
Abstract
Objective
We aimed to perform what is, to our knowledge, the first bibliometric analysis focusing on artificial intelligence (AI) applications in paediatric congenital heart disease (CHD) over a 25-year period (2000-2025). We examined the advancements in research, emerging trends, and principal research topics in this field.
Materials and Methods
Articles on AI and CHD published between 2000 and 2025 were retrieved. The data sourced from the Web of Science Core Collection encompassed 423 qualifying studies that were evaluated using Cite Space and VOSviewer to examine the contributions of various countries, institutions, authors, journals, and keywords. These visualisation tools facilitated the mapping of collaboration networks, co-citation patterns, and keyword trends.
Results
The United States is the main research hotspot in national terms, contributing 40% of the publications in this area, Harvard Medical School is the institution with the most research results, with Pan, Silin being the most prolific researcher. Key research areas include the application of AI in prenatal screening for CHD, diagnosis and treatment of paediatric CHD, long-term management of CHD in children, the role of health professionals, and related risks.
Conclusion
As far as we know, this is the first bibliometric analysis dedicated to AI in paediatric CHD. It shows continuous growth and interdisciplinary potential. We emphasise the need for improved collaboration between different fields of study, use of AI in medical practice to assess individual risks (especially regarding medication safety), and policy initiatives to address the equity gap between high-income regions and those with the most CHD cases.
Keywords
1. Introduction
Congenital heart disease (CHD) is a significant contributor to childhood illnesses and death. According to statistics, the global prevalence of CHD in children aged <5 years was estimated to be >4.18 million in 2021, an increase of 3.4% since 1990. Compared to 1990, CHD-related mortality and disability-adjusted life years have decreased by 56.2% and 55.7%, respectively, owing to increased treatment availability and advancements in treatment. 1 The global burden of this disease poses distinct challenges to healthcare systems.2,3 The cost of consultations for CHD adds to the economic burden on families and the society as a whole. Therefore, CHD imposes a dual burden. First, there is a direct clinical burden on the affected children and their families. Second, there is an indirect burden on healthcare systems that are already strained by limited resources, particularly in low- and middle-income countries (LMICs), where many children with CHD lack access to adequate care.
Several medical disciplines have incorporated artificial intelligence (AI), which indicates the age of AI. In paediatric heart disease, AI can help doctors make more accurate diagnoses, understand images more easily, and personalise risks for each patient. However, significant problems prevent its use in practice. These include the fact that the system cannot be used everywhere, there is not enough data, it is difficult to obtain official approval, and there is a risk that it will make things worse for people who lack resources, especially in places where more people have CHD.
Researchers have gradually applied AI to paediatric CHD for >20 years, resulting in a substantial body of related literature. A few previous studies have assessed the use of AI in certain areas of cardiology; for example, a systematic review specifically focusing on AI in paediatric CHD was recently conducted by Venna et al., and 68 studies were identified in the areas of diagnosis, prognosis prediction, and training tools, 4 AI techniques for cardiovascular disease diagnosis via X-ray sensor-based coronary angiography, 5 and AI for cardiology: From diagnosis to management. 6 Methodological and numerical bibliometric investigations in this area of AI for paediatric CHD are still needed. The focus of existing bibliometric studies in the broader cardiovascular field is often on adult populations or specific techniques, such as imaging, individualised cardiovascular therapeutics via AI-powered cardiovascular imaging, 7 and the application of AI in echocardiography. 8 Although several narrative reviews have summarised the applications of AI in cardiovascular medicine, including comprehensive overviews 6 and technique-focused syntheses, 8 a systematic bibliometric analysis that identifies the key players and uncovers the evolutionary nuances and emerging frontiers of AI in paediatric CHD is needed. Such a study should also address the critical gap between academic output and implementation in low-resource settings, which was recently highlighted by Liastuti et al. 9 Based on our literature search, no prior bibliometric study has focused on AI in paediatric CHD. This study aimed to provide clinicians and researchers with a unique data-driven perspective that complements traditional narrative reviews. To this end, this study employed bibliometric methods to offer an extensive examination of this interdisciplinary field. This study aimed to address these gaps by: 1) quantifying the growth trajectory and geographic distribution of AI research in paediatric CHD from 2000 to 2025; 2) identifying the most productive countries, institutions, authors, and journals that are shaping the field; 3) analysing the intellectual structure of the field by leveraging map collaboration networks and research clusters; 4) tracking the evolution from a pathophysiological focus to innovation driven by deep learning by analysing keyword bursts and thematic shifts; and 5) evaluating the alignment between research trends and clinical implementation needs, particularly focusing on needs in low-resource settings. Our study provides clinicians, researchers, and policymakers with a data-driven foundation for advancing this field.
2. Materials and Methods
A series of key terms and related combinations are used to retrieve the information: #1 TS=(heart* OR *cardia* OR coronary OR ‘atrial septal’ OR ventricle OR pericardi* OR epicard* OR myocard*),#2 TS= (Congenital and a*no*mal* OR deformit* OR defect* OR malformatio* OR disorde* OR diseas* OR aberration),#3 TS=(‘AI’ OR ‘artificial intelligence’ OR ‘computational intelligence’ OR ‘machine intelligence’ OR ‘computer reasoning’ OR ‘computer vision system*’ OR ‘support vector machine’ OR ‘random forest’ OR ‘transfer learning’ OR ‘neural network*’ OR ‘machine learning’ OR ‘deep learning’),#4 TS=(child*),#5 #1 AND #2 AND #3 AND #4. The full search strings, including Boolean operators and field tags, are provided in Appendix S1 (Supplementary Material). A thorough review of the literature was performed using the Web of Science Core Collection (WOSCC), selecting studies published from 1 January 2000 to 5 June 2025. We retrieved articles and review articles published in English. Notably, 519 records were retrieved from the WOSCC during the initial search. After excluding 12 studies published before 2000 (1997: n=3, 1998: n=1, 1999: n=8), 507 studies published between 2000 and 2025 were screened. Only articles or review articles were included, resulting in 504 retrieved records. Seven records in languages other than English were excluded from the screening (Spanish: n = 3, French: n = 2, German: n = 1, Japanese: n = 1), leaving 497 records for full-text assessment. After full-text screening, 74 records were excluded due to their irrelevance to AI or paediatric CHD. Three reviewers (Yinmin Zhang,Yuting Lu and Xiong Qian) independently screened the titles and abstracts of the retrieved records. Studies were included if they (1) focused on CHD in children (aged 0–18 years); (2) involved the application of AI, machine learning, or deep learning techniques; and (3) were peer-reviewed original articles or reviews. The detailed inclusion and exclusion criteria are listed in Appendix S1. Disagreements were resolved through discussion or consultation with a third reviewer. Our search terms were broad. They may have found papers on other heart diseases. But each paper was checked by title and abstract. We kept only those about CHD. After removing irrelevant articles, the data were downloaded in plain text format, yielding an aggregate of 423 entries. Finally, 423 studies were included in the bibliometric analysis. The complete selection process is illustrated in the Preferred Reporting Items for Systematic reviews and Meta-Analyses-style flow diagram (Figure 1). We performed a careful bibliometric analysis of the retrieved content using VOSviewer (version 1.6.20; https://www.vosviewer.com) and Cite Space (version 6.3. R1; https://citespace.podia.com).VOSviewer was used to construct the collaboration networks. These networks included countries, institutions, and authors. The software also created keyword co-occurrence maps. We employed Cite Space to conduct co-citation analyses of references and journals, detect keyword bursts, and generate timeline visualisations of the research hotspots. To ensure that our findings can be reproduced, all key parameter settings, including thresholds, counting methods, pruning techniques, and clustering algorithms (e.g. Log-Likelihood Ratio for cluster labelling) are documented in Appendix S1 (Supplementary Material). All the primary data used in our research came from public databases; therefore, an ethical review was not required. PRISMA 2020 flow diagram for study selection process.
