
Abstract
Objective
Adapting Evidence Based Interventions (EBIs) for digital delivery can increase reach to additional populations and address barriers to engaging in traditional in-person programs. This mixed-methods study assessed the acceptability of a selection of digitally adapted content from StrongPeople Strong Hearts, an evidence-based cardiovascular disease (CVD) prevention program for women.
Methods
Eighteen women (mean age = 57.6 ±11.1, age range 37-74, 66.7% non-Hispanic White) were enrolled in a 4-week single-arm pilot study where adapted content was delivered through a private Facebook group. Mixed-method approaches assessed the acceptability of this abbreviated digital program. Participants completed feedback surveys (n=15) and focus groups (n=7) at the end of the study period.
Results
Participants reported enjoying their overall experience with the adapted content (average score of 4.71 ± 0.59 out of 5) and reported learning new or valuable information (average score of 4.64 ± 0.61 out of 5). Analysis of focus groups revealed that participants (1) appreciated the variety of content, which provided flexibility for program engagement; (2) enjoyed shorter nutrition videos but preferred longer exercise videos; (3) desired more external motivation from the program; and (4) desired further support with food portions and tracking.
Conclusions
This study supports the acceptability of StrongPeople Strong Hearts content adapted for digital delivery. Findings are comparable to the acceptability of the original program but highlight distinct challenges in transitioning some elements from an in-person to digital format. To address these needs, the complete digital adaptation of the program will continue to deliver a variety of content to allow for flexible engagement. Furthermore, additional content will consider the appropriate length and include more about food portions. Additional external motivators, such as a badge system and goal check-ins, will be integrated into the full program.
Keywords
Introduction
Cardiovascular diseases (CVDs) including heart disease and stroke are the leading causes of death and disability in women, affecting 44.8% of women above the age of 20. 1 Lifestyle risk factors such as obesity, poor nutrition, sedentary behavior, and stress are important factors to decrease risk of CVD.2–6 Previous CVD prevention interventions have effectively improved health behaviors and downstream risk factors such as BMI and systolic blood pressure.7,8 Even greater reduction in CVD risk can be achieved through multi-component programs that concurrently address multiple risk factors (i.e., diet and physical activity).9,10 However, traditional behavior change interventions delivered in-person present barriers to participation due to a lack of time, transportation, or substantial resources required for intervention delivery.11–14 One strategy to address these barriers is to deliver these programs through a digital platform (i.e., mobile app).15–17
Digital interventions targeting physical activity, nutrition, and other CVD risk factors have become more common in healthcare and research.18,19 Although access to certain digital technology varies, across all demographics, an average of 90% of US adults have smartphones, 20 approximately 68% use social media, 21 and over 60% use mobile health apps. 22 While smartphone ownership does not vary across genders, 23 social media use, especially Facebook, is higher among women. 24 Considering these statistics, digital mobile health apps that integrate social media-like features may be helpful for reaching more women in CVD prevention programs. Digital interventions have demonstrated efficacy in increasing physical activity, improving dietary behaviors, and improving cardiovascular disease risk factors.25–27 Utilizing digital technologies may also reach greater populations, as long as considerations are made for the unique needs and context of the community during the design and implementation of the program. 28 However, effect sizes in these trials are often small, which may be reflective of a lack of evidence and theory used in digital interventions. 29 Adapting existing EBIs for digital delivery can allow for the digital program to still be grounded in evidence and theory.
In addition to reach and feasibility, adapting existing evidence-based interventions (EBIs) may also be more efficient and cost-effective than developing a new digital intervention, especially when adjusted in the appropriate context for the new population or setting.30,31 Furthermore, adapted digital health interventions have shown equivalent efficacy to their in-person modality,32,33 and are perceived as similarly useful by participants. 34 Considering these factors, adapting an existing evidence-based program into a digital format may be valuable in targeting multiple lifestyle CVD risk factors for a wider audience.
