
Abstract
Introduction
Infantile hypertrophic pyloric stenosis (IHPS) is a common surgical condition, but there are no guidelines regarding preoperative fluid resuscitation. Our aim was to evaluate a novel consensus care pathway for IHPS, incorporating a standardized fluid and electrolyte replacement regime.
Methods
One hundred patients were initially reviewed and compared to thirty-three patients following the introduction of a clinical pathway, whereby infants requiring electrolyte correction received 150 ml/kg/24 h of 0.45% saline, 5% dextrose and 10 mmol KCl, with systematic blood sampling until correction was achieved. We measured time to electrolyte correction, time to surgery and total length of hospitalization. Data were described using the median and interquartile range, and differences between the groups’ categorical and continuous data were described using Chi-squared and the Mann–Whitney U–tests, respectively.
Results
Time in hours taken to correct electrolytes was reduced: 25(16.5–42) versus 9.5(4.5–24.75) p = 0.004. Time to surgery from admission in uncorrected patients decreased from 50(40.25–66.75) to 39(28.75–41.75) p = 0.018. Subsequently, there was a reduction in total length of stay: 94(71–93.5) versus 75(64.5–93.5) p = 0.025. Parental satisfaction increased from 77% in the pre-pathway group to 83% in the pathway group.
Conclusion
A consensus care pathway for IHPS reduces the time taken to correct preoperative electrolyte abnormalities, decreases length of hospitalization and improves parental satisfaction.
Keywords
Introduction
Infantile hypertrophic pyloric stenosis (IHPS) is one of the most common surgical presentations in infants, typically presenting between 2 and 12 weeks of age, with an incidence of 2–4/1000 live births.1,2 Because it was first reported by Ramstedt more than 100 years ago, 3 almost all cases have been managed surgically with a pyloromyotomy, either performed through an open incision or laparoscopically. 4 Clinical outcomes are now widely accepted to be excellent. 5 However, these infants may be initially significantly dehydrated and classically, but not universally, present with a profound metabolic alkalosis requiring time to correct.6,7 This can be a lengthy process and represent a source of much anxiety for families as they wait for their child to undergo surgery.
Currently, there are no widely accepted guidelines to inform the choice of fluid and electrolyte replacement therapy for these infants, consequently significant variation in practice between units exists. 5 The pre-operative period is distressing for families and staff, due in part to the necessity for the infant to remain nil by mouth during the administration of intravenous fluids to correct dehydration and alkalosis. Therefore, our aim was to evaluate the effects of a standardized fluid resuscitation and electrolyte replacement regime within the context of a clinical care pathway for IHPS, with the goals of reducing length of stay and ultimately improving parental satisfaction.
This study addresses the following hypothesis: The implementation and use of a structured care pathway for IHPS reduces length of stay in hospital and increases parental satisfaction.
Methods
Study design
The study was designed as an observational, pre- and post-intervention comparison, with the consensus care pathway for IHPS being the intervention.
The pre-pathway cohort (Group 1), comprised 100 retrospectively identified patients undergoing pyloromyotomy over an eight-month period at a single tertiary referral centre. In this group, pre-operative intravenous fluid and electrolyte replacement therapies had been administered according to individual clinician preference.
The second group was a cohort of 33 patients, (Group 2), who were prospectively analysed over a 3-month period, 12 months following the implementation of the care pathway. All of the infants in this second cohort were managed as per the pathway.
Development of consensus guidelines and care pathway
A committee of surgeons, anaesthetists, nurses and parents were assembled to discuss the current standard of care delivered to infants with IHPS in our unit. The results from Group 1 highlighted potential areas for improvement within the pre-operative management of these infants. Guidelines were subsequently produced following thorough discussion within the consensus committee and approval from the Hospital Review Board. These guidelines were then incorporated into a clinical care pathway for IHPS, which was piloted for three months. Following this, a further consensus meeting was held, and permission was granted by the reviewing committee for the care pathway to be used to standardize care provided to these infants. A ‘bedding-in’ period of 12 months was then utilized prior to data being collected from Group 2.
Pre-operative fluid and electrolyte management
Children in both cohorts had capillary blood gases (CBG) and serum urea and electrolytes (U&E) analyzed on admission, and were stratified into two groups: those who had normal CBG and U&E 8 (corrected), and those who had metabolic alkalosis (uncorrected).