3. Results
3.1. Annual publication trend
Our survey showed that 423 papers contributed significantly to AI and its use in CHD in children between 2000 and 2025. Figure 2 shows that the number of published articles and citations has increased annually. By 2024, the number of publications reached 110, and with this in mind, it is clear that the figure will soon hit an all-time high. This clearly indicates that research in this area has become popular among scholars. Annual publications and citations of AI in pediatric CHD research (2000-2025).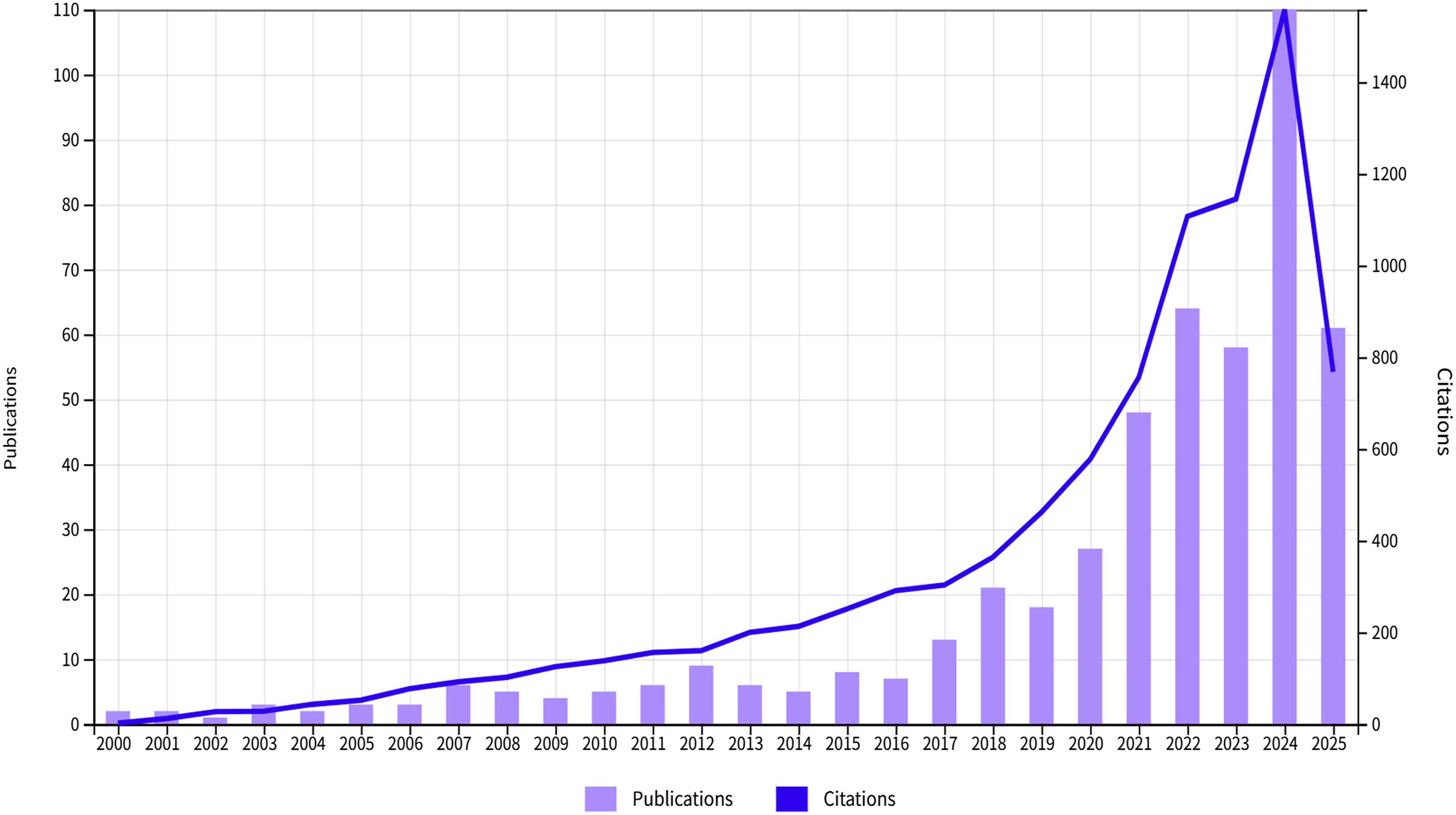
3.2. Co-authorship analysis
3.2.1. Countries
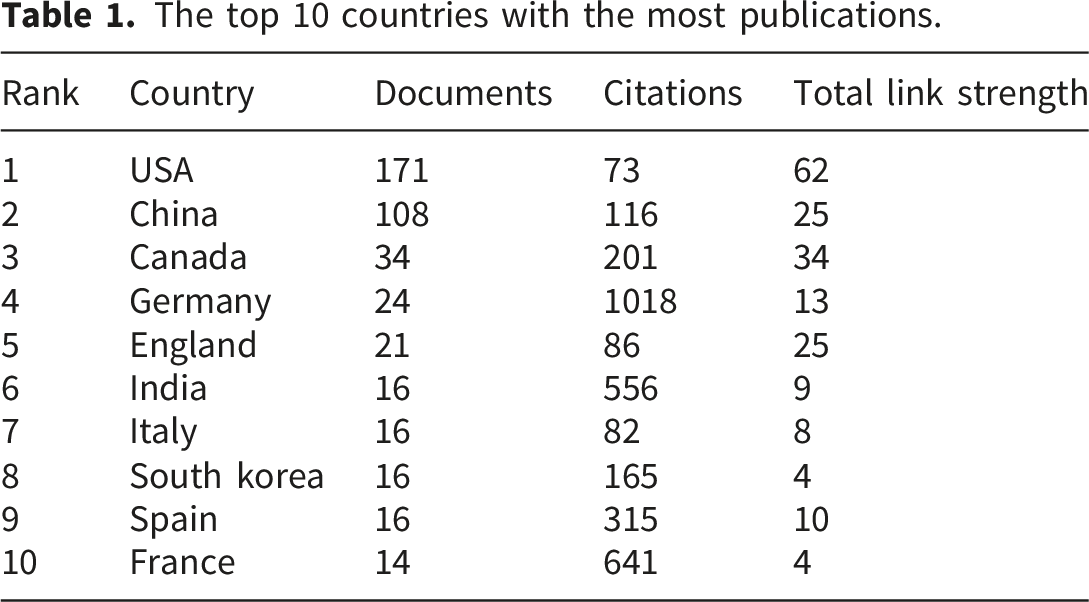
This study analysed the publication output from 71 countries and regions, with the United States (US) accounting for approximately 40% of the articles, and China contributing approximately 25.6%. Figure 3(a) shows the extensive collaboration among various countries in this field, with the highest activity levels in the US and China. Within particular clusters, the partnership between the US, China, and Canada is the closest, indicating their shared research interests and collaborative foundation in this area, as well as highlighting their significant influence and leadership in research in AI and CHD in children. Table 1 shows that the countries exhibiting the strongest collaborative ties with