
Abstract
Objective
To systematically identify and critically evaluate research evidence on the association between digital health literacy (DHL) and healthy lifestyle behaviors (HLB) among youth.
Methods
A systematic search was conducted of five English-language databases—Web of Science, Scopus, ProQuest, EBSCO, and PubMed—covering publications from January 2006 to October 2025. This search was supplemented by reference list screening, resulting in the inclusion of 33 studies in the final review.
Results
Overall, youth exhibit a relatively high level of DHL, and the eHealth Literacy Scale (eHEALS) is the most frequently employed instrument for its assessment. HLB associated with DHL primarily encompassed domains such as physical activity, sleep, diet and nutrition, as well as mental health and stress management. Higher levels of DHL among youth were associated with more favorable HLB, but the magnitude and consistency of these associations varied across behavioral domains.
Conclusion
This study aims to examine variations in the role of DHL across different HLB domains, guided by the COM-B behavior change model, which emphasizes the interaction of capability, opportunity, and motivation. Further research is warranted to clarify the mechanisms linking DHL with specific HLB, particularly through high-quality longitudinal and intervention studies. In addition, DHL measurement instruments should be refined to ensure their validity and applicability within the rapidly evolving digital health environment.
1. Introduction
Promoting healthy lifestyle behaviors (HLB) is a central objective of global health policies. However, this goal is largely unmet among young people. Accordingto the World Health Organization (WHO), over 80% of adolescents worldwide fail to achieve recommended physical activity levels,1,2Similarly,adherence to other health-related behaviors, including healthy eating, sufficient sleep, and stress management, is also low.3,4 Alarmingly, these behaviors may elevate the risk of developing diseases later in life.
According to a report by the International Telecommunication Union (ITU), Internet usage among young people shows a significant upward trend. Approximately 80% of adolescents worldwide, and 52% of individuals aged 15–24 in middle-income countries, use the Internet. 5 The rapid advancement of digital media and communication technologies has led to more diverse access to information. Emerging methods, such as online medical consultations, health tracking apps, and the dissemination of health information via social media,6,7 continue to develop. Increasingly, health-related information is accessible online, providing an efficient pathway to promote healthier lifestyle behaviors. However, individuals may be exposed to misleading or low-quality information when accessing the Internet, placing them at risk. 8 Furthermore, the acquisition of health information is uneven due to individual differences in skills and the digital divide. 9 Therefore, to navigate the complex and diverse health information available online, individuals must be well-equipped with digital health literacy (DHL) and capable of accessing the information they require. To manage the complexity and diversity of online health information, individuals require adequate DHL. 10 This is especially crucial for youth, who are undergoing critical stages of physical and mental development. DHL is the ability of an individual to locate, access, comprehend, and critically evaluate health information from digital sources, and to use this knowledge to address health-related issues. 11 Studies have demonstrated an association between DHL and various health behaviors. 12 College students with high DHL tend to perform better in health information acquisition, healthy lifestyle development, self-management, and self-efficacy.13,14
Although DHL has received growing attention in recent studies, several gaps remain. First, the target populations are relatively homogeneous: most studies focus on adults or individuals with specific health conditions,15,16 while research on the youth population iscomparatively scarce. Secondly, most existing studies use a cross-sectional design and lack longitudinal or intervention studies, making it difficult to determine the causal relationship between DHL and HLB, as well as their underlying dynamic mechanisms. Building on this, the present study systematically reviewed the literature on the associations between DHL and HLB among youth, aiming to address the following research questions: (1) What is the level of DHL among youth? (2) What is the relationship between DHL and HLB in youth? (3) How can policy and educational interventions improve DHL in youth?
2. Methods
2.1. Search strategy
This study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to conduct and report this review, with protocol registration number: CRD420251273165. In accordance with the PRISMA statement, 17 5 major English-language literature databases were systematically searched for this study, including Web of Science, Scopus, ProQuest, EBSCO and PubMed. The reference lists of relevant studies were also screened to identify potentially missing articles. The concept of DHL was first formalized by Norman and Skinner in 2006, 11 therefore, the literature search for this review was limited to publications from January 2006 to October 2025. The literature search strategy was initially developed by the authors and then reviewed by peer experts in scientific information retrieval, following the PRISMA-S (Preferred Reporting Items for Systematic Reviews and Meta-Analyses Search Extension) guidelines, which are designed to ensure a transparent and reproducible search process. The search strategy combined medical subject headings and free-text terms to construct keyword combinations around three core concepts: (1) forms of intervention (e.g., Digital Health Literacy, eHealth Literacy, e-Health Literacy, Electronic Health Literacy); (2) target behaviors (e.g., Lifestyle Behavior, Behavior Change, Health Behavior, Exercise); and (3) study populations (e.g., Adolescents, Teenagers, Youth). Boolean operators (AND, OR) were applied to balance search sensitivity and specificity. The complete English search formulas for all databases are provided in Appendix 1.
