
Abstract
Background
Studies from several jurisdictions suggest that compared to male individuals, female individuals are less likely to get placed on the waiting list for kidney transplantation and less likely to receive a transplant. However, we poorly understand where sex disparities arise within four key steps in the pathway to kidney transplant.
Objective
To measure how sex influences key steps to kidney transplantation.
Design
We conducted a population-based cohort study using linked administrative healthcare databases.
Setting
Ontario, Canada.
Patients
The study included people with kidney failure. This group comprised patients approaching the need for dialysis and those receiving maintenance dialysis from November 1, 2017, to December 31, 2021 (with follow-up to March 31, 2023). All patients had no recorded contraindications to receiving a kidney transplant.
Measurements
We assessed patient access to four key steps toward kidney transplant: (1) referral to a transplant centre for assessment; (2) they had a potential living donor contact the transplant centre for evaluation; (3) addition to the deceased donor waitlist; and (4) transplantation from a living or deceased donor. We examined each step separately.
Methods
We compared male and female individuals on the four steps in the kidney transplant process, using the incidence rate and cumulative incidence function (95% confidence interval [CI]). We used Cox proportional hazards analysis to examine the association between sex (using male as the reference group) and each transplant step, adjusting for patient characteristics. We also examined if age (<45, 45 to <55, 55 to <65, and 65 to 75 years) changed the relationship between sex and access to transplantation.
Results
We included 17,993 patients with kidney failure (11,076 male and 6,917 female individuals). Of these, 15,238 entered the cohort approaching the need for dialysis, and 2,755 entered already receiving maintenance dialysis. Over follow-up, 4,945 (32.5%) patients in the approaching the need for dialysis cohort started dialysis. Female individuals had a significantly lower rate of referral to a transplant centre for assessment than male individuals (9.35 vs 10.91 referrals per 100 person-years; adjusted hazard ratio [aHR] 0.86 [95% CI: 0.81, 0.92]). The disadvantage female individuals faced in transplant referral increased with age (age 65 to 75 years, aHR 0.73 [95% CI: 0.64, 0.84]; P-value for interaction <0.001). After we adjusted for patient characteristics, we found no significant sex-based differences for any other step in the transplant process, including living donor contact, waitlisting, or transplant. For all outcomes, a significant interaction was found between age and sex (P-value for interaction < 0.001). The kidney transplant access disadvantage for female compared to male individuals was greater in older age groups (for example, aged 65 to 75 years).
Limitations
We could not adjust for all factors influencing transplant access (for example, frailty, smoking status, and patient preference).
Conclusions
Female individuals who were likely eligible for transplant were significantly less likely to be referred to a transplant centre for assessment. This disadvantage increased with age. However, we observed no significant differences between male and female individuals for other steps in the transplant process. Further research should examine possible barriers to transplant referral among female individuals.
Introduction
The optimal treatment for most patients with kidney failure is a kidney transplant. Compared to dialysis, a kidney transplant offers prolonged survival and improved quality of life.1-3 Despite this, many barriers prevent most patients from receiving a kidney transplant, including various inequities.4-7 One factor that could impact transplant access is a patient’s sex assigned at birth. Studies have described sex differences in the incidence, progression, and outcomes of chronic kidney disease (CKD). Females receive a diagnosis of CKD more often, 8 but they are less likely to progress to kidney failure. Once diagnosed with kidney failure, evidence suggests female individuals may face disadvantages in accessing treatment, such as starting dialysis, transplant referral, waitlisting, and transplant.9-11
Previous research in both privately and publicly funded healthcare systems suggests that sex-based inequities affect access to kidney transplants.9,12-18 Of note, prior studies may have inconsistently used the terminology “female/male” versus “women/men” to describe sex differences in transplant access. This study uses the terms “female” and “male” throughout to describe sex differences.
A recent Canadian cohort study showed female individuals with kidney failure were much less likely to receive a transplant. 12 In the United States, female individuals are less likely than male individuals to receive a referral for a transplant evaluation, complete the workup, be waitlisted, engage living donors, or receive a transplant.14,15,19,20 Recent evidence from Nova Scotia, Canada, also demonstrated lower referral and transplant rates among female individuals, especially in older age groups. 16 Comorbidities, sensitization, or age do not fully explain these disparities. These results suggest that systemic and sex-based barriers exist in care processes.13,15
A comprehensive understanding of sex-based barriers to kidney transplant remains essential for developing effective solutions, as prior studies have notable limitations. First, few previous studies have examined sex-based disparities across four distinct steps in the transplant process, with no studies examining contact by a potential living donor with the transplant centre to initiate an evaluation. Prior work suggests that each transplant step presents a unique set of barriers, 21 which may necessitate tailored solutions. Second, few studies have examined sex-based disparities restricting to individuals who are likely eligible for transplant. Third, limited studies have included patients approaching the need for dialysis, with most previous studies restricting to the dialysis population. Therefore, we conducted this study to evaluate sex differences in the rates of key steps along the pathway to kidney transplantation: (1) referral to a transplant centre for assessment, (2) contact by a potential living donor with the transplant centre to initiate evaluation, (3) placement on the deceased-donor waitlist, and (4) receipt of a kidney transplant from a living or deceased donor. We also assessed whether age modifies the association between sex and transplant access, the rate of steps completed toward receiving a transplant, and the median time to complete these steps.
