
Abstract
Introduction
Challenges are often observed during care transitions from home to hospital among frail elderly individuals who tend to be treated by different providers. This study evaluated the effectiveness of early care information transfer on the quality of care transitions among home-dwelling elderly patients in Japan who needed acute hospitalization.
Methods
A cluster randomized controlled trial with a clinic as a clustering unit was conducted with patients aged 65 years and older who had home-visit care and then needed to be hospitalized for acute care. The main outcomes were the quality of care transition perceived by the patient, measured by a self-administered questionnaire, and patient satisfaction, measured by the Hospital Patient Satisfaction Questionnaire. Multilevel regression analysis was used to adjust for clustering and covariates.
Results
Among 177 patients (78 patients in the intervention group vs. 99 patients in the control group) from 17 clinics (8 vs. 9 clinics) who were admitted to hospitals during the study period, 112 patients with main outcomes were included in the analysis (45 patients vs. 67 patients). Quality of care transition was not statistically significantly different between groups (understanding of home care situations: 58.8 vs. 58.2, p = 0.88; preference on where to be cared for: 58.1 vs. 59.6, p = 0.67; goal for discharge: 71.9 vs. 70.9, p = 0.79; care coordination: 66.3 vs. 63.8, p = 0.56).
Discussion
Early care referral in care transition did not show effectiveness in the quality of care transition and patient satisfaction. Studies on information-sharing in the care transition from home to hospitals are needed.
Introduction
Currently, older adults have more chronic diseases and may live with them for many years. Among patients older than 65 years in Japan, more than 52% have at least two chronic diseases, and 19.5% have three or more chronic diseases. 1 Older patients with multiple medical problems tend to be treated by different providers, and thus, they have a great need for care of transitional services.2,3 Additionally, with the pressure to shorten the length of hospital stay, much attention has been focused on challenges at the time of care transition from home to hospital.
Care transitions, or the movement of patients between care settings or care providers, 4 often cause complications and breakdowns5,6 that influence not only patients and their families but also care providers and the whole care team. Studies suggest that older patients with chronic diseases are particularly susceptible to breakdowns in care and have a greater need for continuity and coordination of care. Although high-quality transition of care is essential for these patients to achieve optimal outcomes,4,7 the main cause of breakdown is poor communication in care transitions.8,9
Poor communication between primary care physicians (PCPs) in the community and acute hospital specialists causes discontinuations of medications, 6 adverse events, 5 and greater use of hospital and emergency services. 5 For frail elderly patients, transfer of information about their personal circumstances and care needs at home, such as cognitive, functional, and social deficits; information about caregivers; and advance care planning, 10 as well as medical information is essential for continuity of care.
Under the pressure of shortening the length of hospital stay, the early acquisition of patients’ essential information is critical for developing an optimal discharge plan. However, studies have shown that hospital staff tend to fail to obtain comprehensive information on frail elderly individuals at admission. Some studies have focused on information transfer at admission,11–13 with mobility impairments receiving rehabilitation services 11 or pre-admission risk assessment for elective surgery. 13 Few studies have emphasized the early transfer of care information for older patients with acute hospitalization. Studies have also shown provider-to-provider communication at admission is essential to mitigate the information gap, 12 and to improve both patients and providers’ satisfaction, 14 but the best mode of communication is unclear and varies among countries.
The referral template, which comprises necessary information in a concise manner, showed to improve the quality of referrals and patient outcomes15,16; however, few studies have focused on the care information of older patients with acute hospitalization. This study aimed to explore the effectiveness of early care information transfer using referral templates on the quality of care transition from home care to hospitals among frail elderly patients receiving home care who experienced acute hospitalization in Japan.
Methods
Study design and study setting
This study was designed as a cluster-randomized study with the clinic as the clustering unit. The participating clinics were recruited nonrandomly by the authors and were scattered geographically in Japan. The clinics were primary care clinics providing both home care visits and ambulatory care or home care visits only (enhanced home care clinics). Twenty primary care clinics providing home care visits were randomly assigned to either an early care referral group or a control group in a 1:1 ratio.
When eligible patients of the participating clinics needed to be hospitalized for acute episodes, home visit physicians filled out a standardized early care referral template and sent it to the hospitals along with an ordinary medical referral letter (intervention group) or just an ordinary medical referral letter (control group). After discharge, the questionnaires were mailed to patients from participating clinics and returned to the study administrative office directly.