2.2. Inclusion and exclusion criteria
Based on the PICOS principles, peer-reviewed literature was screened to assess its relevance to the purpose of this study. The specific inclusion criteria were as follows: (1) Population: According to the World Health Organization, youth are defined as individuals aged 15–24 years. 18 Therefore, included studies were required to focus on participants within this age range, regardless of their health status or social identity; (2) Intervention: Studies should examine the association between DHL and youth health behaviors; (3)Comparison: Comparison groups may include traditional interventions, no intervention, or standard care, inclusion of a comparison group is not mandatory; (4) Outcomes: Studies were required to report indicators related to HLB, including physical activity, sedentary behavior, dietary habits, and sleep, and to examine their association with DHL; (5) Study Design: All types of original studies were eligible, including cross-sectional studies, cohort studies, and randomized controlled trials. Excluded literature included: (1) conference abstracts, dissertations, unpublished manuscripts, and other gray literature, as such sources often lack peer review and methodological transparency, potentially affecting study quality comparability and result reproducibility; (2) studies that did not explicitly focus on DHL, such as traditional health education or interventions not involving digital technologies; (3) studies that did not report outcomes related to HLB; and (4) studies not published in English or for which full texts were unavailable.
2.3. Study selection
All retrieved literature was imported into the Rayyan platform for de-duplication and screening. 19 Before screening, all operators received standardized training to ensure a consistent understanding of the inclusion and exclusion criteria. The first step involved two independent researchers (XRL and JJJ) screening the titles and abstracts of all initially retrieved studies. The second step consisted of a full-text review of potentially relevant studies by the same researchers (XRL and JJJ) to determine the final set of studies related to this research topic. Disagreements during the screening process were resolved through discussion. If consensus could not be reached, a third reviewer (YZH) adjudicated the conflict.
2.4. Data extraction and synthesis
Characteristics of included studies (N=33).

2.5. Quality assessment
After completing data extraction, all included studies were identified as cross-sectional. Therefore, the Joanna Briggs Institute (JBI) cross-sectional study quality assessment tool was used to evaluate the quality of the 33 included papers. The tool comprises 8 evaluation criteria, including sample representativeness, description of the study population, validity of measurement instruments, and appropriateness of statistical analyses. 53 Each criterion was scored on a dichotomous scale: 1 point if the criterion was met and 0 points if not, resulting in a total score ranging from 0 to 8. Two researchers (XRL and JJJ) independently performed the scoring, achieving an inter-rater agreement of 84.8%. In cases of disagreement, a third researcher (YZH) reviewed the scores, comparing each item with the official JBI quality assessment manual guidelines to reach consensus.
Based on relevant literature and the recommended criteria for cross-sectional study quality assessment in the JBI manual, 54 the included studies were classified as follows: (1) High-quality studies (6–8 points): studies with rigorous design, valid measurement instruments, and appropriate, fully reported statistical analyses; (2) Moderate-quality studies (3–5 points): studies with relatively reasonable design but some methodological limitations or incomplete reporting; (3)Low-quality studies (0–2 points): studies with substantial methodological flaws and incomplete reporting of results.
2.6. Coding
Each study included in the systematic review was coded as follows 55 : a positive correlation between a specific HLB and youth DHL was coded as “+”, a negative correlation as “−”, no correlation as “0”, and an uncertain relationship as “?”.
3. Results
3.1. Screening and inclusion results
3.1.1. Search and screening results
From 2,684 initially identified articles, and after removing duplicates across 5 English electronic databases, 2,061 studies proceeded to the title and abstract screening stage. After initial screening, 1,945 studies that clearly did not meet the inclusion criteria were excluded. The remaining 116 studies underwent full-text review, resulting in 25 studies meeting the inclusion criteria and 91 studies being excluded (Appendix 3) for the following reasons: (1) inappropriate document type (N=11); (2) full text unavailable (N=5); (3) did not explicitly focus on DHL (N=28); (4) no content related to HLB (N=35); and (5) study population not composed of youth (N=12). An additional eight studies were identified through manual searching of reference lists. Ultimately, a total of 33 studies met the inclusion criteria. The study screening process is illustrated in the PRISMA flow diagram (Figure 1). Prisma flow diagram of the study selection process.
