
Abstract
Many countries are experimenting with new models to better integrate care; yet, innovative care models are often implemented as time-limited, localised projects with limited impact on service delivery more broadly. This paper seeks to understand the processes behind successful projects that achieved some form of ‘routinisation’ and informed system-wide integrated care strategies. It draws on detailed case studies of three integrated care experiments: the ‘Integrated effort for people living with chronic diseases’ project in Denmark; the Gesundes Kinzigtal network in Germany; and Zio, a care group in the Maastricht region in the Netherlands. It explores how they were developed, implemented and sustained, and how they impacted the wider system context. All three models implicitly or explicitly adopted processes shown to be conducive to the dissemination of innovations, including dedicated time and resources, support and advocacy, leadership and management, stakeholder involvement, communication and networks, adaptation to local context and feedback. Each showed robust evidence of improvements on a number of service and patient outcomes and these findings were central to their wider impacts, shaping country-wide integrated care polices. However, the wider dissemination of projects occurred in an incremental and somewhat haphazard way. To further redesign health and social care a more formal strategy, alongside resources, may thus be needed to provide funders and providers with genuine incentives to invest in new business models of care. There remains a crucial need for better understanding of specific local conditions that influence implementation and sustainability to enable translation to other contexts and settings.
Introduction
One of the core challenges facing health systems globally is the rapid rise in the number of people with multiple health and care needs. This, in combination with population ageing and increasing frailty at old age, requires a rethinking of health and care services that can bridge the boundaries between professions, providers and institutions and so provide appropriate support to people with long-standing health problems. 1
In Europe, countries have sought to create a regulatory and policy framework to promote better care integration and improve coordination between sectors and levels of care. 2 Systems have tended to focus on implementing strategies within existing service structures while more innovative care models that perhaps challenge established ways of organising services are often implemented as time-limited pilot or small-scale, localised projects. 3 There is however a small number of projects that have expanded beyond the initial stages, achieving some form of ‘routinisation’ within the system or informing coordinated care approaches across the country more widely.
This paper examines three such pilots in, respectively, Denmark, Germany and the Netherlands, seeking to understand how they were developed, implemented and sustained, and how they impacted the wider system context. It draws on detailed case studies of the ‘Integrated effort for people living with chronic diseases’ (SIKS) project in Copenhagen 4 ; the Gesundes (‘healthy’) Kinzigtal integrated care network in Germany 5 ; and Zio, a care group in the Maastricht region in the Netherlands, 6 which were conducted as part of a World Bank project. 7 The selection of case studies was informed by earlier work of the authors, 3 and case studies followed a structured data collection template. 7 We first set out the general health system context within which the projects have evolved and then synthesise the main observations from the detailed case studies of integrated care as they relate to (i) design features, (ii) financing arrangements, (iii) organisational structures and processes, (iv) implementation and (v) outcomes and impacts. We conclude by drawing lessons from the case studies for the further dissemination of integrated care.
Health system context
Denmark, Germany and the Netherlands provide universal and reasonably equitable access to health care for their population. They are financed primarily through taxation (Denmark) or statutory health insurance (SHI) (Germany, the Netherlands) and have similar levels of health spending in terms of percentage of national income, at 10–11% in 2013 (OECD average: 8.9%) (Appendix 1). 8 The three countries vary however in relation to health care governance structures and organisation. Thus, Denmark and Germany have devolved administrative and political responsibility fully or in part to local and regional authorities or federal states. In Germany and the Netherlands, corporate actors (e.g. insurers, providers) also play an important role in governing the health system.
The general practitioner (GP) typically serves as the first point of contact for non-urgent care in all three systems. Denmark and the Netherlands operate a system of GP patient registration and offer choice of a GP (although restricted to within geographical areas in Denmark), who controls access to most specialist care in non-urgent cases.9,10 In Germany, patients can see any GP; they also have direct access to medical specialists outside hospital. 11 Voluntary GP gatekeeping has been in place since 2004, but only about 20% of eligible population have opted for this. 12
Care fragmentation, along with overall substandard levels of quality of care delivered to those with chronic care needs has been a main concern in all three countries, and this has prompted a series of regulatory measures and policy initiatives, although the pace, breadth and depth with which these have been implemented has varied (Appendix 2). 3
Developing and implementing integrated care: The Danish SIKS project, Gesundes Kinzigtal in Germany and the Maastricht care group Zio
Key features of the SIKS project, Gesundes Kinzigtal and the Maastricht diabetes care group.