Methods
Design and Setting
We used linked administrative healthcare databases from Ontario, Canada held at ICES (ices.on.ca/) to conduct a population-based cohort study. These datasets were linked using unique encoded identifiers and analyzed at ICES, which is an independent, non-profit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement. The use of data in this project was authorized under section 45 of Ontario’s Personal Health Information Protection Act, which does not require review by a Research Ethics Board. We have reported this work using the Reporting of studies Conducted using Observational Routinely-collected health Data (RECORD) Statement (Supplemental Table 1). 22
Data Sources
We used several linked administrative databases detailed in Supplemental Table 2. Key data sources included the following: (1) Ontario Health Information Plan, which identifies physician billings and diagnoses; (2) Ontario Laboratories Information System, which provides serum creatinine and urine albumin-to-creatinine ratio data to identify patients approaching the need for dialysis; (3) Ontario Renal Reporting System, which identifies patients receiving maintenance dialysis; (4) Registered Persons Database, which determines vital status and sex; (5) Canadian Institute for Health Information Discharge Abstract Database, which records hospitalizations; and (6) Trillium Gift of Life Network, which captures data on the four key steps toward kidney transplantation.
Study Population
Using data from November 1, 2017, to December 31, 2021, we assembled cohorts of patients approaching the need for dialysis and patients receiving maintenance dialysis. We included the approaching the need for dialysis cohort because these patients can take steps towards transplantation, though transplantation at this stage is uncommon. The approaching the need for dialysis and maintenance dialysis cohorts were not mutually exclusive. When patients in the approaching the need for dialysis group started maintenance dialysis, we censored them and began attributing their person-time to the maintenance dialysis cohort (if they remained eligible for inclusion).
Approaching the Need for Dialysis Cohort
We identified adult patients who were approaching the need for dialysis in whom a transplant work-up would be reasonable, defined as satisfying at least one of the following kidney function criteria: (1) two outpatient estimated glomerular filtration estimates (eGFR) < 15 mL/min/1.73 m2 (estimated using the 2021 CKD-EPI equation without race) 23 or (2) two 2-year Kidney Failure Risk Equation measures ≥25% (KFRE, estimates the 2-year probability of kidney failure). 24 The two measures of eGFR or KFRE had to be separated by at least 90 days but no more than 365 days. We set the cohort entry date as the date the patient met the kidney function criteria (i.e., date of the second qualifying eGFR or KFRE).
Maintenance Dialysis Cohort
We included incident adults (aged ≥ 18 years) on maintenance dialysis, either at home or in centre. To exclude patients on acute dialysis, we required at least 90 days on dialysis. The cohort entry date was 90 days after the start of dialysis.
Exclusion Criteria
For both the approaching the need for dialysis and maintenance dialysis cohorts, we excluded individuals with any of the characteristics that, in a previous study, were found to preclude transplantation in Ontario in more than 97% of cases: age greater than 75 years, end-stage kidney disease-modified Charlson comorbidity index score ≥7 (a higher score represents greater comorbidity), use of home oxygen, dementia, residence in long-term care, use of at least one physician house call in the prior year, or a history of cancer in the last several years (e.g., lung, lymphoma, cervical, colorectal, liver, active multiple myeloma, and bladder cancer). 25 This created a cohort of patients who were likely eligible for transplant (i.e., no recorded contraindications to transplant).
Exposure
Our study exposure was the patients’ sex assigned at birth (male or female) at the time of cohort entry. The Registered Persons Database sex variable represents the most recent recorded sex designation indicated on an individual’s Ontario health card, which may differ from their sex assigned at birth if there have been formal changes in sex designation. In our cohort, we found no instances of recorded changes in sex designation. Therefore, we likely exclusively captured sex assigned at birth in our study.
Outcomes
Primary Outcome: Steps Completed Toward Receiving a Kidney Transplant
Our outcome was the completion rate of key steps towards kidney transplantation: (1) patient referral to a transplant centre for assessment (i.e., referral); (2) their potential living donor contacts the transplant centre for evaluation (i.e., living donor contact); (3) addition of the patient to the deceased donor waitlist (i.e., waitlisting); and (4) kidney transplantation from a living or deceased donor (i.e., transplant). We examined each step separately.
