
Abstract
Objective
Social media has become an important channel for obtaining information about vertigo. Benign paroxysmal positional vertigo (BPPV) is the most common peripheral vestibular disorder, yet the quality and reliability of BPPV-related content on social media platforms remain limited. Inaccurate information may mislead patients or encourage inappropriate self-management. This study quantitatively assessed the quality and reliability of BPPV-related short videos on Douyin (the Chinese version of TikTok) and Bilibili.
Methods
On September 28, 2025, videos about BPPV on Douyin and Bilibili were retrieved, and various key information such as video types, content, parameters, and user participation was extracted. The Global Quality Scale (GQS) and modified DISCERN (mDISCERN) were used to evaluate video quality and reliability, and non-parametric testing, correlation analysis, and multivariable logistic regression were used for data analysis.
Results
The quality and reliability of BPPV videos on Douyin and Bilibili were rated as fair quality (median GQS = 3) and low reliability (median mDISCERN = 2). Doctors were the main uploaders, but their scores were close to the overall average. User engagement (likes, collections, comments, shares) was highly correlated but had no relationship with video quality. The duration of videos with high user participation was 60–180 seconds on Douyin and 150–300 seconds on Bilibili. Longer duration independently predicted higher video quality (OR = 1.003, P = 0.024).
Conclusions
The quality and reliability of BPPV short videos on Douyin and Bilibili were suboptimal. Improving this situation requires the joint efforts of doctors, patients, and social platforms.
Keywords
Introduction
Benign paroxysmal positional vertigo (BPPV) is a peripheral vestibular disorder that causes brief episodes of vertigo when the head moves into certain positions.1,2 This condition mainly occurs when otoconia move into the semicircular canals, which triggers abnormal vestibular signals during head movement. 3 It was reported that the incidence of BPPV is about 64 cases per 100,000 people, and about 2.4% of people experience BPPV in their lifetime.2,4 Repeated vertigo is closely related to the patient’s risk of falling, anxiety, avoidance of activities, and decline in quality of life, and brings a heavy medical burden.1,5–9 Despite its considerable burden, many individuals with vertigo or dizziness do not seek professional care.10–12 This shows a gap between health needs and the reliable information people can access.
In recent years, the Internet has become a mainstream source for the public to obtain information about vertigo and dizziness. 13 Among the various online channels, short-video formats on social media have gained popularity due to their engaging and intuitive presentation.14,15 In this setting, a quick search using relevant keywords can yield numerous video-based resources on BPPV. However, the use of these platforms also has limitations. The accuracy of the content varies, and much of it is produced without any form of review. For a condition like BPPV, one concern with popular science videos is that some patients may try to perform self-repositioning maneuvers after watching them. These limitations may cause patients to misunderstand their condition and even make poor health choices.16,17 Despite the growing availability of such content, quantitative assessments of BPPV-related short videos on social media remain limited. A quantitative assessment of their quality and reliability is needed, as this is critical for both patients and video creators.
In China, Douyin (the Chinese version of TikTok) and Bilibili are among the most popular video social media platforms. To address the current lack of quantitative evaluation for content related to BPPV, the Global Quality Score (GQS) and the modified DISCERN (mDISCERN) were used to assess the quality and reliability of the videos. In addition, we examined how video characteristics (e.g., source, content type, duration) and engagement metrics (e.g., likes, collections, comments, shares) were associated with quality scores. By identifying the existing shortcomings, this study aims to provide viewers with a reference for the quality of BPPV-related short videos on these platforms and to offer suggestions for improving the practical dissemination of BPPV knowledge.
Methods
Platform overview
China’s Douyin (https://www.douyin.com) and Bilibili (https://www.bilibili.com) are the most popular video-sharing platforms. 18 Both platforms share a high level of interactivity. Douyin is characterized by a larger user base and generally shorter video durations.
Study design and setting
This was a cross-sectional content analysis study of publicly available BPPV-related short videos on two Chinese video-sharing platforms, Douyin and Bilibili.
Search strategy
To reduce potential bias from personalized recommendation algorithms, searches were performed using a newly created account with no prior browsing history records. All data were collected on September 28, 2025. A single systematic search was performed on each platform using the same search procedure and default platform search settings: the Chinese keyword “耳石症”, a commonly used Chinese lay expression for BPPV, was used to search for BPPV-related videos on Douyin and Bilibili. The search results were recorded in the default order determined by the platforms’ recommendation systems.
Inclusion and exclusion criteria
To ensure stable statistical results, at least 100 videos were required for the analysis.19–21 A total of 240 BPPV-related videos were initially identified. Exclusion criteria included: (1) duplicate content; (2) lack of medically relevant information on BPPV; (3) content primarily promoting commercial products or services. Videos meeting any of these exclusion criteria were removed. If the final number of eligible videos was fewer than 100 on either platform, additional videos were included according to the initial search order until the predefined sample size was reached.
Video feature extraction
Two investigators independently extracted video-related characteristics, followed by a consistency check; any disagreements were reconciled through discussion. Recorded variables included uploader name, channel or video URL, video title, posting date, video length, number of followers of the uploader, cumulative likes of the uploader, and engagement indicators (likes, collections, comments, and shares).
Uploaders were classified into seven source categories:
(1) doctors; (2) other healthcare workers; (3) hospitals or healthcare departments; (4) science communicators; (5) non-medical organizations; (6) patients; and (7) the general public.
Video content was coded into nine thematic domains: (1) treatment; (2) general overview of BPPV; (3) diagnosis; (4) prevention; (5) patient experience; (6) etiology or triggers; (7) symptoms; (8) pathophysiology and anatomy; and (9) differential diagnosis.
Video quality and reliability
The GQS and the mDISCERN instrument were applied to evaluate the overall quality and credibility of BPPV-related videos.18,22,23 Two authors with clinical experience in otolaryngology and BPPV management independently scored each video, and any differences in their ratings were settled through discussion. Each video was scored according to the original GQS and mDISCERN criteria. For BPPV-specific content, the established 2017 Clinical Practice Guideline: Benign Paroxysmal Positional Vertigo (Update) from the American Academy of Otolaryngology–Head and Neck Surgery Foundation was used as the main reference standard. 5 The raters considered whether the videos accurately presented key BPPV-related information covered by the guideline, including positional vertigo symptoms, diagnostic maneuvers such as the Dix-Hallpike maneuver and supine roll test, differentiation from other causes of dizziness or vertigo, canalith repositioning procedures, medical therapy, follow-up assessment, evaluation of persistent symptoms, recurrence risk, and patient education.
