
Abstract
Objectives
A self-care smartphone application, JoyHer Pro, was developed to support midlife women experiencing menopausal symptoms by providing daily symptom tracking, personalized healthcare plan recommendations, and educational content. A proof-of-concept study was conducted to explore its feasibility and preliminary impact.
Methods
This single-arm pre–post study simulated a health checkup–based model of digital intervention. Ninety-one Japanese women aged 45–55 years with moderate menopausal symptoms used JoyHer Pro for six months. The primary outcome was the change in total scores on the scaled Questionnaire for the Assessment of Climacteric Symptoms in Japanese Women (sQACS) from baseline to six months.
Results
The six-month follow-up rate was 96%. Participants recorded symptoms on a median of 165 days (90% of the study period) and logged self-care activities on 59% of days. They accessed a median of 42 educational topics (72% of available content). The total sQACS score significantly decreased from baseline to three and six months (both p < 0.001). Participants also reported improvements in their perception and attitude toward menopause, as well as greater self-assessed knowledge and coping ability. Some participants newly sought or planned medical consultation following app use.
Conclusion
This proof-of-concept study suggests that JoyHer Pro is a feasible digital self-care support tool for midlife women with menopausal symptoms and may provide a basis for future research on integrating digital interventions into preventive care and public health strategies.
Introduction
During the climacteric period, women often experience various physical and psychological symptoms, including hot flashes, depression, sleep disturbances, cognitive changes, joint and muscle pain, and headaches. These manifestations are collectively referred to as menopausal symptoms. While they are primarily attributed to the decline in ovarian function, variations in their presentation and severity are influenced by genetic, environmental, cultural, lifestyle, and anthropometric factors.1–3 These symptoms can considerably affect quality of life and work productivity. 4 The management strategies for menopausal symptoms include hormone replacement therapy (HRT), pharmacological treatments such as selective serotonin reuptake inhibitors, and psychotherapeutic interventions such as cognitive behavioral therapy.5,6 Although evidence remains limited, self-care practices and lifestyle modifications before and during the climacteric period may help prevent or alleviate symptoms. 7 Providing accurate, personalized guidance based on individual symptoms, lifestyle, and preferences may contribute to more effective symptom management.
From a public health perspective, several challenges exist in the effective management of menopausal health in Japan. Current general health checkups are not designed to assess or address menopausal symptoms. Moreover, accessibility to gynecological care varies considerably across regions, partly due to the geographical maldistribution of obstetricians and gynecologists. 8 Many women with symptoms hesitate to seek medical consultation, 9 resulting in missed opportunities for early guidance and intervention. In addition, limited consultation time in outpatient clinics may hinder sufficient discussion of self-care strategies and long-term lifestyle support, thereby limiting the comprehensive implementation of individualized care.
In this context, technological advancements and the increasing adoption of digital health solutions have the potential to transform healthcare delivery, improving accessibility and clinical efficiency, ultimately promoting health equity.10,11 In recent years, several studies have reported mobile applications designed for the management of menopausal symptoms.12–16 These apps offer a variety of functionalities, including symptom tracking, educational content, self-care training, exercise coaching, psychological interventions, specialist referrals, support for collaboration with healthcare professionals, and user community forums, with some of these functionalities being personalized. Current findings suggest the potential of these applications to alleviate symptoms and enhance women’s self-management and quality of life; however, the evidence remains limited, and further research is required to optimize these solutions.
To address these challenges, we developed JoyHer Pro, a smartphone-based self-care support application for women with menopausal symptoms. The application enables users to track their symptoms and self-care activities, receive personalized healthcare recommendations, and access educational content. This proof-of-concept study simulated a health checkup–based model of menopausal care, in which midlife women attending a routine health examination were offered digital self-care support. The study aimed to explore the preliminary impact of this approach and assess the feasibility of the JoyHer Pro application as a digital self-care tool.