For the outcome of referral, we created a sub-cohort excluding patients who had been referred or waitlisted prior to the cohort entry date, ensuring patients were eligible for the outcome (i.e., patients are generally only referred once, and to be waitlisted, an individual must first be referred). Similarly, we created another sub-cohort for the waitlisting outcome by excluding patients who had been waitlisted prior to the cohort entry date.
Secondary Outcomes
In the approaching the need for dialysis cohort, we examined the outcome of pre-emptive transplant, which was defined as receipt of a living or deceased donor kidney transplant with no evidence of maintenance dialysis for 90 days or more prior to the transplant. We also examined the rate of steps completed towards kidney transplantation per 100 person-years (a maximum of four steps could be completed per individual).26,27 Patients can start in any step (e.g., referral) except kidney transplant and each step can be completed only once. Lastly, we examined the time required to complete key steps in the kidney transplant process (e.g., the time from starting maintenance dialysis to referral), with details provided in Supplemental Table 3.
Statistical Analysis
We reported continuous variables as medians (25th, 75th percentiles) and categorical variables as proportions. For each outcome, we reported the incidence rate per 100 person-years (95% confidence interval). We censored individuals at death, loss to follow-up (which is rare), study conclusion (March 31, 2023), or development of any of the previously mentioned contraindications to transplantation, except when they reached an age greater than 75 years. For each step in the kidney transplant process, we also calculated the cumulative incidence using the cumulative incidence function (non-parametric Aalen-Johansen estimator), which accounts for the competing risks of death and the development of a recorded contraindication to transplant. 28 We used the associated Gray’s test to determine whether there is a statistically significant difference in the cumulative incidence of outcomes between male and female individuals.
To examine the relationship between patient sex and steps achieved towards kidney transplantation, we used the Cox proportional hazards model, adjusting for the following variables: age (per 5-year increase), diabetes, end-stage kidney disease Charlson comorbidity index, neighbourhood income quintile, treatment modality (approaching the need for dialysis, hemodialysis, other dialysis modality [e.g., peritoneal dialysis]), body mass index (<18.5, 18.5 to <25, 25 to <30, 30 to <35, ≥35 kg/m2, missing), cardiovascular disease (yes versus no and was defined as: abdominal aortic aneurysm or bypass, stroke or transient ischemic attack, coronary artery angioplasty or bypass surgery, coronary artery disease with angina, congestive heart failure, myocardial infarction, or peripheral artery disease), and year of cohort entry (2017, 2018, 2019, 2020, 2021). The proportional hazard assumption was tested using weighted Schoenfeld residuals. To investigate whether the relationship between sex and access to transplantation was modified by age, we repeated the primary outcome analyses in sub-groups divided into the following age categories: <45, 45 to <55, 55 to <65, and 65 to 75 years, reporting the interaction P-value using the Wald Chi-square test. In an additional analysis, we used the Fine and Gray model to compute subdistribution hazard ratios (sdHR), accounting for competing risks and adjusting for the same variables described above.
Baseline information was complete with the following exceptions: income quintile (<0.5% missing; imputed quintile 3), rural residence (<0.5% missing; imputed urban residence), KFRE (10.3% missing in the approaching the need for dialysis cohort; kept missing category), cause of kidney failure (0.4% missing in the dialysis cohort, kept missing category), and body mass index (BMI) (14.4% missing; kept missing category). Our outcome data was over 98% complete, with the imputation of missing data being previously described. 26 The most common reason for imputing outcome data was when we identified a step towards transplant without the required preceding step. For example, in Ontario, a patient cannot be added to the waitlist without first being referred for transplant. Therefore, when we identified patients who were waitlisted without a recorded referral date, we imputed the referral date.
We defined a 2-sided P-value <0.05 as statistical significance. Confidence interval widths were not adjusted for multiple testing. We conducted all analyses using SAS version 9.4 (SAS Institute, Cary, NC).
Additional Analysis
Given it is not always appropriate in Ontario to refer patients who have not yet started dialysis, as the patient may spend several years on the deceased donor waitlist (pre-emptive deceased donor transplants are relatively uncommon), we repeated our primary analysis in a sub-cohort of patients receiving maintenance dialysis.
Post-Hoc Analysis
To better understand the effect of sex on steps completed toward receiving a kidney transplant, we conducted an additional analysis using the same inclusion and exclusion criteria described above, but we restricted to patients who had been referred for transplant and examined the incidence rate of waitlisting, kidney transplant (living and deceased) and living donor transplant. We performed another analysis examining the incidence rate of deceased donor kidney transplant among individuals who made it to the referral and waitlisting stage.