Children in Group 2 then had their treatment standardized according to the pathway protocol, depending on whether their CBG and U&E were corrected or uncorrected.
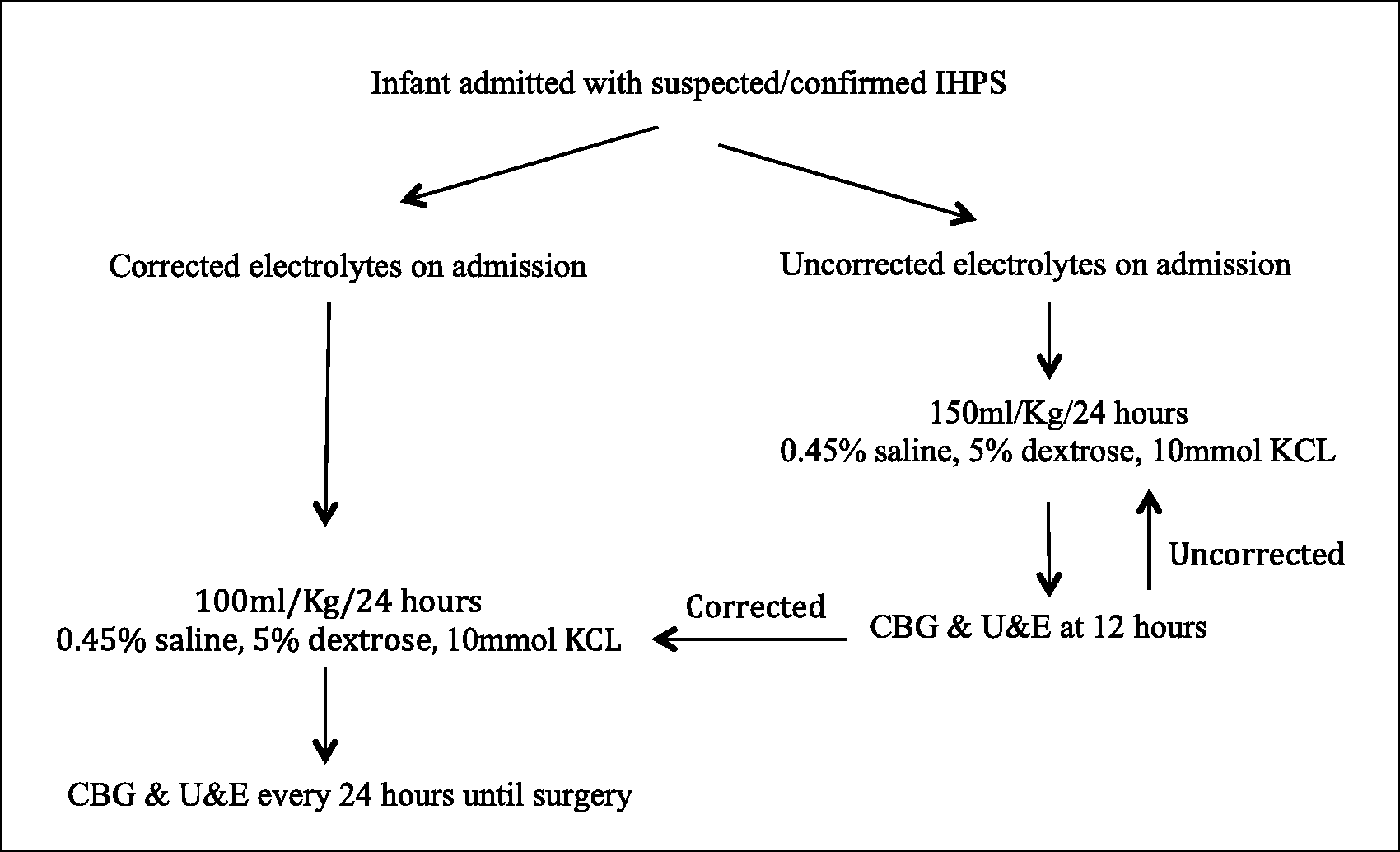
The care pathway guideline fluid regime was
corrected: 0.45% saline, 5% dextrose and 10 mmol potassium chloride (KCl) at the rate of 100 ml/kg/24 h. uncorrected: 0.45% saline, 5% dextrose and 10 mmol KCl at the rate of 150 ml/Kg/24 h.