3.1.2. Quality assessment results
Following quality assessment, 21 of the 33 included studies (63.6%) were rated as high-quality, 9 (27.3%) as moderate-quality, and 3 (9.1%) as low-quality (see Appendix 2). Specifically, most studies provided comprehensive descriptions of the study population, appropriate application of DHL and healthy lifestyle behavior measurement tools, and clear reporting of statistical analysis methods, demonstrating good methodological standardization. However, certain common methodological limitations were still observed in some studies. For example, many studies had relatively homogeneous samples, primarily consisting of college students, which limited sample representativeness.21,23–25,27,28 Additionally, studies varied in their control of confounding factors, with some including fewer covariates, which likely contributed to heterogeneity in the findings.32,33,37,39 In addition, most studies relied on self-reported measures of DHL and HLB,22,25–27,31 which may compromise result accuracy. Participants may have imperfect recall and may also provide responses influenced by social desirability. Overall, the included studies were of moderate or higher quality, demonstrating a reasonable degree of reliability, but further standardization in study design and implementation is warranted.
3.2. Data extraction results
Table 1 summarizes the main characteristics of the 33 included studies, all of which were cross-sectional. Most studies (N=29, 87.9%) were published after 2020, while four studies were published before 2018.24,25,38,39 Most studies were conducted in China (N=18, 54.5%), followed by Turkey (N=6, 18.3%), Pakistan (N=2, 6.1%), South Korea (N=2, 6.1%), the United States (N=1, 3%), Jordan (N=1, 3%), Indonesia (N=1, 3%), Saudi Arabia (N=1, 3%), and Iran (N=1, 3%), indicating that the majority of studies were conducted in Asia. Sample sizes ranged from 138 30 to 14892, 27 and most studies (26/33, 78.8%) recruited college students as participants.
3.2.1. The measurements of DHL and its levels among youth in the included studies
In the included studies, the 8-item Digital Health Literacy Scale (eHEALS) was the most commonly used tool, applied in 22 of 33 studies (66.7%), to evaluate DHL in youth populations. Several studies employed translated versions of the eHEALS, including the Chinese version,21,40,46–49 the Turkish version,8,29 and the Korean version, 30 These versions were validated, demonstrating good reliability and internal consistency. Additionally, five studies employed the 12-item Digital Health Literacy Scale (eHLS),23,24,32,38,39 Another five studies used the 20-item Collegiate Students’ eMedia Health Literacy Scale (CSDHLS).41,44,50–52 One study applied a subscale of the 12-item Digital Health Literacy Instrument (DHLI). 36
Among all studies, 3 did not report the DHL of their survey respondents.24,33,38 In studies using the eHEALS (maximum score 40) to measure youth DHL, the lowest score was observed in the Jordanian population (M=16.61±4.1)36, while the highest was reported in the US population (M=31.92±5.68). 25 Using a score of 26 as the threshold for high DHL,56,57 17 of the 21 studies (80.9%) exceeded this threshold, indicating that overall digital health literacy among youth is high. Findings from studies using other scales also support this conclusion.