Methods
Study design
This proof-of-concept study simulated a setting in which midlife women attending a health checkup were offered a digital self-care support program designed to enhance awareness of menopausal health and promote ongoing symptom self-management. The study adopted a single-arm pre–post comparison design and was conducted between October 2023 and April 2024. The study protocol was approved by the Ethics Committee of the Kyoto University Graduate School and Faculty of Medicine (C1634). The study was conducted in accordance with the Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects and the Ethical Guidelines for Medical and Biological Research Involving Human Subjects in Japan. The trial was registered in the University Hospital Medical Information Network Clinical Trials Registry (UMIN-CTR; UMIN-ID: UMIN000052302). All participants provided written informed consent before enrollment.
Participants
Recruitment was conducted by the Non-Profit Organization “Health Promotion Zeroji-Club” in Nagahama City, Shiga Prefecture. Participants were recruited through poster displays, leaflet distribution, invitations extended to Zeroji Club members and their acquaintances, and social media outreach. Participant registration for the trial was conducted between September 22 and October 15, 2023. Participants were required to be employed at the time of enrollment because the study was conducted within a research project focusing on health support for working women.
Eligible participants were Japanese women who (1) aged 45–55 years; (2) had irregular or absent menstruation; (3) had moderate menopausal symptoms, defined as a Simplified Menopausal Index (SMI) score ≥26 and <66 (see
Eligible participants underwent blood tests and body composition analyses. Hematological, metabolic, and biochemical parameters were measured, including complete blood count (CBC), liver and renal function tests, lipid profile, electrolytes, iron-related indices (serum iron, ferritin, and total iron-binding capacity), and 25-hydroxyvitamin D, and follicle-stimulating hormone levels. The detailed list of laboratory parameters is provided in Supplemental Table S1. Body composition analysis was performed using an InBody S10 device (InBody Japan, Japan).
Interventions
This study implemented a digital self-care intervention using the JoyHer Pro smartphone application, developed by YStory Inc., a digital health company specializing in women’s healthcare applications, in collaboration with clinicians specializing in menopausal medicine. The application was designed to help midlife women manage menopausal symptoms by enabling daily tracking of symptoms, self-care behaviors, and potential triggers, providing personalized healthcare plans, and offering educational content on self-care and lifestyle modification (Figure 1). JoyHer Pro was available exclusively for iOS devices and solely for use in this study.
At study initiation, participants downloaded the application and self-reported their physical and psychological symptoms, as well as their preferred self-care methods. Based on these baseline data, an initial predefined healthcare plan was automatically selected and displayed within the application through a built-in algorithm. Participants then recorded their daily symptoms, self-care activities, stressors, and potential symptom triggers. After the first month, healthcare plans were updated monthly by the researchers, who accessed an online dashboard integrating biometric and user-entered data. Using a curated library of self-care tips based on current clinical knowledge and expert consensus, the researchers generated personalized healthcare plans tailored to each participant’s symptom patterns and progress. In addition, educational content encompassing 58 topics related to menopausal health was provided, including symptom management, lifestyle modification (nutrition, exercise, and sleep), and common postmenopausal conditions such as hypertension, dyslipidemia, diabetes, frailty, and osteoporosis. Each topic was prioritized and presented according to individual symptom patterns and symptom severity using an algorithm that ranked topic relevance. The healthcare plan list and educational content were developed and reviewed by clinicians and women’s health experts to ensure clinical relevance and validity. Participant data entered through the application were stored on secure servers managed by YStory Inc. Access to the data was restricted to authorized members of the research team. Personally identifiable information was removed prior to analysis, and only anonymized data were used for statistical analyses.
