
Abstract
Purpose
To evaluate the accuracy, stability, and dynamic BP tracking capability of a cuffless continuous non-invasive blood pressure (CNIBP) wearable system (Shenzhen Mindray Bio-Medical Electronics Co., Ltd.) to track dynamic blood pressure (BP) changes in intensive care unit (ICU) patients.
Methods
A multicenter, prospective clinical trial enrolled ICU patients aged ≥ 12 years who required continuous invasive blood pressure (IBP) monitoring for ≥ 24 h. The mWear wearable monitoring system (Mindray) served as the test device, with IBP as the reference standard. The study followed the International Organization for Standardization (ISO) 81060-3:2022 guidelines to evaluate the accuracy, stability, and dynamic BP tracking.
Results
Forty-nine participants (mean age, 57.3 ± 18.7 years) were included in the study. The mean differences between CNIBP and IBP measurements for systolic blood pressure (SBP), diastolic blood pressure (DBP), and mean arterial pressure (MAP) were -0.31 mmHg, -0.81 mmHg, and -0.37 mmHg, respectively, all within the predefined 95% confidence interval (CI). The corrected experimental standard deviations (SD) were 5.3, 3.6, and 3.6 mmHg, respectively, consistent with the ISO 81060-3:2022 criteria (mean difference: -6 to 6 mmHg; corrected experimental SD: ≤10 mmHg). The Pearson correlation coefficient (PCC) exceeded 0.9, indicating a strong linear correlation. Stability assessments demonstrated that CNIBP remained within ISO error ranges over 24 h. For BP change-tracking ability, the median absolute error (E percent , 50th percentile) averaged ≤25%, and the 85th percentile averaged ≤50%, both of which met ISO requirements.
Conclusion
The findings indicate that CNIBP device measurements are consistent with IBP readings in terms of accuracy, stability, and dynamic BP tracking capability within the ICU. This consistency effectively supports real-time hemodynamic assessment in critically ill patients.
Keywords
Introduction
Blood pressure (BP) is a fundamental vital sign routinely monitored in intensive care unit (ICU) patients. Dynamic fluctuations in BP reflect the underlying physiological state and may indicate pathological processes associated with adverse outcomes.1,2 Therefore, real-time, accurate, and continuous BP monitoring is essential for timely clinical decision-making and effective therapeutic interventions in critically ill patients.
Invasive blood pressure (IBP) monitoring provides a direct measurement of intravascular pressure via an arterial catheter and is widely regarded as the gold standard for continuous BP assessment. 3 Despite its accuracy, IBP is associated with risks, such as infection, 4 catheter insertion failure, and artifacts resulting from resonance and damping effects. 5 Additional technical challenges may also arise in patients with peripheral vascular abnormalities. 6 In contrast, traditional cuff-based non-invasive blood pressure (NIBP) monitoring—including oscillometric 7 and auscultatory methods 8 —avoids vascular puncture; however, it remains intermittent, time-consuming, and sensitive to variations in cuff size, 9 placement, patient position, 10 age, 11 and arterial stiffness, which can compromise measurement accuracy. 12 Moreover, its inability to provide continuous BP monitoring may lead to missed or delayed detection of hypotensive events during anaesthetic induction. 13
The introduction of cuffless continuous BP monitoring systems have emerged to address the limitations of traditional cuff-based methods. Early investigations began in 1963 with arterial tension measurement, 14 followed by the introduction of continuous finger-cuff BP monitoring technology using the volume-clamp method. 15 More recently, advancements in sensors and signal processing have enabled the development of estimation methods based on pulse wave velocity (PWV) and pulse wave analysis (PWA), which have become prominent areas of research. 16 Despite the diversification of these technological approaches, cuffless devices still face challenges related to measurement accuracy, individual calibration, and clinical validation.
To address these limitations, Shenzhen Mindray Bio-Medical Electronics Co., Ltd. developed a new type of cuffless BP monitor based on the pulse wave transit time (PWTT) principle. PWTT refers to the time interval between the R wave of the electrocardiogram (ECG) and the arrival of the peripheral photoplethysmography (PPG) signal. This technology is integrated into a wearable terminal, enabling continuous non-invasive BP monitoring. Compared with traditional cuff-based devices, the wrist-worn design enhances patient comfort. Moreover, unlike devices that only support intermittent measurements 17 or exhibit 24h drift,18,19 this device provides true continuous output and can accurately track rapid BP fluctuations.