Design features
While evolving against a similar background of shortcomings posed by the existing service delivery system, the three approaches vary in terms of specific aims and objectives, populations targeted and the range and number of providers involved. For example, the SIKS project was set up as a research project that operated from April 2005 to September 2007 in Copenhagen.4,14 Funded by the Ministry of Interior and Health, it focused on the implementation of rehabilitation programmes for people with type 2 diabetes, chronic obstructive pulmonary disease (COPD), heart disease or with balance problems following falls, requiring close collaboration between a local health care centre, a local hospital and GPs. The target population was the resident population of the Østerbro district of Copenhagen, with around 700 patients receiving services over the duration of the project (Table 1). As a research project, the SIKS model was completed in 2007, but the interventions implemented as part of the project informed the development of similar integrated care models elsewhere in the country as well as policy development for coordinated care approaches in Denmark more widely (see below).
The Gesundes Kinzigtal integrated care approach was set up in 2005 as a pilot project on the initiative of a local physicians’ network in the Kinzigtal region in southwestern Germany and a health care management company. 5 It sought to develop a regional health care delivery system that provides value for money through producing better outcomes, improved quality of care and enhanced patient experience for the resources spent. It is financed by two regional SHI funds through an arrangement made possible by the 2004 health care reform, which enabled SHI funds to designate financial resources for selective contracting with single providers or networks of providers until 2008. 11 The Kinzigtal approach targets the entire population in the region, and by the end of 2014, about one-third of the eligible SHI population had signed up. It coordinates about 160 partners, mostly office-based physicians, as well as hospitals, nursing homes, home care services and others. SHI members enrolling in the programme maintain choice of provider and can leave at the end of each quarter. A key design feature is a shared savings contract between the contracting partners, which we discuss below. 15
Similar to Gesundes Kinzigtal, the care group Zio in the Maastricht region in the Netherlands has its origins in a pilot project that was established by the Maastricht University Medical Centre in 1996, and which used specialised diabetes nurses to reduce the number of diabetes patients seen by medical specialists in outpatient settings. 16 Demonstrating beneficial effects in terms of process and outcome measures, the pilot was developed further into the Matador programme in 2000, 17 and by 2006, about 70% of GPs in the Maastricht region participated in the programme. In 2008, Matador was eventually transformed into the primary care group Zio, which covers a broader spectrum of conditions. The health insurer VGZ acts as principal contractor for the diabetes type 2 programme in the Maastricht region, on the basis of a bundled payment contract (see below). From 2008 onwards similar programmes were developed for patients with asthma, COPD, cardiovascular diseases (CVD), mental health problems and frail elderly. 18