Results
Baseline Characteristics
Baseline Characteristics of Adults With Kidney Failure Presented by Sex

Data are presented as n (%) or median (25th, 75th percentile).
aSD is the standardized difference for male vs female individuals. Standardized differences measure the difference between groups divided by the pooled standard deviation; a value >10% is a meaningful difference between male and female individuals. Bold standard differences denote a meaningful difference.
bIncome presented as quintiles of average neighborhood income. Income was categorized into fifths of the average neighborhood income, with the first quintile representing the lowest income and the fifth quintile representing the highest income. Those with missing income status (0.3% of the cohort) were assigned a value of the third quintile.
cRurality: Population less than 10,000. Those with missing residence status (0.1% of the cohort) were assigned to the value of urban residence.
dEstimated glomerular filtration rate value closest to cohort entry date. This metric was only measured for those who were approaching the need for dialysis
eEstimated 2-year risk of kidney failure within 1-year of the cohort entry date (if multiple values the most recent one was selected). This metric was only measured for those who were approaching the need for dialysis
fCardiovascular disease defined as a composite of abdominal aortic aneurysm or bypass, stroke or transient ischemic attack, coronary artery angioplasty or bypass surgery, coronary artery disease with angina, congestive heart failure, myocardial infarction, or peripheral artery disease.
gA higher Charlson comorbidity index score indicates greater comorbidity.
*In accordance with ICES privacy policies, cell sizes less than or equal to five cannot be reported; this includes being able to calculate small cells based on other information provided. Therefore, data is presented as ranges.
Patient Follow-Up
For the overall cohort, 2,303 (12.8%) received a transplant, 3,816 (21.1%) died, 3,082 (17.1%) developed a recorded contraindication to transplant, 8,682 (48.3%) reached the end of follow-up with no event, and 110 (0.6%) were lost to follow-up. Individuals were followed for a median of 3.2 years (1.9, 4.9). Follow-up duration and the proportion of follow-up events were similar between male and female individuals.
Primary Outcome
Female individuals had a lower cumulative incidence of referral compared to male individuals (P-value Gray’s test <0.001) (Figure 1A). For example, the 5-year cumulative incidence of referral was 27.7% (95% CI: 26.5, 28.9) in female individuals compared to 31.6% (95% CI: 30.6, 32.6) in male individuals. In the unadjusted and adjusted Cox proportional hazards models, we found female individuals had a significantly lower rate of referral compared to male individuals. For example, after adjusting for patient characteristics, female individuals had a 14% lower rate of referral compared to male individuals (adjusted hazard ratio [aHR] 0.86, 95% CI: 0.81, 0.92) (Table 2). To further explore this finding, we conducted a post-hoc analysis restricted to patients who had been referred for transplant assessment. Within this group of 4,173 patients, we found that, compared to male individuals, female individuals who had been referred were more likely to be waitlisted (aHR 1.16, 95% CI 1.03 to 1.30) but were no more likely to be transplanted (aHR 1.09, 0.96 to 1.24) (Supplemental Table 4). (A) Cumulative incidence of kidney transplant referrals, in patients with kidney failure (i.e., approaching the need for dialysis or receiving maintenance dialysis), displayed by males vs females. (B) Cumulative incidence of living donor contacts, in patients with kidney failure (i.e., approaching the need for dialysis or receiving maintenance dialysis), displayed by males vs females Outcome Events Among Male Versus Female Individuals With Kidney Failure Bold hazard ratios denote statistical significance. ¶Adjusted for the following variables: age (per 5-year increase), diabetes (yes vs no), Charlson comorbidity index (end-stage kidney disease modified, continuous), neighbourhood income quintile (1,2,3,4,5), modality (approaching the need for dialysis, hemodialysis, home dialysis modality), body mass index (<18.5, 18.5-<25, 25.0-<30, 30-<35, ≥35 kg/m2, missing), cardiovascular disease (yes vs no, including: stroke or transient ischemic attack, coronary artery angioplasty or bypass surgery, coronary artery disease with angina, congestive heart failure, myocardial infarction, peripheral artery disease), year of cohort entry (2017, 2018, 2019, 2020, 2021). ¥For the pre-emptive transplant outcome, the cohort was restricted to individuals who had no evidence of maintenance dialysis prior to entering the cohort and patients were censored when they initiated dialysis during follow-up.