The GQS rates the quality of a video by looking at its accuracy, completeness, and usefulness. It uses a 1–5 scale, with higher scores reflecting better quality. The mDISCERN is similar in structure but focuses on reliability. It contains five yes-or-no items that examine whether the video is easy to understand, cites its sources, presents information objectively, offers additional details, and acknowledges uncertainty. Details for both tools can be found in Supplementary Table S1 (GQS) and Supplementary Table S2 (mDISCERN).
For easier interpretation, both scoring systems were grouped into broader categories. GQS scores from 1 to 5 represent very poor, poor, fair, good, and excellent quality. For mDISCERN, the five levels were defined as follows: 0 for unreliable, 1–2 for less reliable, 3 for fairly reliable, 4 for relatively reliable, and 5 for reliable.
Statistical analyses
Statistical analyses were conducted using R software (version 4.3.2). The distribution of continuous variables was examined using the Shapiro–Wilk test. Continuous variables were summarized as median (interquartile range, IQR) because the distributions were generally non-normal, whereas categorical variables were presented as counts and percentages [n (%)]. Differences between two groups were analyzed using the Mann–Whitney U test, whereas comparisons across more than two groups were performed using the Kruskal–Wallis test; categorical variables were compared using the chi-square test or Fisher’s exact test, as appropriate. Inter-rater reliability was evaluated using the intraclass correlation coefficient (ICC). 24 Correlations were examined with Spearman’s ρ, interpreted as: |ρ| < 0.20, very weak; 0.20–0.39, weak; 0.40–0.59, moderate; 0.60–0.79, strong; and ≥0.80, very strong. 18
To identify independent factors associated with video quality, a parsimonious multivariable logistic regression model was constructed. High-quality videos were defined as those with both a GQS >3 and a mDISCERN score >3. Variables representing video characteristics and source credibility were considered for multivariable analysis. Among them, video duration and uploader type were included in the final model as key predictors of video quality. Uploader type was categorized as professional (doctors, other healthcare workers, hospitals/departments, and science communicators) or non-professional (non–medical organizations, patients, and the general public). Engagement metrics (likes, collections, shares, and comments) were excluded from the model because they are highly intercorrelated and conceptually represent consequences rather than determinants of video performance, which could introduce reverse causality and multicollinearity. Odds ratios (ORs) with 95% confidence intervals (CIs) were reported, and statistical significance was set at p < 0.05.
Results
Video screening process
In total, 240 BPPV-related videos were initially identified (120 from Douyin and 120 from Bilibili). After eligibility screening, 17 videos were excluded due to duplication (Douyin: 9; Bilibili: 8) and 2 were excluded because they lacked BPPV-specific information (both from Bilibili). Consequently, 221 videos (Douyin: 111; Bilibili: 110) were included in the final analysis. The screening process is illustrated in Figure 1. Flowchart of video identification and selection across Douyin and Bilibili.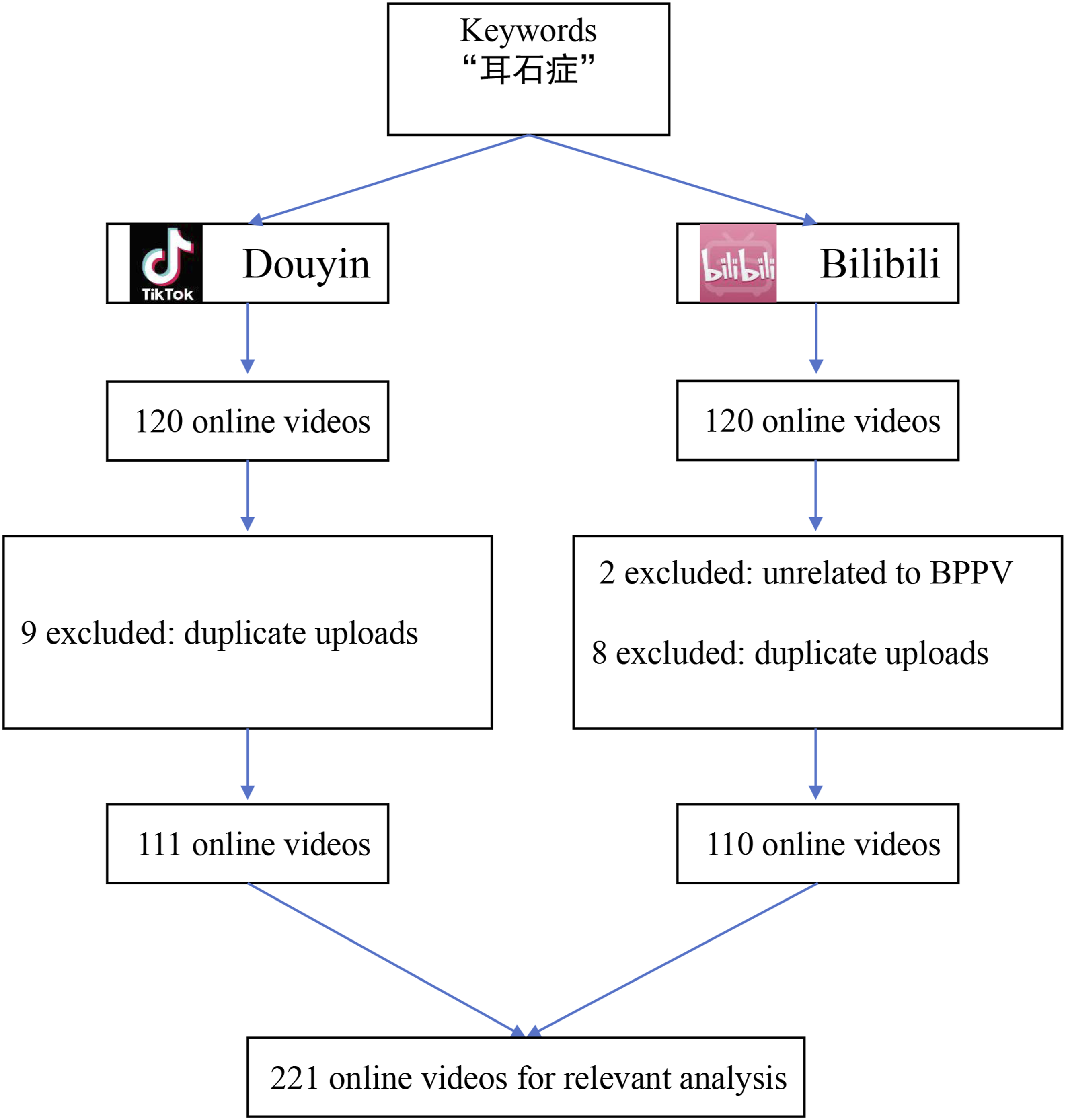
Video characteristics
Characteristics of BPPV-related videos on douyin and bilibili.

