
Abstract
Background
With the evolving role of pharmacies over past decades, app-based medication adherence services have gained more attention in health services research. However, it is unclear how pharmacy staff members, as key stakeholders in implementing the service, perceive its suitability and how its introduction in practice could be facilitated.
Aim
To investigate pharmacy staff perceptions of the suitability of an app-based therapy support and to identify practice-relevant strategies for its implementation in community pharmacies.
Methods
We conducted an anonymous online survey among Swiss pharmacy staff (approximately 24,000 individuals) to evaluate suitability of app-based adherence services, usefulness of 14 different implementation strategies, and feasibility of 12 implementation strategies. We analyzed participants’ ratings of each statement using a 5-point Likert scale. We performed subgroup analyses within the categories age, sex, work experience, location, and role in the pharmacy.
Results
A total of 233 participants (mean age 45 years, 79% female, 90% pharmacists) completed the survey. Over 95% of participants strongly agreed on the general need for adherence support and over 80% perceived app-based services as particularly suitable for patients with chronic medication or polypharmacy. Willingness to offer app-based services received high agreement. With over 90% of participants indicating agreement or high agreement, implementation strategies such as access to a support person, using informational materials, and participating in training sessions emerged as particularly useful and feasible.
Conclusion
Pharmacy staff members acknowledge the need for adherence support and appear open to provide an app-based service. The findings emphasize the need for structured implementation planning and staff training ahead of national rollout. Highly rated strategies represent promising approaches to facilitate service implementation in practice.
Keywords
Introduction
Medication non-adherence is a critical issue in clinical practice. In chronic conditions, adherence rates are estimated at 50%, indicating a significant proportion of patients not taking their medication as prescribed. 1 Such deviations from treatment plans have been associated with reduced therapy success, increased hospitalization rates, higher mortality, and higher healthcare costs. 1 With the growing digitalization of healthcare and widespread access to smartphones, mobile health (mHealth) interventions like adherence-related mobile applications have emerged as potential tools to address medication adherence difficulties. 2 A large number of such mobile apps are currently available on the market, varying in terms of functionality, content, and quality. 3 While these apps are primarily intended to support medication self-management, recent research has also begun to explore their potential for integration into clinical practice as part of professional adherence services. Such services may include structured counselling on sampled adherence data.4–6
Overall, healthcare systems aim to be affordable, preventive, curative, and of high quality. 7 To meet this standard, newly developed innovations or services need to demonstrate effectiveness, suitability, and cost-effectiveness to qualify for reimbursement. 8 For smartphone-based adherence services, prior research could already show significant improvements in medication adherence rates, indicating their effectiveness.9–11 Given the substantial additional costs associated with medication non-adherence, it seems likely that such smartphone-based services are cost-effective. However, there remains a lack of evidence regarding cost-effectiveness of such interventions. 12
In the assessment of the suitability of app-based adherence services, prior research primarily focused on the patients’ perspective, specific apps, or app-based services for specific diseases.13–16 A qualitative interview study showed that patients perceive pharmacist-driven mobile app support as beneficial. 13 They particularly appreciate accessibility and direct communication with the pharmacist, and expressed openness to receive feedback. 13 Qualitative studies involving healthcare professionals (HCPs) have shown that HCPs familiar with mHealth applications recognized potential benefits for patients and expressed willingness to recommend them. 17 However, the perspective of pharmacy staff appears to be underrepresented in the existing literature. Prior research on pharmacy staff perceptions mainly focused on medication adherence apps as simple tools that may be recommended to patients.18,19 However, these studies did not examine apps as part of comprehensive pharmacy services with ongoing support and counseling, despite evidence that HCP interactions within such apps enhance the patient-provider relationship and clinical outcomes.20,21 In 2019, a Dutch study examined pharmacists’ perceptions of an adherence support intervention, including an app designed to promote self-management and adherence in asthma patients. 16 The majority of community pharmacists in this study perceived the app as useful and considered the pharmacy an appropriate setting for mHealth interventions. 16 Nevertheless, this study focused on one disease-specific app and included only a small number of pharmacists, half of whom were actively involved in service delivery. Consequently, there is currently little evidence regarding the perception of pharmacy staff of the suitability of non-disease specific app-based adherence support. Since pharmacy staff members could act as potential service providers in the future, a comprehensive understanding of their perspectives is necessary to fully evaluate on the suitability of app-based adherence services.
Besides recognizing the suitability of app-based adherence services, the practical introduction of the service will play a crucial role in its successful implementation in community pharmacies. Recent studies reported various difficulties in the implementation of new services in primary care settings like community pharmacies, together with potential strategies to overcome implementation barriers.22–24 However, the suggested strategies often draw on literature-based recommendations, such as the Expert Recommendations for Implementing Change (ERIC). 25 and are generally universal in nature, aiming to be applicable across diverse implementation settings and interventions. Nevertheless, their actual practical relevance has been scarcely examined. In the literature, the implementation of new practices is commonly assessed based on key factors such as usefulness (also referred to as appropriateness) and feasibility. 26 These factors are considered essential for determining whether new practices can be successfully applied in real-world settings. However, with regard to app-based adherence services, it remains unclear whether the predominantly literature-based and broadly formulated strategies are perceived as useful and feasible within the daily business of community pharmacies.