As the intervention was actively used by PCPs in the intervention group, the PCPs could not be blinded. The patients were blinded to the patient intervention status. The hospitals were blinded to the study purpose.
Participants
Patients were eligible if they were older than 65 years, certified at two or higher levels of eligibility for long-term care, and had been availing home-visit care for longer than two months. In Japanese long-term care insurance, elderly patients receiving home care visits were certified at either level (from one to five) of eligibility for long-term care, and as the need for care increased, so did the certification level.
Patients were excluded if their home visit intervals were longer than three months, and their caregivers were unable to fill out a questionnaire because of cognitive or physical reasons or were judged unsuitable by the home visit physician.
Patients who were admitted to the hospital for more than 90 days or died during hospitalization were excluded. The study was conducted between May 2017 and April 2018.
Intervention
A standardized early care referral template was used for information transfer. At the time the study was conducted, there were no validated tools for information transfer in the care transition of the frail elderly with social and other care needs from the point of continuity of care; therefore, we developed a standardized early care referral template based on qualitative research. 17 In brief, we conducted semistructured in-person interviews with five participants and two focus group sessions with sixteen participants. Participants were PCPs, nurses, pharmacists, and care managers who were engaged in acute hospital settings or primary care settings in the community. Interviews and focus group discussions revealed the components of essential information on hospital admission and discharge. Based on these qualitative studies, we developed a standardized early care referral system. In the one-sheet template, a home visit physician had to fill out 1) basic care information; 2) living and care situation at home; 3) contents of explanation given to patients and family about the medical condition when hospitalization was discussed; 4) purpose of hospitalization; and 5) advance care planning.
To standardize the description of the template, we sent writing guidance and entry examples of those template components to each participating clinic via documents and videos.
Outcomes
Our main outcomes were the quality of care transition and patient satisfaction during hospitalization. These were measured using a self-administered questionnaire mailed to patients from participating clinics after discharge. The caregivers were asked to complete and return it to the study administrative office directly.
Quality of care transition
No validated parameters to measure quality of care transition focusing on continuity of care were available when we planned this study; therefore, we developed a questionnaire with 17 question items in four categories (understanding of home care situations and preference on where to care, goal for discharge, and care coordination). We extracted these four categories from the factor analysis. Briefly, we performed exploratory factor analyses with 20 question items that were developed based on a literature review and the researcher's discussion to identify four empirical factors and reduce the number of items to 17. Each question item was measured on a 5-point Likert scale with responses ranging from “strongly agree” to “strongly disagree.” Category scores were calculated by summing item scores before converting them into 0–100 points.
To examine the psychometric performance, we used Cronbach's alpha coefficient as an index of internal consistency for each factor. The alpha value of each factor was greater than 0.8.
Patient satisfaction
Patient satisfaction during hospitalization was measured using the Hospital Patient Satisfaction Questionnaire (HPSQ-13), 18 which was developed and validated in Japan. The HPSQ-13 has 13 items rated on a 5-point Likert scale ranging from “strongly agree” to “strongly disagree. It has three subscales: Communication, Amenity, and General Satisfaction. Subscale scores were calculated by summing item scores before converting them into 0–100 points.
Sample size
Differences were considered significant when the standardized effect size was set at 0.5 for quality of care transition. The required sample size was calculated to be 64 or 67 in each group with a significance level of (two-sided or Wilcoxon–Mann–Whitney test) α = 0.05 and statistical power 1-β=0.2. We targeted 100 participants in each group, taking dropouts into account.
Statistical analysis
Quality of care transition and HPSQ-13 scores were converted into 0–100 for each category or subscale. Descriptive analyses were used to summarize the two randomization groups. Continuous variables were compared using the Mann–Whitney test, and categorical variables were compared using the Chi-square test.
We used multilevel regression analysis that included a random effect for the clinic and covariates. We included covariates for age and sex of the patients and age, gender, and self-rated health of the respondents; all analyses were performed using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan).
Ethical considerations
We explained the purpose of the study to the participating clinics and patients with leaflets and then obtained written consent for the use of their results in this study. This study was approved by the institutional review board (IRB Number R18-009).
Results
Study samples
A total of 20 clinics were assigned to either group, but one clinic in the early care referral group was withdrawn before data collection because of technical reasons. The number of eligible patients did not reach the targeted number during the planned study period (one year), and hence it was extended by six months. Among the 19 participating clinics, 16 were enhanced home-care clinics. Figure 1 shows the flow of the participants in this study.