The care pathway guideline blood sampling regime was
corrected: repeat blood sampling every 24 h, if required, prior to surgery. uncorrected: repeat blood sampling every 12 h until correction was achieved (Figure 1). Infants with initial substantial electrolyte derangement also had repeat CBG and U&E 6 h post admission. Infants with haemolysed blood samples underwent repeat blood sampling as soon as possible to obtain a true result. Patients in the post-pathway group (Group 2), received the standardized fluid replacement and monitoring regimes contained within the care pathway, as appropriate for their biochemical status on admission to our unit.
Every child had CBG and U&E taken at approximately 07:00 h on the morning of planned surgery. All infants were listed on the emergency operating list only once any alkalosis was corrected and parental consent had been obtained. The clinical care pathway contained removable parent/guardian information leaflets and pre-printed consent forms. All infants from both cohorts underwent open pyloromyotomy via a supraumbilical incision. Areas in the care pathway were made available for tick-box style recording of operation notes and post-operative instructions. In addition, it was agreed that eligible infants for pyloromyotomy would be operated upon between 08:00 h and 22:00 h in the presence of a consultant paediatric anaesthetist.
No changes were made to the initiation of postoperative feeding, whereby infants in both groups were either commenced on the post-pyloromyotomy feeding regime used by most consultants in our unit, or put to the breast depending on parent preference.
Pathway compliance
One hundred percent compliance was observed with the clinical care pathway and the peri-operative fluid and electrolyte management guidelines contained therein. 100% of infants had radiologically confirmed IHPS prior to proceeding to theatre. Sixty-seven percent received a senior surgical review from an ST3 trainee 9 or above within 4 h of admission and 100% had post-operative instructions for feeding for the nursing staff. Pathway compliance was defined as the appropriate use of the clinical care pathway, i.e for each consecutive infant admitted with a diagnosis of IHPS, a care pathway was completed and the guidelines followed appropriately.
Data collection
The hospital computer administration system, medical and nursing notes were all consulted to obtain the information required. Time of presentation, time to electrolyte correction, time to surgery, time to discharge and total length of hospitalization were all recorded. The primary outcome measure for this study was total length of stay. Secondary outcome measures assessed individual aspects of pre- and post-operative management, in addition to parental satisfaction with the service they had received.
The parental satisfaction questionnaire used in this study was designed and developed specifically for parents of infants with IHPS. It comprised a series of 10 questions relating to various aspects of care for infants with IHPS and individual parental views on their overall satisfaction with care received. The questionnaires were given to parents or carers once their child was ready for discharge from the unit. Parents were allowed to complete the survey in private and then instructed to place their answers in a blank envelope, which they left at the cot-side upon their departure from the unit. For each question, answers were recorded as
1. poorly satisfied, 2. somewhat satisfied, 3. neutral, 4. very satisfied and 5. excellent care received.
These data were then analyzed objectively by the authors such that a score of four or five was taken to indicate that parents were satisfied with that aspect of care. Answers scoring a one, two or three were regarded as not satisfied. Unanswered questions were excluded from both numerator and denominator data.
Statistical analysis
Data are described using the median and interquartile range (IQR), unless otherwise stipulated. Differences between the groups’ categorical and continuous data were described using chi-squared and the Mann–Whitney U–tests, respectively using IBM SPSS version 20. p ≤ 0.05 was considered statistically significant. Additionally, a post-hoc power calculation was performed.
Data sets derived from the parental satisfaction questionnaires were analyzed descriptively.
Results
Patient demographics: There was no statistical difference in age between the pre- and post-pathway groups.
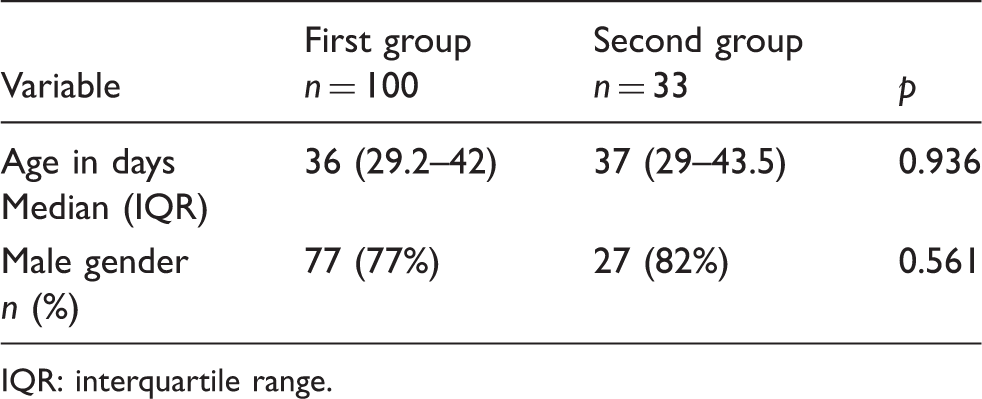
IQR: interquartile range.