Selected design features and processes of the SIKS project, Gesundes Kinzigtal and the Maastricht diabetes care group.
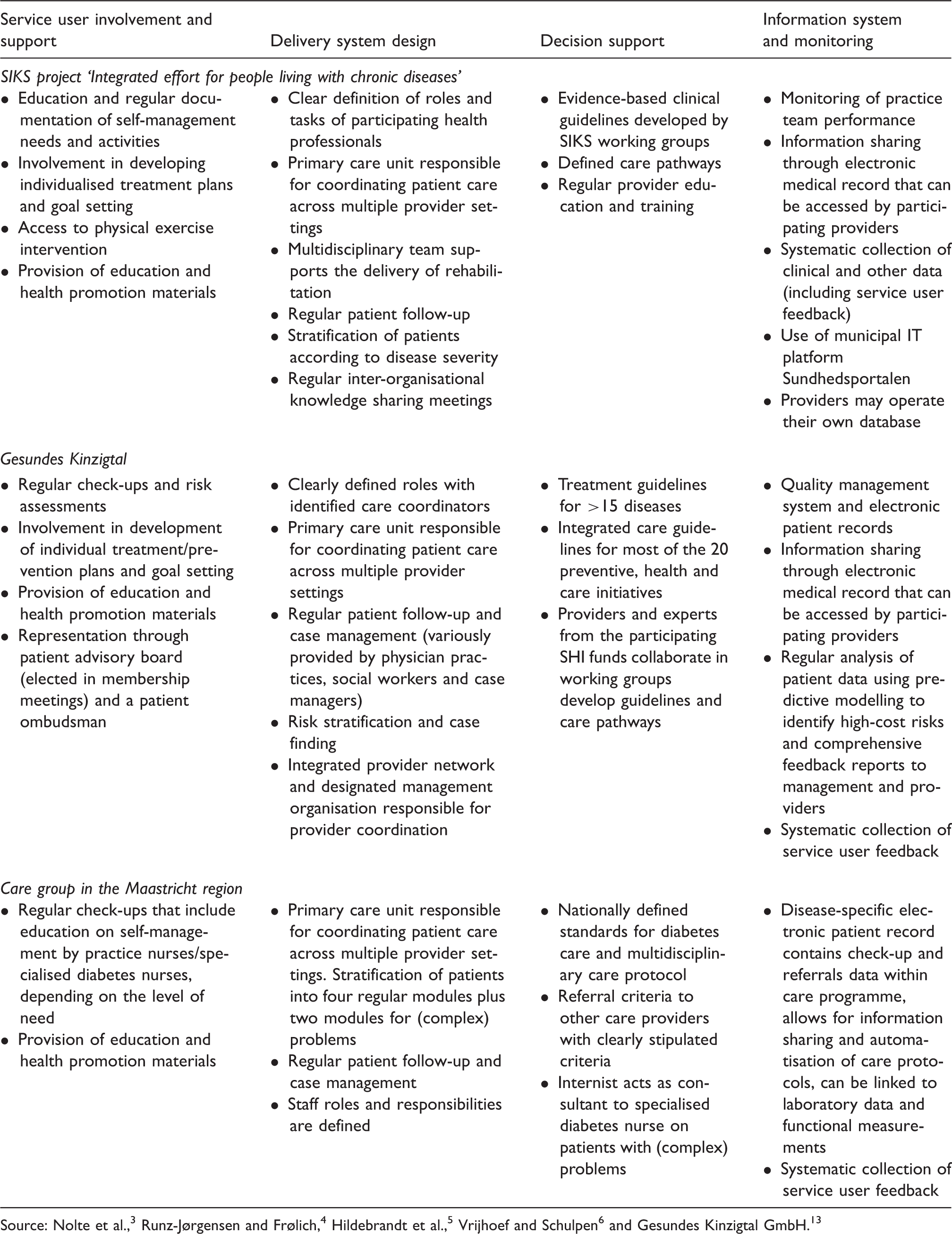
Patient-centredness is at the core of each of the three care models, with all incorporating a systematic approach to patient self-management support, shared decision-making and the development of care plans tailored to individuals’ needs and preferences. Approaches also use some form of risk stratification to allocate patients to the appropriate level of care and decisions are supported by the use of evidence-based and integrated care guidelines. Models further permit the sharing of patient information across different provider levels using electronic medical records. All three approaches draw on multidisciplinary teams and seek to systematically collect and analyse data to measure quality and monitor provider performance to inform improvement efforts.
Financing arrangements
The SIKS project was established within the financing context of usual care and it did not foresee specific incentives for partners collaborating in the project. 4 Gesundes Kinzigtal and the Zio care group have established contractual relations between collaborating partners which include performance agreements. Both approaches also include specific payment mechanisms that allow for budgetary flexibility across provider levels.
Gesundes Kinzigtal is coordinated and managed by a regional integrated care management company (‘Gesundes Kinzigtal GmbH’) that brings together the aforementioned local physicians’ network and health care company. 5 The management company oversees the health care budget for all SHI members of the two SHI funds, with start-up funding of about €4 million used to set up management, quality control, evaluation projects and additional services. Comprehensive integrated care services are offered only to those enrolled in the programme although some services are accessible to all SHI members in the region, such as seminars or occupational health services. Health care providers are reimbursed as under usual care, with additional payments for time spent on patient activation programmes and upgrading of IT infrastructure; providers also receive a share of the company’s profit through a shareholder arrangement. Additional payments comprise 10–15% of providers’ other income. Profit is derived solely from realised savings relative to the average risk-adjusted costs of care, shared between the management company and the SHI funds on the basis of a negotiated shared savings contract. As a for-profit company, the Gesundes Kinzigtal GmbH may reinvest its profits into additional preventive programmes or health promotion facilities or distribute it as part of the profit to its shareholders as above.