BPPV, Benign paroxysmal positional vertigo; IQR, interquartile range; GQS, Global Quality Score; mDISCERN, modified DISCERN.
On Douyin, the types of video uploaders ranked from most to least common were: - Doctors (77.5%, 86/111) - Patients (11.7%, 13/111) - Other healthcare workers (7.2%, 8/111) - Hospitals or clinical departments (2.7%, 3/111) - The general public (0.9%, 1/111).
On Bilibili, the types of video uploaders ranked from most to least common were: - Doctors (46.4%, 51/110) - Science communicators (32.7%, 36/110) - The general public (12.7%, 14/110) - Patients (5.5%, 6/110) - Hospitals or departments (2.7%, 3/110).
For video content, most videos focused on a few main themes: treatment, general overviews, and patient experiences. Content related to common symptoms was also presented but to a lesser extent, whereas topics such as pathophysiology, etiology, diagnosis, prevention, and differential diagnosis were rarely covered. Figure 2 shows the distribution of video sources and content categories. Comparison of video source types and content categories between Douyin and Bilibili. (a) Source distribution; (b) Content distribution.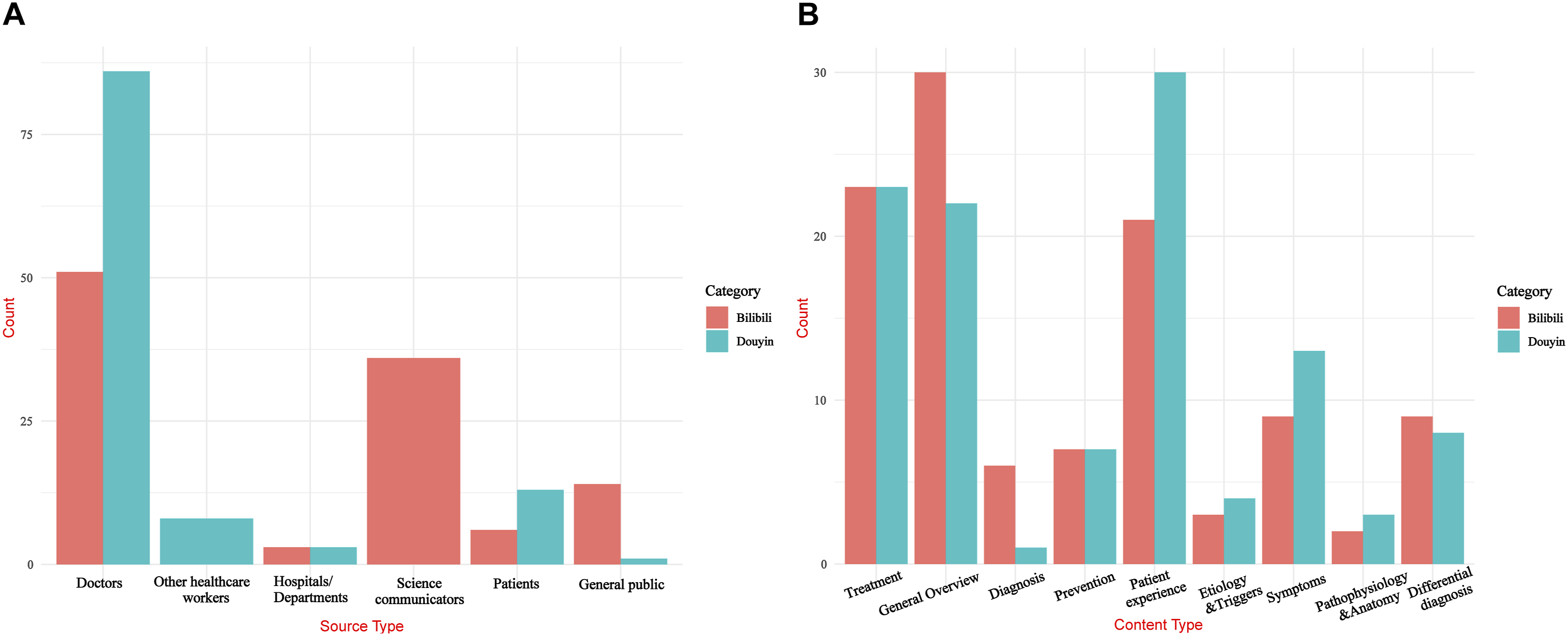
Video quality
The ICC for interobserver reliability was 0.892 (95% CI, 0.871–0.910), indicating strong reliability. The median [IQR] GQS was 3.00 [2.00–3.00] for Douyin and 3.00 [2.00–3.00] for Bilibili (P=0.227). The corresponding median [IQR] mDISCERN scores were 2.00 [1.50–3.00] and 2.00 [2.00–3.00], respectively (P=0.216) (Table 1). According to the grading thresholds in Methods section, videos on both platforms were rated as fair in GQS and less reliable in mDISCERN. Figure 3 visualizes quality scores. Violin plots showing the distribution of Global Quality Score and modified DISCERN scores for BPPV-related videos on Douyin and Bilibili.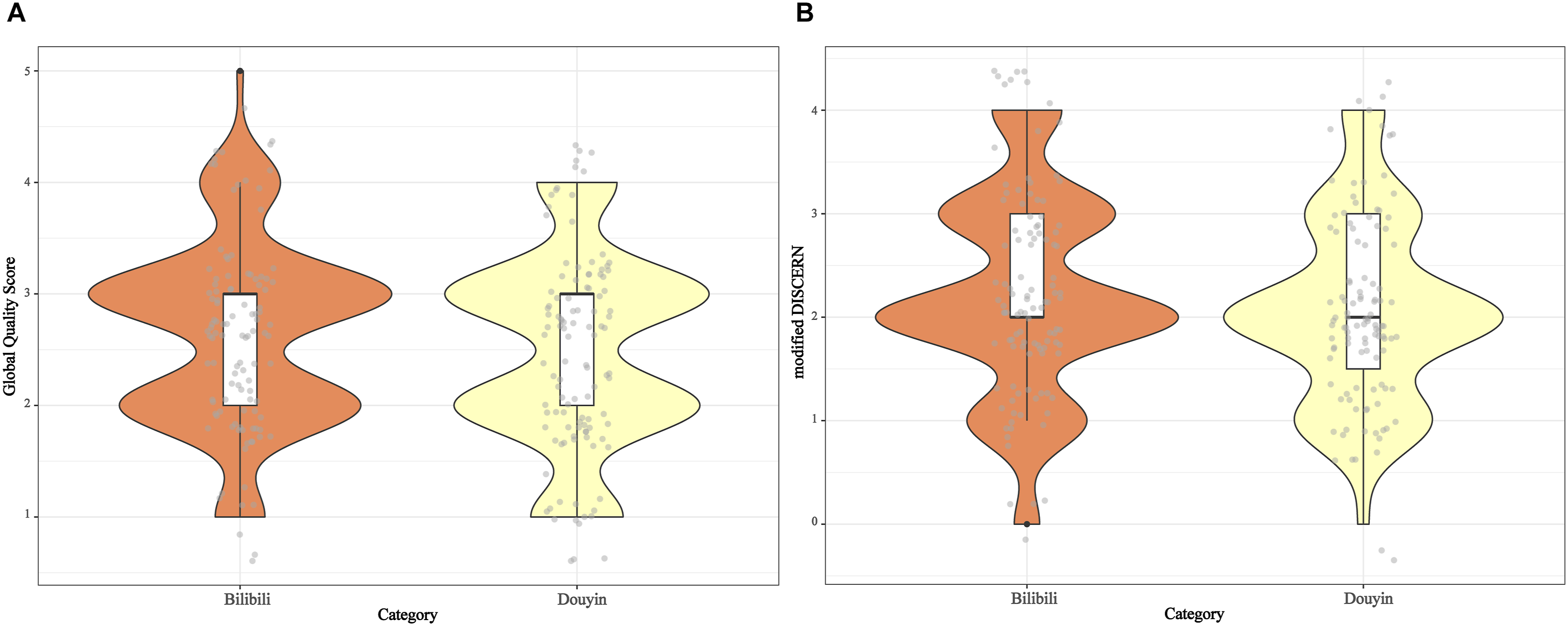
Subgroup data by platform
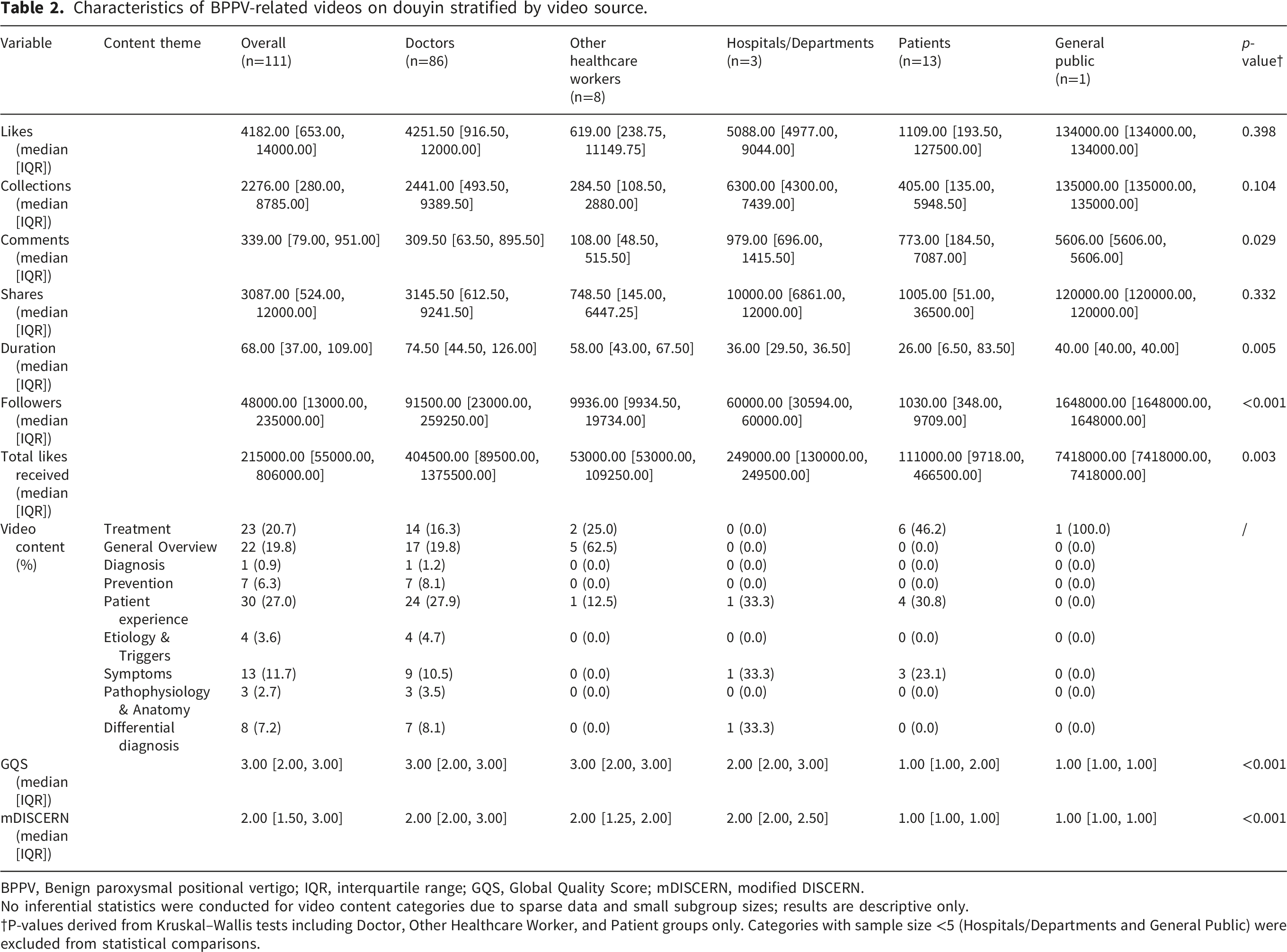
Characteristics of BPPV-related videos on douyin stratified by video source.