Blood test results were communicated to participants after the study was completed. For laboratory abnormalities considered to require early medical attention, participants were notified by email approximately one month after study initiation. The thresholds for notification were hemoglobin <10.0 g/dL and platelet count <100 × 109/L to screen for potential hematologic disorders. For other parameters, cutoff values were based on those used in the Japanese national health screening program for lifestyle-related disease prevention, which specifies thresholds prompting either health guidance or medical referral. 18
Outcomes
Outcomes included symptom severity, health-related quality of life, work productivity, perceptions and attitudes toward menopause, self-assessed knowledge and coping ability, and behavior changes related to application use. Unless otherwise specified, outcomes were assessed at baseline, 3 months, and 6 months. Outcome measures assessed at different time points are described below. The primary outcome was the change in menopausal symptom severity between baseline and 6 months, measured using the total score of the scaled version of the Questionnaire for the Assessment of Climacteric Symptoms in Japanese Women (sQACS). All other outcomes and comparisons were treated as secondary and exploratory analyses.
Symptoms severity
Menopausal symptoms were assessed using the scaled version of the Questionnaire for the Assessment of Climacteric Symptoms in Japanese Women (sQACS) and the Simplified Menopausal Index (SMI).
The sQACS is a modified numerical rating scale derived from the original QACS. The original QACS, developed in 2001 by the Japan Society of Obstetrics and Gynecology, assesses 21 symptoms commonly observed among Japanese women during the climacteric period. 19 In the original version, each symptom is rated on a three-point scale (severe, weak, or none). Although the original version does not include a quantitative severity score, it has been widely used in clinical practice owing to its simplicity and its relevance to the symptom patterns typically observed in Japanese women. The sQACS used in this study consists of the same 21 items, each rated on a 6-point scale (0 = none, 1 = very slight, 2 = mild, 3 = moderate, 4 = severe, and 5 = very severe), yielding a total score of 0–105.
The SMI, developed by Koyama et al. in 1992, is a Japanese index comprising 10 symptoms commonly observed in middle-aged women. 17 The scoring system assigns greater weights to symptoms considered to be estrogen-related, with a total score ranging from 0 to 100. Scores are categorized as follows: 0–25 (no abnormality), 26–50 (monitoring of diet and exercise), 51–65 (recommended outpatient clinic visit), 66–80 (long-term treatment planning), and 81–100 (specialist consultation and extended care). Although the formal validity of the SMI has not been established, it remains widely used in clinical practice in Japan due to its simplicity and ease of interpretation. The SMI was assessed at screening (baseline) and then monthly for up to 6 months.
Depression, anxiety, and gastrointestinal symptoms were evaluated using the Patient Health Questionnaire-9 (PHQ-9),20,21 Generalized Anxiety Disorder-7 (GAD-7),22,23 and the Gastrointestinal Symptom Rating Scale (GSRS),24–26 respectively. Other symptoms (e.g., skin irritation, leg cramps, eyelid twitching, muscle pain, and weather-related discomfort) were rated on a 6-point scale (0 = none to 5 = very severe).
Health-related quality of life and work productivity
Health-related quality of life (HRQOL) was evaluated using the Medical Outcomes Study 36-Item Short Form Health Survey (SF-36).27,28 The scores for the three-component summaries (physical, mental, and role-social components) and eight subscales (physical functioning, role physical, bodily pain, social functioning, general health, vitality, role emotional, and mental health) were calculated.
Work productivity (absenteeism/presenteeism) was assessed using the World Health Organization Health and Work Performance Questionnaire Short Form (WHO-HPQ).29,30 The questionnaire provides estimates of absolute and relative absenteeism over the previous four weeks and measures both absolute and relative presenteeism. Absolute absenteeism reflects the number of work hours missed due to health problems during the previous four weeks, whereas relative absenteeism represents the proportion of expected work time missed. Absolute presenteeism represents self-rated job performance on a scale from 0 to 100, with higher scores indicating better work performance. Relative presenteeism reflects the ratio of an individual’s performance compared with that of a typical worker in a similar job.