We aimed to investigate the pharmacy staff perceptions of the suitability of an app-based adherence service and to identify practice-relevant strategies for its implementation in community pharmacies.
Methods
Survey design and data collection
We conducted a cross-sectional online survey among Swiss pharmacy staff. The questionnaire consisted of five demographic questions (age, sex, region, position in the pharmacy and work experience) and three sections with one response matrix per section (see supplemental material).
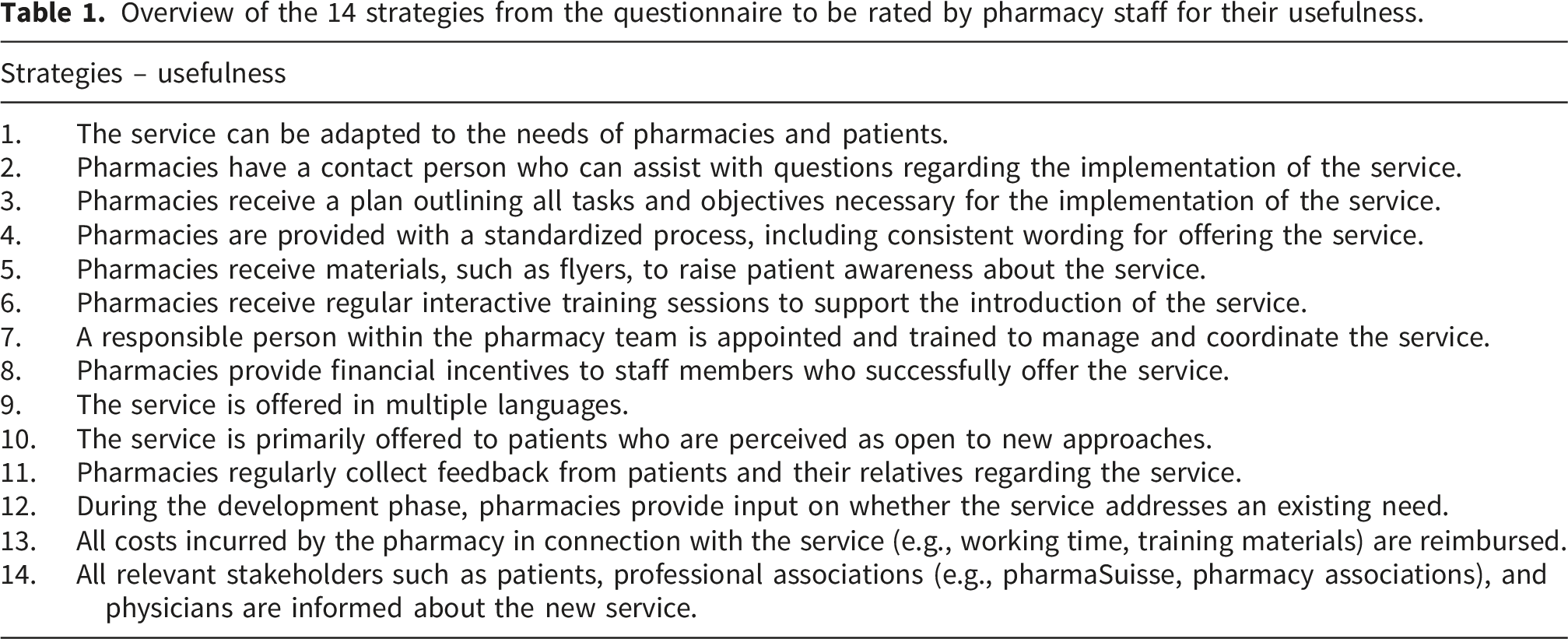
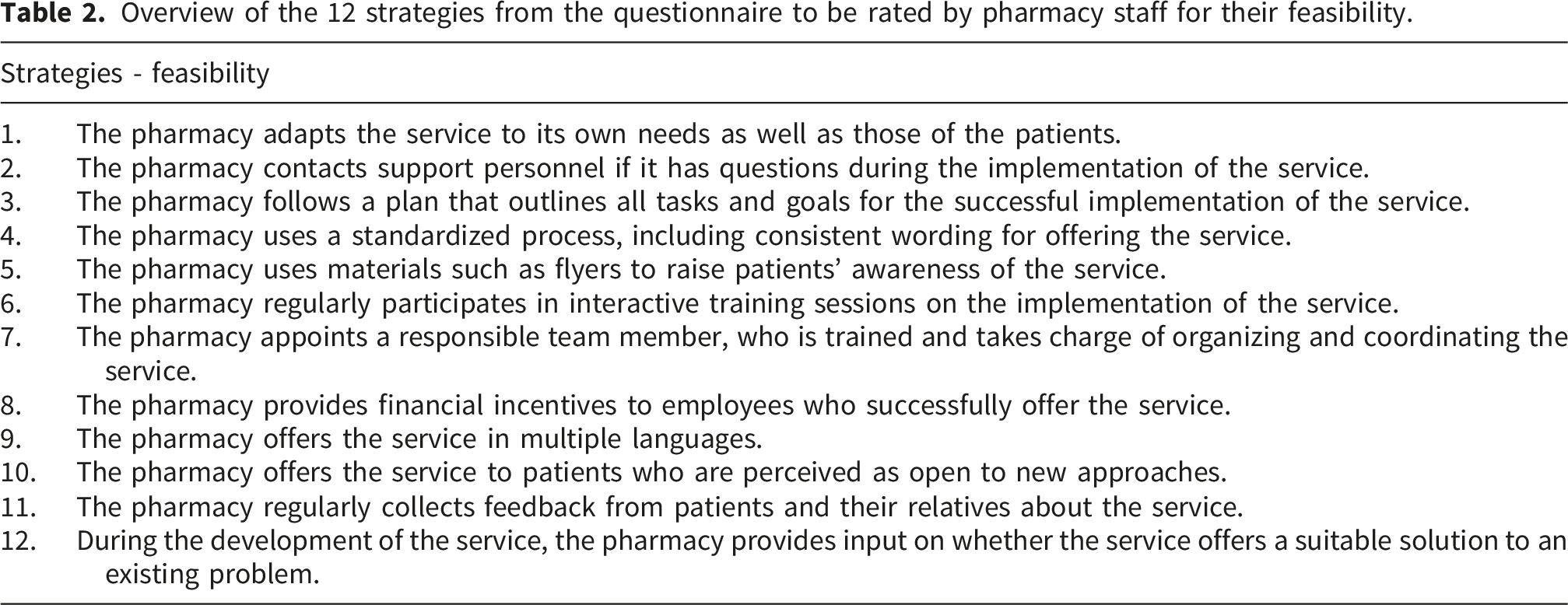
The first section included nine statements and one follow-up question focusing on app-based therapy support. This section explored pharmacy staff members’ perceptions regarding the medical need, the appropriateness of using an app, potential use cases, and their attitudes toward providing such a service. The second and third section included 14 and 12 statements, respectively, and assessed the pharmacy staff members’ view on different implementation strategies regarding their usefulness and feasibility. In all three sections, the participants rated each statement on a 5-point Likert scale. Additionally, participants had the option to select “no answer”. Every section included a free comment field at the end.
Overview of the 14 strategies from the questionnaire to be rated by pharmacy staff for their usefulness.
Overview of the 12 strategies from the questionnaire to be rated by pharmacy staff for their feasibility.
The questionnaire was pretested to ensure comprehensibility of its content and language. Four young researchers, three senior researchers, two pharmacy master students and two pharmacists participated in the pretest. Six out of the seven researchers were pharmacists by training and three were currently in practice. Pretest participants were selected based on their high similarity to the sample population. Feedback was collected through written comments and individual discussions. Minor revisions, including shortening the introductory text and adding a “no answer” option, were made to enhance usability and clarity. No iterative testing was conducted.
The survey was offered in German and French language. The questionnaire was developed and tested in German. The final version was translated into French using ChatGPT (GPT-4, OpenAI, 2025). The model was instructed to prioritize conceptual rather than literal equivalence and to maintain the original meaning and response scales. No formal back-translation was performed. However, two pharmacists fluent in German and French independently compared the German and French versions item by item to identify potential discrepancies. Discrepancies were resolved through discussions with the researchers to ensure a conceptually appropriate translation of the questionnaire. Minor wording adaptations were made to improve cultural appropriateness.
This survey study was reported in accordance with the Consensus-Based Checklist for Reporting of Survey Studies (CROSS; see supplemental material). 27
Sample characteristics
We calculated a target sample size of 379, assuming a population of 24,000 Swiss pharmacy staff members, 28 a 95% confidence level, and 5% margin of error. Since target sample size could not be reached, we calculated the margin of error for our final sample size at a 95% confidence level (MOE95), using a Z-value of 1.96. This margin of error is purely nominal and based on the hypothetical assumption of simple random sampling. Given the use of convenience sampling, it does not imply sample representativeness and should not be interpreted as enabling inference to the target population. The MOE95 is reported for orientation only.
Survey administration
We used the secured web application RedCapTM for data collection. We used a non-probability rather than a random sampling approach, in which participants were selected based on accessibility and willingness to participate. The survey link was distributed via email by the Swiss pharmacy association pharmaSuisse and through iMail-Offizin, a subscription-based magazine for pharmacists. PharmaSuisse sent the invitation to all Swiss pharmacies (approximately 1,800 pharmacies), which employ around 24,000 pharmacy staff. iMail Offizin sent the questionnaire to 2,021 subscribers. We cannot rule out that the 2,021 subscribers who received an invitation partly overlap with the 24,000 pharmacy employees. As multiple submissions could not be technically prevented, we checked the dataset for potential duplicates in participant characteristics. Potential duplicates were not considered for the analysis. The survey was open for four weeks. No reminder was sent to participants during this time.
Statistical analysis
For the analysis, only completed surveys were considered. Incomplete surveys were excluded from the analysis. Items for which participants selected “no answer” were treated as missing values. These missing values were excluded from descriptive and inferential statistical analyses. The proportion of missing data for each item is reported to ensure transparency.
Descriptive statistics were calculated by mean and standard deviation or median and interquartile range (IQR). We conducted subgroup analyses based on age, position and work experience, using non-parametric tests. Since some Swiss cantons allow physician dispensing (PD), we conducted a subgroup analysis comparing the perceptions of pharmacy staff members working in fully PD regions, partially PD regions, and non-PD regions of Switzerland. The Kruskal-Wallis test was used for comparisons involving more than two categories, and the Mann–Whitney U test for two-category comparisons. As it is generally recommended to have a minimum sample size of 15-20 participants per group to obtain robust and reliable results from the Kruskal-Wallis test, subgroups with less than 15 participants were excluded from comparisons.29,30 For subgroups with significant differences, post hoc analyses using Dunn’s test were conducted to examine pairwise group differences. To evaluate the effect sizes, we calculated Cliff’s Delta (δ). To control for type I error due to multiple testing, we applied the Bonferroni correction to all reported p-values. Because the same strategies were assessed under both Usefulness and Feasibility, the correction was applied across all tests for these items to account for multiple comparisons and maintain the familywise error rate. P-values < 0.05 were considered statistically significant.