This study is the first to systematically validate the accuracy, long-term stability, and dynamic tracking capability of a wrist-worn, continuous non-invasive blood pressure (CNIBP) monitoring device based on PWTT in an ICU setting, in accordance with the International Organization for Standardization (ISO) 81060-3:2022. 20 Unlike previous studies that focused only on short-term accuracy, this standard provides a more comprehensive statistical framework, enhancing the reliability of the evaluation. The present validation establishes a solid foundation for the clinical application of CNIBP monitoring in critically ill patients. This approach offers a safe and effective alternative, particularly when arterial cannulation is contraindicated or prolonged monitoring is required, thereby supporting real-time hemodynamic management.
Methods
Written informed consent was obtained from all participants or their legal guardians prior to enrollment in the study.
Device details
Test Device: The mWear wearable monitoring system (Shenzhen Mindray Bio-Medical Electronics Co., Ltd.) was utilized, comprising an EP30 main unit, a pulse oximetry sensor, a 3-lead ECG, and a multi-parameter mobile module (ES30) for CNIBP monitoring based on PWTT (Figure S1). The device provides CNIBP readings at a minimum interval of 3 s and requires recalibration every 24 h. Additional physiological parameters measured included body temperature, oxygen saturation (SpO2), and respiratory rate (RR), with all data displayed on a monitor for clinical analysis.
Reference Standard: In accordance with ISO 81060-3:2022, CNIBP measurements were compared with IBP values obtained from arterial catheters placed in the radial, brachial, or femoral arteries. CNIBP data were collected using an ePM 12M patient monitor (Shenzhen Mindray Bio-Medical Electronics Co., Ltd.).
Device familiarization
The research team comprised ICU nurses, each with at least five years of clinical experience and having performed over 400 IBP measurements. All procedures were conducted in strict accordance with ISO 81060-3:2022, a joint standard issued by the International Organization for Standardization (ISO) and the International Electrotechnical Commission (IEC), ensuring methodological rigor. To ensure standardized data collection, the team underwent a familiarization phase with the device and calibration measurement process prior to study initiation and protocol implementation.
Sample size
The sample size was determined in accordance with ISO 81060-3:2022 guidelines. 20 An estimated intraclass correlation coefficient (I CC_est = 0.87) for systolic, diastolic, and mean arterial pressures was derived from preliminary pilot data. A minimum sample size of 45 participants was required to ensure sufficient statistical power and meet the relevant regulatory requirements (see Equations S1-S5 and S8 in the Supplementary Material).
Recruitment
This multicenter, prospective trial recruited participants between January 8 and August 14, 2024, from the ICUs of three tertiary hospitals in Shenzhen, China: Shenzhen People’s Hospital, Shenzhen Bao’an District People’s Hospital, and Huazhong University of Science and Technology Union Shenzhen Hospital. Following screening and written informed consent, 54 participants were enrolled. Of these 49 participants who met the inclusion criteria—being over 12 years of age and requiring continuous IBP monitoring for ≥ 24 h via arterial catheters in the radial, brachial, or ulnar arteries—were ultimately included in the study.
The exclusion criteria were as follows: a perfusion index (PI) below 0.3; persistent agitation or tremors; pregnancy, frequent arrhythmias such as atrial fibrillation (AF); concurrent participation in other clinical trials; and investigator-determined unsuitability. Participants who withdrew voluntarily, did not complete 24 h monitoring, or experienced technical disruptions were excluded from the final analysis (Figure S2).
Blood pressure measurement procedure
Patients in the ICU who required continuous IBP monitoring for ≥ 24 h due to clinical necessity were enrolled in this study. All participants were bedridden and simultaneously connected to both the CNIBP device and an IBP system during data acquisition. Prior to trial initiation, arterial catheter placement was verified to ensure that the IBP transducer was positioned at the level of the right atrium. The CNIBP device was applied according to the manufacturer’s guidelines, with both CNIBP and IBP monitoring performed on the same upper limb and the SpO2 probe aligned at heart level. Initial IBP values were used to calibrate the CNIBP device, and the calibration time was recorded. Continuous BP data, including systolic blood pressure (SBP), diastolic blood pressure (DBP), and mean arterial pressure (MAP), were collected ≥ 24 h post-calibration. If the vasoactive drug regimen was modified, including initiation, discontinuation, or dose adjustment, the device was recalibrated within 5 min, and a new 24 h data collection cycle was initiated. No adverse events related to device wearing or arterial catheterization were observed during the study period.