BPPV, Benign paroxysmal positional vertigo; IQR, interquartile range; GQS, Global Quality Score; mDISCERN, modified DISCERN.
No inferential statistics were conducted for video content categories due to sparse data and small subgroup sizes; results are descriptive only.
†P-values derived from Kruskal–Wallis tests including Doctor, Other Healthcare Worker, and Patient groups only. Categories with sample size <5 (Hospitals/Departments and General Public) were excluded from statistical comparisons.
Characteristics of BPPV-related videos on bilibili stratified by video source.
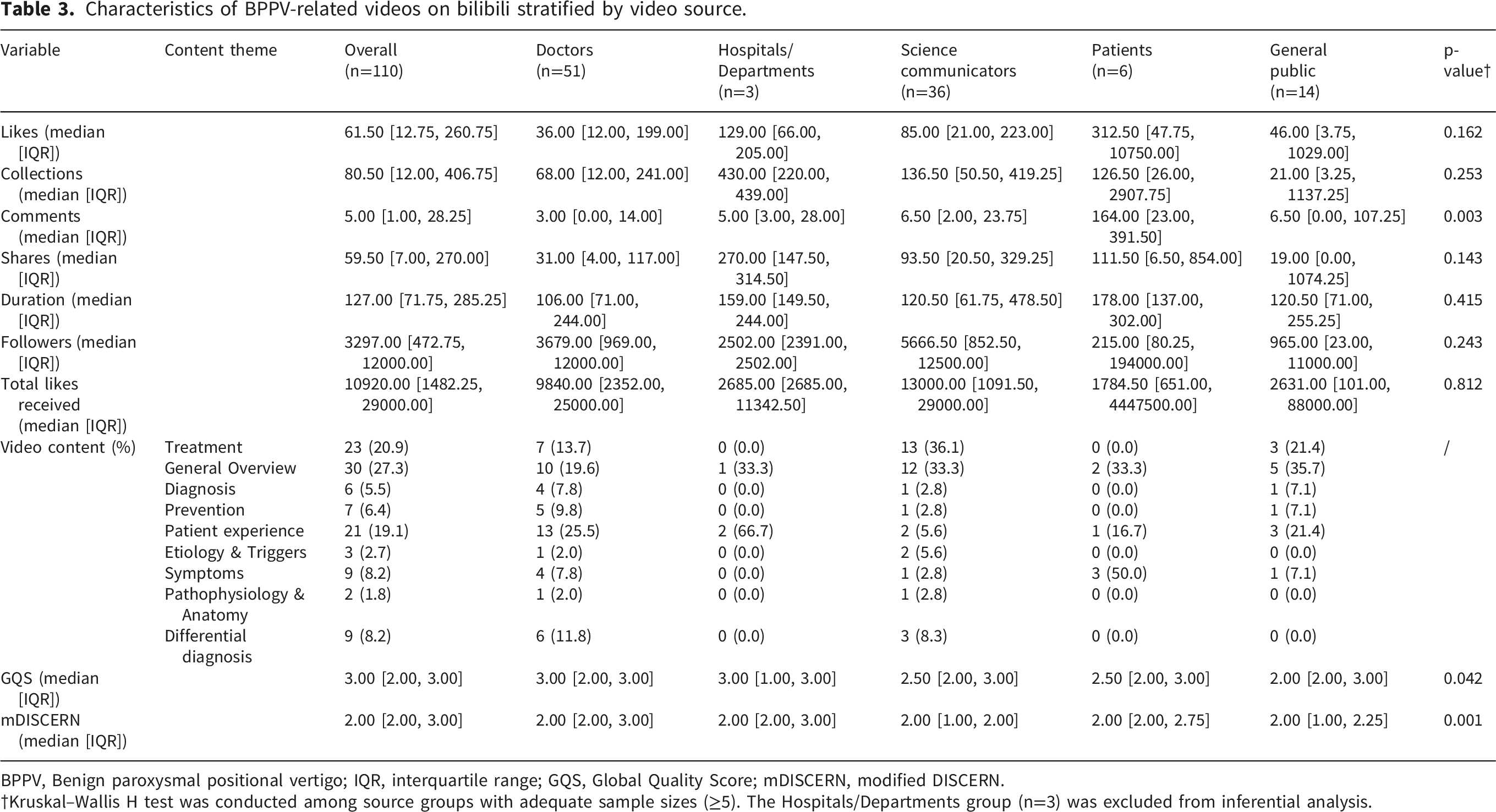
BPPV, Benign paroxysmal positional vertigo; IQR, interquartile range; GQS, Global Quality Score; mDISCERN, modified DISCERN.
†Kruskal–Wallis H test was conducted among source groups with adequate sample sizes (≥5). The Hospitals/Departments group (n=3) was excluded from inferential analysis.
Significant differences in BPPV video quality were observed across content categories on both platforms. For Douyin (P<0.001), the median GQS values for treatment, general overview, prevention, patient experience, symptoms, and differential diagnosis were 2, 3, 3, 2, 3, and 3, respectively; the corresponding median mDISCERN scores were all 2 (Supplementary Table S3). For Bilibili (P<0.05), the median GQS values were 2 for treatment, 3 for general overview, 2 for diagnosis, 3 for prevention, 3 for patient experience, 2 for symptoms, and 4 for differential diagnosis; the corresponding mDISCERN scores were 2, 3, 2, 3, 2, 3, and 3, respectively (Supplementary Table S4). Content types with fewer than 5 videos were excluded from subgroup analysis to minimize potential bias.