the US are China, Canada, and Germany. The most cited countries were Germany and France. Figure 3(b) shows the publication situation for each country using a density view. Collaboration networks in AI for pediatric CHD research (2000-2025). The top 10 countries with the most publications.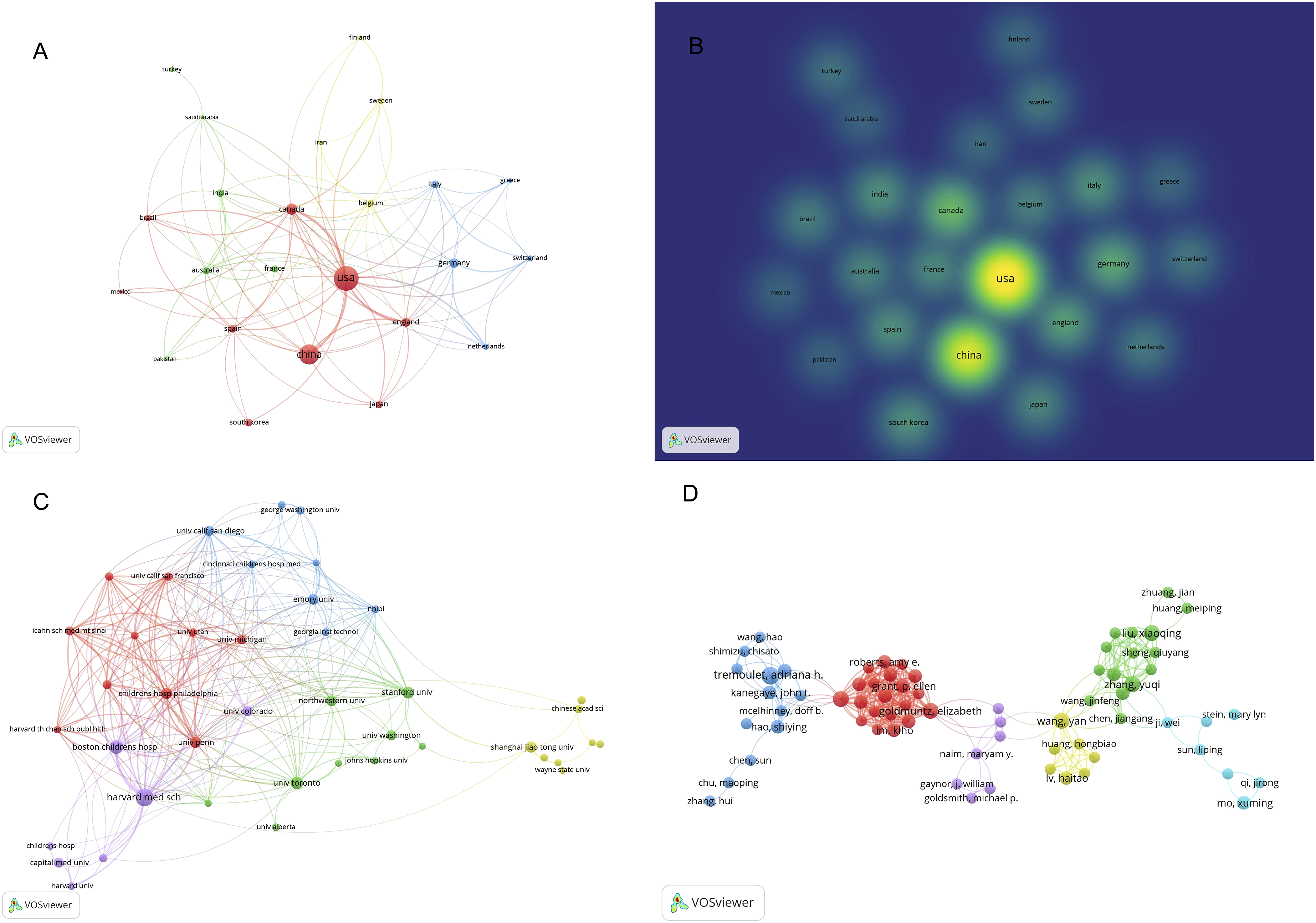
3.2.2. Institutions
A total of 1,010 institutions have published studies in this field. We used VOSviewer for a comprehensive visualisation of the institutions involved in research on AI and CHD in children (Figure 3(c)), with a requisite minimum of five published articles, resulting in 45 institutions being entered into the visualisation analysis. Each cluster included 7–10 entities, with 10 prominent emerging institutions: Harvard Medical School, Boston Children’s Hospital, University of Toronto, Stanford University, Children’s Hospital Philadelphia, Shanghai Jiao Tong University, University of Pennsylvania, Emory University, Northwestern University, and Capital Medical University. Critically, a significant number of leading institutions are located in the US (and some institutions are from China), with Harvard Medical School and Boston Children’s Hospital as leading institutions in this field. Shanghai Jiao Tong University has emerged as a prominent institution, especially in China, with the highest number of citations from China.