Female individuals had a higher cumulative incidence of living donor contacts compared to male individuals (P-value, Gray’s test = 0.0285) (Figure 1B). For example, the 5-year cumulative incidence of living donor contacts was 14.2% (95% CI: 13.4, 15.1) in female individuals compared to 13.1% (95% CI: 12.5, 13.8) in male individuals. However, no significant sex-based differences were found in the unadjusted and adjusted Cox proportional hazards models (Table 2). The incidence rate and cumulative incidence for waitlisting and transplant (including living and deceased donor transplant, and pre-emptive transplant) were similar between male and female individuals (Figure 2A–D, Table 2). For example, the 5-year cumulative incidence of kidney transplant in male individuals was 14.5% (95% CI: 13.8, 15.3), and in female individuals, it was 14.1% (95% CI: 13.2, 15.0) (Table 3). Similar results for waitlisting and transplant were observed in both the unadjusted and adjusted Cox proportional hazard analyses (Table 2). For all steps in the transplant process, we found comparable results when comparing our Cox proportional hazards model to the Fine and Gray model (Supplemental Table 5). (A) Cumulative incidence of being added to the deceased donor waitlist in patients with kidney failure (i.e., approaching the need for dialysis or receiving maintenance dialysis), displayed by males vs females. (B) Cumulative incidence of kidney transplant (living and deceased donor kidney transplant), in patients with kidney failure, displayed by males vs females (C) Cumulative incidence of kidney transplantation from a deceased donor in patients with kidney failure, displayed by males vs females (D) Cumulative incidence of kidney transplantation from a living donor in patients with kidney failure, displayed by males vs females Cumulative Incidence Functions (CIF) for the Total Population, Male and Female Individuals

Similar results were also found when the patient population was restricted to individuals receiving maintenance dialysis (Supplemental Table 6). However, after restricting the analysis to the maintenance dialysis population, female individuals had an even lower rate of referrals compared to male individuals, with female individuals having a 22% reduced rate of referral (aHR 0.78, 95% CI: 0.71, 0.85). Unlike what was observed in the entire kidney failure cohort, when restricting the analysis to the dialysis cohort, female individuals had a higher rate of living donor kidney transplant compared to male individuals; however, after adjusting for patient characteristics, this difference did not reach statistical significance.
Additional Analyses
Adjusted Hazard Ratios (HRs) for Female vs. Male Individuals Across Age Groups for Key Steps Toward Kidney Transplantation
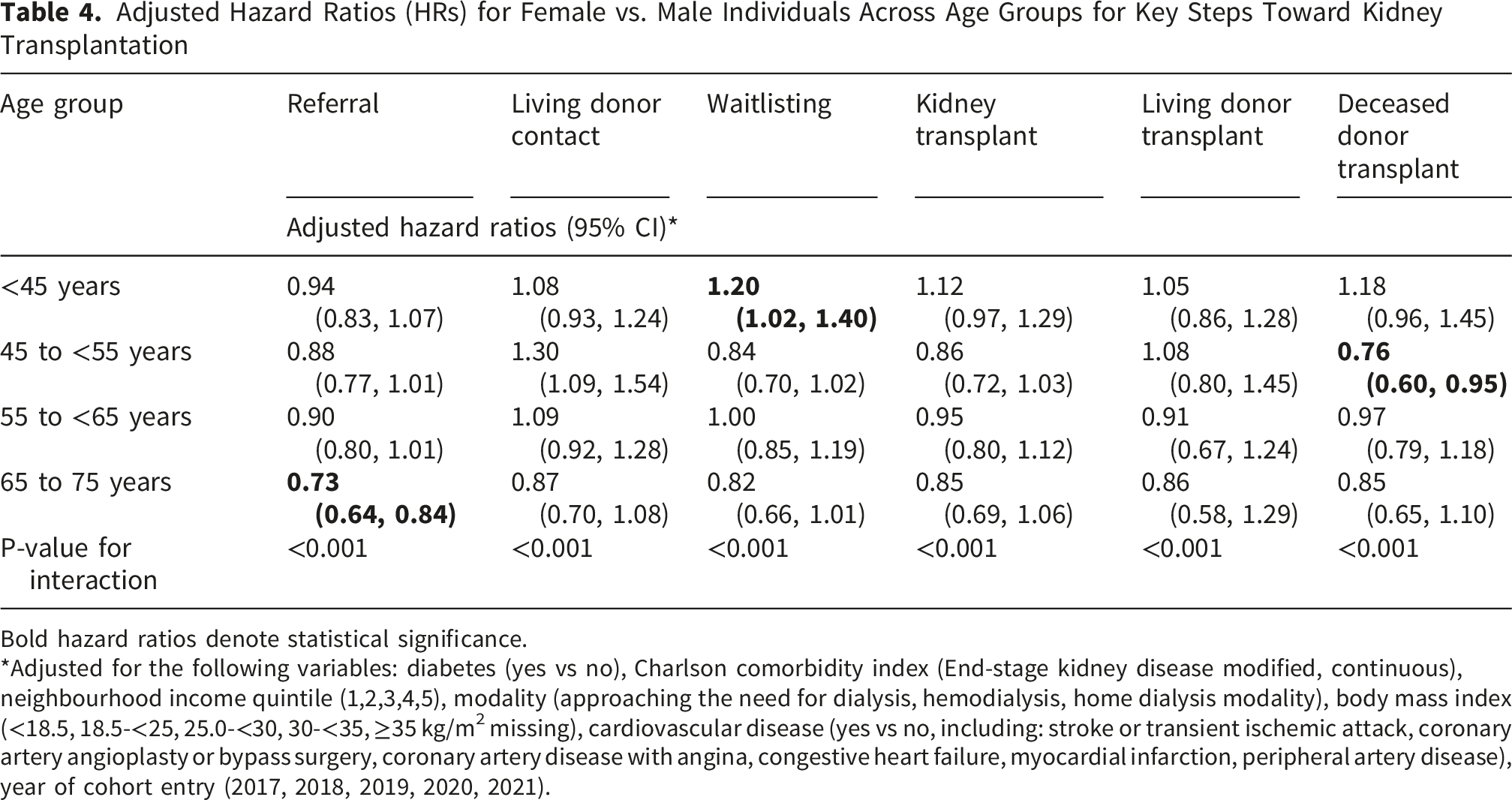
Bold hazard ratios denote statistical significance.