Association between video duration and user engagement
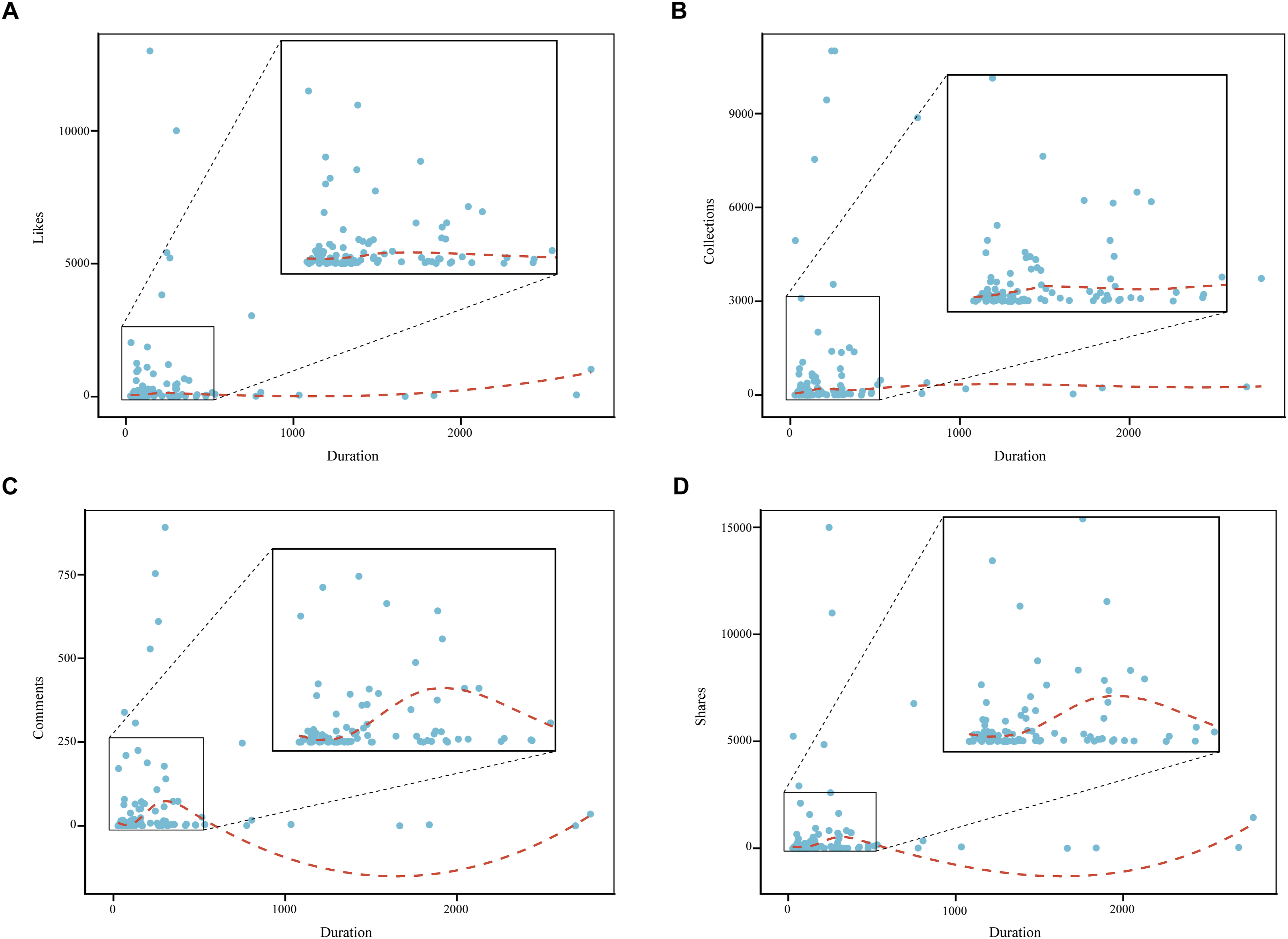
Figures 4 and 5 use smoothed curves to show the relationship between video duration (X-axis) and user engagement (likes, collections, comments, and shares; Y-axis). Association between video duration and user engagement indicators for BPPV-related videos on Douyin. (a) Likes; (b) Collections; (c) Comments; (d) Shares. Association between video duration and user engagement indicators for BPPV-related videos on Bilibili. (a) Likes; (B) Collections; (c) Comments; (d) Shares.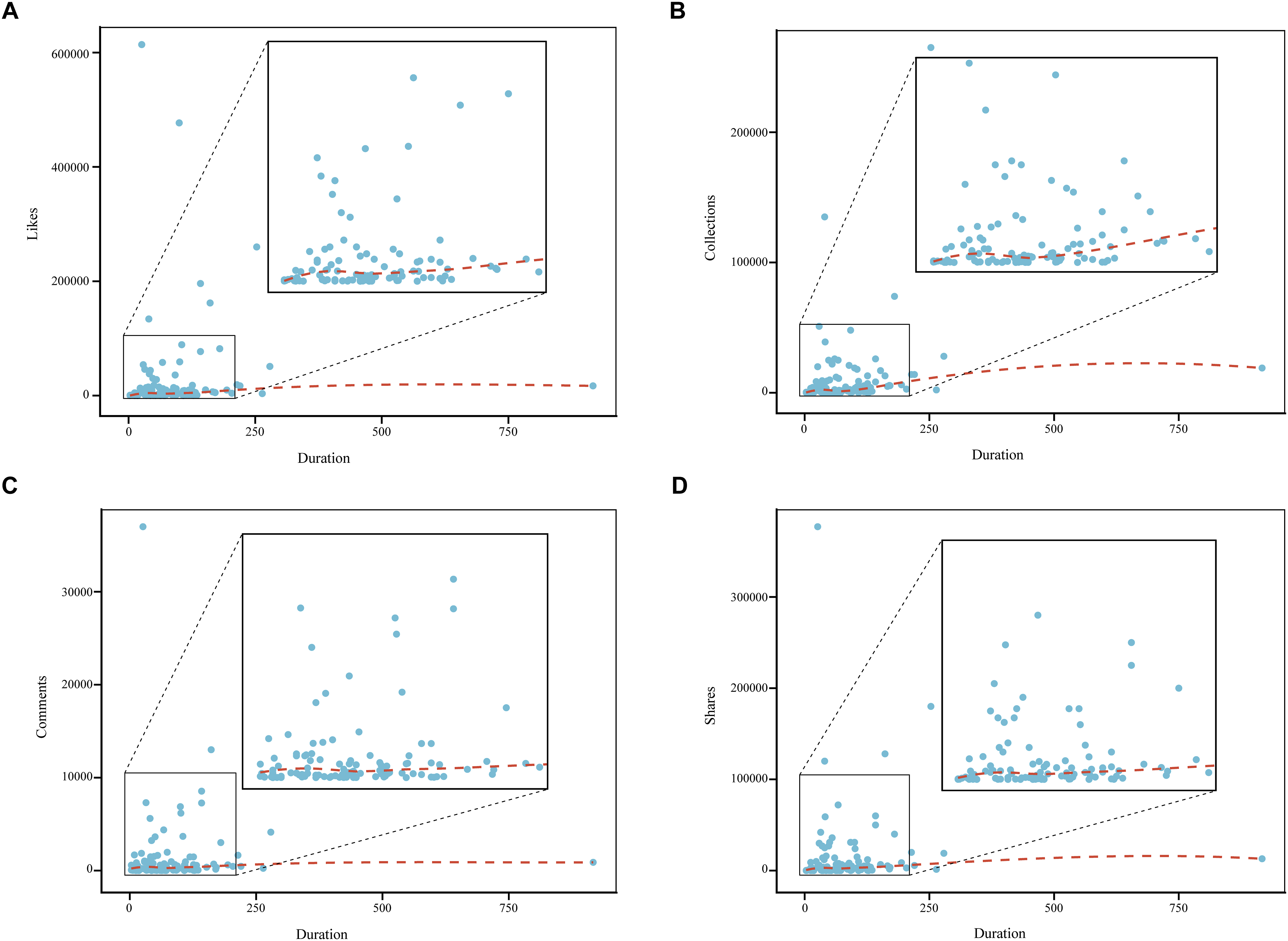
For Douyin, the curves did not show a clear pattern. Most videos were between 0 and 250 seconds long, and after removing a few extreme values, the videos with higher engagement were generally in the 60–180-second range (Figure 4).
