
Abstract
Introduction
Heart failure is a widespread chronic cardiac illness with varying etiologies. If the HF patients manage themselves at home by following the appropriate advice by healthcare professionals, they tend to have better quality of life and less readmissions. This study was aimed to identify and explore practices of self-management by heart failure patients, home management of heart failure by their family caregivers and hospital management by healthcare providers.
Methods
A qualitative study was conducted in a tertiary care center in Northern India on participants (patients, their family caregivers, doctors and nurses) who were recruited purposively and interviewed individually by principle investigator using semi-structured questionnaires. Interviews were audio recorded and transcribed after taking informed consent. Iterative process including coding, reviewing and analyzing was done by four researchers and themes were finalized.
Results
Total 41 participants (15 patients, 12 family caregivers, 4 doctors and 10 nurses) completed the interviews. It was observed that patients and family caregivers were not able to manage heart failure efficiently. Nurses and doctors reported many barriers to provide specialized care to these patients.
Discussion
There were definite barriers and challenges in the management of heart failure symptoms by the stakeholders. For the patients and family members who suffer this debilitating illness, managing heroically is a challenge. It is important to develop self-care management protocol for the heart failure patients. Healthcare professionals must overcome the barriers to train patients and family caregivers. Multidisciplinary integration can fulfill the gap in providing care to such patients.
Introduction
Heart failure (HF) is a common cardiovascular illness responsible for significant hospital readmissions especially, in older ages.1,2 It has been reported that Indian patients of HF present at least a decade earlier than the western counterpart thereby, increasing significant morbidity, mortality as well as an increased burden on healthcare cost. 3 In addition to guideline-directed medical therapy (GDMT), patients are educated about how to care for themselves at home. Managing patients at home includes keeping themselves physically fit, periodic weight monitoring, taking medications as prescribed, adhering to dietary precautions and regular follow up.4,5 Both patients and caregivers play a pivotal role in the overall management of HF when it comes to a team approach to HF management. However, living with the disease is itself challenging for both patients and caregivers as coping with symptoms and complex therapeutic regimen is tough. 6 Following this they exhibit depression and limited functional capacity. It has been seen that effective management of HF requires partnership and trust within and between patients, families, and healthcare professionals. 7
We do not know how much patients and their families know about HF and the necessary ways to tackle symptoms in settings like ours. A paucity of time and overburdened health facilities find themselves unable to enquire patients and their caregivers about how do they manage themselves at home; what are the barriers and challenges while caring for such patients; how and when do they decide to visit a health facility for intervention etc. Qualitative research is warranted to explore the impact of caregiving on the management of HF symptoms and the complexity of care. 8 Various factors act as barriers while adopting and implementing treatment due to which patients do not get the required treatment. 9 –10 The barriers faced by cardiologists while managing HF patients are also not well determined and such issues are never addressed even in the tertiary care centers. Although there are standard guidelines by advisory committees regarding HF management with or without various comorbidities still, data is lacking on how far the low resource settings like ours adhere to such recommendations. In addition to this, it has been reported that even trained healthcare workers feel hesitant in performing interventions required to empower heart failure patients in managing themselves. 11 Nurses rendering care to HF patients may not be trained always to manage HF including dose titration of medications. Moreover, if their interaction with patients is limited, they may be unable to understand patients’ perspectives of HF. Lack of time for patient education and lack of coordinated care among various specialties are the other barriers to provide optimal care. 12 So, if any disease management program has to be effective, addressing issues from patients, family caregivers, doctors, and nurses are necessary.
The main focus of the current study was to gain insight into how the HF is being managed by patients, their family caregivers, cardiologists, and nurses. HF management practices of patients mean how patients identify worsening symptoms and manage by themselves at home. HF management practices of caregivers, mean how to they manage HF symptoms, challenges, and barriers faced by them while caregiving. And regarding healthcare workers (doctors and nurses), how do they manage in resource-limited settings. Whether they can lessen the gap between standard guidelines and actual care being delivered to these patients or not. Keeping this in mind, this study was conducted to explore and identify the practices of self-care, home care, and hospital management of heart failure by the patients, their family caregivers, and health care providers (doctors and nurses).
Methods
The study was conducted in a tertiary care center in Northern India from 4th June – 31st July 2018.
It was a qualitative study to explore the practices of self-management, home care management, and hospital management of HF by the patients, their family caregivers, and healthcare workers (doctors and nurses) respectively. Study participants were patients suffering from HF attending cardiology OPDs (out-patient departments) of a tertiary care center, their caregivers, nurses, and doctors managing the heart failure. Participants meeting inclusion/exclusion criteria were selected by the principal investigator.