Perception and attitude toward menopause and self-assessment of knowledge and coping ability
Perception and attitude toward menopause were evaluated before and after the intervention using the question: “Please choose the option that best represents your current perception or attitude toward menopause.” Responses were rated on a 7-point scale (1 = negative, 7 = positive). Self-assessed knowledge of menopause and perceived ability to manage physical and mental discomfort were evaluated before and after the intervention using the questions: “Do you think you have appropriate knowledge about menopause?” and “Do you think you can manage physical and mental discomfort well?” Responses were recorded on a 5-point scale (not at all, not really, neutral, agree, strongly agree).
Behavior changes related to application usage
Behavioral changes attributable to application use were assessed at 6 months using questions about medical consultations and non-medical therapies. Participants were asked, “Did you visit a medical provider for physical or mental discomfort as a result of using this application?” Response options were “Yes,” “Had been seeing a doctor before using this application,” and “No.” Participants who responded “No” were further asked: “Do you plan to visit a medical provider in the future?” Response options were: not at all, not much, neutral, I think so, and I strongly think so. A parallel set of questions was used to evaluate the use of non-medical therapies. Participants were asked: “Did you seek non-medical therapy for physical or mental discomfort as a result of using this application?” Response options were “Yes,” “Had received non-medical therapy before using the application,” and “No.” Those who responded “No” were further asked whether they planned to seek non-medical therapy in the future using the same five-point response scale.
Stages of behavioral change regarding lifestyle habits were assessed using the question: “Do you plan to improve lifestyle habits, such as exercise and diet?” Response options were: no intention to improve; intend to improve (within approximately 6 months); intend to improve (within approximately 1 month); intend to improve and have started gradually; and already working on improvement (less than 6 months).
Statistical analysis
Descriptive statistics were used to summarize participant characteristics. Continuous variables were expressed as mean (standard deviation [SD]) or median (interquartile range [IQR]), as appropriate, and categorical variables were expressed as frequencies and percentages. Data distributions were examined prior to analysis, and non-parametric methods were used because several outcome variables were not normally distributed. The primary outcome, prespecified in the Outcomes section, was the change in the total sQACS score between baseline and 6 months, as improvements in symptom perception and self-management behaviors were expected to occur gradually over several months of application use. Therefore, the primary analysis focused on this paired comparison using the Wilcoxon signed-rank test, a non-parametric test for paired data. The sample size was estimated using a paired t-test as an approximation for the Wilcoxon signed-rank test. Because evidence regarding the effect size of self-care smartphone applications for menopausal symptoms was limited at the time of study planning, the expected standardized effect size for the pre–post change in the primary outcome was conservatively set at 0.3. Assuming a two-sided significance level of 0.05 and a power of 0.80, the required sample size was estimated to be approximately 90 participants. Considering potential dropout and missing data, the target sample size was set at 120 participants. Intermediate measurements, including the 3-month sQACS and monthly SMI scores, were included to explore temporal trends descriptively rather than to formally evaluate global differences across repeated measurements. Secondary outcomes were also compared between baseline and follow-up time points using Wilcoxon signed-rank tests, as appropriate. For subgroup analyses, participants were stratified by baseline SMI scores (26–50 vs. 51–65) and menstrual status (irregular menstruation vs. amenorrhea), and changes in total sQACS scores within each subgroup were examined exploratorily. No adjustments were made for multiple comparisons because this was an exploratory proof-of-concept study intended to identify potentially relevant signals and generate hypotheses for future confirmatory studies. Applying strict multiplicity adjustments in this context could increase the risk of type II error and obscure potentially meaningful exploratory findings. Therefore, secondary and subgroup analyses were interpreted as exploratory and hypothesis-generating. A two-sided p value <0.05 was considered statistically significant. All analyses were performed using R statistical software version 4.2.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Participant characteristics
Between September and October 2023, 204 individuals were screened for eligibility, and 92 were enrolled in the study (Figure 2). One participant was excluded owing to technical issues, resulting in 91 participants receiving the intervention. Baseline characteristics are summarized in Table 1. The median (IQR) age of the participants was 52 (50–54) years, and the median (IQR) BMI was 21.1 (19.6–23.4) kg/m2. Menstrual cycles were irregular in 52 participants (57.1%), whereas 39 (42.9%) had experienced amenorrhea for more than one year. Only one participant (1.1%) was receiving hormone replacement therapy. Regarding blood test results, the median (IQR) serum 25-hydroxyvitamin D level was 17.9 (14.8–21.8) ng/mL, indicating a low range, whereas the median values of other laboratory parameters were within normal limits (Table S1). Representative screens of the JoyHer Pro application Baseline characteristics. Abbreviation: IQR, interquartile range.