Power calculation
A post-hoc power calculation was performed and revealed an acceptable power of 80.8%.
Primary outcome
Primary and secondary outcome results.

IQR: interquartile range.
Secondary outcomes
Secondary outcomes evaluated individual aspects of the pre-operative period in an attempt to distinguish which, if any, were responsible for impeding the infants’ journey to theatre and thus length of stay. The most striking observation was a marked reduction in time taken to normalize electrolytes from 25 h (16.5–42.0) to 9.5 h (4.5–24.8); p = 0.004. This observation was echoed by the finding that the time in hours to surgical intervention from admission was also reduced in the uncorrected infants from 50 h (40.3-66.8) to 39 h (28.8–41.8); p = 0.018. However, as expected, the time to surgery in children who had normal electrolytes on admission remained unchanged: 25 h (20.0–42.5) versus 25 h (14.0–38.5); p = 0.445 (Table 2). No complications were attributable to the change in fluid regime.
Parental satisfaction
The return rate of parental satisfaction questionnaires was 63% in the pre-pathway group versus 52% for the post-pathway group. Twenty-nine of sixty-three (43%) of parents in Group 1 were satisfied with the pre-operative counselling they had received in our unit compared to 17 of 17 (100%) in Group 2. Thirty-three of sixty-three (52%) versus 11 of 17 (64%) were pleased with the time taken to take their child to theatre in Groups 1 and 2, respectively. Only 3 of 17 (18%) parents in Group 2 were content with the time taken from theatre to discharge, which remained unchanged compared to 12 of 63 (19%) in Group 1. Overall, 15 of 17 parents in the post-pathway group (88%) felt that the service they had received was above the standard they had expected and would recommend our unit to friends or relatives, increasing the overall standard of parental satisfaction from 48 of 63 (76%) in the pre-pathway group.
Discussion
Infants presenting with IHPS are often dehydrated and demonstrate electrolyte abnormalities such as hypochloraemia, hypokalaemia and metabolic alkalosis, requiring intravenous fluid replacement therapy5,6,10 representing a significant pre-operative delay. There is currently a paucity of evidence regarding the optimum type and rate of fluid replacement to correct electrolyte abnormalities in IHPS. To the best of our knowledge, there are no published studies related to the use of care pathways incorporating standardized fluid regimes and CBG/U&E monitoring for IHPS. The degree of initial biochemical derangement and rate of correction of alkalosis in infants with IHPS has been shown to correlate significantly using a standardized fluid regimen, 11 but the effect of this on overall length of hospitalization remains to be evaluated. The consensus fluid and electrolyte replacement therapies used in our unit were agreed upon by the consensus group involved in developing the care pathway for IHPS as described in Figure 1.
All of the health care professionals in the consensus group were involved in the day-to-day care of infants with a wide range of surgical conditions, including, of course, IHPS. Our surgical unit is in one the largest dedicated children’s hospitals in Europe, with a catchment area of approximately 7.5 million children. Five to ten cases of IHPS are admitted and managed in our unit every month, and the members of our consensus committee were considered well qualified to provide opinions on the clinical care pathway based on the wealth of their expertise and experience in caring for infants with IHPS. Parents who were invited to join the consensus group were those whose infants had been operated on in our unit for IHPS and therefore had direct experience of care for this condition in our unit.