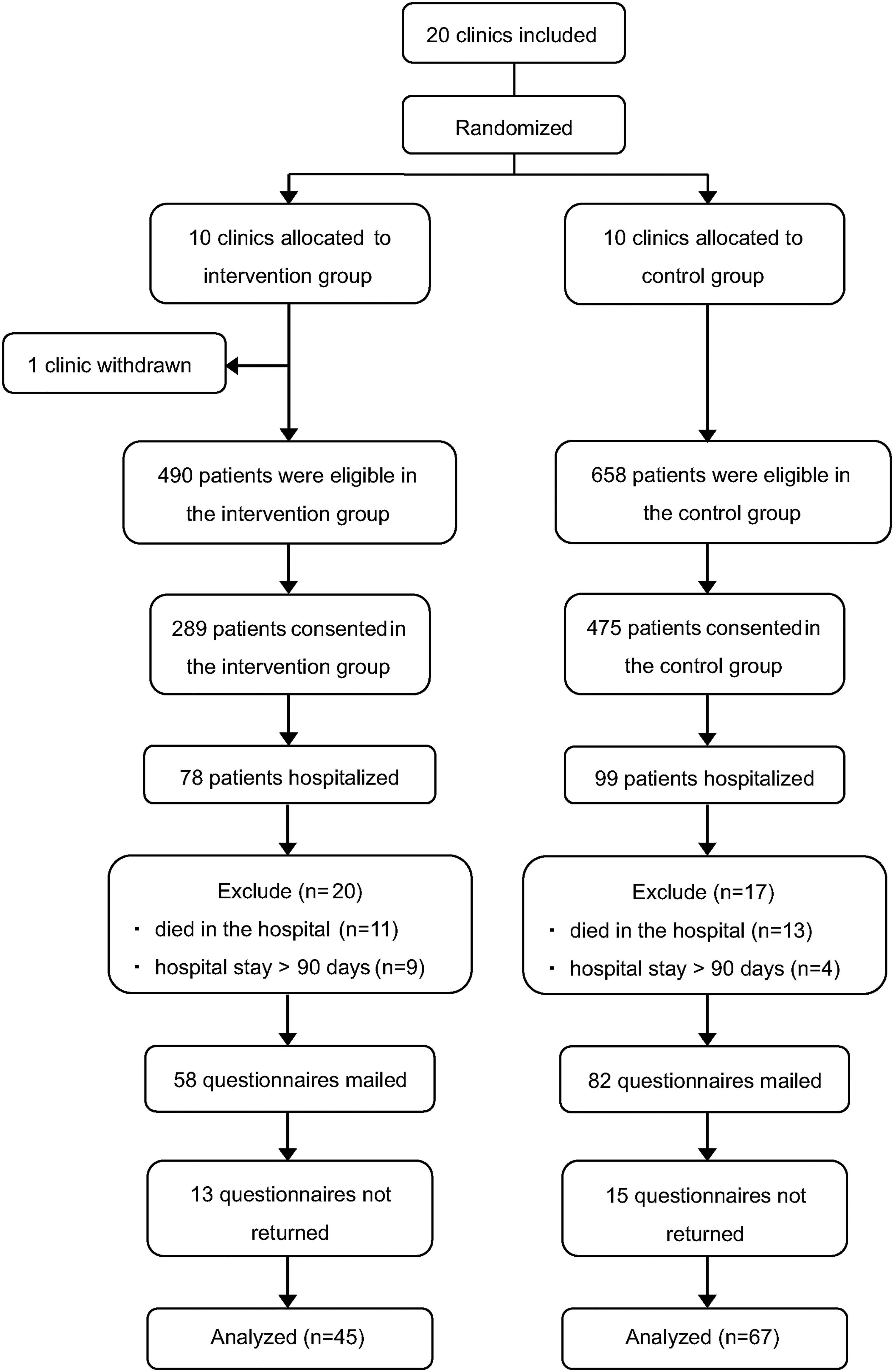
The flow of the participants in the study.
Of the ten clinics in the intervention group, one clinic did not enroll any patients. Among the 764 patients in the 18 clinics with written consent, 177 patients (78 in the early care referral group and 99 in the control group) were hospitalized during the study period.