*Adjusted for the following variables: diabetes (yes vs no), Charlson comorbidity index (End-stage kidney disease modified, continuous), neighbourhood income quintile (1,2,3,4,5), modality (approaching the need for dialysis, hemodialysis, home dialysis modality), body mass index (<18.5, 18.5-<25, 25.0-<30, 30-<35, ≥35 kg/m2 missing), cardiovascular disease (yes vs no, including: stroke or transient ischemic attack, coronary artery angioplasty or bypass surgery, coronary artery disease with angina, congestive heart failure, myocardial infarction, peripheral artery disease), year of cohort entry (2017, 2018, 2019, 2020, 2021).
Time to Complete Key Steps in the Kidney Transplant Process by sex
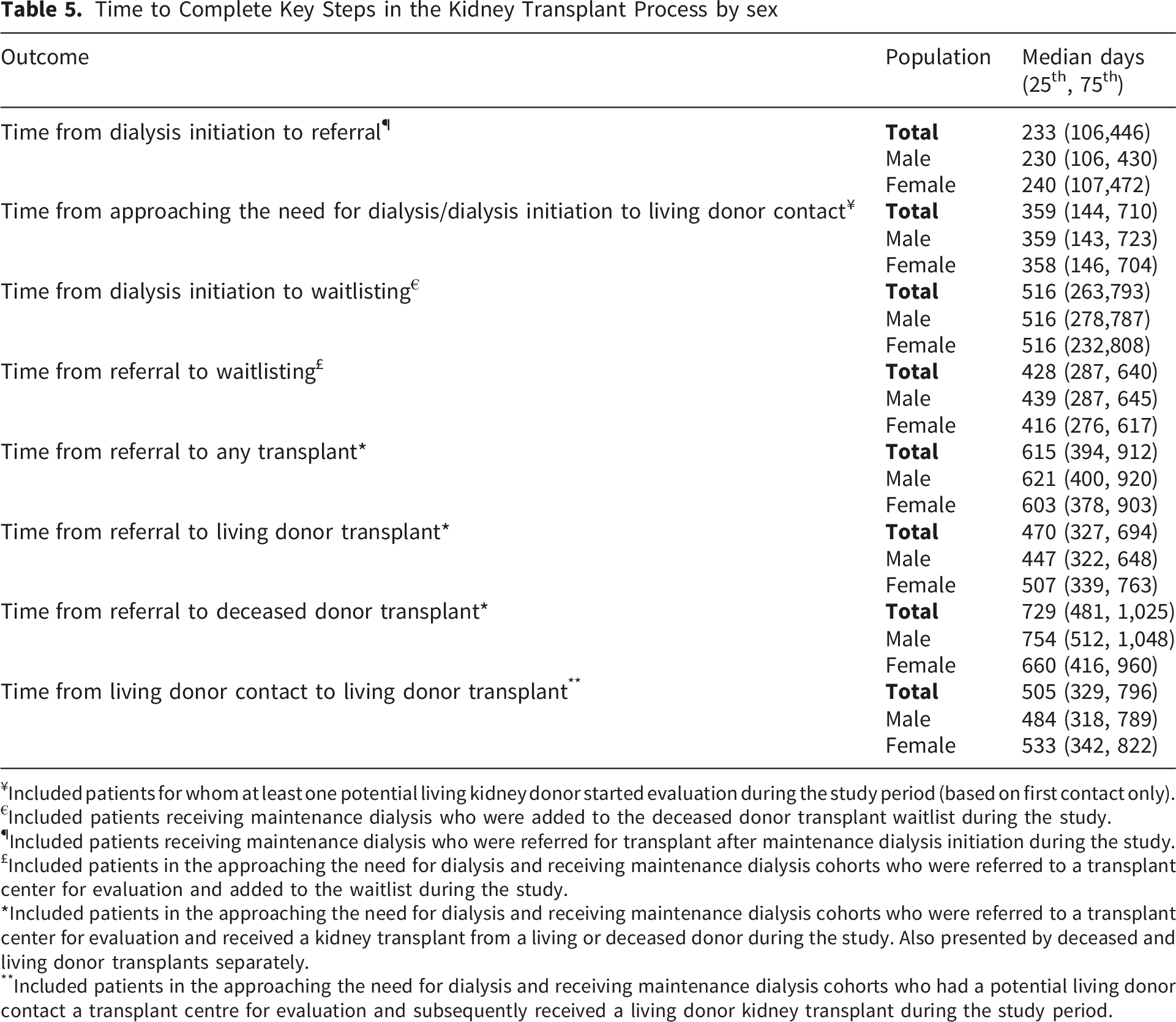
¥Included patients for whom at least one potential living kidney donor started evaluation during the study period (based on first contact only).