Inclusion and exclusion criteria
Unstable heart failure – Acutely decompensated heart failure (ADHF) when a patient requires in-patient management for worsening of symptoms. We didn’t enroll such patients as they are directly admitted to the cardiac intensive care unit from the emergency area.
Participants were selected purposively and interviewed face to face regarding their current practices of management of heart failure symptoms separately after obtaining written consent.
The research team consisted of a principal investigator (BK), an M.Sc. cardiovascular and thoracic nursing student, two post-doctoral nursing faculty members (SK and MD) having experience in qualitative methods, one professor (AB) and one associate professor (PB) from the department of cardiology and one faculty member (KK) from the department of biostatistics.
Data collection
Data were collected using in-depth semi-structured interviews using interview guides (Supplemental Table 1 and Table 2) by principal investigator in the clinic. Principle investigator introduced herself before initiating the interview. The purpose and need of the study were explained to the participants. It was clearly announced that the treatment of participants will not be affected by their participation or non-participation in this study. The average time to conduct an interview was explained to the participants in the beginning. The tool was pilot tested initially on four participants and appropriate changes were incorporated to enhance the feasibility and clarity.
The interview lasted for 10–15 minutes. No other person was present in the clinic apart from the participants and principal investigator during the interview. Interviews were audio-recorded after taking informed consent from the participants. They were transcribed and the verbatims were written in their language. Data saturation was not awaited as the interview guide was semi-structured. Transcripts were returned to the patients and caregivers during their next scheduled visit to comment upon. It was not returned to the doctors and nurses as they affirmed their responses. Information regarding demographic characteristics and status of illness was obtained from the patients. They were enquired about how do they monitor and manage themselves at home; adhere to the therapeutic regimen; follow up; identify worsening symptoms and anticipate prompt action. Family caregivers were asked about how long they were actively taking part in the care of the patient and what is their role in the management of heart failure patients, how do they tackle emergencies and how do they make patients adhere to the prescribed therapy. Prompts were given in between to facilitate clarity of their responses.
A separate semi-structured interview schedule was prepared for family caregivers of heart failure patients, nurses working in cardiology OPD, and cardiologists managing heart failure patients. Four cardiologists having work experience of more than three years in cardiology were interviewed regarding how do they classify and treat heart failure patients; schedule follow up; and what are the barriers and facilitators of providing optimal specialized care to these patients. Ten nurses working in cardiology units form the last 6 months to ten years were interviewed regarding the burden of heart failure in the same institute; the way they handle emergencies and anticipate urgent intervention, barriers, and facilitators of providing optimal care to such patients. Three patients, three caregivers, two nurses, and one doctor refused to be study participants due to lack of time. No repeat interviews were carried out.
Data analysis
The recorded interviews of participants were listened to, ranscribed to written form, checked for accuracy, and anonymized afterward. The data were openly coded by four coders and similar codes were written together to create themes. Themes and subthemes were made and reported using six-step approach.13,14
A common consensus of coders was considered regarding themes generation. No electronic software was used to manage the data. To clarify the process of themes generation, the statements of participants were given in their original verbatims along with their codes. Participants didn’t provide any feedback on the findings of the study.
Trustworthiness of the study was ensured by multiple ways. For credibility, we made observation of the participants for long time (nearly 1 year) in the same area regarding their practices of heart failure management. Data triangulation was done by making the field notes and collecting data from various resources like hospital database and different type of participants. Audit trail was done as the data was systematically organized, documented and rechecked by all the authors at regular intervals. The findings like ‘common HF symptoms’ can be transferable globally but the barriers and challenges faced by all the participants regarding HF management may be transferable to developing nations.
Ethical considerations
The study was approved by ‘Institute Ethics Committee of Post Graduate Institute of Medical Education and Research Chandigarh, India’ and was registered in CTRI (Clinical Trials Registry-India) also. Participants were told about the aim of the study and those who consented to participate, were included in the study. Written informed consent was obtained from the participants. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki, revised in 2000 as reflected in a priori approval by the institution's human research committee.