Once the consensus committee was established, meetings were held to initially present the data from the pre-pathway cohort of 100 patients, detailing which aspects of care were felt to be substandard and where potential improvements could be made. A clinical care pathway was then proposed and a draft pathway was put forward by the paediatric surgical team. Members of the consensus committee evaluated the draft pathway and a consensus was reached taking all members’ views into account. From the results of the pre-pathway group data, it was felt that one of the most important aspects of care to be streamlined was the lengthy time to, and recognition of, correction of metabolic alkalosis. This was felt to be the principle factor involved in ‘delays’ to the infant going for surgery by all members of the consensus group. Some of the issues that were more difficult to reach consensus on were the perceived priority of infants with IHPS on the emergency operating list, and the appropriate times of day or night to operate on these infants. The paediatric surgical team felt that patients with IHPS should be prioritized as patients with gastric outlet obstruction who were nil-by-mouth and dependent on intravenous fluids and electrolytes. Senior paediatric anaesthetists had some conflicting priorities based on their availability, as they were not required to be present for uncomplicated older children going to theatre but they were required for the few-week old infants with IHPS. Surgical unit bed managers also preferred other smaller cases such as nailbed or facial lacerations to be operated first on the emergency operating list as these patients could go home the same day and not take up any bed spaces. These conflicts are not unique to our unit and are an inherent consequence of health care resource rationing, such as is necessary within the National Health Service (NHS) in the United Kingdom. Agreements over the fluid regimes and timing of CBG/U&E measurements were easily made, as was the universal use of the post-pyloromyotomy feeding regime.
Once the clinical care pathway had gone through an initial pilot period of three months, the consensus committee was again assembled to work through any minor amendments felt necessary, which were brought to light by the clinical and nursing staff who were using the pathway day-to-day. The pathway was then put to use for all patients with IHPS for a period of 12 months to allow its use to become common-place prior to collecting data from the post-pathway cohort of patients. The consensus committee was assembled for a final meeting to present the results of the post-pathway group compared to the pre-pathway group, and also to integrate the standardized fluid and electrolyte replacement and monitoring regime into local guidelines. These guidelines were then disseminated to the referring units in our catchment area, for use by paediatricians caring for infants diagnosed with IHPS prior to their transfer to our unit for definitive surgery.
‘Normal range’ biochemical values were used according to UK national paediatric biochemistry laboratory guidelines. 8 In the stratification of patients into ‘corrected’ and ‘uncorrected’ arms, we used measurements for capillary pH, bicarbonate and base excess on the CBG and potassium and chloride on the U&E. Normal ranges and units of measurement vary somewhat from unit to unit in the United Kingdom and also more widely internationally, and we have therefore deliberately limited our description of biochemical results as corrected or uncorrected metabolic alkalosis. We would thus advise readers to continue to use their standard method of determination of biochemical correction of metabolic alkalosis in IHPS prior to using our fluid and electrolyte replacement regime if desired.
Twelve-hourly monitoring of electrolytes was selected, as this time frame has been used effectively in previous studies examining the range of electrolyte disturbances in IHPS. 12 Additionally, 12-hourly blood sampling was thought to be the most appropriate by the parents within the consensus committee. Previous authors have described reductions in duration of hospitalization by using standardized post-pyloromyotomy feeding regimens. 13 The post-operative feeding regime we used is well established and preferred by the majority of clinicians in our unit, and thus was included in the care pathway.
Clinical pathways are used in a variety of clinical scenarios, and act to minimize variability in care, as well as providing useful tools for audit, re-audit and quality assurance. 14 A number of supporting factors contributed to our units decision to implement a care pathway for IHPS and helped to inform the implementation process. For example, our institution has previously demonstrated an improvement in outcomes following the introduction of an integrated clinical pathway for acute appendicitis, whereby the complication and readmission rates were significantly reduced. 15 Some disease processes are more applicable than others to care pathway implementation, and the suitability of IHPS in the context of clinical pathways has been previously successfully evaluated. 16
The study design used here was observational, conceived following perceived delays to time to electrolyte correction and to surgery for infants with IHPS, ultimately leading to a lengthier stay in hospital and anecdotal poor parental satisfaction with care provided. The 100 patients in the pre-pathway group were chosen arbitrarily to inform the consensus group in more detail as to the variables involved in pre- and post-operative care of patients admitted with IHPS. Prospective analyses carried out on the post-pathway group was felt to yield more accurate data collection despite differing in methodology from the retrospective analysis of Group 1. Following a preliminary data collection period of three months, the pre- and post-intervention groups were compared. A post-hoc power calculation revealed an acceptable power of 80.8%, and having achieved our aim of statistically significantly streamlining care for infants with IHPS, data collection was terminated at this point.