StrongPeople Strong Hearts (SPSH, formerly Strong Hearts Healthy Communities) is a 24-week, multilevel CVD risk reduction program that utilizes the socioecological model to target individual, social, and environmental factors related to nutrition and physical activity. Participants in the SPSH program attended twice-weekly experiential classes that included skills-based education on physical activity and health eating, and in-class strength training and aerobic exercise. SPSH has been shown to improve CVD risk factors, improving physical activity, diet, and BMI in two community randomized controlled trials.35–38 In process evaluations following both trials, a majority of participants reported being satisfied with the overall program and its components (e.g., lessons, discussions, physical activity).14,39 In preparation for a digital adaptation of the program, our team undertook a structured, iterative process to adapt SPSH for delivery through a mobile app.40,41 The purpose of this study was to assess the acceptability of a selection of adapted SPSH content, aligned with the ORBIT model for behavioral intervention development. 42 Qualitative and quantitative feedback from participants, especially in the context of acceptability from the original SPSH program, will inform a full digital adaptation of the SPSH intervention.
Methods
Study design overview
This study was a single-arm pilot study that assessed the acceptability of a portion of SPSH content adapted for digital delivery. The pilot was designed for a 4-week duration, and in-person baseline and endpoint visits were held in Texas A&M AgriLife Research and Extension Center at Dallas. Four weeks of content from SPSH was digitally adapted into content compatible with social media, including short and long-form videos, discussion posts, polls, and infographics. This content was tested in a private Facebook group and posts were scheduled to be uploaded each day at multiple points of the day for the following 4 weeks. Participants interacted with the content asynchronously to fit their schedules. Before the program, participants completed in-person baseline visits to receive study materials and get access to the Facebook group. After the 4-week period, participants returned for an in-person follow-up visit to report their feedback on the program, and some participants were randomly selected to participate in a focus group to give more detailed feedback. These feedback surveys and focus groups analyzed to assess acceptability of adapted content. This study was reviewed and approved by the Texas A&M Institutional Review Board (IRB2022-0802D).
Participants
Recruitment ads were posted on Facebook and Instagram for six days (9/12/2023 to 9/18/2023) and were restricted to the Dallas-Fort Worth metropolitan area. Eligible participants were (1) female, (2) aged 18 and older, (3) had BMI >25, (4) engaged in ≤ 150 minutes of moderate-to-vigorous physical activity (MVPA) per week as measured by the Physical Activity Vital Sign (PAVS),
43
and (5) owned a smartphone capable of downloading mobile applications. Potential participants were excluded if they were (1) pregnant, (2) unable to read and communicate in English, (3) planning to participate in another health behavior change intervention in the next four weeks, or (4) unwilling or unable to provide informed consent. If interested, potential participants completed an online pre-screening questionnaire to assess their eligibility. Eligible participants were then called by the research staff to confirm eligibility and schedule their baseline visit (9/16/2023 to 9/22/2023) at the Texas A&M AgriLife Research and Extension Center at Dallas. Of the 118 people who took the screening questionnaire, 18 enrolled in the program (9/24/2023 to 10/21/23) Figure 1. Recruitment flowchart.
Baseline visit
During the baseline visit, participants signed an informed consent document, completed baseline surveys, joined a private Facebook group that was used for sharing intervention content, and received study materials. Facebook was used as delivery platform due to its familiarity among participants. While exposure to distractions from other posts on personal newsfeeds or privacy concerns may be limitations to this delivery method, a private group was created to dedicate space for the content and to keep involvement in the program hidden from the participants’ public profiles. The study materials included a goal-tracking booklet, a Fitbit Inspire 2, a Withings Body Pro scale, and three sets of weights for strength training exercises. During the visit, participants downloaded the accompanying Fitbit mobile application to their devices with a study account that was not linked to their personal information. The Withings Body Pro scale was assigned prior to the visit, and participants were instructed on how to complete in-home calibration of the scale. Research staff provided suggestions on how often to use the body weight and the activity and sleep tracker, but ultimately the participants decided how they wanted to interact with the tools.
Intervention
Description of program components.

Prior to the start of the program, participants were encouraged to engage with onboarding material, which provided introductory material that was included in the original program’s participant booklet. The onboarding videos introduced the overall program, behavior change principles, the food tracking system, and the exercise components. Additionally, infographics and videos were placed in the library content and were separated by the topics of nutrition, physical activity, and behavior change.