To ensure that the translation did not affect the comprehension of the questions and to justify pooling the German and French responses, we conducted a group comparison for all statements using the Mann-Whitney U test. No adjustments for multiple comparisons were made, as all tests were non-significant. We performed all calculations using R (version 4.5.1; 2025).
Internal consistency of the three survey domains (Suitability, Usefulness, and Feasibility) was evaluated using Cronbach’s alpha with 95% confidence intervals. Dimensionality of each domain was assessed using polychoric factor analysis with maximum likelihood estimation, extracting a single factor per domain. Items negatively correlated with the primary factor were reverse-coded prior to analysis. We examined factor score adequacy through the correlation of regression scores with factors, the multiple R2 of scores with factors, and the minimum correlation of possible factor scores.
Results
Respondent characteristics
Demographic characteristics of the 233 participants who completed the survey compared with national pharmacy statistics. PD: Physician dispensing, SD: Standard deviation, CH: Confoederatio helvetica, N/A: Not available.
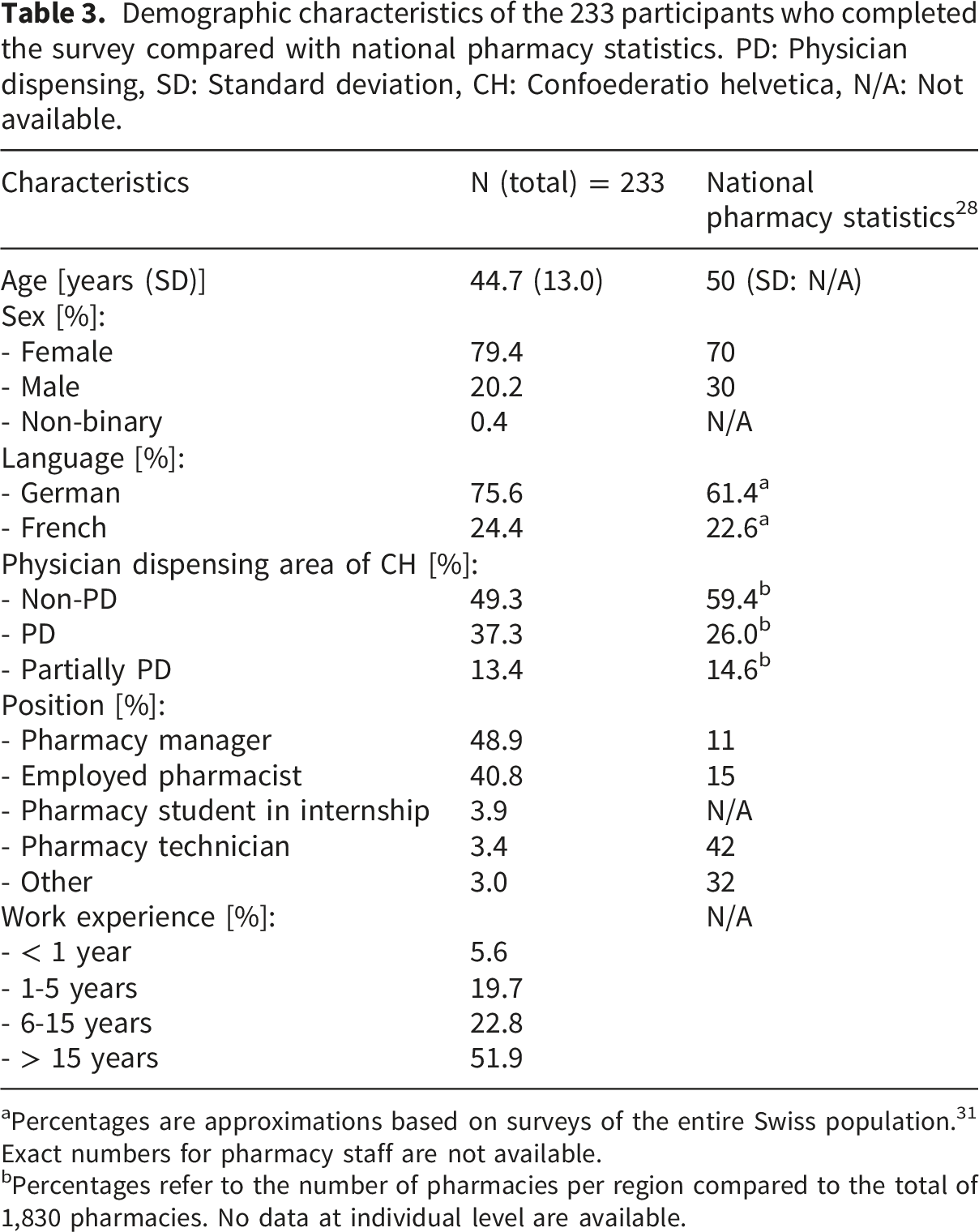
aPercentages are approximations based on surveys of the entire Swiss population. 31 Exact numbers for pharmacy staff are not available.
bPercentages refer to the number of pharmacies per region compared to the total of 1,830 pharmacies. No data at individual level are available.
Suitability of app-based therapy support
Likert-scale responses for suitability presented as median (interquartile range: IQR), including number and proportion of missing responses (N = 233).
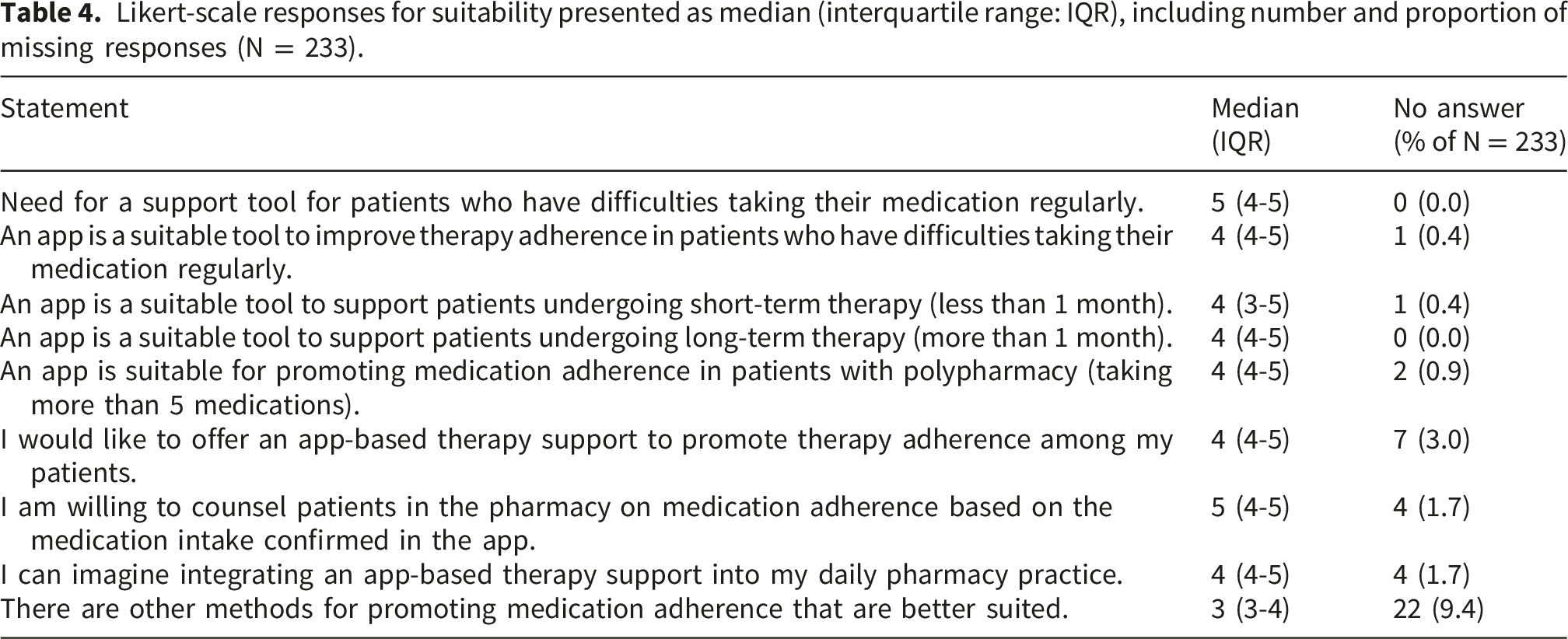
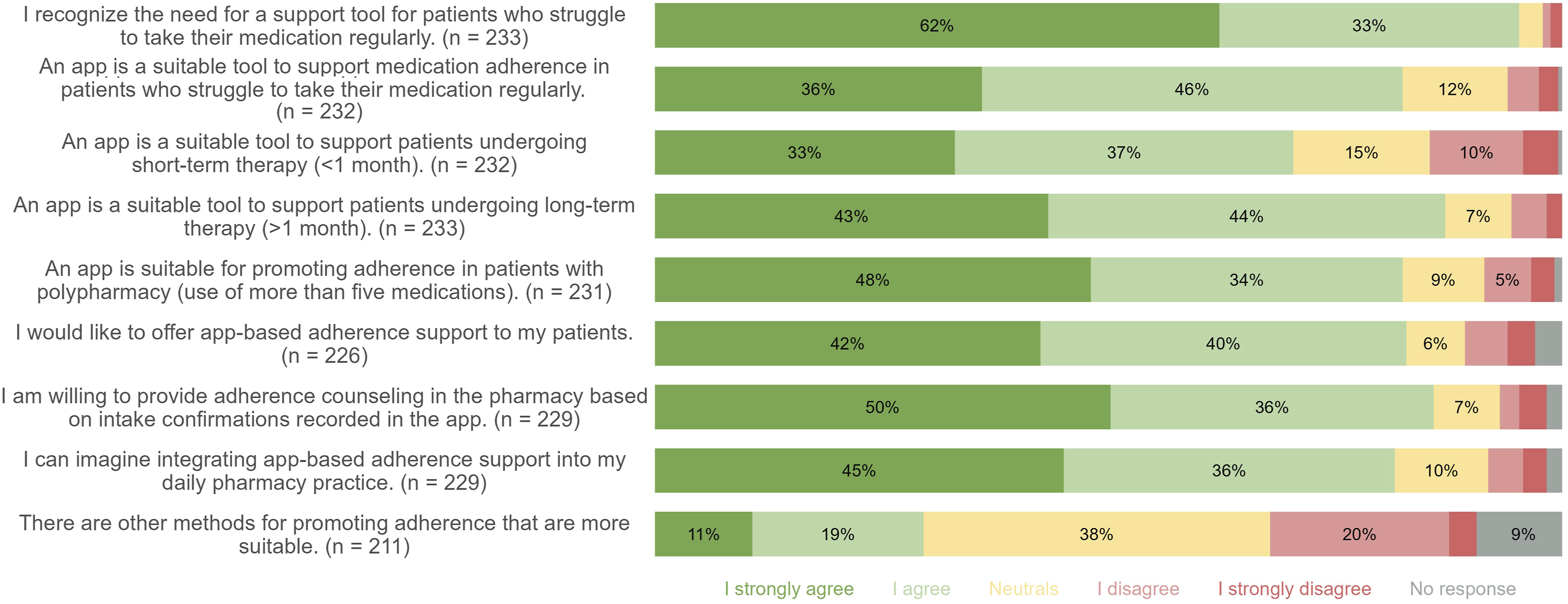
Likert-scale responses on the suitability of an app-based adherence support.
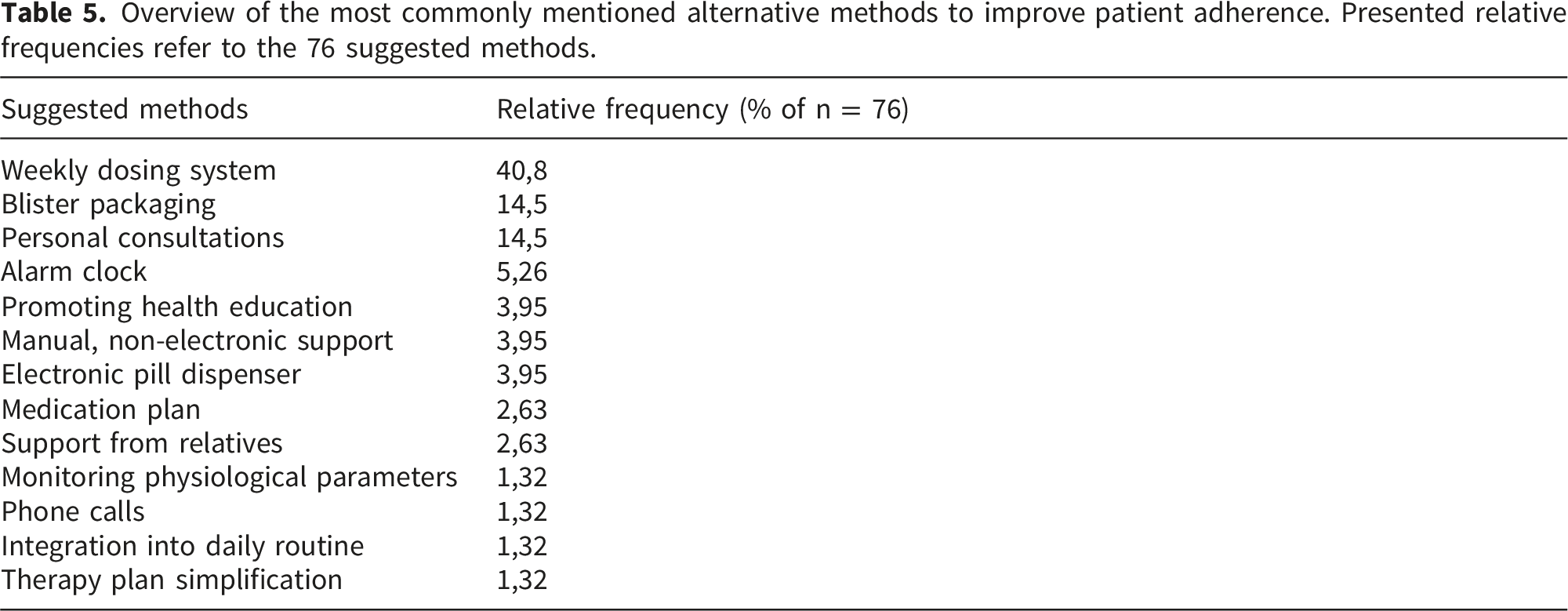
Overview of the most commonly mentioned alternative methods to improve patient adherence. Presented relative frequencies refer to the 76 suggested methods.