For Bilibili, likes and collections showed a slight increase as video duration increased. Comments and shares rose within the 100–300-second range, the subsequent U-shaped pattern at longer durations reflected sparse long-duration outliers rather than genuine trends. Overall, videos lasting around 150–300 seconds appeared to achieve the highest viewer engagement (Figure 5).
Correlation analysis
As illustrated in Figure 6, engagement indicators—including likes, collections, shares, and comments—were strongly interrelated on both platforms, whereas none showed a significant correlation with either GQS or mDISCERN. The follower count was highly associated with the cumulative number of likes received, and a significant positive relationship was found between GQS and mDISCERN scores. Spearman correlation matrices showing the relationships among video characteristics and quality indicators for BPPV-related content. (a) Douyin; (b) Bilibili.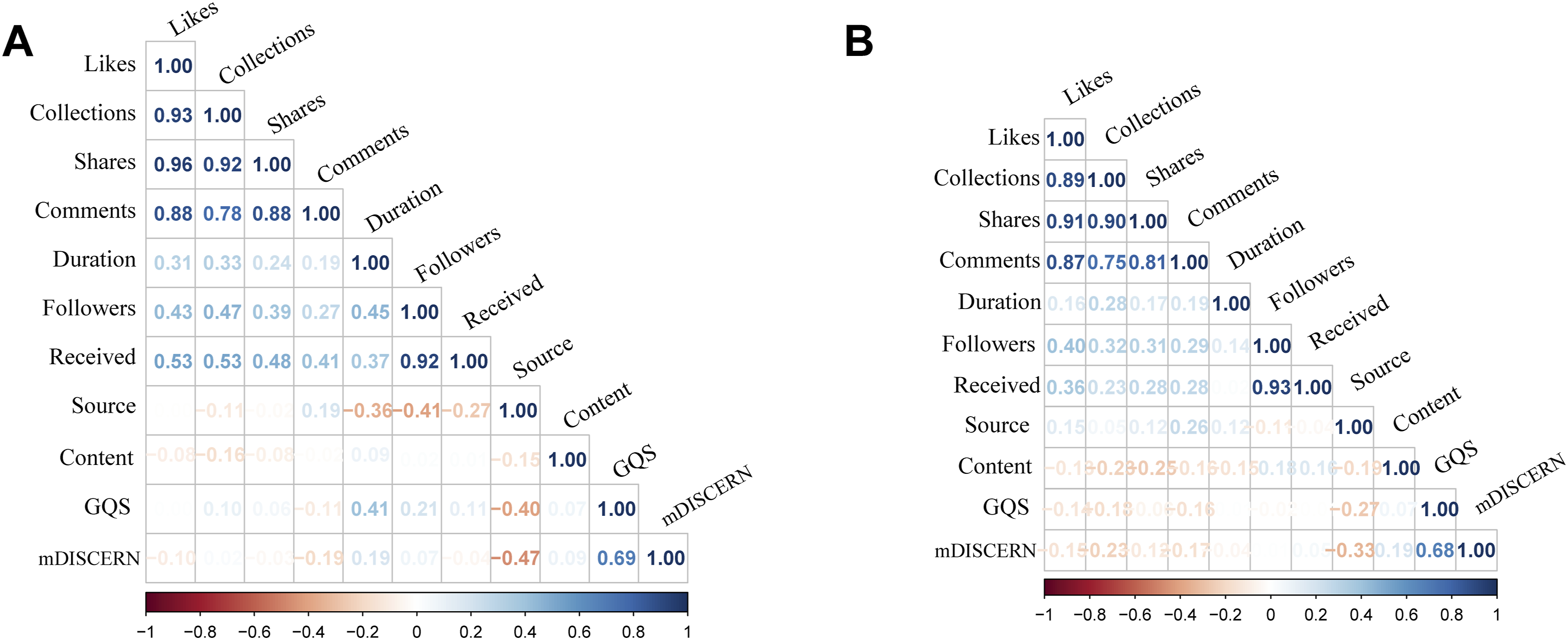
Multivariable logistic regression
Multivariable logistic regression analysis of factors associated with high-quality videos predictor.
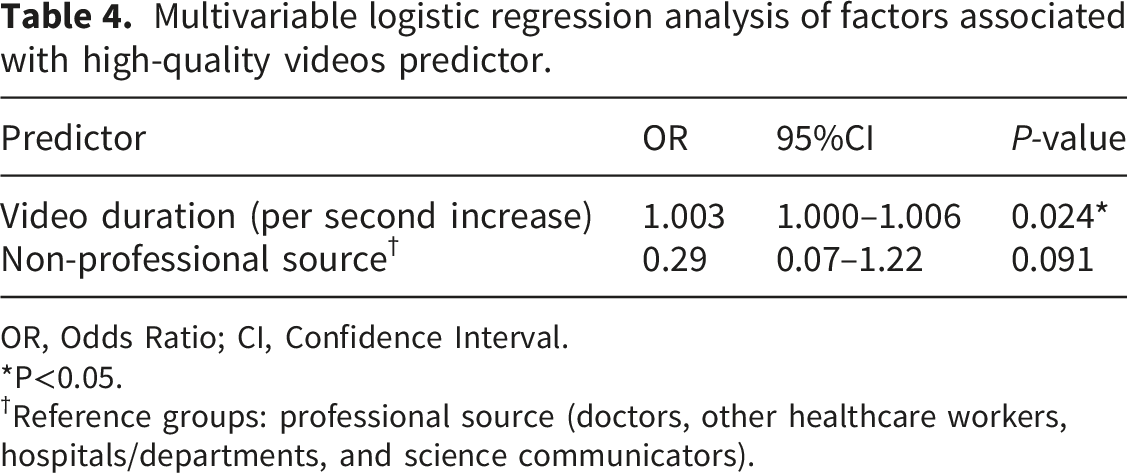
OR, Odds Ratio; CI, Confidence Interval.
