due to safety and efficacy concerns.
Nevertheless, combining HRT with topical phytoestrogens appears to be an interesting approach. Although several uncritical claims related to non-HRT hormonal treatment have been scientifically rejected, this therapy might play a role in the treatment of menopausal skin. However, this should be tested in appropriate studies.
Sixth, it is not known whether treatment targeting the molecular features and pillars of the aging process would be beneficial for menopausal skin. As estrogen deficiency and skin aging form a pathological vicious circle, this speculation seems plausible. Antioxidants, senolytics, sirtuin activators, and other molecules with anti-aging properties may be effective.
Seventh, the highly speculative idea of targeting the decreased vascularization of the skin during menopause deserves some attention. Approaches to improve the endothelium by increasing the expression of the downstream molecule of estrogen, NO, could be beneficial. To date, no studies have investigated this hypothesis.
Eight, whether individualized treatment would be more appropriate than a general ‘one size fits all’ solution has not yet been addressed. Numerous factors could influence the outcome of the various mentioned skin treatments. However, there are no known biomarkers or other criteria that would guide treatment. Overall, biomarkers are needed that reflect the structural and functional characteristics of menopausal skin and would change in parallel with the skin in response to treatment.
Ninth, the effect of healthy lifestyle habits on menopausal skin deserves a well-designed study. A healthy lifestyle affects, at least in part, all the possible intervention targets for menopausal skin. Quantitative measurements, dose dependence, and the role of specific interventions are important. Such research should be included in a comprehensive study of healthy life benefits across multiple functions and tissues during menopause.
Finally, the possible safety issues should be considered. Since melanocytes respond to estrogen stimulation, HRT may hypothetically increase the risk of melanoma. However, to date, there is no convincing evidence for an association between exogenous hormone therapy (oral contraception, fertility treatment, or hormone therapy) and an increased incidence of melanoma. 83 Nevertheless, the relevant real-world data should be continuously monitored.
Overall, several questions remain unanswered and there are numerous controversies and speculations. We have listed some of them. Hopefully, these questions will be explored soon and will lead to progress in the treatment of estrogen-deficient skin.
Future perspectives
As described in this article, several well-designed studies should be conducted to address the most important questions regarding menopausal skin. Ideally, this would lead to the development of effective and safe treatments. This would on one side address estrogen deficiency and, on the other hand, target estrogen receptors in the skin and prevent their decreased expression due to declining estrogen levels. In addition, treatment should aim to prevent a decrease in local estrogen production. Other potential non-hormonal activators of estrogen receptors in the skin of menopausal women need to be investigated, as well as estrogen downstream molecules. Furthermore, ‘anti-aging’ substances, including antioxidants, senotherapeutics, and drugs, that activate sirtuins seem to be beneficial since aging skin and estrogen-deficient skin are tightly connected. Furthermore, investigation of new approaches and ideas, such as improving vascularization, which is reduced by estrogen deficiency, should be encouraged.
Conclusion
Menopausal skin problems are far more than just an aesthetic problem. Effective treatment and management strategies to prevent or alleviate skin changes associated with estrogen deficiency have not yet been established. In addition, the effects of HRT on the skin have not been fully explored. We reviewed major controversies and speculations related to the treatment of menopausal skin, which remain to be addressed and clarified. Such approaches would shed new light on menopausal skin. New high-quality data from well-designed studies are needed.
Practice points
• The skin is an estrogen-dependent tissue affected by estrogen deficiency states such as menopause. • The menopausal skin is not currently adequately addressed, although it has important implications for menopausal women. This issue should be considered like other menopausal health problems. • There is a lack of high-quality data on the efficacy and safety of various non-hormonal and hormonal treatment options, including HRT, for menopausal skin. New studies are urgently needed. • There is much controversy and speculation about the treatment of menopausal skin that needs a proper response. • Skin aging and estrogen deficiency are closely related processes that form a harmful vicious circle. • Despite this high demand, there are no approved effective treatments to prevent or alleviate menopausal skin problems. • In the absence of sufficient data, women should be encouraged to take preventive measures, such as a healthy lifestyle, sun protection, and proper skin care.
Footnotes
Contributorship
EKMŠ reviewed the literature and wrote the initial manuscript. TK and IZ reviewed the literature and completed the manuscript. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
EKMŠ.