All calibrations in this study were conducted using invasive BP readings to ensure the accuracy of the reference standard and rigorously validate the sensor tracking algorithm, thereby minimizing confounding errors associated with oscillometric cuffs. However, in routine clinical practice, the device is calibrated using standard oscillometric non-invasive BP measurements. During data collection, significant signal artifacts or technical interruptions—such as changes in patient position, suctioning procedures, or temporary sensor detachment—led to the immediate marking and exclusion of the affected data segments to maintain the integrity of paired continuous non-invasive and invasive BP measurements. Research nurses who received standardized training recorded all exclusion decisions in real time according to predefined criteria, documenting both the reason for exclusion and its duration to ensure consistency and objectivity. Because exclusion events primarily resulted from transient, random clinical procedures and were not systematically associated with patient severity of condition or BP levels, the risk of selection bias was considered negligible. In clinical emergencies, data were retained whenever signal quality was sufficient, reflecting real-world monitoring conditions. The study protocol did not interfere with routine clinical management, thereby allowing for the natural observation of hemodynamic parameters.
Data preparation
The performance of the CNIBP device was evaluated across three dimensions: accuracy, stability, and BP change-tracking capability, in accordance with ISO 81060-3:2022. The methodology is described in detail below.
For the accuracy assessment, the CNIBP device had a minimum output period of 3 s. In accordance with standard requirements, the IBP data were divided into non-overlapping segments at 1-min intervals. The average value of each segment (Pref j , is the j th reference reading from the first analysis period of the first test period of the i th subject) was paired with the CNIBP output value at the end of the segment (Psut j , is the j th BP determination from the first analysis period of the first test period of the i th subject) to form a paired dataset for accuracy evaluation (Figure S3). The difference x j was then calculated using Equation S1.
Stability assessment: Given the device maximum re-initialization time of 24 h, six accuracy tests were performed (five within the first 5 h and one at the end of the initialization cycle), each lasting approximately 15 min. The test period was divided into equal analysis and interval segments. With 44 repeated measurements per participant and a CNIBP minimum output cycle of 3 s, each analysis segment lasted 2.5 min. Synchronized CNIBP and IBP data were collected during these segments to form a paired dataset for the stability assessment (Figure S4).
To assess the ability to track BP changes, continuous BP data were collected for 30 min following calibration. Given the device interpretation change evaluation interval (I CE ) is 120s, BP changes during this interval were calculated using (Equation S9), with t start and t end representing the start and end times of BP fluctuations, respectively. For the CNIBP to be considered capable of accurately tracking BP changes within I CE , the analysis segment was required to contain more than 50 BP fluctuations. A BP fluctuation was defined as a change in IBP or CNIBP, where the absolute value of ΔP meets SBP ΔP ≥ 15 mmHg, DBP ΔP ≥ 10 mmHg, or MAP ΔP ≥ 12 mmHg (Equation S10). The absolute error was calculated using (Equation S11), and the specific values are shown in Figure S5.
Statistical analyses
All statistical analyses were performed using SPSS (Version 29.0.1.0). BP values are reported as the mean ± standard deviation (SD), age as the median ± interquartile range (IQR), and categorical variables as percentages.
The accuracy and stability of CNIBP were evaluated using mean error (x̄, Equation S6) and corrected standard deviation (
Results
Participants demographics
Clinical characteristics of the study participants.