3.2.2. Health lifestyle behaviors and their associations with DHL
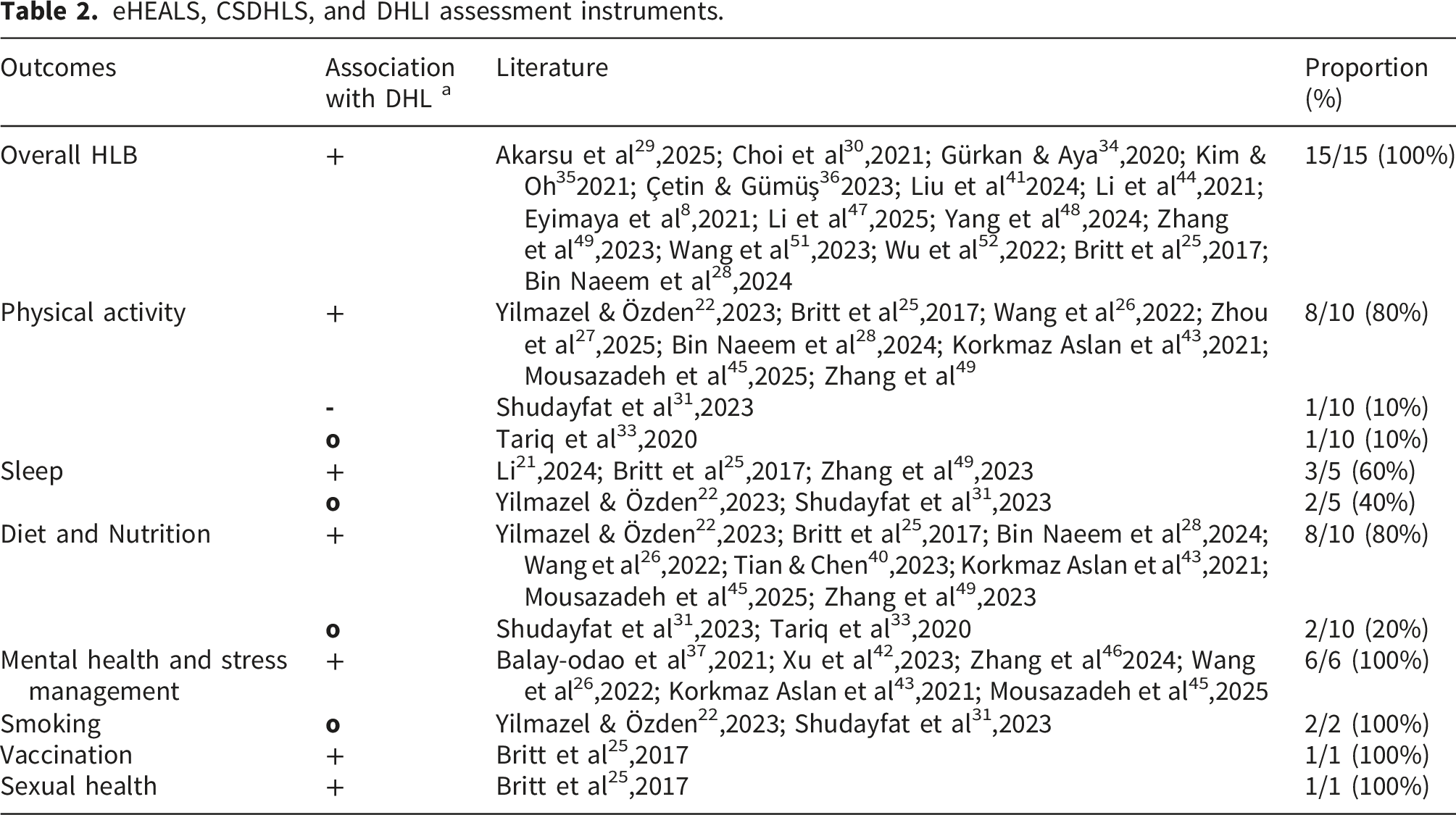
eHEALS, CSDHLS, and DHLI assessment instruments.
eHLS assessment tools.

In most studies assessing DHL with English or other language versions of eHEALS, CSDHLS, and DHLI, a consistent positive association was observed between youth DHL and HLB. According to the summary results in Table 2, all 15 studies using overall HLB as outcome indicators demonstrated a significant positive association with DHL. Notably, not all studies reported outcome indicators explicitly as HLB,25,28,29 but they were consistently categorized as such because their content was substantially equivalent.
Regarding specific HLB dimensions, physical activity and diet/nutrition were the two areas most consistently associated with DHL. Among the 10 studies that used physical activity as an outcome variable, 8 reported a positive association between DHL and physical activity. This pattern was observed in youth samples including Chinese university students, 27 Iranian medical students, 45 and Turkish students. 43 Higher DHL scores were associated with greater adherence to recommended physical activity standards set by official organizations. In contrast, Tariq’s study reported no significant correlation between DHL and physical activity. 33 This may be explained by the lack of culturally appropriate infrastructure in developing countries such as Pakistan, including safe outdoor spaces and public facilities for young females—such as sports fields, parks, and gyms—even within university campuses. 58 Shudayfat’s study found a negative correlation between DHL and physical activity, with students who never exercised exhibiting higher DHL than those exercising three times or less per week. 31 This may be because individuals who do not engage in physical activity have more time and energy to access health knowledge online.
Outcomes related to diet and nutrition behaviors were similarly characterized by positive correlations. Among the 10 studies that examined diet and nutrition behaviors as outcomes, 8 reported a significant positive correlation between DHL and healthy eating behaviors. Youth with higher DHL scored higher on the Eating Behavior Scale.22,25,26,28,43,45,49 Additionally, studies have shown that higher DHL is associated with lower fear of novel foods among college students, suggesting a potential link between DHL and greater openness toward food. 40 In contrast, two studies with Jordanian and Pakistani youth samples found no significant association between DHL and dietary supplement use or specific dietary behaviors,31,33 suggesting that dietary behaviors are largely influenced by factors such as cultural preferences.
Evidence on sleep-related behaviors shows some inconsistency. 3 out of 5 studies reported significant positive associations between DHL and sleep among youth.21,25,49 In contrast, studies involving Turkish and Jordanian youth did not find a significant association between DHL and sleep.22,31 The association between DHL and sleep appears less consistent than its association with physical activity and dietary behaviors. This inconsistency may be due to the influence of multiple external factors on sleep, including academic pressures, work-rest schedules, and social rhythms.
