
Abstract
Case summary
A 15-year-old, male neutered domestic shorthair cat presented with anuria due to urethral obstruction. The cat had a history of several urinary and systemic comorbidities at the time of presentation. Velagliflozin therapy had been started recently after a new diagnosis of diabetes mellitus. A mixed urinary tract infection caused by Escherichia coli and Candida albicans was diagnosed. The cat was initially managed with urinary catheterisation, antibiotics and antifungals, showing a favourable response. However, recurrent urinary obstruction occurred, requiring multiple urinary catheterisations. Approximately 2 weeks after presentation, urethral rupture was diagnosed using contrast urography. Urethrostomy was declined and the cat was ultimately euthanased.
Relevance and novel information
The most frequent adverse effect reported in human patients treated with sodium–glucose cotransporter 2 inhibitors (SGLT2is) is mycotic genitourinary infection, particularly caused by C albicans. Several risk factors have been identified in humans; however, this association has not been previously demonstrated in cats. This is the first report describing a urinary tract infection caused by C albicans in a cat treated with velagliflozin. These findings emphasise the importance of monitoring for this potential adverse effect in cats receiving SGLT2is, particularly in those with comorbidities, and encourage further evaluation of SGLT2is as a putative risk factor for C albicans urinary tract infections in these patients.
Introduction
Sodium–glucose cotransporter 2 (SGLT2) inhibitors (SGLT2is) are oral antihyperglycaemic agents used for the management of type 2 diabetes mellitus (DM) in human patients. 1 More recently, velagliflozin and bexagliflozin have demonstrated efficacy in cats.2–4 By competitively inhibiting SGLT2, expressed in proximal renal tubules and responsible for reabsorbing approximately 90% of filtered glucose, these drugs increase urinary glucose excretion and lower blood glucose in patients with DM. 5
In human medicine, glucosuria has been recognised as a potential risk factor for genitourinary infections (GUIs),6–9 comprising both urinary tract infections (UTIs) and genital infections. 10 The most common SGLT2i-related complication is mycotic GUI primarily caused by Candida species, particularly Candida albicans, whose growth is promoted by glucosuria. 7 The most frequently reported adverse effects of SGLT2is in cats include euglycaemic diabetic ketoacidosis and gastrointestinal issues.2–5 This report describes the first documented case of C albicans UTI in a cat receiving velagliflozin treatment.
Case description
A 15-year-old, male neutered domestic shorthair cat was initially presented to the Internal Medicine Department at AniCura Ars Veterinària Hospital Veterinari in Barcelona for evaluation of multiple conditions previously diagnosed at another veterinary clinic, including a low-grade alimentary lymphoma with hepatic involvement and concurrent proteinuric, non-hypertensive chronic kidney disease (International Renal Interest Society stage 2). The cat also had a prior history of multiple episodes of non-obstructive feline idiopathic cystitis (FIC). The patient was receiving dexamethasone (0.2 mg/kg q24h), chlorambucil (2.2 mg/m2 three times per week) and benazepril (1 mg/kg q24h). Chlorambucil was replaced with cyclophosphamide (171 mg/m2 every 2 weeks) before presentation at our hospital because of suspected lymphoma progression. However, sterile haemorrhagic cystitis developed, prompting discontinuation of cyclophosphamide and reinitiation of chlorambucil.
At initial presentation in our hospital, a left forelimb abscess was noted. The cat lived indoors with another cat, and a bite wound was considered the most likely cause, exacerbated by immunosuppression associated with chemotherapy. Wound culture showed a mixed infection of Staphylococcus aureus, Streptococcus canis and Staphylococcus felis. Treatment with amoxicillin–clavulanate (22 mg/kg q12h) was initiated for 2 months, showing an initial good response, although the abscess was not fully resolved. Marbofloxacin (3 mg/kg q24h) was introduced after antibiotic susceptibility testing, while chemotherapy was continued.
The cat developed DM 3 months after initial presentation following Agreeing Language in Veterinary Endocrinology criteria of repeated blood glucose between 126 and 270 mg/dl, with classic clinical signs of hyperglycaemia and more than two episodes of glucosuria on naturally voided samples acquired at home after more than 48 h of a stressful event. 11 The most prominent clinical signs were weight loss and polyphagia, whereas polyuria and polydipsia were mild. At that time, the cat’s blood glucose concentration was 262 mg/dl (reference interval [RI] 74–159). Fructosamine was measured 2 months earlier and was at the upper limit of the RI (276 μmol/l, RI 137–286). However, it was not re-evaluated when clinical signs suggestive of DM developed owing to financial constraints. Insulin was initially recommended but declined by the caregiver because of administration difficulties and concerns about hypoglycaemia.