Sample week content plan.
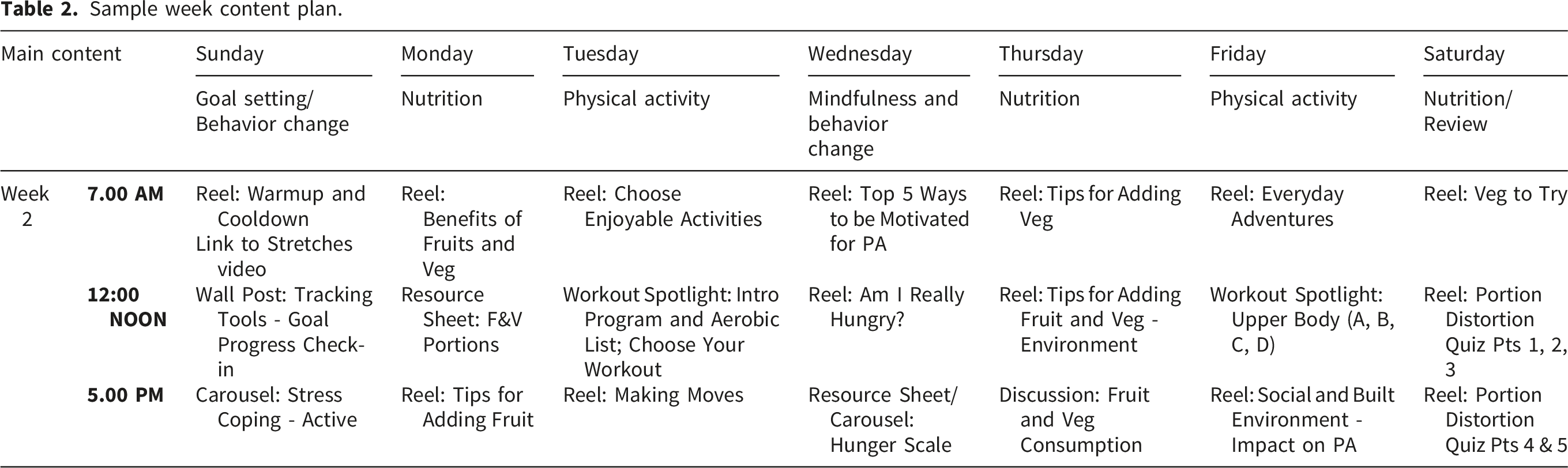
During the 4-week intervention period, participants were instructed to engage with posted content, write in their booklet to track goals and food portions, wear their Fitbit device at all times (except for when charging the device), weigh themselves on the scale at least once per week but not more than once a day, and use the weights as needed for the strength training component. Research staff monitored and observed the participants’ interaction with the content and answered participant questions. Beyond this facilitation, research staff minimized their activity in the group to reduce their direct influence on the participants’ engagement with the content.
Follow-up visit
Following the intervention, participants attended a follow-up visit (10/24/2023 to 11/03/2023) to return the Fitbit and scales, and to complete follow-up surveys. Participants were randomly invited to give additional feedback in a focus group, and those who opted-in joined a focus group. Random selection was used to allow participants to share a range of opinions and experiences.
Demographics and post-intervention satisfaction survey
Participants completed a demographic survey including date of birth, race, ethnicity, education, and household income during their baseline visit. Response variables for race included American Indian or Alaska Native, Asian, Black or African American, Hispanic or Latinx, Native Hawaiian or Other Pacific Islander, and White, with an ability to select more than one race if applicable.
Acceptability was evaluated through the post-intervention satisfaction survey. Participants rated their degree of satisfaction with each component of the program: onboarding content, newsfeed videos, library content, exercise demonstrations, and polls and discussions. Participants rated each program component on a scale from 1 (strongly disagree) to 5 (strongly agree) within the subcategories enjoyability, sufficient information, and quality. These subcategories were adapted from commonly used categories in user satisfaction surveys for mHealth of “quality”, “usefulness”, and “satisfaction”, the latter of which was further specified into “enjoyability” and “sufficient information” to apply this program’s educational content. 45
Demographic information was summarized and a descriptive analysis of data from the post-intervention satisfaction survey was conducted to assess the participants’ perceived enjoyability, helpfulness, and quality of each program component.