In the free comment section, a total of 72 participants provided additional comments regarding the usefulness of an app-based adherence support. One central theme was the limited suitability of such apps for certain patient groups with 35 participants addressing this issue. Participants particularly mentioned older patients and those with cognitive impairments, for whom the use of digital interventions poses challenges. Participants emphasized that apps are not suitable for these groups (“An app can be a suitable tool as soon as digital competence is present. For some, especially older individuals, this is not yet the case. However, the proportion of these individuals will certainly decrease over the coming years.” - Pharmacist, male, 30 years old). In this context, the primary target group for app-based adherence support was identified as the younger generation with technical affinity, although this is expected to change in the future as digital competence increases across all age groups.
Furthermore, it was noted that there is no method universally suitable for all patients, as individual needs must be taken into account. (“Just as people are different and have different needs, different offerings for promoting medication adherence should be provided.” - Pharmacist, female, 59 years’ old). Additionally, participants pointed out that adequate reimbursement must be ensured for the successful implementation of such a service in pharmacies.
Pharmacy staff also expressed privacy concerns regarding new adherence apps and advocated for integrating such a feature into existing, certified tools already used in Swiss pharmacies, such as mobile or web-based applications that offer various health services. Participants further stated that integrating a new adherence-optimizing feature into existing tools could reduce barriers for pharmacies and patients who may already be familiar with these platforms.