Results
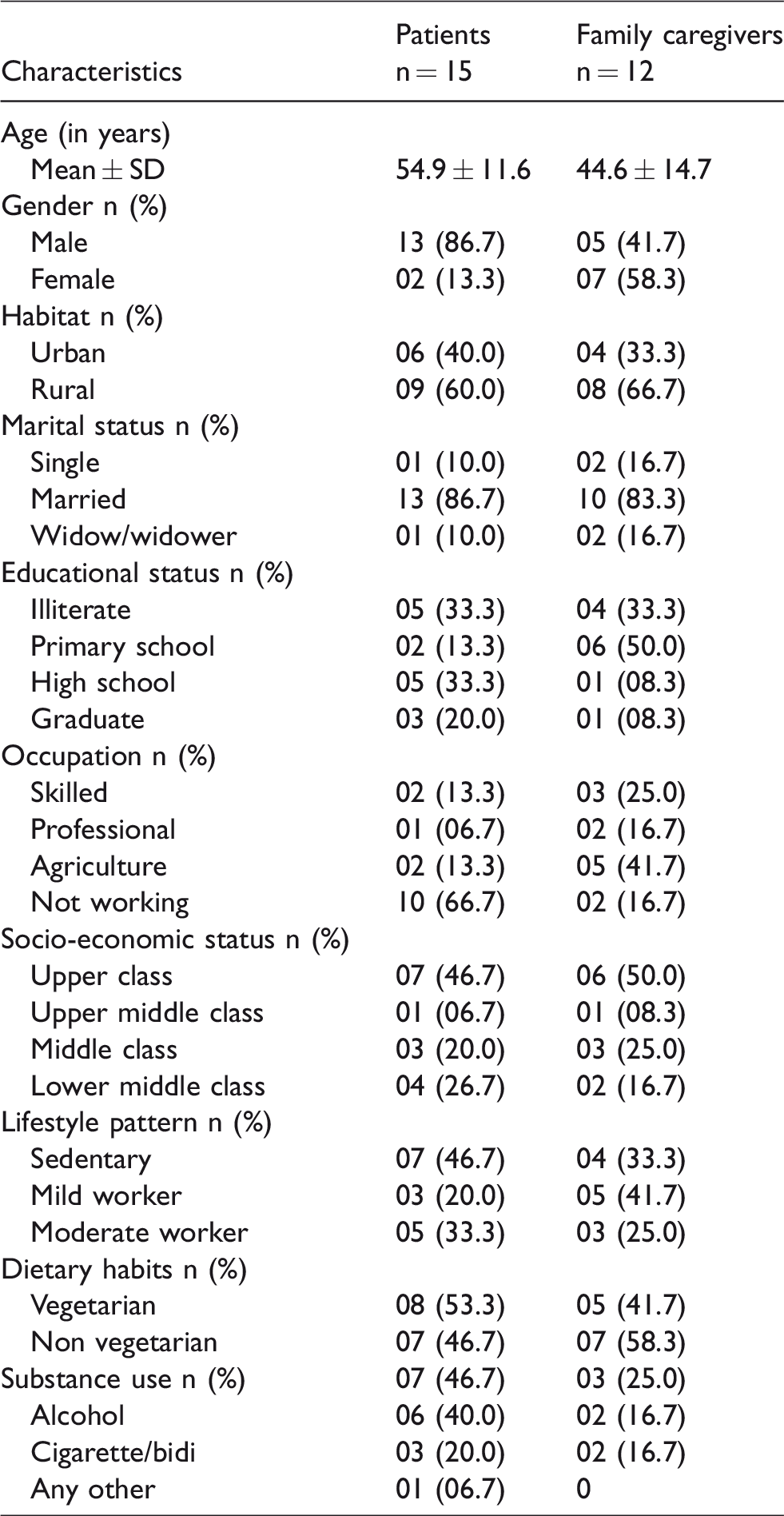
Total 41 participants (15 patients and 12 family caregivers, 4 doctors and 10 nurses) completed the interviews. The mean age of patients and family caregivers was 54.9 ± 11.6 years and 44.6 ± 14.7 years respectively. The rest of the demographic and personal characteristics of the patients and caregivers are mentioned in Table 1. In this study, various themes and subthemes were finalized after analyzing the interviews separately with HF patients, their family caregivers, doctors, and nurses caring for these patients. Majority of the participants were patients (36.6%) followed by caregivers (29.2%), nurses (24.4%) and doctors (9.7%).
Baseline Characteristics of patients and caregivers who underwent one to one interview regarding their current practices of self- management of heart failure.
Interviews with patients
Nine themes were generated using content analysis of interviews with the patients who were suffering from HF for at least six months (Table 2). Patients revealed that their family members played an important role in their care. They reported classical features of HF like breathing difficulty, pedal edema, generalized weakness, and few miscellaneous symptoms.
Themes and subthemes from interviews with patients and caregivers who underwent one to one interview regarding their current practices of management of heart failure.

The themes and subthemes are represented by bold letters and non-bold letters respectively.