Focus groups
Acceptability was further assessed through post-intervention focus groups conducted during the follow-up visit. The focus groups were conducted in-person by two full-time research team members (AO, LB) and the project Principal Investigator (CDR) who followed a semi-structured interview guide developed to get feedback on different components of the intervention. Topics included the overall program (e.g. “Tell me about your overall experience in the Strong Hearts program for the last month.”), physical activity (e.g. “Tell me about your experience with the physical activity part of the program.”), food and nutrition (e.g. “Tell me about your experience with the food and nutrition part of the program.”), and platform features (e.g.” What features in the Facebook group did you find helpful, that you’d like to continue to see in an app-based version of this program?”). The focus groups were an average of 36 minutes. CDR had no contact with the participants prior to the focus group, but AO and LB had limited contact with participants through Facebook due to their roles in moderating the 4-week program. To reduce bias, participants were encouraged to share all their feedback and experiences, regardless of the sentiment. The two focus groups were recorded using Microsoft Teams with auto-generated transcripts. These transcripts were cleaned by the research staff (AO, LB).
Qualitative analysis
The research team followed Braun and Clarke’s six-step process to facilitate thematic analysis of the focus group transcripts. 46 Two researchers (AO, LB) read the transcripts and noted initial ideas in preparation for creating the codebook. A postdoctoral researcher (PG) met with the two research staff members (AO, LB) to discuss these initial ideas and afterwards developed a codebook to guide the full coding of the transcripts. The two research staff members (AO, LB) then coded all transcripts using this codebook on Microsoft Word and grouped the categories into potential themes in a separate document. PG, AO, and LB met on multiple occasions to review, discuss, and revise these potential themes, identify example quotes for each theme, and to resolve any differences in coding or interpretation. The coders re-read the transcripts on Microsoft Word to ensure full analysis of the data. Saturation was likely not reached due to the limited number of focus groups. However, the capacity to reach saturation was limited with the restraints of the smaller study sample and the goal to include about half of the remaining enrolled participants in FGs. However, the goal of this qualitative analysis was to get initial thoughts of a selection of content for an official pilot that will later be delivered. Therefore, the themes that did emerge were still used and considered for directions for future iterations of the program.
At the time of the interviews and analysis, CDR and PG had previous training and professional experience in focus group delivery and qualitative research methods. AO and LB were trained and supervised in focus group delivery and qualitative research by CDR and PG.
Results
Participant demographic characteristics.

Acceptability survey
Participant satisfaction survey.

From the two focus groups (n=7), the following themes regarding the acceptability of the digital program were identified: (1) participants appreciated the variety of content and tools, which provided flexible ways to engage with the program; (2) participants liked the short nutrition videos and new recipes, as it made nutrition changes seem more approachable; however, longer instructional videos for exercises were preferred; (3) participants desired more external motivation from the program to support goals and (4) participants sought further support in understanding and tracking food portions.
Theme 1: Participants appreciated the variety of content and tools, which provided flexible ways to engage with the program
Participants appreciated the flexibility in how they could interact with the content and resources from the program. In terms of content, some participants enjoyed the discussions, which involved more time and disclosure, while others enjoyed polls, which were quick and less intrusive. Having a variety of posts allowed for more flexibility in accommodating participants’ preferences. “I enjoyed the discussion that happened, which is really what you're talking about… Ah, but it was really nice to have just the exchange of information and ideas, umm, if you can't be in a class in person, like sitting down together.” “I like the surveys. I'm usually not going to say the words… but I will click on stuff and get my answers.” Some participants enjoyed the devices, but others did not find them helpful or encountered barriers in their use. As such, the continued flexibility in how they could use their devices may be helpful. “So I don't have an Apple Watch, so it [Fitbit] was great. And I was able to see what was going on that day.” “It is hard - It's [the Fitbit] small. I have all the time to be like pressing to see what's happening and it was just hard to use it.” “Yeah. Mine [scale], you know, had problem. Couldn’t use it for some time. Then I figured out it was batteries. So I bought the batteries. But the scale that I was seeing was still not accurate, because I have another one at home which was different. So I was confused…It’s reading low. Even today, it’s still low.” “…it really motivated me, the scale, because I saw my BMI going down.”