Usefulness of implementation strategies
Likert-scale responses for usefulness presented as median (interquartile range: IQR), including number and proportion of missing responses (N = 233).

Likert-scale responses on the usefulness of 14 implementation strategies. Strategies sorted in descending order of agreement.
Feasibility of implementation strategies
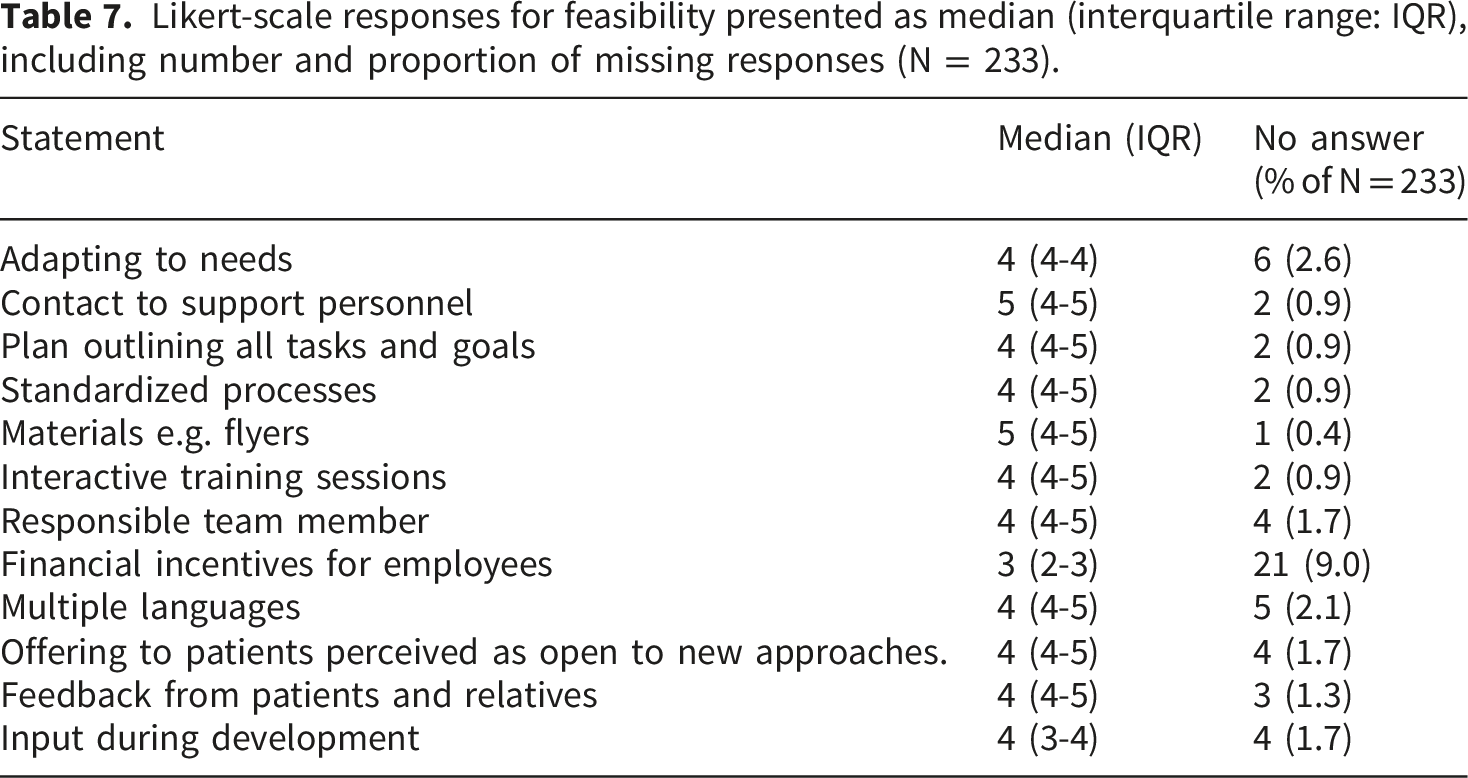
Likert-scale responses for feasibility presented as median (interquartile range: IQR), including number and proportion of missing responses (N = 233).