Regarding mental health and stress management, existing research demonstrates a consistent positive trend. Six studies reported a significant positive correlation between DHL and mental health among young people. Specifically, studies involving Saudi nursing students, young digital media users in China, and undergraduate nursing students indicated that higher DHL was associated with higher self-assessed mental health scores.37,42,46 In both Chinese and Turkish studies, higher DHL among youth was associated with higher scores in effective stress management behaviors and mental health-promoting lifestyle measures.26,43,45 This suggests that DHL is not only associated with physical lifestyle behaviors but may also be closely linked to mental health status in youth who primarily rely on the Internet and social media for information.
The number of studies investigating risky and preventive behaviors is relatively limited. Two studies examining smoking behaviors found no significant association between DHL and smoking status among youth.22,31 This suggests that DHL is not yet a reliable predictor of whether a young person smokes or their smoking frequency. In contrast, a study of US college students found that individuals with higher DHL literacy were more likely to complete vaccinations and practice safer sexual behaviors. 25 These findings suggest that DHL plays a more prominent role in preventive behaviors that require proactive access to and evaluation of professional health information. In contrast, its association with smoking behaviors appears weaker, likely due to strong influences from peer norms, family environment, and addiction mechanisms.
The eHealth Literacy Scale (eHLS) comprises 12 items across three dimensions: functional DHL (3 items), interactive DHL (4 items), and critical DHL (5 items). 59 Functional DHL evaluates the extent to which an individual applies their reading and writing skills to comprehend basic online health information. Interactive DHL evaluates their ability to apply these skills to access and extract information from diverse social online environments. Critical DHL measures their capacity to critically appraise online health information and make informed health decisions based on this evaluation. As shown in Tables 3 and in Shoji’s study, 32 all three types of DHL among youth were positively correlated with HLB, indicating that higher DHL is associated with a greater likelihood of adopting healthier lifestyle behaviors. In the remaining 4 studies,23,24,38,39 critical DHL showed a consistently positive correlation with youth HLB, including diet and physical activity. In contrast, correlations between functional or interactive DHL and these HLB were generally weaker. These findings suggest that while youths’ abilities to comprehend health information and engage interactively are foundational to DHL, their associations with HLB are not consistently stable. Critical DHL represents a higher-order cognitive ability compared with functional and interactive DHL. 60 Accessing health information alone is insufficient,individuals also need to critically evaluate it and apply it to informed health decisions.
3.2.3. Potential mediators and moderators of the effect of DHL
Mediating variables are factors that explain the mechanisms linking DHL to HLB. Among the 33 included studies, four investigated potential mediators in the relationship between DHL and HLB. The studies found that physical literacy, 29 peer relationships, 27 health self-management skills, 46 self-care behaviors, social media use, and health information-seeking behaviors mediate the relationship between DHL and outcomes such as sustainable healthy lifestyles, physical activity, mental health, and health promotion behaviors. 35 Moderator variables influence the strength or direction of the association between DHL and HLB. However, research on their moderating effects remains limited. A study of college students reported that sleep quality significantly moderated the relationship between DHL and physical activity. 27 Specifically, the positive association between DHL and physical activity was weaker when sleep quality was poor. These findings suggest that moderators, including individual states and contextual factors, should be considered when examining the role of DHL.
4. Discussions
This study systematically reviewed and synthesized evidence on the association between DHL and HLB among youth. Specifically, the study presented a measurement tool for assessing youth DHL and its levels. It also categorized the HLB examined in the included studies and summarized their associations with DHL. This suggests that, when explaining the association between DHL and HLB, it is important to consider the variability in the plasticity of different types of health behaviors and their context-dependence. 61 Based on the COM-B Behavioral Change Model, this study suggests that DHL primarily functions as a foundational competency that supports health decision-making and the implementation of behaviors. This competency interacts with real-world contexts, social support, and the behavioral environment. From the perspective of the interplay among competencies, opportunities, and motivations, DHL, combined with contextual factors such as the real environment, social support, and individual behavioral willingness, influences actual health behaviors in youth.
Studies consistently show that youth DHL is significantly and positively associated with healthier lifestyles, particularly from the perspective of overall HLB. This finding aligns with established evidence at the broader population level.12,62 From a behavioral change perspective, youth with higher DHL are more likely to identify and evaluate credible health information, understand its applicability, and translate it into actionable behaviors. 63 This provides the necessary foundation for implementing HLB. DHL may play a crucial role in enabling the formation of HLB among youth. HLB are not solely the result of applying one piece of knowledge. They also depend on supportive external conditions in schools, families, and digital environments, as well as youth’s willingness to maintain healthy behaviors and their self-management tendencies. As such, they reflect the combined influence of individual capabilities, real-world conditions, and behavioral dispositions. Therefore, a longitudinal study is needed to assess whether DHL can continuously influence HLB during youth development. At the practical level, DHL should be considered a foundational competency in health promotion programs. It should be integrated with various behaviors to implement comprehensive interventions, rather than focusing on sporadic interventions targeting a single HLB.