Theme 2: Participants liked the short nutrition videos and new recipes, as it made nutritional changes seem more approachable; however, longer instructional videos for exercises were preferred
Participants expressed that the short-form nutrition videos and recipes were relevant to them, as it sparked conversation and intention for dietary changes.
“Yeah, I love the food part, where the small explanation about the protein foods and where to get them. Yeah, so I love that part.”
The single 30-minute weight training video that was provided was acceptable and helpful. “Yeah, but the one video [intro strength workout] of them showing the strength training was very good. I thought it was a really good video to show a good basic strength training.”
However, short strength training videos, which demonstrated how to do each strength training movement separately, were not as useful due to the volume of material. “...they [strength training demonstrations] were in smaller bits like you do this and move this. It's not something like continuous for like maybe for 30 minutes going to do this and I don't want something where I have to click on this, move to this.”
Theme 3: Participants desired more external motivation from the program to support goals
Participants indicated that they faced multiple barriers to engaging in behavior change, such as lack of time and lack of motivation, and expressed a need for more external motivation to combat these barriers. They wanted dedicated interaction with moderators and other participants, such as weekly goal check-ins, real-time conversations, and reminders about their goals to keep them on track. Furthermore, participants wanted challenges and rewards for completing in-app activities, such as a badge system to make the program more engaging and fun. “You have to discover your internal motivation for your goal setting. But let's be real. It's really a lot about the dopamine, and we love a good challenge.” “Get me a badge, I will work for a badge.” “Or maybe a live, let's say a live chat. Yeah, maybe once a week or twice a week have something that we can get on there and even just comment. “I would have liked to have seen more conversations in the group about goals and goal setting amongst the members.”
Theme 4: Participants struggled with understanding and tracking food portions
The program offered a food tracking system where participants tracked what they consumed in each food group (carbohydrates, dairy, protein, fats, vegetables, fruit, and extras). Despite providing onboarding materials and portion tracking content, participants struggled with understanding food portions and applying this knowledge to track their nutrition intake. Therefore, additional guidance about food portions with practical applications was requested to make tracking easier for participants. “Serving sizes is kind of overwhelming” “It was hard whenever I cooked to track, how much is this and what do you need for this? “Yeah, we actually cook at home and you're not just making a single ingredient item. Like I didn't just cook a chicken breast, and some broccoli and a sweet potato.…It, it becomes overwhelming” “And the only problem I had was like, how do you know to do the portion control?
Discussion
This study aimed to assess the acceptability of content adapted from the Strong People Strong Hearts (SPSH) program for digital delivery to inform the future full digital adaptation. Similar to the previous program’s findings, the content delivered in this 4-week testing period was acceptable to participants and was perceived to improve knowledge and support behavior change, especially related to nutrition. The study’s focus on acceptability is informed by the ORBIT model for behavioral intervention development. 42 In addition, the variety of content and tracking tools allowed participants to engage in their preferred way. However, additional feedback called for more external motivation features, longer exercise videos, and additional guidance with portions and food tracking. This is somewhat aligned with participants’ reports of facing barriers with physical activity and healthy eating from the original program. However, these specific desires are unique to iteration of the program, which may be due to the modified program structure and social support from transitioning to a digital format. The feedback obtained from this pilot is intended to be implemented into the full digital adaptation.
Although the content was deemed acceptable and helpful, participants did note several factors they perceived would be helpful in a full digital intervention. Participants expressed the need for more external motivators in a self-paced program. The literature affirms that lack of time and entrenched attitudes and behaviors are barriers to behavior change. 47 However, consistent cues may influence decision-making for behavior change despite barriers.48,49 While aspects of our digital program were designed to be self-paced (i.e., how and when to engage in physical activity), some structure, such as regular dedicated discussions about goal setting and self-monitoring may be helpful to aid in the adoption of behavior change in participants in this asynchronous setting. 50 This may especially be pertinent in the context of the original SPSH program, as such discussions of goal-setting and self-monitoring were often integrated into the class curriculum itself and were reported be liked components by the participants. 14 In the full digital program, the aim is to include a badge system based on engagement with content, weekly goal check-ins, real-time conversations, and goal reminders to support participants in staying on track as well as occasional “fitness challenge” prompts with a recommended exercise program that are clear and directed.