Velagliflozin (1 mg/kg q24h) was initiated after informing the caregivers of its off-label use and potential risks. Concomitant treatments were maintained, although dexamethasone dose was reduced (from 0.2 to 0.1 mg/kg q24h). DM-associated clinical signs remarkably improved but did not fully resolve during velagliflozin treatment. Notably, euglycaemia was achieved and glucosuria increased compared with baseline after treatment initiation.
After 19 days of velagliflozin treatment, the cat presented to the emergency service with a 72-h history of dysuria, stranguria and pollakiuria, which had progressed to anuria over the preceding 24 h. Velagliflozin had been discontinued by the caregivers 3 days before presentation. On admission, pale mucous membranes, a grade 3/6 systolic murmur and a distended, painful bladder were noted. Laboratory results showed normocytic, normochromic, regenerative anaemia (haematocrit 19.4%, RI 30.3–52.3), neutrophilic leukocytosis (24.07 × 10³/µl, RI 2.87–17.02; with neutrophils 20.79 × 103/µl, RI 2.30–10.29), creatinine 3.97 mg/dl (RI 0.30–2.10), blood urea nitrogen 116.40 mg/dl (RI 20.00–92.00) and hypochloraemia 110 mmol/l (RI 112–129). Blood glucose concentration was 134 mg/dl (RI 74–159) (Table 1). Remarkably, euglycaemia was maintained during hospitalisation. Blood gas was normal, with beta-hydroxybutyrate 0.1 mmol/l (RI <2.4). 12 Urinalysis revealed a specific gravity of 1.013, pH 6, blood 3+, protein 2+, and abundant rods and fungal hyphae with spores on sediment examination (Table 2, Figure 1). Urine culture identified Escherichia coli and C albicans (Table 3).
Haematological and serum biochemical results on presentation from the cat with urinary obstruction receiving velagliflozin

Values outside the reference interval (RI) are highlighted in bold
Urine analysis results on presentation from the cat with urinary obstruction receiving velagliflozin
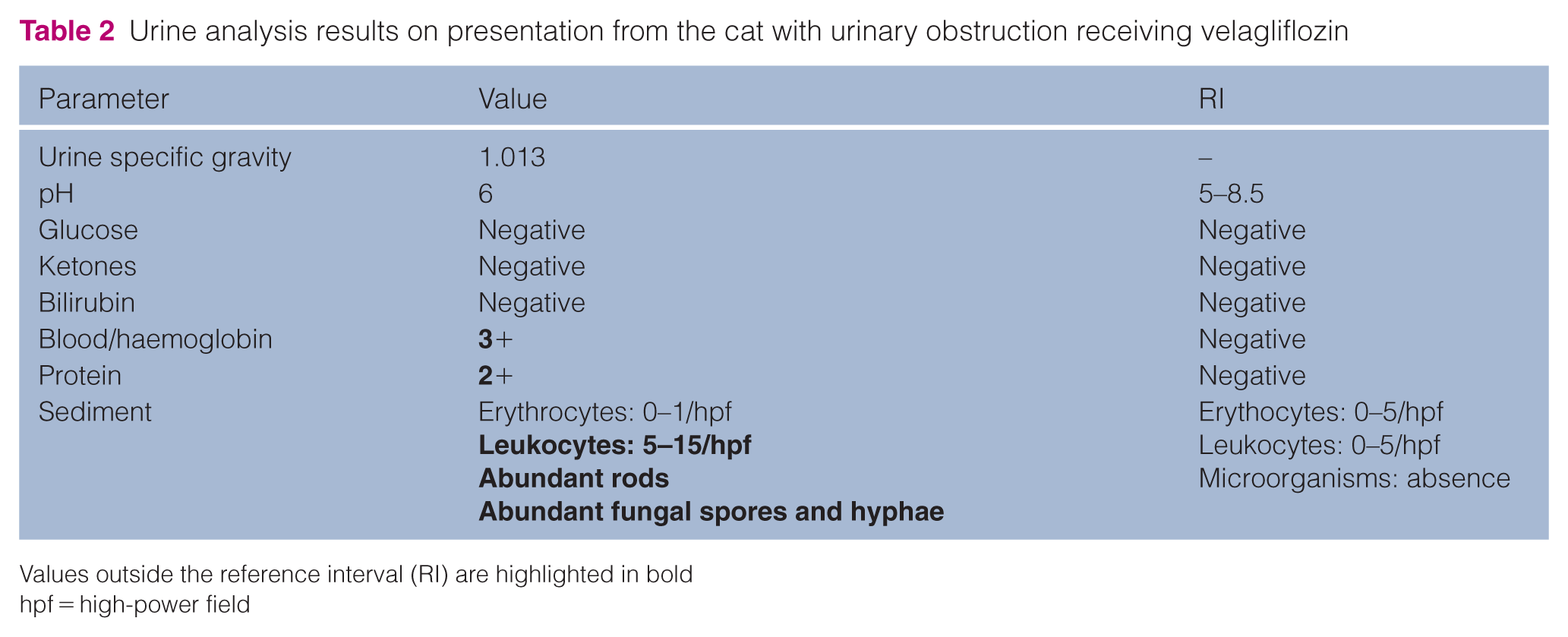
Values outside the reference interval (RI) are highlighted in bold
hpf = high-power field

Urine sediment from the cat with a fungal urinary tract infection receiving velagliflozin, showing abundant fungal spores and hyphae, with a moderate number of neutrophils and erythrocytes (Diff-Quik stain, 40 × high-power field)
Urine culture results from the cat with urinary obstruction receiving velagliflozin

Positive cultures indicate bacterial or fungal growth, with susceptibility testing performed according to standard laboratory protocols. Urine sample obtained by catheterisation
CFU = colony-forming units; I = intermediate; N/A = not applicable; R = resistant; S = susceptible