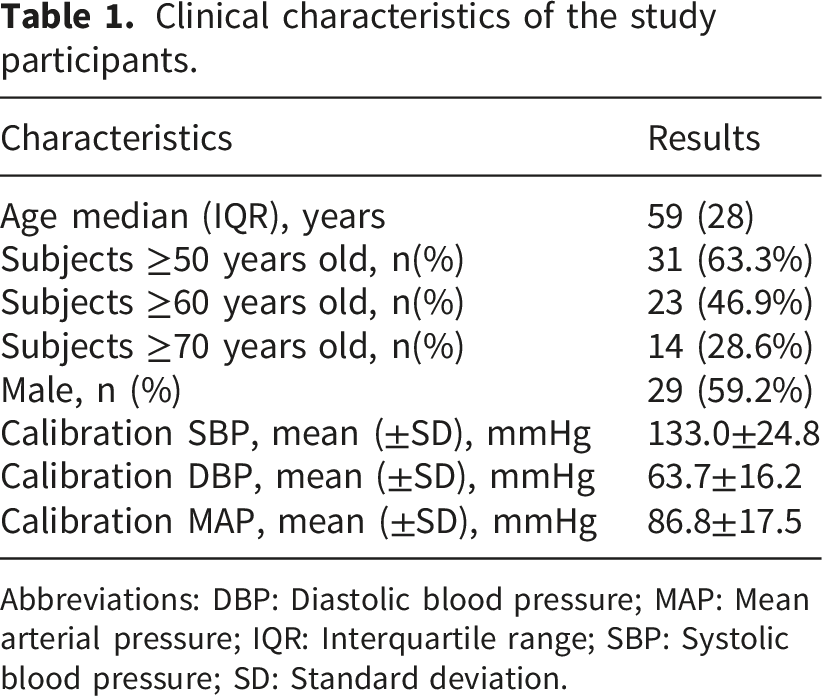
Abbreviations: DBP: Diastolic blood pressure; MAP: Mean arterial pressure; IQR: Interquartile range; SBP: Systolic blood pressure; SD: Standard deviation.
Assessment of BP accuracy
Agreement between continuous non-invasive blood pressure and invasive blood pressure for accuracy assessment.

Abbreviations: BP: Blood pressure; CNIBP: Continuous non-invasive blood pressure; CI: Confidence interval; DBP: Diastolic blood pressure; MAP: Mean arterial pressure; N
ind:
The number of independent measurements; PCC: Pearson correlation coefficient; SBP: Systolic blood pressure;

Bland-Altman plot comparing the continuous non-invasive blood pressure and invasive blood pressure device. Note that “ME” (Mean error) in the figure is equivalent to
Results for assessment of BP stability
Agreement between continuous non-invasive blood pressure and invasive blood pressure for stability assessment.

Abbreviations: Anal. Per.: Analysis Period; BP: Blood pressure; CNIBP: Continuous non-invasive blood pressure; DBP: Diastolic blood pressure; IBP: Invasive blood pressure; MAP: Mean arterial pressure; Nind: the number of independent measurements; SBP: Systolic blood pressure;
Assessment of tracking dynamic BP changes
Agreement between continuous non-invasive blood pressure and invasive blood pressure for blood pressure changes assessment.

Abbreviations: BP: Blood pressure; DBP: Diastolic blood pressure; MAP: Mean arterial pressure; SBP: Systolic blood pressure.
Discussion
This study is the first to investigate the PWTT-based BP device in routine clinical use across three critical dimensions: accuracy, stability, and BP change tracking capability, in strict adherence to ISO 81060-3:2022 guidelines. The results demonstrate that the CNIBP device achieves clinically acceptable agreement with IBP measurements (the gold standard). Both
The wrist-worn CNIBP device evaluated in this study is user-friendly, transmitting data in real time via Bluetooth to the bedside monitor without interfering with nursing procedures, such as patient turning or suctioning. Nurses reported that the device was convenient to use. Calibration is required every 24 h, and recalibration must occur within 5 min following adjustments to vasoactive medications. On average, one to two planned calibrations were performed per case, each taking approximately 30 sec, resulting in minimal disruption to the clinical workflow. However, frequent calibration during periods of rapid hemodynamic change may increase the nursing workload and may require further optimization. The device is reuseable, offering long-term cost advantages compared to single-use arterial catheters. Proficiency in device operation can be achieved after 30 min of standardized training, with no additional personnel required.
Compared to conventional methods, PWTT-based CNIBP offers several advantages over traditional oscillometric cuff-based NIBP techniques. These advantages include continuous 24 h monitoring for dynamic BP tracking, which enhances clinical sensitivity and early warning capabilities. The real-time responsiveness of PWTT-based CNIBP enables detection of rapid BP changes with minimal latency. Compared to IBP methods, PWTT-based CNIBP reduces safety risks by eliminating those associated with arterial puncture, making it suitable for patients with vascular abnormalities or coagulation disorders. Additionally, its wearable design enhances patient comfort, reduces procedural complexity, and improves patient compliance.