The 6-month follow-up rate was 96% (87/91). During the 184-day study period, symptoms were recorded for a median (IQR) of 165 (97.5–183) days, representing 90% (53.0%–99.0%) of the study duration. Self-care activities were logged for a median (IQR) of 108 (45.5–165) days, corresponding to 59% (24.0%–90.0%) of the period. Participants were assessed a median (IQR) of 42 (17–58) educational topics, accounting for 72.4% (29.3%–100%) of all available topics. Notifications recommending early medical consultation based on blood test results were sent to 23 participants. The details were as follows: hemoglobin ≤10.0 g/dL (n = 2), platelet count <100 × 109/L (n = 1), hemoglobin A1c ≥6.5% (n = 2), aspartate aminotransferase ≥51 U/L (n = 2), alanine aminotransferase ≥51 U/L (n = 2), gamma-glutamyl transpeptidase ≥101 U/L (n = 2), low-density lipoprotein cholesterol ≥140 mg/dL (n = 15), and triglyceride ≥300 mg/dL (n = 2).
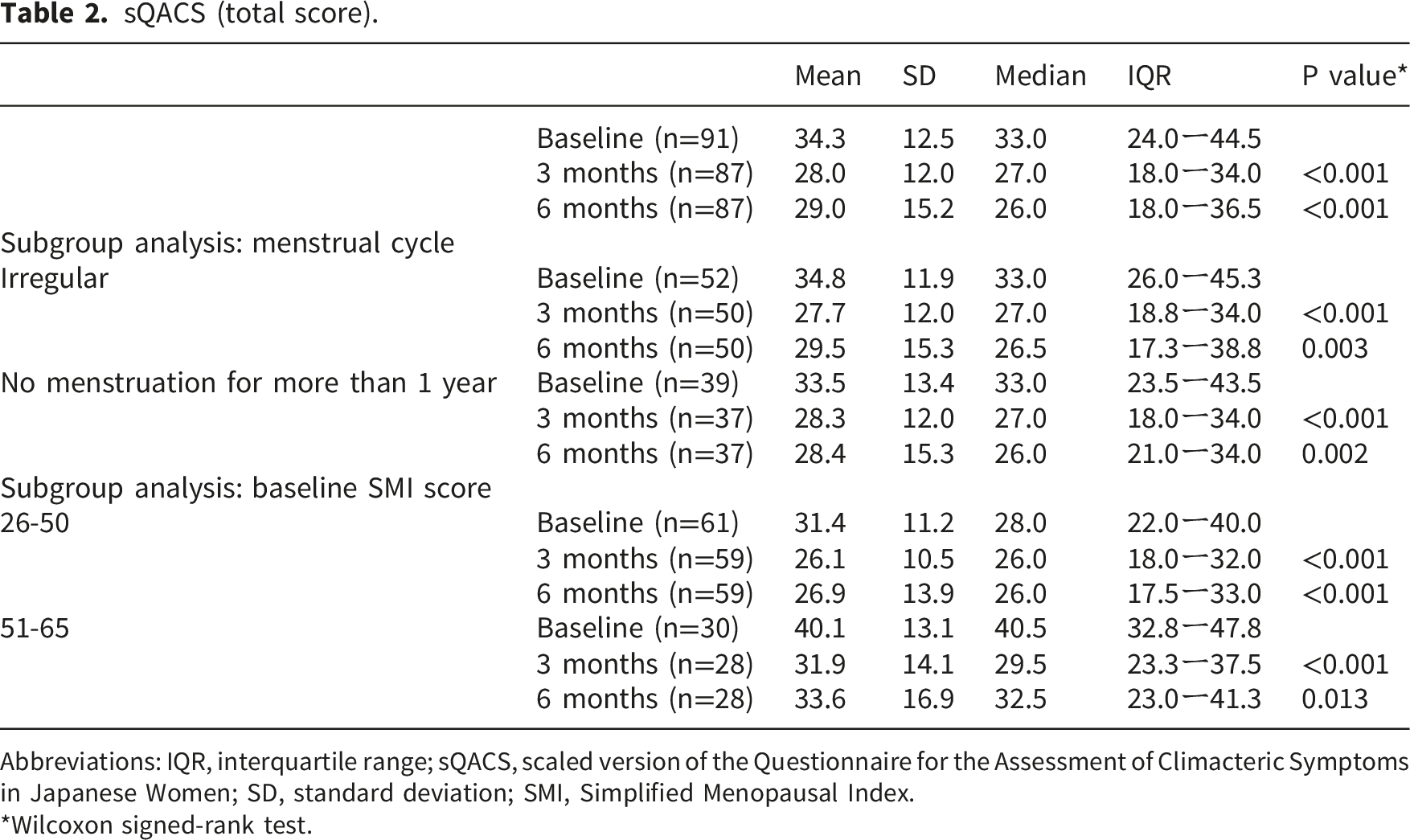
Symptoms severity
Overall, menopausal symptom severity improved during the intervention period. The total sQACS score showed a significant reduction, with a median (IQR) of 33.0 (24.0–44.5) at baseline, decreasing to 27.0 (18.0–34.0) at 3 months and 26.0 (18.0–36.5) at 6 months (both p < 0.001; effect size r = 0.45 at 6 months) (Figure 3, Table 2). Improvements were observed across several symptoms (Tables S2 and S3). Subgroup analyses confirmed consistent improvements regardless of menstrual status or baseline symptom severity (Table 2). The SMI total score decreased from 45.0 (38.5–53.0) at baseline to 32.0 (21.8–41.3) at 1 month and remained stable thereafter (Table 3). By 6 months, 35.6% of the participants had an SMI score of 0–25, indicating symptom