One of the participants said – Previously I used to watch television, talk to family members, etc. Now, I don’t watch television. I don’t feel like talking over the phone also. – Participant 11
Another verbalized – In a week, sadness and anxiety occur 2–3 times due to illness. I feel like family members are in problem because of me – Participant 14
Participant 3 said – Medicines don’t work properly. I feel like to leave medicines. I leave medicines in between.
Interviews with the family caregivers of HF patients
Seven themes and various subthemes were generated through content analysis of interviews with the family caregivers who were an active partner in the care of HF patients since the occurrence of symptoms (Table 3). They reported that the patients experience a variety of heart failure specific and non-specific symptoms. They handled many problems in home care settings only by following the advice given by health care professionals.
Themes and subthemes from interviews with doctors and nurses who underwent one to one interview regarding their current practices of self- management of heart failure.

The themes and subthemes are represented by bold letters and non-bold letters respectively.
One of the participants said – He (patient) is mentally upset. Other symptoms are: excessive sweating, bradycardia, breathing difficulty, pain in legs, and constipation – Participant 8
Participant 1 verbalized – We take our patient to the hospital due to fever and breathing problems. When medication dose is missed, we consult locally.
Participant 8 told – Health care professionals have advised us not to give juice. We provide tea without sugar, boiled vegetables, low salt and, spices. They (health care professionals) told to take 1.2– 2 liters of water a day)
One of the participants told – We don’t maintain any diary but sometimes if BP is monitored, we record it on a paper and show it to the doctor at the time of follow-up. Whenever he feels low, we reassure him that your treatment is being taken from best place and you will be fine.
Interviews with doctors
Eight themes and various subthemes were generated through content analysis of interviews with the cardiologists (Table 3). All of the participants opined that approximately 20–30 patients of HF visit OPD per day. The no. was not fixed and average no. of patients visiting OPD kept changing.
Participant 2 told – Yeah, medication wise we are doing a good job but as already told, lack of time is a constraint. We cannot say the same thing to 25 people .One thing that can be done is, we can dedicate specific days of OPD for HF patients. Classes also can be taken for these patients.
Participant 1 suggested – If we have dedicated HF clinic with adequate support staff it will be good to manage these patients. Definitely, it will be helpful for patients. If there will be dedicated HF clinics having the trained nurses in that specialty, many of the patients can be sent there for their lifestyle modification. The patients will be properly explained. It will save the time as well as it will be helpful for the patients. But the problem is to have a dedicated HF clinic.
Interviews with nurses
Seven themes and various subthemes were generated through content analysis of interviews with the nurses (Table 3). Everyone reported variable no. of patients visiting cardiology OPD. The reason was, patients did not go to nurses directly. They went to nurses after their routine follow-up to get injections or advice related to the medication schedule.
One of the participants said – We don’t manage these patients. So I cannot comment on this question. They first go to the doctor and then seek clarification regarding medications from the nurses. We don’t have an active role in the management of these patients here in OPD- Participant 2
Participant 1 verbalized – As such the patients do not come to us directly. They go to the doctor and some of them leave from there. Whatever the doctor writes them on their cards, we advise them the same. We advise them the medications and answer their queries regarding exercise and lifestyle modifications. We don’t have any written informational material for these patients.
Participant 1 opined – Patients ask their queries many times. The questions which they ask the doctors, the same questions they ask from nurses. If we have well-defined disease management protocols, then we would know whatever we are teaching them is uniform and correct. Moreover, patients will not be confused. There will be no chance to confirm again and again. It will be time-saving also.
Discussion
Systematic evaluation of responses of participants provided a clear insight into how the patients manage themselves at home and the probable reasons behind readmissions in the hospital. Caregivers revealed that due to lack of awareness regarding preventable strategies, they were not able to encourage patients to remain asymptomatic for a considerable period and landed up in frequent health checkups or emergency interventions. Being in a tertiary care center, cardiologists were adhering to the international standards of classification of disease and prescription of drugs but due to paucity of time and lack of standard institutional protocols, they were not able to control emergency hospitalizations and the overwhelming burden of HF patients. Nurses working in cardiology OPD of the same institution were optimally knowledgeable regarding various aspects of care of these patients. Lack of clear roles and responsibilities and no nurse-led heart failure clinics in the OPD were the main obstacles to provide specialized care to HF patients. In-depth interviews with the participants allowed them to speak freely about their current practices of HF management. Dependability of the data couldn’t be checked. Though the findings of qualitative research do not produce evidence that is generalizable as quantitative research. The transferability of the current findings in other areas can be judged. Doctors and nurses working in the cardiology units were quite enthusiastic to share the challenges and barriers in providing optimal care to HF patients. Current study did not include dieticians, physiotherapists, and social workers who too contribute to the care of HF patients.