3.2.3. Authors
The top 10 productive authors in the field of congenital heart disease.
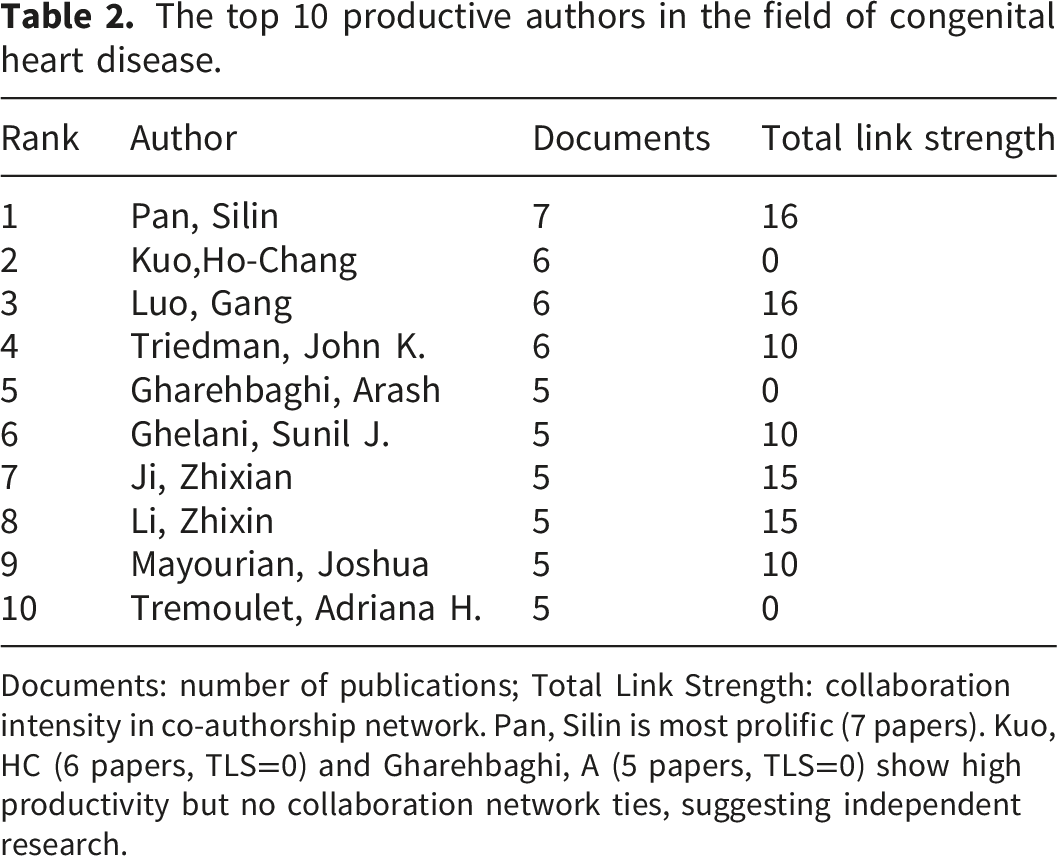
Documents: number of publications; Total Link Strength: collaboration intensity in co-authorship network. Pan, Silin is most prolific (7 papers). Kuo, HC (6 papers, TLS=0) and Gharehbaghi, A (5 papers, TLS=0) show high productivity but no collaboration network ties, suggesting independent research.
3.3. Co-citation analysis
3.3.1. Journals
Top 10 co-cited journals with citations and top 10 co-cited authors with citations.
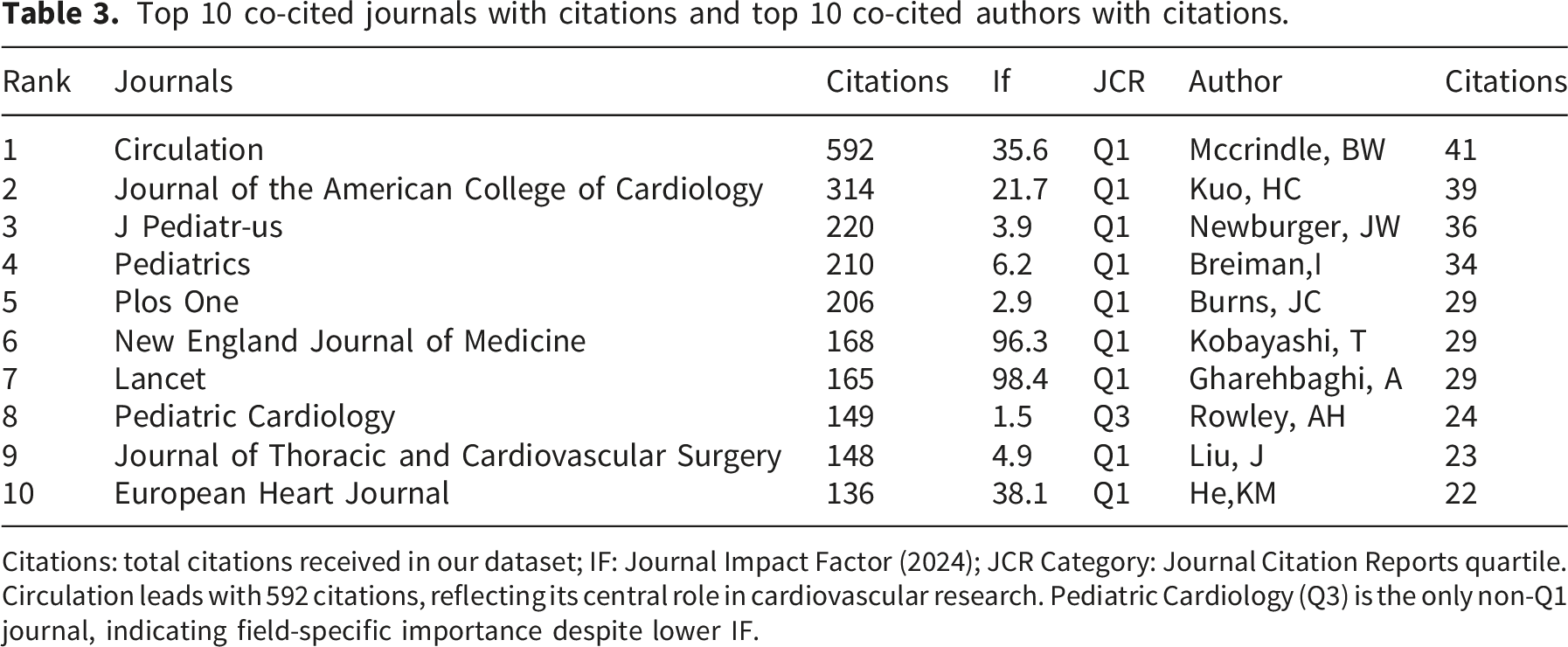
Citations: total citations received in our dataset; IF: Journal Impact Factor (2024); JCR Category: Journal Citation Reports quartile. Circulation leads with 592 citations, reflecting its central role in cardiovascular research. Pediatric Cardiology (Q3) is the only non-Q1 journal, indicating field-specific importance despite lower IF.