resolution. Flowchart of the participant selection process. sQACS (total score). Abbreviations: IQR, interquartile range; sQACS, scaled version of the Questionnaire for the Assessment of Climacteric Symptoms in Japanese Women; SD, standard deviation; SMI, Simplified Menopausal Index. *Wilcoxon signed-rank test. SMI. Abbreviations: IQR, interquartile range; SD, standard deviation; SMI, Simplified Menopausal Index. *Wilcoxon signed-rank test.

No significant changes were observed in PHQ-9, GAD-7, or GSRS scores at 3 and 6 months (Table S3).
HRQOL and work productivity
Baseline SF-36 scores suggested that participants generally reported relatively favorable HRQOL at study entry. At 3 months, the SF-36 physical component summary score improved from 47.6 (43.1–52.0) at baseline to 50.1 (45.1–54.4), whereas the role-social component summary score declined from 54.4 (48.7–58.2) at baseline to 51.0 (46.3–56.5). By 6 months, neither component showed significant differences from baseline (Table S4).
At baseline, absolute and relative absenteeism were near zero, absolute presenteeism (self-rated job performance on a 0–100 scale) was approximately 70, and relative presenteeism was close to 1 (Table S5). No significant changes were observed in absenteeism or relative presenteeism. Absolute presenteeism showed a modest increase at 3 months (median 68.0 to 73.0, p=0.014), indicating a temporary improvement in self-rated work performance, but this difference was not maintained at 6 months. Total sQACS score at baseline, 3 months, and 6 months
Perception and attitude toward menopause and self-assessment of knowledge and coping ability
Perception and attitude toward menopause and self-assessment of knowledge and coping ability.