Most studies in the area of physical activity have found a positive association between DHL and physical activity, although a few have reported no association or negative results. The global prevalence of physical inactivity among adolescents, 3 DHL provides a cognitive foundation for promoting physical activity among youth. It helps youth identify problematic exercise prescriptions, understand the risks and benefits of exercise, and use digital tools for goal-setting, feedback monitoring, and social support to enhance exercise participation.64,65 Critical DHL can help individuals assess the credibility of exercise-related information, understand the context in which different exercise recommendations apply, and make informed judgments about the content. Physical activity, however, is highly dependent on real-world conditions and resources. For young people, even with high levels of critical DHL, factors such as scheduling, available facilities, peer environments, and family support may present constraints.66–70 Future research should systematically consider opportunity factors, such as the social environment and resource accessibility, as potential moderating variables to clarify the role of DHL in different physical activity contexts.
The available evidence generally shows a positive correlation between DHL and diet and nutrition, although a few studies have found no significant association. Youth with higher DHL are typically better able to understand nutritional advice, assess the credibility of online dietary information, and make healthier dietary choices, 71 providing a cognitive foundation for developing healthy eating behaviors. Youth with higher critical DHL are more likely to make prudent judgments about dietary advice, commercial promotions, and faddish health information online. However, this may not always translate into the adoption of healthy eating behaviors in their daily lives. Dietary behavior is not only an active health choice but is also deeply influenced by family culture, economic conditions, and social norms.72,73 It is largely shaped by factors such as food price, convenience, dietary preferences, and sociocultural influences. Future studies should distinguish between different types of dietary behaviors, such as “dietary intake structure” and “motivation for dietary behaviors,” and incorporate factors such as accessibility and social norms. This will help better identify the explanatory power of DHL across various dietary behavior dimensions.
Research on sleep-related behaviors shows more significant inconsistencies than studies on physical activity and dietary behaviors. Youth with higher levels of DHL may be more knowledgeable about sleep hygiene but are still affected by external factors such as academic pressures, work schedules, and social rhythms, which can more strongly constrain their sleep behaviors. In this context, even with high levels of DHL, young people may still struggle to achieve the recommended 8-10 hours of high-quality sleep due to the constraints of work schedules and environmental pressures. 74 Additionally, behaviors such as staying up late and scrolling before bedtime are often driven by habitual tendencies and a desire for instant gratification. 75 Therefore, simply enhancing youth’s understanding of sleep literacy may not be enough to bring about lasting changes in their routines. As a result, the association between DHL and sleep behavior is less stable than its relationship with physical activity and eating behaviors. Future studies could adopt a longitudinal design to further examine the relationship between DHL, media use, and sleep. This would help avoid explanatory bias caused by reverse causality and potential confounders in cross-sectional studies.
In the field of mental health and stress management, existing studies consistently show positive associations. Given youth’s high reliance on the Internet for mental health information, DHL, as a key psychological competency, may serve as the foundation for positive help-seeking and coping behaviors by enhancing the ability to identify information and access resources. This competency is more likely to translate into effective stress management behaviors when influenced by opportunistic factors, such as the availability of online support and service resources.
76
These behaviors, in turn, are positively associated with higher levels of psychological well-being. Mental health-related behaviors depend not only on an individual’s ability to recognize and understand information but also on their willingness to seek help and develop positive coping strategies
77
DHL does not show a stable association with smoking behavior. This may suggest that smoking behavior is more influenced by a combination of addictive mechanisms, social environment, and psychological factors, and that behavior maintenance and change are not primarily dependent on an individual’s ability to understand health information. Even when youth understand the harms of smoking and recognize cessation messages, they may still struggle to change their behavior, as smoking is strongly associated with peer norms, emotional regulation needs, and habitual responses over time. 81 In addition, the analysis is limited by the small number of studies included and by differences in the measurement of the indicator outcomes. As a result, drawing robust conclusions is challenging at this time. In contrast, vaccination and other disease prevention behaviors are more strongly associated with DHL. These behaviors depend heavily on an individual’s ability to actively obtain, understand, evaluate health information, and make informed decisions and take appropriate action. Future studies should integrate various types of health behaviors to better distinguish the role of DHL in information-driven behaviors versus those driven by habits or addiction. It is essential to develop more specific theoretical models to comprehensively identify the boundaries of DHL’s role in preventing risky behaviors.