The Maastricht care group Zio, as any other care group in the Netherlands, is a legal entity. A care group primarily comprises of primary care providers; it enters into contracts with health insurers to coordinate and provide high-quality chronic care in a specified region. 18 Zio negotiates with the health insurers the content and price of, for example, the diabetes care package for all patients diagnosed with type 2 diabetes in the region who are under the care of a GP or internist. The agreements are captured in a diabetes diagnosis-treatment-combination diagnose-behandelcombinatie (dbc), which defines the precise nature of care to be reimbursed, from diagnosis to the (possible) resultant treatment, along with referral pathways. All care components included in the DBC are covered by the bundled fee that is negotiated between the health insurer and the care group. This makes it possible to purchase care as a single product, even though components are delivered by different health care providers in a range of settings. The care group holds sub-contracts with other partners for the delivery of services not provided by the group. The DBC and sub-contracts include performance agreements to encourage the delivery of high-quality and cost-efficient care. The care group also negotiates with specialists at the local hospital for consultations provided in secondary care; however, financing of secondary care is (as yet) not included in the bundled payment but paid for separately.
Organisational structures and processes
Selected features of organisational structures and processes of the SIKS project, Gesundes Kinzigtal and the Maastricht care group.

All three approaches were guided by a policy framework, which included a strategy or mission statement, a document detailing the planning or design of the care model, and, importantly, a dedicated design and implementation team alongside start-up funding to strengthen capabilities and readiness. Each put in place governance mechanisms to ensure adherence to service requirements specific to the individual approach. In the case of Gesundes Kinzigtal and the Maastricht care group, this involved the conclusion of formal contracts between participating providers or provider organisations that set out performance agreements; governance arrangement also include the use of sanctions for breaching processes and procedures. The Danish SIKS project did not use a formal contracting model; instead it set up a dedicated leadership and management structure to oversee the development and implementation of the rehabilitation programmes across the three participating organisations. The actual rehabilitation programmes were considered as formal agreements by the management and leadership and among health professionals within and between organisations. 4
The governance and management mechanisms implemented by individual care models were seen, in part, to offset a perceived low degree of administrative and organisational integration observed for the SIKS project and Gesundes Kinzigtal (Table 3). In both cases, this lack of actual integration was attributed to the wider system context within which the respective care model was implemented, such as the division of responsibilities for primary, hospital and rehabilitation care between the regions and municipalities in Denmark. 4 However, both approaches demonstrate that it is still possible to achieve a form of virtual integration at the administrative or organisational level where ‘true’ integration is not (yet) possible because of the external regulatory and policy environment. Conversely, the Dutch approach to creating care groups is seen to have been successful in achieving administrative integration and, to a lesser degree, organisational integration. 6 However, the integration effort has so far been limited to the horizontal level, by integrating primary care providers that are part of a care group, strengthened by means of the bundled payment mechanism. Secondary care is not yet part of the bundled payment and the degree of organisational integration between the care group and the hospital has remained low.
Implementation
Considering the actual implementation process, each of the integrated care models reviewed here identified a range of facilitators that were believed to promote integration efforts but they also described aspects, which, while not necessarily hindering successful implementation, were seen to slow down the overall process.
Evidence from research on the diffusion of innovation highlights a number of factors found to be conducive to implementation: dedicated time and resources, support and advocacy, leadership and management, stakeholder involvement, intraorganisational communication, interorganisational networks, adaptation to local context and feedback. 20 All of these factors are reflected in the implementation efforts reported by the three integrated care approaches although their relative importance in supporting the implementation process varied, mirroring the starting point and the complexity of the care model to be implemented.
As noted, each approach established a dedicated design and implementation team to guide implementation of the respective project (Table 3). In the case of Gesundes Kinzigtal, this also involved drawing on the evidence of comparable experiments elsewhere to inform implementation. 5 The SIKS project used existing conceptual frameworks such as the chronic care model 19 to support the development of new management practices and enhance those already in place to promote integrated care. 4 All three models were also able to draw on upfront funding to strengthen capabilities and readiness, although, with the possible exception of the Maastricht care group, the case studies did not explicitly refer to start-up funding as a key factor that facilitated implementation.
Support and advocacy, coupled with leadership and management were seen to be core to the implementation of the integrated care model in each of the three systems, with for example the SIKS project highlighting the key role of the executive leadership of each of the three organisations (the hospital, GP representatives and the City of Copenhagen representing the municipal health care centre) in overseeing integrated service delivery through regular meetings to sustain the development and implementation of the rehabilitation programmes (Table 3). Setting up adequate leadership and management structures was also seen to be key to build trust among participating organisations. The Gesundes Kinzigtal experience highlighted however that while trust among partners was a necessary condition, it was not seen to be sufficient to guarantee successful implementation. 5 Here, the role of contractual arrangements that support the creation of a secure environment with clear roles and responsibilities, allocation of tasks and possible long-term gains for all participating providers was perceived to be vital for the sustainable implementation of the new care model.