Current NIBP measurement technologies offer distinct advantages and limitations. Sleeveless watch-style devices that utilize PPG and PWA 21 provide convenient wearability, making them suitable for outpatient settings and long-term hypertension management. However, their accuracy is compromised by limb movement and hypoperfusion, and these devices often fail to capture rapid BP fluctuations in real time, limiting their applicability in hemodynamically unstable intensive care environments. Finger-ring devices employing pulse decomposition analysis (PDA) 22 deliver beat-by-beat BP waveforms with high temporal resolution and have been validated in ICU patients. However, the finger-ring design can cause discomfort and venous congestion, limiting prolonged use. Additionally, the validation of these devices was performed according to earlier intermittent BP monitoring standards (ANSI/AAMI/ISO 81060-2:2013), which are less rigorous than the latest standards for continuous monitoring, particularly regarding dynamic BP tracking and long-term stability.
Several CNIBP monitoring devices utilizing PWTT technology have been reported. For example, the chest-adhesive device developed by John Smith et al. 23 integrates the monitoring of multiple physiological parameters, including SpO2, heart rate (HR), BP, RR, body temperature, and hemodynamics. However, this device supports only the “spot-check” mode and does not enable high-frequency continuous BP monitoring, thus limiting its application in the real-time management of critical emergencies. Moreover, Hellou et al. 24 applied similar technology to post-cardiac surgery patients, but their validation focused primarily on accuracy and did not systematically assess long-term stability or dynamic tracking in accordance with ISO 81060-3:2022. Similarly, the cuffless PWTT device examined by Krisai et al. 25 demonstrated satisfactory short-term accuracy and performed effectively in both outpatient and hypertensive populations. However, it showed systematic overestimation during 24 h monitoring, particularly at night, with deviations of up to 15–18 mmHg compared to reference measurements, limiting its reliability for full-day monitoring.
In contrast, the PWTT-based mWear wrist-worn device evaluated in this study integrates ECG and PPG signals, thereby providing enhanced physiological validity and plausibility, and greater resistance to signal interference. The device enables continuous monitoring at intervals of at least 3 sec. Its wrist-worn design optimizes patient comfort and supports long-term wearability, extending recalibration intervals to 24 h. This study complies with ISO 81060-3:2022 by systematically validating measurement accuracy, long-term stability, and dynamic BP tracking capability in hemodynamically complex ICU patients. These features build upon existing evidence and collectively advance cuffless continuous BP monitoring technology towards standardization and broader clinical applications. However, as with other cuffless technologies, recalibration is necessary after significant changes in vasoactive medication regimens or abrupt alterations in patient positioning. This requirement represents a common challenge in the ongoing development of CNIBP monitoring.
Rigorous statistical methods, implemented in accordance with ISO 81060-3:2022 (such as the calibrated test standard deviation s corr , intraclass correlation coefficient Icc, and the number of independent measurements Nind), enhance the evaluation of device performance. These methods account for data independence, the effects of repeated measurements, and inter- and intra-individual variability. The use of more complex statistical models provides a more comprehensive assessment of errors. This approach ensures that the samples have sufficient statistical power and more accurately reflect the device performance under varying conditions. Consequently, these methodological and statistical advancements offer stronger evidence supporting the clinical use of CNIBP monitoring devices, including the device examined in this study.
This study demonstrated significant improvements in clinical performance assessment by employing a rigorous clinical trial design, thereby providing more reliable evidence for clinical evaluation and application. The validation of the device ability to accurately track dynamic BP changes in real-world ICU settings underscores its potential role to facilitate timely therapeutic interventions, particularly during vasopressor titration and early detection of hemodynamic instability. The device addresses the critical gap between traditional intermittent cuff measurements and IBP monitoring, overcoming the longstanding clinical challenge of reconciling continuous monitoring with non-invasive techniques. The results indicate that this device may be particularly beneficial in several key clinical scenarios. In this study, IBP calibration was used to ensure methodological rigor, whereas NIBP calibration is sufficient for practical clinical application. The device serves as a valuable alternative for patients with contraindications to arterial catheterization, such as peripheral vascular disease or coagulation disorders, in whom invasive monitoring poses a substantial risk. Additionally, it also provides an effective bridge for patients moving from intensive IBP monitoring to general ward care, offering continuous surveillance at a higher resolution than intermittent cuff measurements, without the associated risks of invasive monitoring. Furthermore, its extended hemodynamic profiling capability makes it ideal for cases requiring prolonged BP trend analysis, without the infection risks associated with long-term arterial lines, thereby expanding the options for continuous hemodynamic surveillance across various clinical settings.