Abdominal radiographs confirmed bladder distension without additional abnormalities. Abdominal ultrasonography demonstrated marked urinary bladder distension with a thickened, irregular cranial wall and moderate echogenic sediment. The urethra was diffusely dilated to the intrapelvic segment. Both kidneys exhibited irregular contours and reduced corticomedullary differentiation, with 10 mm pelvic dilation in the left kidney. Ureters were normal. In addition, the pancreas was thickened with surrounding hyperechoic peritoneum. Hepatomegaly with homogeneous echogenicity and normal gallbladder morphology were observed. The small intestine retained normal wall layering, with mild muscular thickening.
Urethral urinary obstruction (UO) was diagnosed and attributed to UTI, recurrent FIC or urethral plug. The cat was hospitalised and a 5 Fr 15 cm indwelling urinary catheter (MILA Tom Cat; MILA International) was placed under sedation without complications. Treatment included fluid therapy with lactated Ringer’s, marbofloxacin (3 mg/kg q24h), itraconazole (5 mg/kg q24h), dexamethasone (0.1 mg/kg q24h), maropitant (1 mg/kg q24h) and buprenorphine (15 µg/kg q8h). Velagliflozin remained discontinued. After 24 h, the cat self-removed the urinary catheter but was able to pass small amounts of urine; therefore, catheterisation was not repeated, and medical management with prazosin (0.5 mg/cat q12h) and gabapentin (25 mg/cat q12h) was initiated. Dysuria worsened 12 h later, necessitating re-catheterisation.
By day 5, the cat had improved clinically and was able to void around the catheter. Euglycaemia was maintained, creatinine had decreased to 1.80 mg/dl (RI 0.30–2.10), electrolytes were within the RI and urinalysis sediment revealed no bacteria or fungi. The urinary catheter was removed. Anuria recurred 1 day later, requiring re-catheterisation. Contrast urography using iohexol revealed no urethral or bladder abnormalities. Three days later, considering the positive clinical course, the catheter was removed and spontaneous urination resumed. The cat was discharged with continuation of the same therapy and environmental enrichment measures to minimise stress, following treatment guidelines. 13
The cat re-presented with recurrent anuria 2 days later. Urinary catheterisation was attempted but proved technically challenging, so contrast urography was repeated and revealed urethral rupture (Figure 2). Urethrostomy was recommended but declined by the caregiver. Considering the poor prognosis and multiple comorbidities, euthanasia was elected.