Leadership and management structures were also seen to be important in providing support to contracting partners and so strengthen their engagement in the integrated care model. For example, GPs involved in the Maastricht care group were reported to benefit from the care group, which represents and focuses the GPs’ interests in negotiations with other parties, as well as from more practical support such as provider education, protocol development or the facilitation of meetings between health care providers involved in the care group. 6 The Gesundes Kinzigtal experience highlighted the need to provide this type of support on a continuing basis in order to keep network participants engaged, in particular where partners remain separate organisational entities. 5
All three integrated care models also stressed the importance of involving different stakeholders and frontline staff affected by the innovation, for example in the development of structures, guidelines and indicators in order to secure buy-in from participating partners. This was seen to be particularly pertinent in order to win over physicians who tended to be resistant to proposed changes in all three cases.4–6 The active involvement of clinicians, in particular, has been highlighted to be critical to successful implementation of innovation in other contexts also, noting the large degree of control of health professionals in health care organisations such as primary care practices and hospitals. 21 Failure to engage them in the process is likely to hamper sustainable change. In this context, the experience of Gesundes Kinzigtal also emphasised the importance of prioritising collaboration with different providers over competition in order to achieve larger scale buy-in and, ultimately, sustainable change. 5 A similar issue was raised by the Maastricht care group, which highlighted that the collaboration between GPs and the specialists working at Maastricht University Medical Centre was possible because of differences in financing streams, so removing competition for funds between providers. 6
All three approaches built on local relationships and local capacity, so allowing to focus on what is relevant and what works locally. However, there was recognition that where larger networks are concerned there needed to be a balance between local leadership and expertise vis-à-vis centralised functions to optimise strengths and economies of scale. This point was specifically raised by the Gesundes Kinzigtal, which for example centralised functions that do not require specific local knowledge such as data analysis, the development of a data warehouse, or review of national and international best practices to inform guideline development, among other things, while the organisational work, the adaptation of quality guidelines to the local context and local public relation and marketing activities are the responsibility of the Gesundes Kinzigtal GmbH. 5
At the same time, implementation of the new integrated care approaches also faced some challenges and one core factor highlighted by Gesundes Kinzigtal was that of the time that would be required for some aspects of the care model, such as guideline development (getting different stakeholders on board), the development of the financial model (developing and calculating the cost–benefit and the additional fees for the different providers involved in providing services) or the training of staff in delivering the health programmes and engaging patients. 5 Other aspects included the need to understand the capacity of partner organisations to provide innovative care components, in particular where these have to be delivered alongside usual care, or the uptake of information technology, again coupled with the capacity to apply the new system where it is being used in addition to existing approaches. The SIKS project further highlighted challenges associated with awareness of and information about the project at different levels within partner organisations, leading to suboptimal implementation, and, possibly, performance of the intervention. 4
Outcomes and impacts
Each of the three integrated care approaches was subject to a series of evaluations and these have shown evidence of improvements on a number of process and outcome measures, as well as selected utilisation measures. These include significant improvements on intermediate outcomes such as glycaemic control, blood pressure or body weight among patients with diabetes 22 and significantly smaller increases in the number of hospital admissions, bed days and outpatient visits over a two-year period among people with COPD in the SIKS project 23 ; improvements in process measures such as guideline adherence, measures of health care utilisation, health outcomes such as a reduction in the prevalence of fractures sustained by people with osteoporosis, a reduction in the proportion of people requiring long-term care and a reduction in the number of potential years of life lost in the intervention group, measures of patient satisfaction, and costs measured as relative cost savings in the Gesundes Kinzigtal;5,24 or the cost-effective delivery of integrated diabetes care 25 and clinically relevant improvements among patients with poorly controlled diabetes in the Maastricht programme. 26
However, in addition to the direct impacts on service and patient outcomes, individual care models had important wider impacts. The SIKS project is reported to have influenced the way integrated care has been conceptualised in Denmark. 4 For example, the project involved the establishment of a new health care centre in the Østerbro district of Copenhagen, and after completion of the project, a similar centre, based on the SIKS model, was established in the Nørrebro district of Copenhagen. This was followed by the establishment of health care centres in other districts of Copenhagen and, eventually, across Denmark. Furthermore, the experiences obtained in the SIKS project are seen to have crucially informed wider policy development for coordinated care approaches in Denmark and, ultimately, the introduction of regional disease management programmes. 27 The scaling up of the SIKS project was further informed by a research collaboration between the Danish health care system and Kaiser Permanente that compared important aspects of chronic care and that led to important learnings.28,29