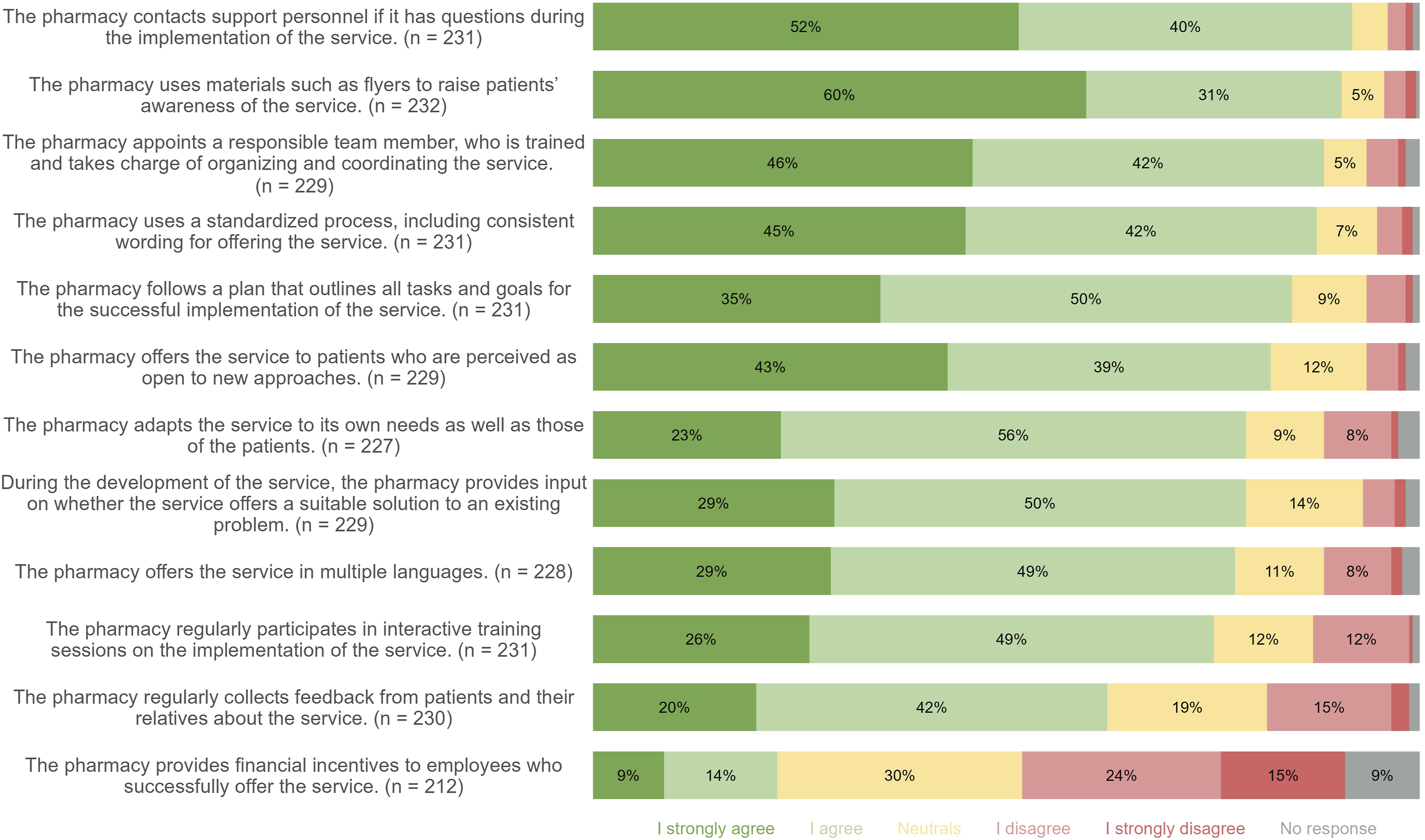
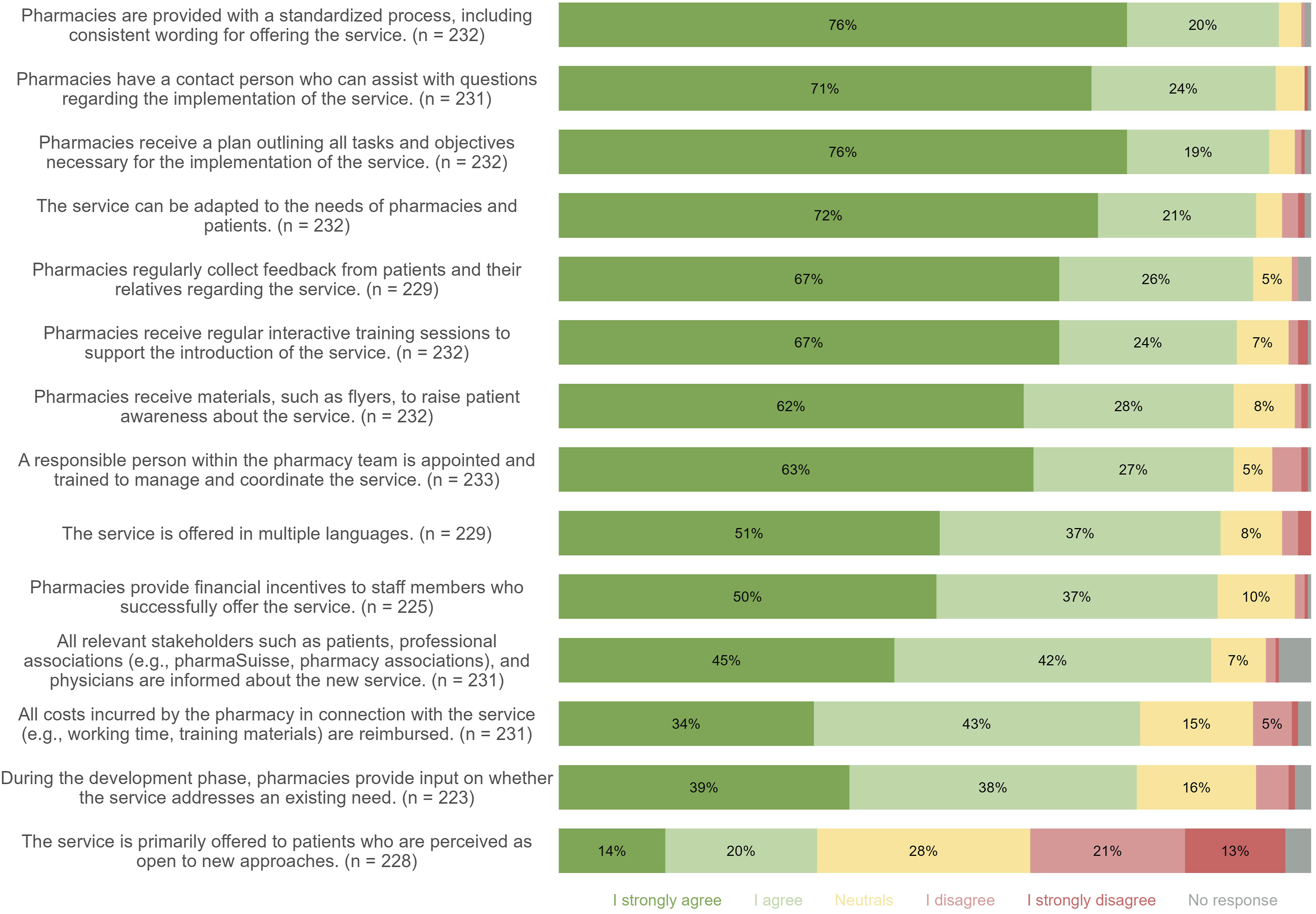
Likert-scale responses on the feasibility of 12 implementation strategies. Strategies sorted in descending order of agreement.
Subgroup-analyses and correlations
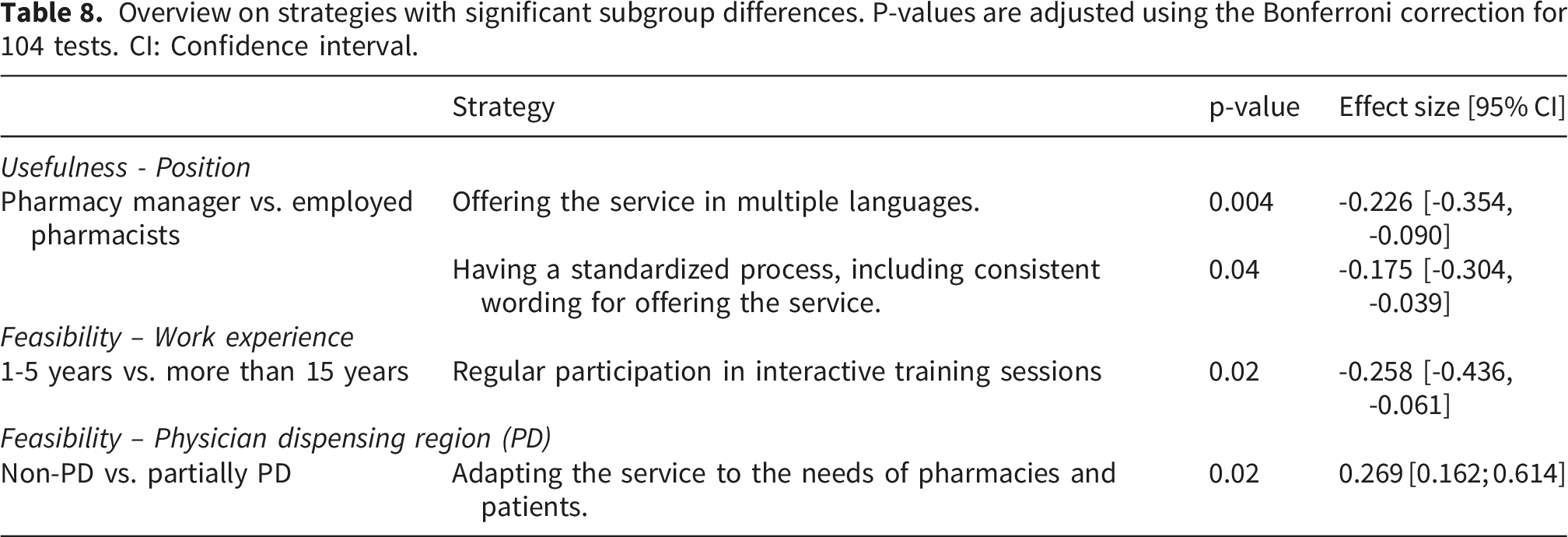
Overview on strategies with significant subgroup differences. P-values are adjusted using the Bonferroni correction for 104 tests. CI: Confidence interval.