Journal co-citation network with top-cited journals labeled (Circulation, JACC, J Pediatr) and node size = citation count.
3.3.2. Authors
A total of 14,475 authors contributed to the 423 articles included in this study. Table 3 presents the 10 authors who achieved the highest total citation counts for their publications, spanning from 2000 to 2025. A comparison of Tables 2 and 3 reveals that the authors who published articles most frequently did not necessarily coincide with the authors of the most cited articles. Among the 10 leading authors, the articles by Kuo, HC, and Gharehbaghi, A, have the highest citation counts.
3.3.3. References
Co-citations, also known as co-cited literature, are citations that appear in multiple publications. Using Cite Space to cluster and analyse the retrieved literature, we derived four clusters, as shown in Figure 5. These clusters were well-structured (Q=0.8739) and highly reliable (S=0.9394). In recent years, the trend of research on the correlation between AI and CHD has shifted towards specific fields (clusters #0, #2, #3, and #4). The connections between the differently coloured areas represent the associations between different topics. For example, connections were observed between Kawasaki disease and ventricular dysfunction, indicating that there may be cross-research between these two topics in certain studies. Top 25 reference bursts with clusters.
We analysed 25 references with citation bursts to identify the most frequently cited studies in recent years, We analysed 25 references with citation bursts to identify the most frequently cited studies in recent years (Figure 6). The cut-off date was 5 June 2025. The most recently cited literature included a 2019 Attia study (strength: 3.08, time span: 2020–2025), which indicated a sharp increase in citations related to major cardiovascular findings. Most bursts occurred after 2010, particularly between 2015 and 2025. Citation bursts can last from a few years to more than a decade. Koenig (2006) experienced a citation burst between 2006 and 2009, whereas Attia (2019) experienced one burst between 2020 and 2025. Recent studies have attracted many citations, possibly owing to the rapid development in this area and the frequent dissemination of new findings. These studies span multiple disciplines including cardiovascular diseases, medical engineering, public health, computer vision, and neuroscience. This finding indicates that citation bursts occur across various fields. Many publications appear in high-impact journals such as Circulation, Nature Medicine, and JAMA Pediatrics, and the high impact of these journals may also be one of the reasons for the corresponding citation bursts. Some studies have short citation burst periods but high citation intensity, whereas others have long citation burst periods but low citation intensity, indicating that citation bursts exhibit different characteristics across studies. Reference co-citation timeline with clusters.
3.4. Keyword analysis
3.4.1. Co-occurrence
In Figure 7, ‘congenital heart disease’ and ‘children’ are positioned in the centre, indicating that these topics are the core themes of the research, suggesting that the field primarily focuses on CHD in children. In addition to the central themes, there are several high-frequency keywords closely surrounding the central themes, such as ‘machine learning’, ‘artificial intelligence’, ‘risk’, ‘diagnosis’, and ‘treatment’. The high frequency of these keywords indicates their significance in the research, representing the main methods, focal points, or objectives of the studies. This figure illustrates the thematic structure of hotspots in research on CHD in children. The core themes concentrate on the diagnosis, treatment, and risk assessment of CHD in children. The application of AI and machine learning technologies in this field is also an important research direction. Additionally, there were some emerging or less considered themes, such as long-term management and the role of health professionals, suggesting potential directions for future research, thereby helping scholars better understand the current state and development trends of research in this field. Keyword co-occurrence map.
3.4.2. Timeline clustering
The timeline chart in Figure 8 illustrates the evolution of research topics from 2000 to 2025. The themes of the systematic reviews using machine learning, AI, digital health, and atrial function began to emerge around 2020 and gradually developed in the following years, intersecting with other topics. As shown in the chart, research topics are becoming increasingly diverse, with new themes continuously emerging, and connections and intersections between themes becoming more complex. In recent years, themes related to machine learning, AI, and digital health (e.g. #5, # 6, and #7) have gradually become research hotspots, demonstrating the importance and application prospects of these fields in medical research. Timeline of keyword clusters (2000-2025).
3.4.3. Keyword bursts
As illustrated in Figure 9, in terms of time, the keywords for which there have been citation bursts have gradually evolved from early terms such as ‘coronary heart disease’ and ‘atherosclerosis’ to ‘cardiovascular disease’ and ‘heart rate variability’. Initially, the focus was mainly on the pathophysiology, diagnosis, and treatment of paediatric cardiovascular diseases. The figure illustrates the development of these keywords from topics beginning to gain attention in the early stages to new hotspots in (congenital) cardiovascular disease research. Regarding the intensity of citation bursts, the presence of terms such as ‘heart rate variability’ (intensity: 3.99) and ‘cardiovascular disease’ (intensity: 2.34) indicates their significant influence and attention in cardiovascular disease research. Some keywords, such as ‘convolutional neural network’ and ‘deep learning’, primarily relate to research on AI and machine learning and have become hotspots in emerging technology research, indicating that the research trend in paediatric cardiovascular diseases is shifting from aspects such as pathophysiology, diagnosis, and treatment to emerging technologies and metabolic syndrome, with a significant portion also moving towards areas such as ‘convolutional neural networks’. Top 25 keyword bursts (2000-2025).
4. Discussion
4.1. Overall trend
Using Cite Space and VOS viewer software, we statistically analysed 423 papers from 71 countries involving 2,784 authors and 1,010 institutions and sorted and visualised the findings in the fields of AI and CHD in children. Since 2016, research in this field has significantly increased. The peak years for research activities were 2022 and 2023, indicating that research in this field and its influence is constantly growing, with a particular spike occurring after 2016.
The US and China are the most active countries in terms of research in this field, publishing the largest number of documents. Not only are they active in their own research, but they also have extensive cooperative relationships with many countries. For instance, the US cooperates with countries such as Canada, France, and Germany, whereas China frequently cooperates with countries such as Japan, South Korea, and Australia. Their research directions and achievements have significantly impacted the development of research on AI and CHD in children worldwide. Harvard University, Stanford University, and the University of Toronto are relatively active in research in this field; simultaneously, these institutions have strong relationships with multiple institutions. Harvard University School of Medicine and Boston Children’s Hospital have absolute dominance in terms of the number of published articles (31and18), number of citations (573and508), and strength of links (95and71). Shanghai Jiao Tong University has a relatively large number of published papers, but its total link strength is weak (7), suggesting that it may emerge in terms of research on AI and CHD in children; however, it may not have formed a stable cooperative network yet. Most cooperative institutions are limited to intraregional connections.