Our original hypothesis was that by implementing a care pathway for IHPS, which incorporated a standardized fluid and electrolyte replacement regime, we could decrease length of hospitalization for these infants and their parents. We demonstrated a reduction in length of stay in hospital from a median of 94–75 h (p = 0.025), statistically significantly reducing the time required to be in hospital for these families and their newborns. This also equates to 26 bed days every quarter, and over 100 bed days per annum released for use by other children requiring tertiary paediatric surgical care. A standard ‘bed day’ in our unit equates to 24 h inpatient hospital stay on a surgical ward, requiring standard multi-professional care. In our unit, the cost of each bed day is approximately £600 (€780, $870), leading to a potential saving of £60,000 (€77,800, $87,000), purely as a result of implementing our clinical care pathway.
Our secondary outcomes were based on a breakdown of aspects of care addressed in the care pathway and are summarized in Table 2. We found that by using a standardized fluid and electrolyte replacement regime for infants with uncorrected metabolic alkalosis, we decreased the time for biochemical normalization by 15.5 h (p = 0.004). We also looked at time to surgery from admission and found that this was also decreased in the initially uncorrected infants by 11 h (p = 0.018), but unchanged in patients who had normal CBG and U&E on admission (p = 0.445). These results suggest that using a standardized fluid and electrolyte replacement and monitoring regime as part of the care pathway decreases the time to correction of metabolic alkalosis.
The parental satisfaction questionnaires used in our study are as yet unvalidated and provide only the opinions expressed by the parents as they left the surgical unit. The response rate between the pre- and post-pathway groups is comparable (63% vs. 52%, respectively). The overall parental satisfaction increased from 76% to 88% between the pre- and post-pathway groups. We feel this reflects our achievements in statistically significantly decreasing time to procure and recognize biochemical normality, and thus decreasing waiting time to surgery and potentially distressing time spent with the infant being nil-by-mouth. The responses to pre-operative counseling and time to discharge following surgery were very similar between the two groups, reflecting the fact there were no differences in these aspects of care between the pre- and post-pathway groups.
We acknowledge that collection of subjective opinion-based data in the manner described is liable to inaccuracies for multiple reasons. The parents who did not return satisfaction questionnaires may have been less satisfied, and thus felt awkward or embarrassed about giving poor feedback. Alternatively they may not have had strong feelings either way or felt that their opinions would not make any difference. The difficulties of obtaining and interpreting patient/carer opinions are widely appreciated and further interpretations of non-respondence are beyond the scope of this discussion. It was felt, however, that parental satisfaction was also affected by factors such as delayed diagnosis and prolonged waits for correction of metabolic alkalosis in referring units in our catchment area, and also by waiting for an available bed in our unit (which parents had hand written on their questionnaires) and we could not account for these factors in our analysis.
Following the decision to create a clinical care pathway for IHPS in our unit, contributions from all stakeholders involved in our service provision, including parents, were integral to the successful implementation of the care pathway. All infants in the post-pathway group were managed according to the pathway guidelines. The involvement of all those invested in improving care for infants with IHPS, combined with the increasing use of clinical care pathways in our unit undoubtedly contributed to the universal compliance with care pathway utilization.The resultant impact of our intervention on length of hospitalization has been similar in magnitude to that found in a randomized controlled trial comparing outcomes following laparoscopic versus open pyloromyotomy. 17 These results serve to highlight that relatively minor changes to routine care can result in significant improvements. Our findings are clinically important and applicable to a large number of patients diagnosed with IHPS and the clinicians responsible for their care.
We feel our work has shown statistically significant improvements in streamlining care for infants with IHPS by the implementation of our care pathway. However, our study was performed at a single institute and it may also be beneficial to repeat the study using multiple paediatric surgical centres to minimize patient homogeneity and eliminate observer bias.
The observational nature of this pre- and post-intervention study has the inherent limitations of being a non-randomized study. The next step could be a prospective blinded Randomized Controlled Trial comparing the standardized fluid and electrolyte replacement and monitoring regime used in the post-pathway group to the adhoc fluid administration and irregular CBG and U&E measurements in the pre-pathway group.
Conclusion
Our care pathway for IHPS reduces the time taken to correct electrolyte abnormalities, decreases length of hospitalization and improves parental satisfaction.
Footnotes
Acknowledgements
We extend our thanks to Dr J. Strong and Dr L. Woodgate for their contributions to data collection in the pre-pathway patient group.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.