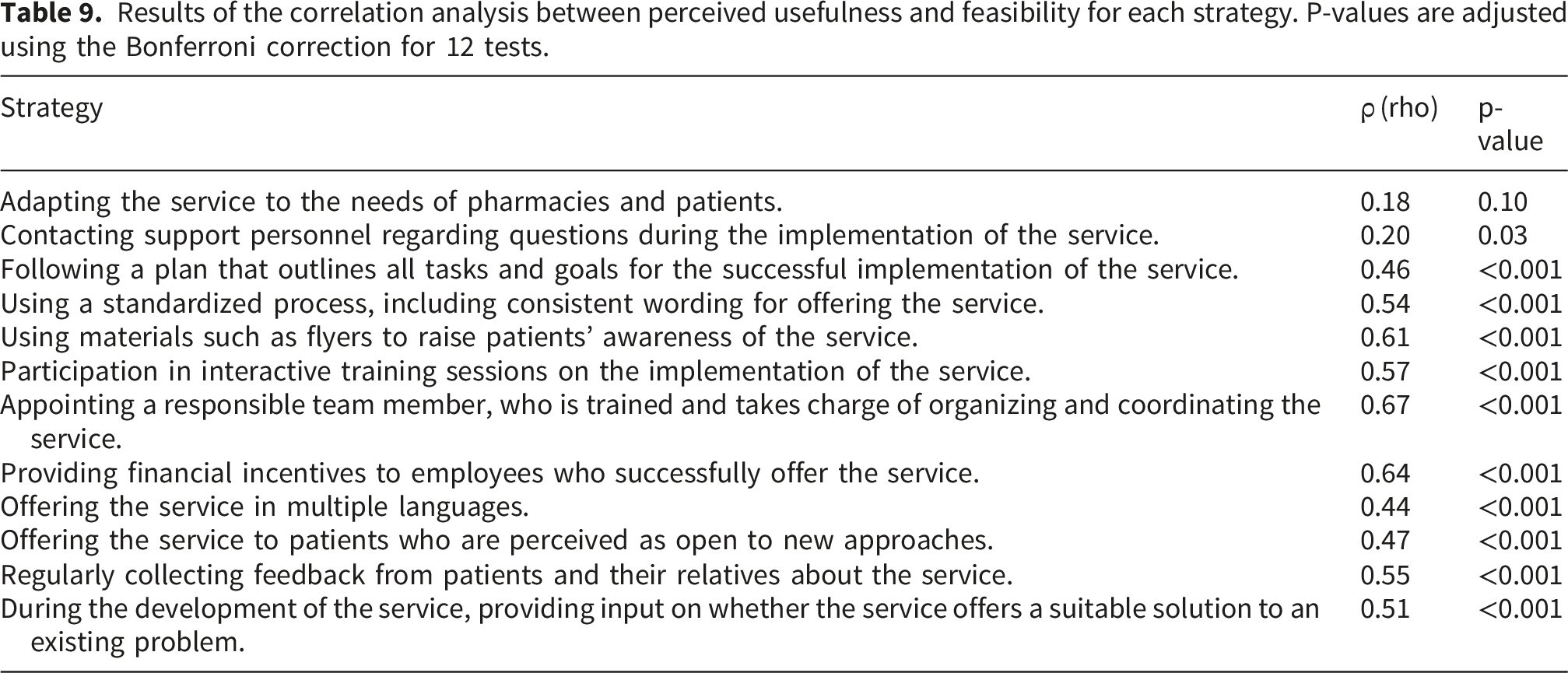
Results of the correlation analysis between perceived usefulness and feasibility for each strategy. P-values are adjusted using the Bonferroni correction for 12 tests.
All three domains demonstrated good internal consistency, with Cronbach’s alpha values ranging from 0.81 to 0.88. The single-factor solutions explained 35% to 59% of the variance, confirming the expected unidimensional structure. Most items loaded strongly on their respective factors, although one item in the Suitability domain loaded negatively and was reverse-coded. Model fit indices were acceptable, with root mean square residuals (RMSR) ranging from 0.08 to 0.10 and off-diagonal fit values between 0.93 and 0.98. Factor score adequacy was high across domains, with correlations of regression scores with factors ranging from 0.94 to 0.97, multiple R2 values from 0.88 to 0.95, and minimum possible factor score correlations from 0.76 to 0.89, supporting the reliability of derived individual scores.
Discussion
Suitability of app-based adherence services
This survey study reveals that pharmacy staff acknowledges the general need of an adherence supporting tool for patients with adherence difficulties, especially for patients with chronic medication and polypharmacy. Overall, pharmacy staff members perceive adherence-optimizing apps as useful and suitable, but express doubts about the suitability for older patients with limited technical experience. This perception is supported by previous research reporting that younger generations are generally more willing to use adherence apps than older individuals. 18 To mitigate this barrier for older individuals, ensuring ease of use is essential when designing and offering adherence apps. 18 With over 80% agreement, pharmacy staff members particularly identifies patients with long-term therapies or polypharmacy as a key target group for an app-based adherence service. This situation might be explained by several factors. Non-adherence in short-term therapies is often driven by intentional behaviors, such as non-initiation due to negative beliefs about the medication or early discontinuation due to side effects or improved well-being.32,33 Consequently, adherence apps primarily associated with reminder functionalities may be perceived as less effective in short-term therapies. Considering the time investment needed, pharmacy staff might prefer offering adherence apps to patients with chronic conditions, where the long-term benefits are more likely to justify the effort.
Further, pharmacy staff members express openness to offer an app-based adherence service in their pharmacy. They consider such a service as feasible to integrate into their daily routine. They are also open to counsel patients who are already using an app about their adherence behavior. Previous studies have shown similar results with the majority of pharmacists indicating willingness to support patients in this area 18 and expressing readiness to recommend adherence apps to patients. 19 Since we did not find statistically significant differences between age groups and willingness to offer an app-based service, we conclude that unlike in the general population digital solutions are gaining popularity across all age groups working in the healthcare service sector. This situation may be attributed to the growing awareness of the benefits of digitalization in the healthcare sector in general. Digital technologies are increasingly recognized for offering new opportunities that enable healthcare providers to deliver personalized care, reduce operational costs, and enhance treatment efficacy. 34 However, the challenges associated with digital technologies persist and are also acknowledged by pharmacy staff members. As noted by participants in the free comment section, privacy concerns remain a significant barrier for pharmacy staff as well as patients for apps sampling health data. Similar findings were reported by Davies et al. where the security of mobile apps emerged as one of the primary concerns among pharmacists. 18
Therefore, it is not surprising that a remarkable proportion of participants (31%) considers alternative adherence-optimizing methods to be more suitable than adherence apps. Among the alternatives, the weekly dosing system is most frequently named as the most suitable method. This finding is plausible given that providing dose administration aids is already one of the most common strategies used by pharmacists to support adherence. 35 In addition, this finding is consistent with participants’ expressed doubts about the universal suitability of adherence apps across diverse population groups, reflecting their view that adherence interventions must be tailored to individual patient needs.
Strategies for implementation in practice
Pharmacy staff members express agreement or strong agreement with most of the suggested strategies regarding their usefulness as well as feasibility. In particular, access to a contact person giving implementation support is perceived as highly useful, and reaching out to such a person is considered as highly feasible by pharmacy staff. Accordingly, the ERIC strategy of providing ongoing consultation to address the CFIR barrier related to implementation team members’ motivation and opportunity appears promising for the implementation of an app-based adherence service. This approach is further supported by recent literature. In a previous study, pharmacists identified regular contact with an implementation coach as one of the most valuable resources when implementing a new service. 36 The regular interactions supported the establishment of accountability, goal tracking, problem-solving, experience sharing, and prioritization of responsibilities. 36 For an app-based adherence service, the designated contact person could be a member from the party interested in adopting the service such as the app-developing company, or if the service is introduced as part of a research project a member of the research team.
In general, most of the suggested implementation strategies require - besides pharmacy staff as intervention deliverers and patients as intervention recipients - an external party to provide the necessary materials for effective service delivery (e.g., informational materials or a plan outlining tasks and objectives). This situation can act as a barrier to the integration of the service in practice, as it involves the investment of valuable resources such as time, staff and money. A collaborative effort between app developers and research teams may offer a promising solution to facilitate the implementation of such services in practice.
Participation in regular interactive training sessions emerges as another promising strategy, receiving strong agreement on its usefulness. Combining the ERIC strategies of ongoing and dynamic training, this approach also targets the CFIR barrier concerning implementation team members’ motivation and opportunity. This strategy was also identified in a survey study from the United Kingdom where 84% of the pharmacists indicated their openness to receive trainings regarding the use of mHealth apps to promote adherence. 18 Studies showed that increased staff training demonstrated more positive results in relation to the outcome. 37 The finding that more experienced pharmacy staff agreed more strongly with the feasibility of participating in training sessions may be due to their greater familiarity with daily pharmacy workflows. This familiarity could give them more capacity to take on additional tasks such as regular training. Since regular training is highly time-consuming for community pharmacies, one possible approach could involve a train-the-trainer strategy. This method was described in a previous study as more feasible and less resource-intensive. 38 The train-the-trainer strategy would also align with the pharmacy staffs’ desire for a responsible person on-site. Defining a responsible person corresponds to the ERIC strategy of identifying and preparing champions to address CFIR barriers related to internal pharmacy culture and tension for change. In addition to facilitating the on-site introduction of the service from an organizational perspective, the responsible person could serve as an intermediary between the pharmacy and the external implementing party. This approach allows a clear delineation of roles which supports workload relief and more efficient task distribution. Previous studies on immunization services in community pharmacies showed that successful adopters of the service often identified a local champion within the pharmacy. 39
Moreover, pharmacy staff members seem to be interested in standardized procedures, such as plans outlining tasks and goals, standardized implementation process, and informational materials such as flyers. These strategies could help overcome key CFIR barriers to digital services, such as innovation complexity and limited resources. The underlying reasons behind the high agreement with these strategies may, again, lie in the limited time and resources in their daily practice. Standardized procedures could help to minimize additional burden associated with service implementation. Furthermore, standardized workflows can positively influence the consistency in the delivery of an intervention. 40 The observed difference between pharmacy managers and employed pharmacists in their perception of the usefulness of standardized processes might be explained by the greater involvement of employed pharmacists in service delivery within the pharmacy. Regular service delivery demands additional time and therefore increases the perceived relevance of standardized, time-saving procedures.