The most popular journals for publication were Circulation, the Journal of the American College of Cardiology, Journal of Pediatrics, and Pediatrics. The core themes focused on the diagnosis, treatment, and risk assessment of CHD in children. The application of AI and machine learning technologies in this field is also an important research direction.
Silin Pan and Gang Luo are outstanding scholars from China and are the top two authors in terms of the number of published articles. They collaborated and used a new deep learning method to predict elevated pulmonary artery pressure in children with ventricular septal defects using standard chest radiographs, which can effectively identify the risk of pulmonary hypertension. 10
4.2. Analysis of research hotspots, trends, and key insights
Keyword analysis is a crucial tool for understanding fundamental themes and cutting-edge developments within a specific research domain. By examining clustering patterns and temporal perspectives, scholars can acquire profound insights into the prevalent topics and nascent trends that characterise an area of study. Emergency terms serve as indicators of cutting-edge topics. 11 Moreover, examining the co-citation network of references can yield valuable insights into the foundational knowledge and development of the research frontier. Drawing from these analyses, we have delineated several key areas and emerging trends in the subsequent sections. 12 The US (40% of publications) and China (25.6%) reflects distinct underlying drivers. US leadership comes from steady funding from the National Institutes of Health and National Science Foundation 13 and from academic medical centres that are integrated, such as Harvard and Boston Children’s Hospital. Whereas, China’s rise is driven by its national AI strategy and concentrated government investment. 14 The current research landscape has been shaped by these contrasting pathways: bottom-up institutional excellence and top-down national priorities.
Our analysis provides several specific insights that were previously unclear, and confirms the overall growth trend.
The focus of studies in this field have shifted from pathophysiology to computational tools. Keyword burst analysis revealed an evolutionary trajectory (Figure 9). Before 2015, research focused mainly on pathophysiology-related terms such as ‘coronary heart disease’ and ‘atherosclerosis’. Since 2020, there has been a significant increase in searches for terms such as ‘convolutional neural network’, ‘deep learning’, and ‘heart rate variability’, suggesting a significant alternation in how people think about this topic. This field now extends beyond the use of AI to solve existing problems. New forms of analysis are driven by computational tools, such as automated image interpretation and risk prediction from routine electrocardiograms (ECGs). This technological shift aligns with evolving clinical needs. Since 2020, there has been a growing demand for prognostic tools to guide personalised management. This differs from the use of diagnostic algorithms. Deep learning techniques can process complicated medical images. This important development may help address implementation challenges in low-resource settings. In this context, a lack of experts restricts access to echocardiography and cardiac magnetic resonance imaging (MRI).
Key publications and authors have played distinct roles (Figure 6 and Table 3). Attia, ZI (2019) has been cited several times since 2020. Research on AI-ECG has significantly affected research into paediatrics in adult cardiology. Moreover, an analysis of Tables 2 and 3 shows a vital difference: high productivity is not equivalent to a high impact. Pan Silin was the most prolific author; however, Kuo, HC, and Gharehbaghi, A. had the most cited works. This indicates that different research groups have different roles; some drive the field forward through volume, whereas others drive it through highly influential methodological or clinical studies.
Research activities and collaboration gaps have been identified. The US is dominant (40% of publications), and Shanghai Jiao Tong University is emerging as a key player in China. However, a potential collaboration gap is indicated by the relatively low total link strength of Shanghai Jiao Tong University (7) compared to its publication output. The global collaborative network has not yet been fully integrated, indicating the need for future cooperation and knowledge transfer between countries. Figure 3(d) shows the author co-authorship network, which was constructed with a co-authorship threshold of 2 and visualised with attraction = 7, repulsion = -1, and clustering parameters = (1, 1). This network revealed six research clusters that focused on different aspects of AI in paediatric CHD. The network structure showed that while individuals within the same group worked well together, those from different groups do not work together much. The co-citation clusters shown in Figure 5 corroborate this pattern. These clusters were ventricular dysfunction (#0), Kawasaki disease (#2), and intelligent auscultation (#4). Each cluster represents a relatively siloed research community. Each community had its own foundational literature. To accelerate the process of transitioning from new methods to their use in patient care, it is essential to combine these technical and clinical groups more closely.
4.3. Application of AI in prenatal screening
A meta-analysis showed that the diagnostic accuracy of prenatal ultrasound for detecting coarctation of the aorta (CoA) was low to moderate for all parameters, a finding consistent with multivariate models. Several prenatal ultrasound parameters were associated with an increased risk of developing CoA after birth. However, even when combined, the diagnostic accuracy was only moderate 15 . The use of AI in ultrasound diagnosis reduces human error and enhances image recognition, helping to detect abnormalities quickly and simplify the operating process. A US study examined the combination of AI technology with echocardiography to improve the detection of congenital heart defects. The sensitivity of AI for foetuses exceeds 90%; however, the current AI technology still has many limitations 16 . A multi-international, multi-centre, and multi-disciplinary study conducted in the UK using deep learning-based image and video analysis to distinguish normal foetal hearts from those diagnosed with CHD is currently in the development, training, and validation stages 17 . Kimd et al. used Heart Assist to conduct AI-based automatic classification, annotation, and measurement of foetal hearts and found that its classification accuracy rate reached 99.4%. 18
Nevertheless, AI has enormous potential for the improvement of medical imaging. It is expected to become a standard diagnostic tool for foetal echocardiography. 19
4.4. Application of AI in the diagnosis of CHD in children