The most important findings of the current study revealed that the patients and their caregivers were not trained enough to tackle emergencies at home without consulting health care professionals. The reasons were never addressed as this study is one of the first of its kind in the institute. The multifactorial cause of their inadequacy of self-care was identified through systematic and detailed inquiry of their current practices to manage their symptoms.
Many reasons for the inadequacy of self-care practices of patients to manage HF symptoms were identified. Common reasons were no monitoring of vital events, parameters, and severity of symptoms; poor compliance to therapeutic regimen; financial constraints due to loss of a job; depression due to illness and its effects; lack of awareness regarding lifestyle modifications including dietary precautions; the indefinite response of medications on varying symptoms; no proper training of how to watch and handle emergencies at home; irregular follow-ups.
Caregivers play a pivotal role by involving themselves in the care of HF patients including understanding discharge instructions, follow up, and making patients adhere to the therapeutic regimen at home. 14 In our study, family caregivers were involved in the care of all patients since the beginning of symptoms. Many barriers to provide optimal care by family caregivers of heart failure patients were identified. They included waxing and vanning symptoms and everlasting nature of the illness; lack of knowledge regarding diet, exercise, medications, and monitoring of vital parameters; monetary constraints; absenteeism from the job; lack of education regarding how to tackle emergent situations at home. As mentioned in a study by Moris et al., that due to unpredictable symptoms, patients feel helpless and become dependent on their caregivers which in turn increases the burden on caregivers. 15 Hence it becomes important to make caregivers engaged in all the instructions being provided to the patients so that caregivers can contribute significantly towards clinical improvement of symptoms.
Although, the cardiologists were doing best on their parts related to diagnosis and treatment of heart failure patients, still their interaction with the patients and their family was so limited that patients felt hesitant to ask many questions. Moreover, language barrier and new doctors on every visit left the patients with the negative thoughts about their illness and treatment. These findings were consistent with Fry et. al. and Glogowska et. al. who stated that poor interaction of patients and attending physicians badly impacts patients’ care.16,17 Nurses also play an important role in providing instructions to the patients and caregivers to comply with. In our study, the role of nurses in making patients aware of the grim symptoms of HF, teaching about lifestyle modifications, and encouraging scheduled follow up as patients were not interacting with them in routine except for some medication queries. Few patients in the present study told that they were being advised about lifestyle modifications at hospital visits but they failed to implement those at home as they had inadequate information about the disease. These findings were similar to the study conducted by Horowitz CR et al. saying that patients could not receive proper advice and preventive tools. Hence, were not able to act accordingly to avoid unplanned hospitalizations. 18 It has proven through studies that the specialized educational interventions in the form of oral or written instructions help reduce worst outcomes of heart failure. 19
The current study necessitates that the patients must be educated to manage their symptoms at home as it has been found in other similar studies.20–23 Specialized HF nurses working in the community areas owe the best opportunities to explore the needs of patients and caregivers and, the ways by which sudden deterioration can be avoided. The findings of this study will be beneficial for constructing training modules for patients, their family caregivers, and health care providers. Specialized HF nurses can set up a ‘nurse-led heart failure clinic’ for telemonitoring and follow-up of heart failure patients on an OPD basis. Protocolized approach is implied for healthcare providers like doctors and nurses starting from the entry point of a patient in hospital till discharge. This study revealed that stable heart failure patients can be adequately seen by specialized HF nurses at out-patient clinics provide that the nurses are appropriately trained. Hence, the cardiologists will be able to dedicate more time to the patients requiring complex medical care.
It is concluded that the patients and their family caregivers were inadequately trained to manage the HF symptoms by themselves in their home care settings. Moreover, the lack of protocolized approach by healthcare providers in addition to other barriers, made the hospital management of heart failure more challenging. The study addressed the gaps in patient-centered research for improving the current health system. The individualized or group training sessions for patients and their family caregivers and formal in-service education for the nurses to manage heart failure patients independently or under the supervision of cardiologists can lower down the burden of large no. of HF visits or readmissions. Future research is warranted to know more about the measures to overcome the barriers and challenges faced by the stakeholders in managing such complex illness.
Supplemental Material
sj-pdf-1-icp-10.1177_2053434520982224 - Supplemental material for Exploring the opinion of stakeholders about self-care, home care and hospital management of heart failure patients: A qualitative study
Supplemental material, sj-pdf-1-icp-10.1177_2053434520982224 for Exploring the opinion of stakeholders about self-care, home care and hospital management of heart failure patients: A qualitative study by Bandna Kumari, Sukhpal Kaur, Monika Dutta, Parag Barwad and Ajay Bahl in International Journal of Care Coordination
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.