Abbreviations: IQR, interquartile range; SD, standard deviation.
*Wilcoxon signed-rank test.
Behavior changes related to application usage
Behavior changes related to application usage.

*Wilcoxon signed-rank test
Discussion
This proof-of-concept study evaluated a health checkup–based model of menopausal care in which midlife women were offered digital self-care support through a smartphone application. The study demonstrated good participant retention and consistent application use over the 6-month period, indicating acceptable feasibility under study conditions. Slight reductions were observed in total sQACS and several subscale scores at 3 and 6 months, as well as in SMI scores within the first month. The 3-month sQACS and monthly SMI assessments were treated as exploratory analyses describing temporal trends in symptoms. Although these changes were modest, the consistent downward trend across multiple domains of symptom reporting may reflect changes in perceived symptom severity. Nonetheless, given the single-arm design, these findings do not provide evidence of causal effectiveness and should be interpreted with caution due to the exploratory nature of the study and the potential influence of placebo effects and natural symptom fluctuations.
Participants reported significant gains in their perception and attitude toward menopause, health knowledge, and self-assessed coping ability. This finding aligns with previous research indicating that health literacy and behavioral reflection can positively influence perceptions and attitudes toward menopause and contribute to symptom relief.31,32 As menopausal symptoms are shaped by both hormonal and psychological factors, the application may provide a complementary approach, particularly in cases where HRT alone may be insufficient.
Within the context of a health checkup–based model, some participants actively sought medical consultations or considered alternative therapies after using the application, suggesting its potential influence on health-seeking behavior. Although HRQOL and work productivity outcomes showed minimal changes, this may be attributable to the participants’ relatively favorable baseline HRQOL and productivity levels. Future studies should consider prioritizing labor productivity and HRQOL as primary endpoints to better assess the broader impact of the application. Although no clear trend was observed in stages of behavioral change, the observed shifts in help-seeking behavior suggest that digital self-care tools may facilitate earlier engagement with medical or supportive services among midlife women. Although the application included guidance on lifestyle habits such as exercise and diet, stage-based measures may be relatively insensitive to small behavioral adjustments that do not result in transitions between stages. In addition, the application may have influenced other forms of health-related behavior, including symptom awareness and help-seeking. Baseline levels of depression, anxiety, and gastrointestinal symptoms also appeared relatively modest in this population, which may have limited the potential for measurable improvement in these outcomes.
JoyHer Pro integrates symptom and trigger tracking, personalized healthcare plans, and symptom-linked educational content, providing a comprehensive framework for symptom management. Beyond symptom control, it supports long-term health literacy related to postmenopausal risks such as cardiovascular disease and osteoporosis. Given the climacteric period’s importance in the onset of these conditions, JoyHer Pro may serve as a preventive tool that fosters self-management and informed decision-making. A notable feature is its real-time data-sharing capability with healthcare professionals, which may enhance clinical efficiency and facilitate telemedicine integration. This study also simulated a checkup-based model of digital health intervention, suggesting that general health checkups may function as an entry point for midlife women’s health support. Although routine checkups in Japan are not yet tailored for menopausal care, this model demonstrates the feasibility of integrating digital self-care support into public health systems to promote early symptom recognition and preventive behavior.