€Included patients receiving maintenance dialysis who were added to the deceased donor transplant waitlist during the study.
¶Included patients receiving maintenance dialysis who were referred for transplant after maintenance dialysis initiation during the study.
£Included patients in the approaching the need for dialysis and receiving maintenance dialysis cohorts who were referred to a transplant center for evaluation and added to the waitlist during the study.
*Included patients in the approaching the need for dialysis and receiving maintenance dialysis cohorts who were referred to a transplant center for evaluation and received a kidney transplant from a living or deceased donor during the study. Also presented by deceased and living donor transplants separately.
**Included patients in the approaching the need for dialysis and receiving maintenance dialysis cohorts who had a potential living donor contact a transplant centre for evaluation and subsequently received a living donor kidney transplant during the study period.
Discussion
In this population-based cohort study of patients who were likely eligible for kidney transplantation, we found that female individuals were significantly less likely to be referred for transplant assessment compared to male individuals. We found that once referred, female individuals were at least as likely as male individuals to be placed on the waiting list and to ultimately receive a transplant. The disadvantage female individuals face in referral for transplant assessment was augmented by increasing age, and although it was only the referral step for which we observed significantly less access in female individuals, in all steps towards transplantation, we observed a greater disadvantage for female individuals compared to male individuals in the oldest age group (aged 65 to 75 years). Our results suggest that in a universal healthcare system, females, particularly older female individuals, are disadvantaged in reaching the first crucial step to receiving a kidney transplant.
Similar to previous studies, we found that female individuals were significantly less likely to be referred for transplant compared to male individuals.16,29-31 Several potential biological and sociocultural explanations have been identified in the literature. Female individuals with kidney failure have consistently been shown to experience fewer transplant-related discussions, 32 and they may also encounter sex-based clinical and social barriers, including higher rates of pregnancy-related sensitization, greater caregiver responsibilities, and lower self-advocacy. Additionally, systemic factors such as implicit bias, limited attention to transplant eligibility in women with complex social circumstances, and concerns regarding surgical risk may contribute to lower referral rates.19,33-35 Another potential explanation for the reduced number of transplant referrals in female individuals is that older female individuals may be more likely to be frail or perceived as frail compared to male individuals of a similar age and health status.36,37 Although frailty is not listed as a contraindication to kidney transplant in Ontario, there are some contraindications listed in the guidelines that could be influenced by frailty status, including a relative listing contraindication for “age and functional status” which indicates that if a transplant candidate is deemed not to have a reasonable probability of surviving beyond the current wait time for transplant they should not be listed. 38
Unlike other studies, we did not find that female individuals were significantly less likely to be waitlisted and transplanted compared to male individuals.12,15,16 A potential explanation for this is that Ontario has a rigorous referral process, which requires patients to complete several medical tests (e.g., echocardiogram, chest x-ray, renal ultrasound). 39 This contrasts with the process in the United States, where self-referral is allowed. 40 It could be that female individuals who complete the referral process in our study represent a unique group of individuals who are more likely to be waitlisted. Given the number of tests required for a patient to be referred for transplant, clinicians may only refer patients for which they have high confidence are healthy enough to be waitlisted and subsequently transplanted. Furthermore, the patient must be highly motivated to complete all the tests required for referral, likely representing a unique patient group. This hypothesis is somewhat supported, as our study found that when we restricted our cohort to patients referred for transplant, female individuals were more likely to be waitlisted compared to male individuals. Female individuals who are referred may represent a healthier subset of the population who have a higher chance of receiving a transplant, which could result in no difference in transplant rates between male and female individuals. Future interventions in Ontario should focus on improving equitable access to kidney transplant referral among female individuals.