A study in Taiwan using AI to analyse ECGs provided a cost-effective alternative to traditional methods for detecting significant CHD in children aged <5 years. The proposed AI model significantly outperformed traditional ECG interpretation by paediatric cardiologists in terms of accuracy (67.1%) and sensitivity (71.6%), highlighting the potential of AI-assisted ECG analysis for screening CHD in infants. 20 Mayourian et al. trained a convolutional neural network using paired ECG–echocardiogram data from patients aged ≤18 years with no significant CHD (with an interval of ≤2 days) to achieve human expert-level classification of severe left ventricular (LV) dysfunction, hypertrophy, and dilatation (separately and as an overall result), with external validation. The model outperformed the paediatric cardiologist benchmark in predicting LV hypertrophy, showing promise for inexpensive screening for LV dysfunction and remodelling in children. 21 Cardiac MRI (CMR) can provide anatomical and physiological assessments of patients that are crucial for diagnosing CHD. However, the execution and analysis of CMR scans can be time consuming, which hinders the broader application of CMR in CHD. Recent studies have suggested that AI has the potential to improve efficiency, enhance image quality, and reduce errors. 22 A recent study found that deep learning-based free-running three-dimensional (3D) dynamic imaging can simultaneously acquire dynamic and vascular images. When evaluating patients with CHD, highly accelerated free-running 3D dynamic imaging combined with deep learning reconstruction reduces the acquisition time and provides volume measurements comparable to those of 2D dynamic imaging and clinical 3D magnetic resonance angiography. 23 Khalaph et al. developed and validated a simplified 12-lead ECG algorithm (SMART-WPW) that can accurately identify the location of the accessory pathway in patients with Wolff–Parkinson–White (WPW) syndrome. In a subgroup of children (n = 76; mean age, 14 ± 3 years; 61% female), the algorithm’s accuracy was higher than that of the Arruda algorithm (97% vs. 62%, p < 0.001). Its use may improve preoperative evaluation and ablation planning in patients with WPW syndrome. 24 AI models can recognise subtle abnormal signals in an ECG, and their accuracy is often higher than that of regular doctors. While traditional cardiology tests require expensive equipment and specialised doctors, AI ECG recognition technology can complete the diagnosis using an ordinary ECG, greatly saving time and effort. An AI model can capture abnormal signals that are easily overlooked by traditional methods, thus reducing misdiagnoses and omissions, adapting to rapid changes in the electrophysiological characteristics of children’s hearts, and providing decision-making support for clinicians to help them judge the condition more accurately and optimise treatment plans. However, AI models have certain limitations. The performance of AI is highly dependent on the quality and quantity of the training data. Biased or incomplete data can decrease the accuracy and reliability of a model. The complex structures of some deep learning models make it difficult to explain their decision-making processes, limiting the clinicians’ trust in the diagnostic results to some extent. Although AI performs well in screening certain types of CHDs, its recognition ability may be insufficient for some complex or rare types of lesions, and it still requires professionals to perform data acquisition, model training, and interpretation of results.
4.5. Application of AI in the treatment of CHD in children
Overreliance on AI technology may cause doctors to lose their clinical skills and reduce their ability to make comprehensive judgments about a disease. Furthermore, the models may misdiagnose, particularly in complex clinical situations. Relying entirely on the diagnostic results yielded by AI can lead to misdiagnoses or missed diagnoses, thereby delaying patient treatment. The application of AI in the medical field has raised ethical and legal concerns. For instance, can AI models be held responsible for medical errors? How can we ensure that AI applications are aligned with medical ethics? Currently, relevant laws and regulations are not well established, posing risks to the use of AI for treating CHD in children. In the drug-based treatment of CHD in children, the drug selection factors to be considered are diverse and complex. Firstly, in regard to the safety and efficacy of the drugs (the primary considerations), because most drugs have not undergone specialised clinical trials for children, many drugs are used ‘off label’, particularly in the treatment of cardiovascular diseases, where this situation is particularly common. 25 Second, the physiological characteristics of children differ significantly from those of adults. The pharmacokinetics and pharmacodynamics of drugs may differ significantly in children. Therefore, individualised adjustments must be made based on the weight, age, and physiological status of the children being treated. Diuretics and cardiac stimulants are the most commonly used drugs. Therefore, during diuretic use, it is necessary to regularly monitor the patients’ electrolyte levels to avoid potential complications. 26
4.6. Application of AI in the long-term management of CHD in children and the role of health professionals
AI technology has great potential for the long-term management of CHD in children, enhancing the accuracy of diagnosis, optimising treatment plans, and improving the quality of life of patients. Nursing staff can use AI systems to monitor patient vital signs, identify potential health issues promptly, and implement appropriate care measures.
Moreover, in recent years, various regions have begun attempting to improve ordinary ECGs and apply them in different industries. Li et al. found that Apple Watch ECG detection could be used to make repeatable and accurate QTc interval measurements, confirm abnormal T-wave morphology, and detect QTc interval prolongation in children and adolescents with long QT syndrome. 27 A convolutional neural network model can easily identify obstructive sleep apnoea in children’s ECG, providing a simpler, faster, and easier-to-implement diagnostic test for clinical practice. 28 Nechita et al. evaluated an AI-enhanced ECG screening program to analyse the cardiovascular risk in athletes. They analysed the resting 12-lead ECGs of healthy children and adolescents participating in handball, football, track and field, weightlifting, judo, and karate. The AI algorithm was trained using a labelled dataset. The parameters included the QTc interval, PR interval, and QRS duration. The accuracy, sensitivity, specificity, and precision of the AI system were 97%.87%, 75%, 98.3%, and 98%, respectively. The statistical and AI-ECG screening programs demonstrated high precision and scalability in the proposed athlete cardiovascular health risk stratification scheme. 29
4.7. Bridging the gap: Implementation challenges in low-resource settings
Our analysis revealed a growing research interest in AI for paediatric CHD; however, a gap remains between publication and real-world clinical implementation, particularly in LMICs, where the CHD burden is the highest. Recent studies have highlighted this issue. Negussie et al. 30 identified multiple barriers to the use of AI-enhanced CMR for CHD diagnosis in sub-Saharan Africa. These are rarely reflected in bibliometric data, but are decisive for technology deployment.
Infrastructure and equipment constraints also exist. The average number of MRI scanners in sub-Saharan Africa is between 0.8 and 1 for every million people. 30 This is in comparison with between 7 and 10 for every million people in European countries such as Romania. More than half of the countries in West Africa have fewer than 0.1 MRI scanners per million individuals. Some nations, including Guinea and Côte d'Ivoire, operate a single MRI unit for over 13 million people. AI-enhanced diagnostic tools are limited by infrastructural deficits, regardless of algorithmic sophistication. There are also gaps in the workforce and training. There is a shortage of trained radiologists, sonographers, and biomedical engineers proficient in both cardiac imaging and AI applications. Even when equipment is available, a lack of local expertise causes underutilisation of equipment. Economic and financial barriers exist. Furthermore, AI integration is expensive in limited settings. Most patients in LMICs pay for advanced imaging themselves because the costs often exceed their monthly income. This contrasts with the assumptions of much published research, which rarely addresses affordability or cost-effectiveness in low-resource contexts. Data representativeness and bias in algorithms may affect the performance in diverse populations owing to differences in the disease spectrum and image acquisition. The CAIFE study 31 protocol noted that a lack of diverse datasets from LMICs risks worsening health disparities.