This study has some limitations. First, the outcome measures relied on self-reported data, as the objective assessment of menopausal symptoms remains challenging. Additionally, the absence of a validated Japanese scale for the comprehensive evaluation of menopausal symptoms represents a methodological limitation that hinders the advancement of menopausal research in Japan. In this study, we therefore used a scaled version of the QACS, developed by referencing previous research. 33 This underscores the need to establish a reliable Japanese scale capable of comprehensively evaluating menopausal symptoms. Second, this study primarily included women with moderate symptoms, excluding those with severe symptoms who may require standard treatments such as HRT. For patients with mild symptoms, this application may serve as a preventive health tool. The recruitment method may also have attracted participants with higher health awareness, indicating the need for future research involving a more diverse population. Therefore, the findings may not be fully generalizable to all midlife women, particularly those with lower health awareness or limited access to digital health technologies. Finally, as an exploratory single-arm pre-post study, the potential influence of placebo effects, biases, and regression to the mean cannot be ruled out. In addition, analyses of secondary outcomes and subgroup analyses should be interpreted as hypothesis-generating. Although the target sample size of 120 participants was not reached during the recruitment period, participant retention was high and the final analyzed sample size for the primary analysis was close to the estimated required sample size. Nevertheless, the statistical power for some secondary and subgroup analyses may have been limited. Future studies should employ rigorous methodologies, including randomized controlled trials, to validate the application’s effectiveness.
Conclusion
This proof-of-concept study provides preliminary support for the feasibility of the JoyHer Pro application as a digital self-care support tool for midlife women with menopausal symptoms. The simulated checkup-based model explored in this study presents a promising framework for integrating digital interventions into preventive care and public health for midlife women. Further research should refine the application and evaluate its efficacy through larger, randomized controlled trials.
Supplemental material
Supplemental material - A self-care smartphone application for midlife women with menopausal symptoms: A proof-of-concept study
Supplemental material for A self-care smartphone application for midlife women with menopausal symptoms: A proof-of-concept study by Takuma Ohsuga, Miho Egawa, Kaori Tsuyuki, Miki Ohtsuki, Yu Wanjie, Shi Juan, Rena Hinotani, Yoshimitsu Takahashi, Takeo Nakayama, Masaki Mandai in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to thank Ms. Kiwa Kojima and Ms. Teruko Tahara for their generous assistance with laboratory procedures.
Ethical considerations
Ethical approval for this study was obtained from the Ethics Committee of the Kyoto University Graduate School and Faculty of Medicine (C1634).
Consent to participate
All participants provided written informed consent to participate in this study.
Author contributions
Conceptualization: TO, ME, KT, YW, SJ, YT, TN and MM.
Data curation: TO, KY, MO, YW, and SJ.
Formal analysis: TO.
Funding acquisition: TO, ME, KT, YW, and SJ.
Investigation: TO, ME, KT, YW, SJ, and RH, Methodology: TO, ME, KT, YT, and TN.
Project administration: ME.
Resources: YW, and SJ, Software: TO, ME, KT, YW, and SJ.
Supervision: ME.
Validation: TO, ME, KT, YW, and SJ.
Visualization: TO.
Writing – original draft: TO
Writing – review & editing: All authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Ministry of Education, Culture, Sports, Science and Technology Grant-in-Aid for Scientific Research (no. 23H03885); the Ministry of Economy, Trade and Industry Subsidy for Demonstration Projects for Femtech and Similar Support Services; and joint research funding from YStory Inc.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The Ministry of Education, Culture, Sports, Science and Technology and the Ministry of Economy, Trade and Industry had no involvement in the study administration, data analysis, or manuscript preparation. YStory Inc. was a collaborative research partner that provided funding for this study and contributed to research management but was not involved in data analysis or interpretation. The application used in this study was developed under a collaborative research agreement with YStory Inc. YT is employed through a joint research fund between Kyoto University and HealthTech Laboratory Inc. HealthTech Laboratory Inc. is not affiliated with YStory Inc. and had no role in the design of the study, data collection, analysis, interpretation of the results, or manuscript preparation.
Data Availability Statement
The datasets analyzed in the current study are available from the corresponding author upon reasonable request.
Clinical trial registration
The trial was registered in the University Hospital Medical Information Network Clinical Trials Registry (UMIN000052302).
Guarantor
Dr. Takuma Ohsuga is the guarantor of this work.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.