Despite the progress achieved, several limitations remain in this study. Firstly, calibration dependency: the CNIBP device requires recalibration following adjustments with vasoactive drugs or changes in the patient’s posture. 26 This dependency limits its application in highly dynamic clinical settings, such as rapid titration of vasoactive medications, intra-aortic balloon pump (IABP) support, or arrhythmia management, where continuous monitoring is essential. Secondly, sample size considerations: although the sample size was adequate to validate the primary endpoints, such as accuracy, stability, and dynamic BP tracking, according to ISO standards, it was insufficient for predefined subgroup analyses (e.g., age ≥ 70 years, comorbidity classification, or varying doses of vasoactive drugs). Future large-scale multi-cohort studies are needed to thoroughly evaluate performance heterogeneity across different patient populations. Thirdly, the study was limited to ICU patients, and a short observation period: a 24 h monitoring period, combined with the exclusive focus on ICU patients, may limit the applicability of the findings to non-ICU settings, such as outpatient, perioperative, or step-down care, where continuous BP monitoring is also essential. Fourthly, there was no evaluation of long-term monitoring beyond 24 h: although the 24 h monitoring period meets the ISO 81060-3:2022 requirement for initial stability assessment, it does not capture potential signal drift or performance decline over extended periods. Future studies should include long-term longitudinal assessments (e.g., extending from 24 h to 7 days) to determine the device durability and calibration requirements in long-term monitoring scenarios. While CNIBP may ultimately complement oscillometric devices in selected clinical contexts, IBP monitoring remains essential for comprehensive hemodynamic assessment in critically ill patients, particularly when frequent blood sampling for metabolic parameters (such as pH and lactate) is required.
Conclusions
In conclusion, this trial demonstrated that the PWTT-based CNIBP device is a viable, ISO-compliant alternative for continuous BP monitoring in ICU settings. This approach bridges the critical gap between intermittent cuff-based methods and invasive techniques. Future research should focus on longitudinal, multi-center validation and explore hybrid monitoring systems that combine the non-invasive benefits of CNIBP with the selective use of IBP in high-acuity cases.
Supplemental material
Supplemental material - Clinical performance evaluation of a cuffless continuous non-invasive blood pressure monitoring device in ICU patients
Supplemental material for Clinical performance evaluation of a cuffless continuous non-invasive blood pressure monitoring device in ICU patients by Yuting Chen, Zhikun Xu, Yonghui Ma, Huaisheng Chen, Hongbo Xu, Yuan Ye, Fang Xue, Haigang Zhang, Shengyuan Su and Xueyan Liu in Digital Health.
Supplemental material
Supplemental material - Clinical performance evaluation of a cuffless continuous non-invasive blood pressure monitoring device in ICU patients
Supplemental material for Clinical performance evaluation of a cuffless continuous non-invasive blood pressure monitoring device in ICU patients by Yuting Chen, Zhikun Xu, Yonghui Ma, Huaisheng Chen, Hongbo Xu, Yuan Ye, Fang Xue, Haigang Zhang, Shengyuan Su and Xueyan Liu in Digital Health.
Footnotes
Acknowledgments
The clinical trial-related device was sponsored by Shenzhen Mindray Bio-Medical Electronics Co., Ltd.Com.
Ethical considerations
This study was conducted with the understanding and the consent of each participant. The study protocol complied with the Declaration of Helsinki and was approved by the local ethics committee (approval number: Shenzhen People’s Hospital, SYL-2023-083-01). Shenzhen Bao’an District People’s Hospital, QX-2023-4. Huazhong University of Science and Technology Union Shenzhen Hospital, I-2023-09-01), registered (ChiCTR2300079037), and monitored externally.
Consent to participate
Informed consent was obtained from all subjects or their legal guardians. All patients provided written informed consent.
Author Contributions
Conception and design: Yuting Chen and Xueyan Liu. Collection and assembly of data: Zhikun Xu, Yonghui Ma, Hongbo Xu, Yuan Ye, Fang Xue, and Shengyuan Su. Data analysis and interpretation: Huaisheng Chen, Shengyuan Su and Haigang Zhang. Manuscript writing: Yuting Chen and Xueyan Liu. Final approval of the manuscript: All authors. Accountability for all aspects of the work: All authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Shenzhen Key Laboratory of Prevention and Treatment of Severe Infections (ZDSYS20200811142804014) and Major Science and Technology Projects of the Shenzhen Science and Technology Innovation Commission (KCXFZ20230731093559005).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request. Supplementary materials may also be shared to support transparency and reproducibility, subject to institutional review board approval and compliance with patient consent agreements. All shared data will be de-identified to protect participant privacy.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.