To address these gaps, we need multifaceted strategies: low-field MRI technologies, public-private financing, trained local workforces, and AI solutions. 30 Future research should prioritise the implementation of scientific approaches that evaluate performance, real-world effectiveness, cost-effectiveness, and impact.
4.8. Bridging bibliometric findings to clinical practice: Implications for medication safety
Our findings directly address the critical clinical challenges in paediatric CHD care, particularly medication safety. This need is also evident in our keyword data. In Figure 9, terms like “prediction” and “outcome” have grown sharply. This demonstrates that the research field is shifting towards risk assessment and patient safety. Children with CHD are vulnerable to drug-related side effects owing to their age, medication regimen, and hospitalisation. 32 These paediatric-specific risk factors demand system-level strategies aligned with the AI research trends identified in our analysis. Our analysis (Figure 9) showed a shift towards ‘deep learning’, ‘prediction’, and ‘personalised medicine’. This change supports new recommendations for safer heart drug therapies. Recent evidence supports Electronic Health Record-based monitoring, personalised dose adjustments, and cardiology-pharmacotherapy teams.33,34 The implementation of these strategies is well-suited to AI-driven tools, particularly those that use deep learning for risk assessment and prediction. Predictive models can be used to identify high-risk patients (young age and multiple medications) and flag drug interactions in real time. This demonstrates how future AI tools can support safer CHD prescriptions and uptake in children. It also addresses the gap between research and clinical implementation.
4.9. Limitations
This study had some limitations that should be acknowledged. First, despite being a leading bibliometric database, the WOSCC is biased towards English language publications and journals from high-income countries. 35 The data sources of this study were limited to the WOSCC and English literature, and important findings in other languages or non-indexed databases may have been overlooked. Consequently, we may have omitted relevant non-English studies on AI applications in paediatric CHD, particularly those published in local journals from LMICs. The results show an overrepresentation of high-income settings, probably due to linguistic and geographic biases (for example, the US accounts for 40% of publications). Future research should integrate multiple platforms, such as Scopus and PubMed, to enhance comprehensiveness. Second, high-income countries were overrepresented. Our findings reveal that research is concentrated in high-income countries and major institutions in China. Regions with a substantial CHD burden, such as sub-Saharan Africa, Southeast Asia, and some parts of Latin America, remain largely underrepresented. This indicates wider inequalities in the global health research infrastructure, not the true spread of the CHD burden. For example, research output from sub-Saharan Africa is minimal despite the region having an estimated birth prevalence of CHD that is substantially higher than that of the US (463 per million population compared to 137 per million). 30 Third, the gap between publication trends and real-world implementation should be addressed. A key issue with bibliometric analysis is that it focuses on research activity (e.g. publications) rather than on clinical implementation.
The growing number of publications on AI in paediatric CHD is a sign of growing academic interest; however, this does not necessarily mean that the technology is being used widely in clinical practice, especially in regions where resources are limited. A recent review by Negussie et al. 30 emphasised this point. Even advanced AI-enhanced diagnostic tools, such as CMR, face formidable barriers to implementation. This is particularly the case in low-resource settings. Inadequate infrastructure is a problem in Africa; for example only 0.8 MRI scanners are available per million people.31Furthermore, power supply is unreliable, Internet connectivity is limited, there is a shortage of trained professionals, and costs are prohibitive. These challenges, which are rooted in the real world, are frequently obscured by analyses driven by publications. However, they are of critical importance in determining whether AI technologies can achieve an equitable impact.
We only used the Web of Science Core Collection and English papers. This may cause bias. English journals are more prevalent in high-income countries. Non-English studies may therefore be missed. This could impact the extent to which our findings can be applied to other regions. One more point: our data demonstrate research interest rather than real-world use. Further research is required to determine whether AI is actually being used in clinics.
5. Conclusion
The management of CHD in children shows promising prospects in the field of AI, with new possibilities for improving the health outcomes and quality of life of patients. Our study demonstrates that the focus has shifted from the study of diseases to innovation driven by deep learning. This is because of the growing need for tools to predict outcomes. For future research, our studies show the need for increased collaborations between computer scientists and children’s heart doctors to convert new ideas into real use. The growing need for personalised risk stratification, especially in the area of medication safety, is in line with the shift towards deep learning and predictive modelling in clinical practice. Children with CHD face distinct risks owing to their young age and use of multiple medications. AI tools integrated with electronic health records can provide safe prescriptions and targeted monitoring. For health policy, the fact that high-income countries are overrepresented, while there is hardly any research from regions with the most problems, such as sub-Saharan Africa, shows a large equity gap that needs to be addressed by giving priority funding to research on how to implement changes. Success relies on a balance between technology and care, safety control, and ethical and legal framework improvements. It is vital to bridge the gap between research and implementation in LMICs where the burden of CHD is the highest. We must address challenges related to infrastructure, workforce, economics, and data representativeness to ensure that AI advances equitably improve child health globally. Children with CHD can truly benefit from AI-driven technologies only if these challenges are adequately addressed. Future research and practice should closely focus on these core issues to promote healthy development in this field.
Supplemental material
Supplemental material - Artificial intelligence in the diagnosis and management of congenital heart disease in children: A 25-year bibliometric analysis
Supplemental material for Artificial intelligence in the diagnosis and management of congenital heart disease in children: A 25-year bibliometric analysis by Yinmin Zhang, Yuting Lu, Xiong Qian, Shufeng Li, Yadan Yao, Shaomei Zhou and Taotao Ge in Digital Health.
Supplemental material
Supplemental material - Artificial intelligence in the diagnosis and management of congenital heart disease in children: A 25-year bibliometric analysis
Supplemental material for Artificial intelligence in the diagnosis and management of congenital heart disease in children: A 25-year bibliometric analysis by Yinmin Zhang, Yuting Lu, Xiong Qian, Shufeng Li, Yadan Yao, Shaomei Zhou and Taotao Ge in Digital Health.
Footnotes
Acknowledgments
I would like to express my appreciation to my co-authors, whose professional knowledge and experience were essential for the success of this study. I would also like to extend my sincere thanks to the reviewers and editors of the journal, whose efforts helped to refine and improve this study.
Ethical considerations
All of the primary data used in our research came from public databases, so an ethical review was not required.
Author contributions
Yinmin Zhang: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing– original draft, Writing– review & editing. Yuting Lu: Conceptualization, Writing– original draft, Writing– review & editing. Xiong Qian: Methodology, Writing– original draft, Writing– review & editing. Shufeng Li: Conceptualization, Writing– original draft, Writing– review & editing. Yadan Yao: Supervision, Writing– original draft, Writing– review & editing. Shaomei Zhou: Writing– review & editing, Taotao Ge: Writing– review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.