Conversely, although the Gesundes Kinzigtal integrated care model has received widespread attention nationally and internationally, it has so far remained local in that the model has as yet to be transferred to other regions in Germany. However, this is slowly changing and there is reported interest in other regions to either directly copy the Kinzigtal model or develop similar structures both within Germany as well as other countries in Europe. 5 The journey of redesigning chronic care delivery by the Maastricht care group has been recognised nationally and internationally, seen to be exemplary mainly for three features: integration of chronic care delivery and its funding, large-scale primary care provision and the interplay between redesigning and scientific evaluation. 30
From implementation to dissemination
In this paper we set out to understand the journey of innovative care models in three countries that have evolved from small-scale research or pilot projects challenging the established ways of organising care and that have achieved some form of routinisation within the system or have informed system-wide coordinated care approaches. Perhaps not unexpectedly, we show that the wider dissemination or scaling up of successful integrated care pilots seems to have taken place in an incremental and perhaps somewhat haphazard way.
There are different ways of thinking about scaling up innovative care models such as the three case studies presented here. 31 One approach is to simply enlarge the models to cover a wider catchment area or population. However, this would mean increasing the number of partners to ensure adequate service delivery for a larger population. The experience of Gesundes Kinzigtal seems to suggest that there is a limit to the maximum number of members a network can accommodate and function effectively. 5 A similar point has been brought forward in relation to care groups in the Netherlands, arguing that a care group would require a certain minimum size (i.e. number of partners) to ensure a critical mass to get a programme off the ground. At the same time, the size of the group should be limited to ensure appropriate governance of the organisation. There was a notion that the ideal size of the care group should be one that facilitates trust and collaboration and that is sufficiently large to present a strong voice in negotiations with health insurers. 6
Another way of thinking about scaling up is to copy the successful model and implement elsewhere and so sustain local identity. While this appears feasible in some settings, and indeed, the SIKS project in Denmark illustrates such an approach, it raises questions of implementability in areas with a different socio-economic and demographic context, different provider mix and other local characteristics that may not be easily transferable.
The SIKS project in Denmark and the care group model in the Netherlands illustrate a further approach to scaling up: the wider dissemination of the respective models has been possible through allowing for some modification of a given approach in order to enable widespread takeup. 32 This might mean that innovative elements may have to be adapted, and although modifications may need to be introduced to make the programme more acceptable to different stakeholders, the wider rollout in the Netherlands was facilitated by supportive measures, such as the introduction of the bundled payment system for care groups. 3
In order to scale up and further redesign health and social care a more formal strategy, alongside resources, at national or perhaps even international level may be needed to provide funders and providers of services with genuine incentives to invest in new business models of care. This can draw on existing evidence of proven strategies for the dissemination of evidence-based practices, 33 further guided by international strategies such as the WHO’s Global Strategy on People-Centred and Integrated Health Services 34 and the forthcoming Framework for Action towards Coordinated/Integrated Health Services Delivery. 35 At the same time, for any effort to elevate innovative models of service delivery that provide promising results to a level beyond pilot project or best practice, there is a crucial need for better understanding of specific local conditions that influence the implementation and sustainability of a given approach so that identified processes can be translated to other contexts and settings. 3
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: EN presented the findings of this study at the BMC Kongress 2016 ‘Innovation’ in Berlin; her travel expenses were paid for by the Bundesverband Managed Care e.V. HH is CEO and owner of OptiMedis and CEO of ‘Gesundes Kinzigtal AG’, which manages the Gesundes Kinzigtal integrated care network; AP is employed by OptiMedis, which provides support to the Gesundes Kinzigtal integrated care network. GJS is the medical director of ZIO Zorg In Ontwikkeling.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the World Bank as part of the project ‘Case Studies on People Centered/Integrated Health Care in OECD countries’. The views expressed in this article are those of the authors alone and the World Bank is therefore not liable for any use that may be made of the information contained herein.