Like previous studies,14,16,41 we found that female individuals in the oldest age group were less likely to access each step in the transplant process, although this difference did not always reach statistical significance. For all four steps in the transplant process, we found a significant interaction between sex and age. As described above, a potential explanation could be that older female individuals are more likely to be perceived by physicians or themselves to be frail and not suitable for transplant.14,16,41 Compared to male individuals, older female individuals may also have a lower socioeconomic status, 42 lower educational attainment, 43 and are more likely to live alone.44,45 All of which may contribute to a lower likelihood of transplant.
Our findings highlight the need for qualitative research to understand the barriers that female individuals, particularly older female individuals, face in being referred for transplant. Interventions should then be designed to address the barriers. Our findings also highlight the need to present quality indicators for access to kidney transplant at a provincial level, stratified by sex assigned at birth and age, to monitor disparities. Ontario has a provincial priority to improve access to kidney transplants. 46 However, in addition to evaluating whether access to kidney transplant is improving in the province, we also need to monitor access presented by different demographics, including sex, age, and race.
Our study has several strengths. First, we conducted a multicentre study that included all six adult transplant centres in Canada’s most populous province and used a contemporary patient cohort. Second, we examined four distinct steps along the pathway to kidney transplantation, enabling a comprehensive assessment of access to transplant care. To our knowledge, we are the only study to include the step of a potential living donor contacting the transplant centre for evaluation. This is an important step, as it marks the beginning of the process toward a patient receiving a living donor transplant. Third, our cohort was restricted to individuals without recorded contraindications to transplantation, improving baseline comparability between male and female individuals. Fourth, we included patients approaching the need for dialysis, with most previous studies restricting to the dialysis population.
There are limitations to our work. First, although we attempted to restrict our study population to individuals who were likely eligible for transplant, in our administrative databases we do not have access to all factors that influence whether a patient is worked up for transplant, including patient preference, certain life style factors (e.g., social support, smoking status), and some comorbidities/medical conditions that contribute to the complexity of whether a physician deems a patient suitable for transplant (e.g., frailty status). Second, our administrative databases do not have access to patient gender, thus we were only able to report on sex assigned at birth. Additionally, the sex variable was derived from administrative data associated with the Ontario health card, which may inconsistently capture sex assigned at birth versus gender identity. Third, this work was completed in Ontario and may not generalize to other jurisdictions. Last, our administrative data does not capture transplant centre-level variation in referral and waitlisting practices.
In conclusion, our study suggests that female individuals are less likely than males to be referred to a transplant centre for assessment, the first crucial step in accessing a transplant. We should continue to monitor access to kidney transplantation by sex and age, identify sex- and age-related barriers along the transplant pathway, develop and evaluate targeted interventions to address these barriers, and promote equitable access to transplantation.
Supplemental Material
Supplemental Material - Association Between Sex and Kidney Transplant Referral, Living Donor Contacts, Waitlisting and Kidney Transplant: A Population-Based Cohort Study
Supplemental Material for Association Between Sex and Kidney Transplant Referral, Living Donor Contacts, Waitlisting and Kidney Transplant: A Population-Based Cohort Study by Kyla L. Naylor, Natalie Zitoun, Graham Smith, Jaffa Romain1, Amit X. Garg, Kate Roberston-Hogg, Gregory Knoll, S. Joseph Kim, Seychelle Yoahnna and Matthew Weir in Canadian Journal of Kidney Health and Disease.
Footnotes
Acknowledgements
K.L.N. is supported by a Canadian Institutes of Health Research Health System Impact Embedded Early Career Researcher Award. A.X.G is supported by the Kay Family Chair in Transformational Kidney Care. M.A.W is supported by the Adam Linton Chair in Kidney Health Analytics. This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). Parts of this material are based on data and/or information compiled and provided by the Canadian Institute for Health Information, the Ontario Ministry of Health, and Ontario Health. The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred. This document used data adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation, and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File, which contains data copied under license from Canada Post Corporation and Statistics Canada. The author(s) acknowledge that the data used in this study were provided by the Trillium Gift of Life Network (Ontario Health), [2023], Toronto, Ontario. The researcher’s interpretations and statements in this publication are those of the researcher only and not those of Trillium Gift of Life Network (Ontario Health).
Ethical Considerations
ICES is an independent, non-profit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze healthcare and demographic data, without consent, for health system evaluation and improvement. The use of data in this project was authorized under section 45 of Ontario’s Personal Health Information Protection Act, which does not require review by a Research Ethics Board.
Consent for Publication
Consent for publication was obtained from all authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from the Canadian Institutes of Health Research (Funding Reference Number 178016).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset from this study is held securely in coded form at ICES. While legal data sharing agreements between ICES and data providers (e.g., healthcare organizations and government) prohibit ICES from making the dataset publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at www.ices.on.ca/DAS (email:
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.