Among the 177 patients, 24 who died during hospitalization and 13 who were hospitalized for more than 90 days were excluded from the final analysis. In addition, 28 patients who did not return the questionnaires were excluded. A total of 112 patients (response rate = 80.0%) were analyzed: 45 patients in the early care referral group (response rate = 77.6%) and 67 patients in the control group (response rate = 81.7%). The response rate did not differ statistically significantly between the groups (p = 0.67). Of the participants, 12.5% lived in care facilities upon admission. The caregivers who answered the questionnaires included 21 spouses, 68 children, and 22 others in their relationship with the patients.
The baseline characteristics of the study participants are shown in Table 1.
Patients baseline characteristics by intervention status.
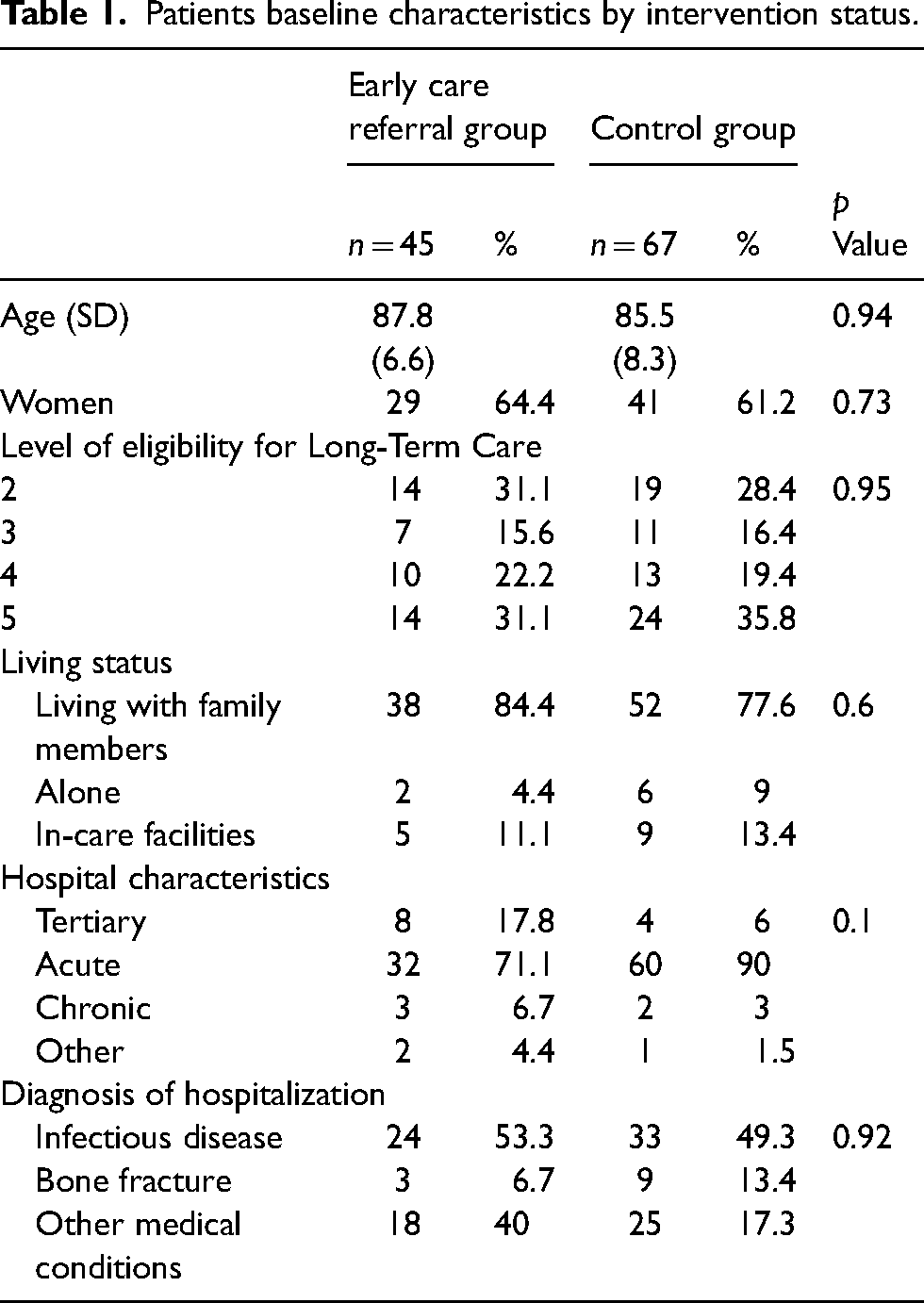
There were 29 women (64.4%) in the early care referral group with a mean age of 87.8 (standard deviation: SD 6.6) years, and 41 women (61.2%) in the control group with a mean age of 85.5 (SD 8.3) years. There were no major differences between the groups in baseline characteristics, admitted hospital characteristics, or diagnosis of hospitalization.