Contrast urography image of the cat with urinary obstruction receiving velagliflozin treatment. The contrast study was performed 2 days after hospital discharge because of recurrent anuria, which revealed a urethral rupture
Discussion
Several risk factors for developing UTIs have been described in cats,14,15 with one study reporting a 13% prevalence among patients with DM, predominantly in females. 16 However, reported UTI prevalence in diabetic cats likely overestimates symptomatic cases (1–3%), as many infections are subclinical and may not require treatment. 16 Bacteria caused all infections in that study, with approximately two-thirds of cases being attributable to E coli. 16 In the present case, a mixed UTI involving E coli and C albicans was diagnosed. Both microorganisms are among the most common UTI pathogens in both humans and cats.6,14,16
A recent scoping review of feline and canine fungal UTIs reported that 17% of affected cats had DM, with C albicans being the most frequently isolated organism. 17 Candida species infections in cats are closely associated with alterations in local or systemic immunity, and managing these risk factors is essential for eradication. 18 Many risk factors have been identified for Candida species UTIs in dogs and cats, including previous antibiotic treatment, immunosuppression, lower urinary tract disease, kidney disease, urinary catheterisation, neoplasia and endocrinopathies, such as DM.18,19 These risk factors are similar to those described in human medicine.18,19 Among cats, antibiotic use, urinary catheterisation and lower urinary tract disease were associated with a major risk of developing Candida species UTIs, whereas the role of DM remains unclear and SGLT2is have not been evaluated.18,19 Interestingly, all the risk factors for Candida species UTIs previously mentioned were present in our patient. Hence, in the context of these multiple comorbidities, velagliflozin treatment – enhancing glucosuria – might be a key precipitating factor, as shown in humans.6,7,9
In humans, the association between SGLT2is and genital infections is well established. 6 In contrast, their link to UTIs remains less consistent.6,7 One proposed explanation is that osmotic diuresis induced by glucosuria and natriuresis increases urine output, thereby reducing bacterial concentrations and limiting ascending infections. 7 Recognised human risk factors include advanced age, reduced glomerular filtration rate, proteinuria, diabetic microvascular complications and, of particular relevance, impaired urine flow due to UO.7,14,20 Notably, most of these factors were present in our patient. Specific risk factors for GUIs in cats receiving SGLT2i therapy have yet to be identified. A study of cats treated with velagliflozin found no difference in the frequency of positive urine cultures compared with insulin-treated cats; however, the study was not designed to specifically assess this potential association. 4
Therefore, although current evidence does not support SGLT2is as a definitive risk factor for feline fungal UTIs, this case raises concern that individuals with comorbidities or predisposing conditions may be at increased risk. In addition, it is unclear whether the fungal UTI caused the UO or developed secondary to it. In our patient, velagliflozin was discontinued because of the severity of clinical signs and the presence of multiple risk factors, following a similar rationale to human medicine, where SGLT2is are maintained in mild GUIs but temporarily withdrawn in severe cases. 6
Fluconazole has been the most commonly used antifungal for these infections, consistent with human treatment guidelines for mycotic GUIs. 17 Prognosis is generally favourable, with approximately 60% of cats achieving recovery. 17 However, data remain insufficient to define therapy or predict outcomes. 17 Owing to the severity of clinical signs at presentation to the emergency service and because of the unavailability of fluconazole, antifungal therapy was promptly initiated with itraconazole, which appeared effective, as no fungal elements were detected on urine sediment examination after treatment. Nevertheless, because urine culture was not repeated when recurrent UO occurred, complete resolution of the fungal UTI could not be confirmed.
Importantly, velagliflozin was used off-label in this case, as its indication is restricted to otherwise healthy diabetic cats without significant comorbidities. 21 Therefore, velagliflozin treatment should not be generally recommended for the management of cases similar to the one we describe. Although insulin therapy was initially proposed as the first-line treatment, the caregiver declined owing to logistical constraints related to administration and concerns about the risk of hypoglycaemia. Velagliflozin was therefore selected as a practical alternative to prevent euthanasia.
Conclusions
This case reports a fungal UTI caused by C albicans in a cat with multiple comorbidities after initiation of velagliflozin therapy. In patients with multiple comorbidities, particularly those recognised as risk factors for fungal UTI, SGLT2i treatment may facilitate fungal UTI development, consistent with observations in humans. This report presents a preliminary observation supporting further investigation into SGLT2is as a potential risk factor for C albicans UTI in these patients. Nevertheless, additional studies are required to more clearly define this potential association.
Footnotes
Acknowledgements
We sincerely thank all members of the Internal Medicine and Intensive Care Service at AniCura Ars Veterinària Hospital Veterinari (Barcelona) for their support and collaboration throughout the management of this case. We also thank Dr Elisenda Climent from the Endocrinology and Nutrition Department at Hospital del Mar, Barcelona, Spain, for her valuable assistance in reviewing the literature and offering expert guidance on the case.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.