Participants expressed a need for more guidance on understanding portions and food tracking. Knowledge of food portions and food tracking are essential to utilize when changing eating behavior.51,52 Beyond knowledge, other individual barriers, such as lack of goal setting, and app-related barriers, such as reliability of the app or food database, are additional challenges to food tracking. 53 Due to the variety of barriers to not using food tracking applications, the most effective method for increasing engagement in food tracking may be to tailor the design of the tracker for specific users goals and needs. 54 This finding was not shared with the original program’s process evaluation, likely due to the difference in length of the original program (24 weeks) and the abbreviated timeline of this pilot study (4 weeks). Considering the need to increase knowledge, implement goal-setting, and tailor the app to the users’ needs, the full digital program, which will span 12 weeks, will provide additional resources on portions, suggestions on setting goals that integrate food tracking, and provide a tracker compatible with the program’s food tracking system directly on the mobile application.
Limitations
The presented results are preliminary findings with limited ability to reach saturation due to a small number of participants. However, the goal of this study was to test the acceptability of only a portion of the digitally adapted materials to inform the full 12-week adaptation following this pilot. Due to this exploratory focus, a fully powered sample size was not necessary to meet the study goals. However, in future investigations of this digital adaptation, an adequately-powered study design including randomization and use of control groups will be required to determine program-related efficacy. Such findings could then be compared with the original SPSH program.
While recruitment was broadly in the Dallas–Fort Worth metropolitan area, the final sample skewed toward individuals with higher education and income, reflecting patterns of digital recruitment. This may limit generalizability to broader, more socio-demographically diverse populations. Future research should consider a variety of recruitment strategies to enhance representativeness. In addition, the study tested only a select portion of the SPSH curriculum over a limited time frame. Further, the post-intervention satisfaction survey, while based on existing validated questionnaires, was not a validated measure on its own. Findings on acceptability may therefore differ in a full-length program. Future studies with a larger sample size, as well as established process evaluation frameworks and questionnaires during evaluation of the full digital program may be even more valuable in understanding the acceptability and feasibility of the complete program.
Conclusion
Content from the SPSH program that was adapted for digital delivery was found to be acceptable by a cohort of women with elevated BMI and promoted knowledge and supported behavior change intentions, especially in the context of nutrition. These findings will support the variety of content and tools in the full adaptation of the program to allow flexible ways to engage with the program. While acceptability for this content showed some similarities to the original program’s acceptability, the main differences may lie in the challenges of transition from an in-person to digital format. The digital adaptation of SPSH and potentially similar programs should consider including longer instructional videos for exercises, external motivation and support for goals, and additional materials on food portions and tracking to bridge some challenges from the replacement of in-person elements.
Ethical considerations
The study protocol (IRB2022-0802D) was approved by the Texas A&M Institutional Review Board.
Footnotes
Consent to participate
All participants completed a written informed consent prior to enrollment.
Author contributions
All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This material is based upon work supported by the Texas A&M AgriLife Institute for Advancing Health Through Agriculture, IHA, and the U.S. Department of Agriculture, Agricultural Research Service, under Agreement No. 58-3091-1-018. Any opinions, findings, conclusions or recommendations expressed in this publication are those of the author(s) and do not necessarily reflect the view of the sponsor.”
Declaration of conflicting interests
RASF is a co-founder of ![]() . No other authors have conflicts of interest to declare. The funders had no role in the design and conduct of this study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
. No other authors have conflicts of interest to declare. The funders had no role in the design and conduct of this study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request. CDR is the guarantor of this work and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Statements and declarations
Permission was given by copyright holder(s) of the original program to use all applicable tools and materials in this study. No AI tools were used in the develop or editing of this manuscript.