Quality of care transition and patient satisfaction
In the four categories of care transition quality, the mean scores were 58.4 (SD 19.2, understanding of home care situations), 59.0 (SD 18.8, preference for where to be cared), 71.3 (SD 18.2, goal for discharge), and 64.8 (SD 21.3, care coordination) out of 100 points. The mean HPSQ-13 score was 68.6 (SD 23.2, amenity), 65.3 (SD 20.0, communication), and 59.6 (SD 18.8, general) out of 100 points.
There were few differences between the early care referral group and the control group in terms of the quality of care transition score and patient satisfaction (Table 2). The adjusted mean differences in the scores between the two groups were not statistically significant.
Results of quality of care and patient satisfaction.

HPSQ-13: Hospital Patient Satisfaction Questionnaire; CI: confidence interval.
Discussion
This study found that an early transfer of information about the care situation and patients’ preferences to the hospitals at the time of admission did not impact the quality of care transition and hospital patient satisfaction of the patients and their caregivers among the frail elderly receiving home visit care.
There are several reasons why our intervention might not have been effective. Our study population was frail elderly individuals at home, whose caregivers may also be in their old age (77.7% of responders were over 60 years old). This may have affected the ability of the intervention and interactions with the hospital staff. Our intervention was an early care referral provided alongside usual medical referral letters. It did not address aspects of hospital workflows or culture, and neither altered the workflows nor the interactions of other care providers, such as care managers, who take responsibility for care planning at home in the long-term care insurance system. Considering that the score of the goal for discharge category, which needs mostly in-hospital interactions, in care transition quality was the highest, the staff patient/caregiver interactions in the hospital seemed to have worked reasonably. Comparing with goal for discharge category, the lower scores of the other three categories in care transition quality that focused on interaction, involvement, and information between the hospital staff and primary care team may reflect a lack of understanding of care transition19–21 and home care 19 among hospital staff. Education and training about care transition should be promoted to improve the quality of care transition.20,21
The current study had several limitations. First, it was unclear whether each early care information referral template contained sufficient care information. The contents described in the template were qualified and standardized, and we sent writing guidance and entry examples of those contents to each participating clinic via documents and videos. However, we could not confirm the quality of the items described by home care physicians because of patients’ privacy. Previous studies have shown that using referral templates could improve the quality of referrals, 16 although there was a wide variety of content in referral letters. 22 Second, the outcomes used in the study measured by caregivers may reflect both the patients’ and caregivers’ points of view. Since our target population was the frail elderly who were often unable to fill out the questionnaire by themselves, answering on their behalf by caregivers was inevitable and caregivers’ point of view itself was also important. Regarding outcome measures, patients’ experiences, instead of patient satisfaction, have only recently started being used as a patient outcome measure. Since there were no validated Japanese patients’ experience measurements for hospitalization at the time of this study, the HPSQ-13, which was developed and validated in Japan, seems to be a reasonable alternative. Third, the number of participants did not reach the number estimated in advance because more patients died during hospitalization than expected; a larger number of subjects may alter the results. Finally, the response rate was high in both groups. However, nonresponse bias was always present.
This study suggests that to improve the quality of care transition, other forms of information transfer or sharing as well as ordinary referrals in written form should be utilized. Considering the current burden on PCPs and hospital staff, future communication among them should be facilitated by technology, such as an interoperable electric health records interface, to reduce this burden. Promoting patients’ and caregivers’ involvement and engagement in the care transition process is also essential to improve the quality of care transition, 23 and digital health technologies including patient-accessible electronic health records may benefit patients and health care providers. 24 Further empirical studies on patient information transfer and sharing, especially elderly patient care information, in the care transition process of home to hospital and patient involvement are required.
In conclusion, there was no apparent effect of the implementation of early care information referrals on the quality of care transition, as measured by patient experiences and satisfaction during hospitalization, was evident. As the number of frail elderly patients increases, the need for information gathering and transfer increases. Studies aimed at understanding and adopting better ways of information technology and patient involvement and engagement are warranted to improve the quality of care transition.
Footnotes
Acknowledgments
The authors are grateful to all the participants and clinics that took part in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the JSPS KAKENHI, (grant number JP15K08864.).