In addition, regarding DHL, this study indicates that the youth group as a whole exhibits a high level of DHL. This characteristic was particularly evident in the study focusing on college students as the main sample. It may be closely related to the group’s higher education level, more frequent Internet use, and greater familiarity with digital technology.82,83 However, this result was also partly influenced by the selection of the DHL measurement tool. Most of the included studies utilized the eHEALs, a widely used tool. However, the eHEALs primarily assesses individuals’ DHL based on self-perception, reflecting their subjective views of digital health competence. This tool is favored in research due to its simple structure, low administration costs, clear and intuitive item presentation, and availability in multiple languages. However, it does not assess individuals’ actual ability to function in real, complex digital health contexts, which can lead to an overestimation of their DHL levels. 84 In fact, it does not adequately reflect the competencies required to operate effectively in complex digital health environments. Meanwhile, some of the included studies used a multidimensional measurement tool, the eHLS. The results indicate that youth groups perform unevenly across the dimensions of DHL, and performance in each dimension does not necessarily correlate with the strengths reflected in the overall scores. This suggests that evaluating the level of DHL among youth based solely on the overall score may overlook potential deficiencies in higher-order competency dimensions. In the current digital health environment, where social media, algorithmic recommendations, and interactive platforms are widely used, the competencies required by the population are no longer limited to youth accessing information. Rather, they should include a comprehensive ability to assess the reliability of information, recognize its commercial or misleading content, and use it appropriately in specific contexts.85,86 Consequently, the conclusion of this review—that “youth DHL levels are high”—should be interpreted within the context of specific measurement instruments and research settings. Future research should adopt or develop measurement tools that capture the multidimensional nature of DHL in youth populations. 87 Additionally, combining objective and expressive indicators is essential to provide a more comprehensive assessment of youth competency levels in real digital health settings. This approach will not only enhance the explanatory power of the study’s findings but also provide a more precise basis for DHL interventions targeting youth groups.
Another significant finding of this review arises from a dimensional analysis of DHL. Studies using the eHLS tool to categorize DHL into functional, interactive, and critical dimensions revealed that the association between critical DHL and HLB was more stable. In contrast, the associations between the functional and interactive dimensions and certain outcome indicators were weaker and exhibited some inconsistency. Regarding the competency structure, critical competency emphasizes in-depth analysis and careful judgment of the quality and meaning of information, which represents a higher level of cognitive engagement. 88 This type of competency is more likely to influence youth’s ability to make informed choices in a complex information environment and to translate health information into accurate, scientifically supported, and sustainable health behaviors. Based on this finding, improving youth DHL should go beyond simply enabling them to search for information or access resources. 71 Greater emphasis should be placed on developing the following competencies: recognizing the credibility of information, identifying commercialized and misleading content, understanding the hierarchy of health evidence and its scope of application, 89 and making rational health decisions amidst multiple or conflicting sources of information.
Additionally, some studies have started to explore the mediating and moderating roles of DHL in the development of HLB. For instance, some studies have suggested that DHL may mediate the relationship between individual factors and HLB. 29 Other studies have developed a multiple mediation model using a sample of nursing students to explain the link between DHL and health-promoting behaviors. 46 Additionally, some studies have employed a moderating mediator model to further investigate the impact of health literacy on differences in physical activity and health-promoting behaviors. A moderated mediation model was also employed to further examine the pathways through which DHL affects physical activity behaviors. 27 These studies provide a foundation for understanding why DHL is associated with health behaviors. DHL may promote the development of HLB by enhancing individuals’ health self-efficacy, improving access to health information, strengthening social support, and increasing health motivation. However, since most existing studies are cross-sectional in design, the causal relationships and their pathways need to be further explored through longitudinal or intervention studies. Simultaneously, attention must be given to the potential for reverse causality, where healthy youth with higher levels of healthy behaviors may be more likely to proactively access health information, thereby exhibiting higher DHL.
Based on these findings, this review offers valuable insights for youth health promotion practices. First, DHL should be considered a key foundational competency for youth health promotion. It may not only be linked to traditional HLB such as physical activity and diet, but also closely associated with mental health and stress management. Second, health education at the school and community levels should incorporate DHL into the curriculum and program design, focusing on improving young people’s ability to access health information. Since young people predominantly rely on social media for information, the focus should be on enhancing their ability to critically evaluate and apply health information, rather than merely training them in technical operations or information retrieval skills. Third, given that young people predominantly acquire information through social media and mobile platforms, health intervention designs should be fully integrated with actual digital contexts, incorporating “information recognition training,” “evidence-based information assessment,” and “health decision-making scenario rehearsal.” Health intervention designs should fully integrate with actual digital contexts, such as “information recognition training,” “evidence-based information assessment,” and “health decision-making scenarios” to enhance the transferability and practical impact of interventions. Lastly, intervention strategies for different HLB should adhere to the principle of localized adaptation. Finally, intervention strategies for various HLB should be adapted to the local context. For example, interventions in areas such as sleep may need to incorporate strategies like time management, academic stress management, and media use management to more effectively translate DHL into behavioral improvements.