In general, it is noteworthy that most of the implementation strategies are analogue in nature, highlighting a contrast between the digital character of the intervention and the implementation approaches. As mentioned above, although pharmacy staff appears to increasingly appreciate digitalization, they continue to value analogue formats. In recent publications, pharmacists especially highlighted technical difficulties as key concern when using digital tools such as mobile healthcare apps. 18 In combination with their desire for ease of use, it appears plausible that pharmacy staff favors analogue channels to manage the complexity and potential challenges associated with digital solutions.
However, although we were able to identify strategies that appear particularly relevant to pharmacy staff members in practice when implementing an app-based service, future research should now focus on testing these strategies in real-world settings to evaluate their actual relevance and effectiveness. Therefore, we propose conducting future studies that test adherence interventions in community pharmacy settings using implementation science-informed trial designs, such as Hybrid Designs. 41 By employing such designs, it becomes possible to evaluate not only the effectiveness of the intervention itself, but also the utility of the implementation strategies applied.
Strengths and limitations
Combining a literature-based approach by selecting implementation strategies derived from expert recommendations and integrating them into a survey to assess pharmacy staff views as key stakeholders in delivering the intervention represents a novel approach in health services research. The presented strategies that received high levels of agreement therefore appear to be of particular relevance for future implementation efforts in the community pharmacy setting. Further, the anonymous online survey may have encouraged more honest and unbiased responses compared to other data collection methods. 42 We therefore claim that the obtained responses reflect the true opinions of the pharmacy staff members and are not substantially affected by social desirability bias.
Nevertheless, this survey has several limitations. First, because the sample was not selected randomly, the results cannot be considered representative and must be interpreted carefully. Although a nominal margin of error is reported for orientation, it does not account for potential selection bias arising from the non-probability sampling strategy. The use of non-probability sampling limits the representativeness of the sample and the generalizability of the results. While most Swiss pharmacy staff were invited to participate, the self-selected sample is not necessarily representative of the whole pharmacy staff population in terms of age, roles, and location. The mean age of our sample is lower than of the general population (44.5 years vs. 50 years). PD regions of Switzerland and pharmacy technicians are underrepresented. 28 As a result, our findings may be influenced by potential sampling bias, limiting their generalizability to the entire Swiss pharmacy staff population, as for example younger participants might be more open to digital solutions. Second, we cannot exclude the possibility of participation bias, as pharmacy staff members with a particular interest in the topic may have been more likely to respond to the survey. In addition, due to its online format, the survey may have attracted more digitally proficient pharmacy staff members, who tend to be more open to digital solutions. Therefore, this survey format may have led to higher ratings regarding the suitability of an app-based service. These effects are further intensified by the low response rate, with only approximately 1% of pharmacy staff providing complete responses, introducing a potential non-response bias. Given this limited participation, it is possible that the views captured do not represent the broader population of pharmacy staff. As a result, the generalizability of the findings is limited. Conclusions regarding the perceived suitability of the service as well as feasibility and usefulness of the implementation strategies should be interpreted with caution. Third, ratings across the entire survey are close to the upper end of the scale (ceiling effect), resulting in little variance in the data and making it difficult to capture the differences in respondents’ true opinions. 43 As a result, it is challenging to clearly determine which implementation strategies are the most relevant. Further, this clustering of high scores not only limits overall variability but also reduces the ability to detect meaningful differences between subgroups, potentially underestimating true differences in perspectives among pharmacy staff. To address this limitation in future studies, Likert scales with more response options such as 7-point scales could be used, allowing pharmacy staff members to give more nuanced answers. 44 Fourth, survey items were initially translated using a machine translation tool without formal forward and backward translation. Although the translations were reviewed by bilingual pharmacists, subtle nuances or cultural differences in item interpretation may not have been fully captured, potentially affecting the clarity and comparability of certain questions across languages. While responses were compared descriptively between the German and French versions, no formal assessment of measurement invariance was conducted. Consequently, pooling responses from both languages may introduce measurement bias, as it cannot be guaranteed that the items function equivalently across linguistic contexts. Fifth, although subgroups with fewer than 15 participants were excluded from the analyses, some remaining subgroups in the Kruskal–Wallis tests were still small or unevenly sized, potentially limiting the statistical power and robustness of the subgroup analyses. Sixth, some items had a higher frequency of missing responses, suggesting that missingness was not entirely random. This issue may reflect challenges with unclear phrasing or difficulties in accurately situating the strategy (e.g., financial incentives for employees successfully offering the service) within its practical context. Even though only a few items had multiple missing responses overall, this could introduce an additional non-response bias, as participants who struggled to interpret or contextualize the strategy may be underrepresented in the responses.
Conclusion
Pharmacy staff members perceive app-based adherence services as a suitable intervention to improve medication adherence in patients with adherence difficulties, with greatest benefit seen in patients with long-term therapies or polypharmacy. They further express their willingness to deliver such a service. However, to support successful implementation, strategies such as having access to a support person, using informational materials, appointing a responsible person, and receiving regular training are perceived as particularly useful and feasible. Since our results reflect pharmacy staff perceptions, potentially affected by participation bias, evaluating these strategies for their actual relevance and effectiveness in practice will be essential to strengthen their evidence base. Identifying strategies that are truly effective and feasible can not only facilitate the integration of digital adherence services into routine pharmacy practice in the future, but also provide the evidence needed to support reimbursement decisions and inform national implementation planning.
Supplemental material
Supplemental material - Pharmacy staff perception of the suitability of an app-based medication adherence service and strategies for implementation - A Swiss national survey
Supplemental material for Pharmacy staff perception of the suitability of an app-based medication adherence service and strategies for implementation - A Swiss national survey by Kirstin Messner, Meret Berger, Lena Walz, Samuel Allemann in Digital Health.
Supplemental material
Supplemental material - Pharmacy staff perception of the suitability of an app-based medication adherence service and strategies for implementation - A Swiss national survey
Supplemental material for Pharmacy staff perception of the suitability of an app-based medication adherence service and strategies for implementation - A Swiss national survey by Kirstin Messner, Meret Berger, Lena Walz, Samuel Allemann in Digital Health.
Footnotes
Acknowledgements
We are grateful to BSc Patrick Penk for his assistance in coding the figures in R. We would also like to thank the participants of the survey pretest. Artificial intelligence-based tools were used to support the translation of the questionnaire and to assist in the development of R code for data analysis. No participant-level or study data were entered into, shared with, or processed by any artificial intelligence system.
Ethical considerations
According to Swiss law and institutional regulations, anonymous surveys that do not involve sensitive personal data do not require approval from an ethics committee. We have ensured that all aspects of the study were conducted according to the Declaration of Helsinki and in compliance with applicable legal and institutional guidelines. Informed consent was obtained electronically from all participants prior to the start of the online survey.
Author contributions
KM, MB, LW, and SA contributed to the conception of the online survey and the data analysis. KM, MB, and LW programmed the survey in RedCap™. Data analysis was carried out by MB and LW, with KM independently verifying the results. KM drafted the first version of the manuscript. All authors provided comments on earlier versions of the manuscript, and all authors read and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Datasets generated and analyzed in this study are not publicly available but are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.