5. Limitations
This review has several limitations. First, this review included studies that reported the association between DHL and HLB among youth, but it did not limit the statistical analysis methods used. Due to differences in the control of confounders across studies, the results may not be fully consistent, which increases the complexity of cross-study comparisons. Second, some specific HLB, such as smoking, vaccination, and sexual health, were reported in only 1-2 studies. The available evidence is insufficient to fully support their association, and more studies are needed to further validate these findings. Thirdly, this review excluded non-Chinese and non-English literature, which limits the generalizability of the findings to studies published in other languages. Most of the included studies used the eHEALs scale to assess DHL, which may have resulted in an overestimation of DHL compared to the general youth population. Finally, the included studies were cross-sectional and predominantly focused on college students. Future research should include longitudinal studies and randomized controlled trials across broader regions, with a more representative sample of young people, to provide stronger evidence supporting the development of precise and stratified youth health promotion strategies.
6. Conclusions
Although the number of studies on DHL has increased in recent years, the understanding of the association between DHL and HLB among youth remains limited. The findings of this review indicate that the overall level of DHL among youth is relatively high, and it is positively associated with HLB. However, this association has not been consistently observed across certain health risk behaviors, such as sleep and smoking. Therefore, it is essential to conduct more high-quality longitudinal and intervention studies in the future to further elucidate the causal relationship between DHL and specific HLB, as well as their underlying mechanisms. This will provide a stronger theoretical foundation for designing digital health interventions for the youth population. Simultaneously, with the ongoing development of digital health tools and social media platforms, it is important to revise and improve existing DHL assessment tools to more comprehensively reflect the competencies and behaviors of youth in the diverse digital health resource environment.
Supplemental material
Supplemental material - The association between digital health literacy and healthy lifestyle behaviors among youth: Systematic review of cross-sectional studies
Supplemental material for The association between digital health literacy and healthy lifestyle behaviors among youth: Systematic review of cross-sectional studies by Ruilin Xu, Jiajun Jiang, Zhihua Yin, Qiying Zhong, Duoer Liu, Mingzhu Sun and Mingliang Xiong in DIGITAL HEALTH.
Supplemental material
Supplemental material - The association between digital health literacy and healthy lifestyle behaviors among youth: Systematic review of cross-sectional studies
Supplemental material for The association between digital health literacy and healthy lifestyle behaviors among youth: Systematic review of cross-sectional studies by Ruilin Xu, Jiajun Jiang, Zhihua Yin, Qiying Zhong, Duoer Liu, Mingzhu Sun and Mingliang Xiong in DIGITAL HEALTH.
Supplemental material
Supplemental material - The association between digital health literacy and healthy lifestyle behaviors among youth: Systematic review of cross-sectional studies
Supplemental material for The association between digital health literacy and healthy lifestyle behaviors among youth: Systematic review of cross-sectional studies by Ruilin Xu, Jiajun Jiang, Zhihua Yin, Qiying Zhong, Duoer Liu, Mingzhu Sun and Mingliang Xiong in DIGITAL HEALTH.
Footnotes
Acknowledgements
The authors thank the participants of this study for their time and dedication.
Ethical considerations
This study did not involve human participants, patient-identifiable data, or animal experiments, and therefore ethical approval was not required.
Consent for publication
This manuscript is original and has not been published previously, in whole or in part, and is not under consideration for publication elsewhere. The manuscript is not simultaneously submitted to any other journal or conference. All authors have approved the submission to the Digital Health.
Author Contributions
XRL designed the study, completed the data analysis, and manuscript writing. JJJ and ZQY collected the data. YZH and SMZ revised the manuscript. LDE and XML provided ideas for revisions and assist in paper revisions. All authors approved the final manuscript. All listed authors meet the authorship criteria and have made substantial contributions to the conception and design of the study, data acquisition, analysis or interpretation, drafting of the manuscript or critical revision for important intellectual content. All authors have read and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Projects of Post-Funded project of China National Social Science Foundation, grant number 25FTYB012; General Project of Shanghai Philosophy and Social Science Foundation, grant number 2025BTY002; Youth Project of Shanghai Eastern Talent Plan, grant number QNJY2025162.The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated or analyzed during this study are available from the corresponding author on reasonable request.
Copyright agreement
The authors agree that, upon acceptance of the manuscript, the copyright or license agreement will be completed in accordance with Elsevier and journal policies.
Data integrity and research integrity
The authors confirm that the data and results presented in this manuscript are accurate and reliable. No data have been fabricated, falsified, or inappropriately manipulated.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.