*P<0.05.
†Reference groups: professional source (doctors, other healthcare workers, hospitals/departments, and science communicators).
Discussion
To our knowledge, this is the first study to evaluate the quality and reliability of BPPV-related health information on China’s two major short-video platforms, Douyin and Bilibili. Overall, both platforms were rated as fair in terms of overall quality (GQS) but less reliable according to the mDISCERN scale. Although the two scores showed strong correlation, differences in scoring criteria might have contributed to slight discrepancies in qualitative interpretation. There was no significant difference in quality or reliability between the two platforms (P > 0.05). This study fills a gap in the evaluation of BPPV-related short-video content.
These findings are consistent with prior evaluations of web-based BPPV information, which likewise report low readability and suboptimal quality. 25 Our results extend this evidence to video-based platforms, where comparable challenges persist in providing clear and reliable educational content. Such difficulties appear common to both web-based and video-based health education, likely because vestibular disorders are highly specialized conditions, and comprehension is closely tied to the audience’s education level. 13 In our study, although doctors made up the majority of uploaders (77.5% on Douyin and 46.4% on Bilibili), their GQS and mDISCERN scores were not higher than the overall average. This suggests that even healthcare professionals may struggle to produce high-quality educational content on BPPV. It also points to the need for more structured ways to improve communication about the disease. Considering these challenges, a few practical suggestions could be useful. First, video content should focus on the main questions that patients care about—for example, diagnosis, symptoms, treatment options, and when to seek medical attention. Large-scale surveys could help identify these needs more accurately. Second, technical terms should be minimized so that viewers without a medical background or with lower education levels can understand the information. Using a structured format may also help viewers follow the content more clearly.
For video content, higher-quality videos were more likely to cover General Overview, Prevention, Symptoms, or Differential Diagnosis. Among these categories, videos on general overviews and differential diagnosis tended to give more detailed explanations of BPPV. Producing this type of content usually requires more background knowledge and preparation, which may help explain why these videos scored higher. These videos give patients a broader and more complete picture of the condition, but the amount of information can also make them harder to understand. In contrast, videos that focus on prevention or symptoms cover a narrower range of content and are easier to make, but they can also oversimplify important ideas and reduce their educational value. These pieces of evidence suggest that as long as the information is clear, simpler video topics can still receive good quality ratings. Video creators need to find a balance between comprehensiveness and simplicity when improving the quality and readability of BPPV-related content. Avoiding highly technical details (anatomical/pathological mechanisms) may help audiences understand the material more easily. More research is needed to determine how to best balance comprehensiveness and simplicity.
During the evaluation of video quality and reliability, we found that the mDISCERN assessment of video content was often limited by insufficient citation of valid information sources (e.g., clinical guidelines, expert consensus statements, or authoritative websites) and by a lack of discussion on uncertain aspects of BPPV. These findings again show that video styles vary widely. This diversity adds richness, but it also highlights the lack of clear guidance. We believe that relevant institutions or platforms should develop standardized guidelines for disease-related educational videos and require creators to provide proper references. This would help improve the reliability of the content and encourage patients to verify the information on their own. Therefore, video creators should be encouraged to reference credible sources to improve information transparency and enable viewers to verify the accuracy of the presented content.
To further identify independent factors associated with video quality, a multivariable logistic regression analysis was performed. The results indicated that video duration was an independent determinant of higher quality. However, excessively long videos may discourage viewer retention, whereas overly short videos may fail to convey adequate information. User engagement can therefore serve as an indirect indicator of whether a video’s duration is appropriate. Prior studies have reported mixed findings—some showing a positive association between duration and engagement, while others suggesting that shorter videos attract greater attention.26,27 The innovation of our study lies in visualizing the fitted relationship between video duration and user engagement on both platforms, which allowed us to estimate the effective engagement time window for BPPV-related short videos. The optimal engagement durations were approximately 60–180 seconds on Douyin and 150–300 seconds on Bilibili. It should be noted, however, that these intervals are approximate and may vary depending on content characteristics, audience preferences, and platform algorithms. These ranges should be viewed as estimates rather than fixed rules, since they may shift with differences in content, audience behavior, and the platforms’ recommendation algorithms.
In addition to content and structure, the spread of health information on short-video platforms is also influenced by recommendation algorithms and viewer attention patterns. These mechanisms may amplify popular but potentially low-quality content while limiting access to more professional resources. There may also be interactions between algorithmic factors and audience behavior, and understanding these dynamics is essential for improving the accuracy of BPPV-related video dissemination. Future studies could further explore how algorithms and audience characteristics affect short-video performance and compare the quality of BPPV-related health information across multiple platforms, including globally accessible social media platforms.
This study has several limitations. First, the GQS and mDISCERN are subjective rating tools, and although we assessed interrater agreement using ICC, some degree of bias is still unavoidable. Second, as a cross-sectional study, our findings reflect only one point in time; the quality and reliability of videos and search results may change with shifts in content, platform dynamics, audience behavior, geographic location, device type, time of search, and network environment. Third, because our analysis was limited to Chinese short-video platforms, the generalizability of our conclusions may be restricted. Despite these limitations, this study provides a quantitative evaluation of the quality and reliability of BPPV-related videos on the major Chinese platforms Douyin and Bilibili. These data may serve as a practical reference for both patients and healthcare professionals.
Conclusion
The overall quality and reliability of BPPV-related health information on Douyin and Bilibili remain suboptimal. For viewers, video duration and professional source attribution appear to be key indicators of perceived quality. For content creators, several approaches may help enhance both the quality and impact of BPPV-related videos: maintaining a balance between comprehensiveness and simplicity, selecting an appropriate duration to sustain engagement, citing credible information sources, and acknowledging areas of uncertainty. Improving the quality of BPPV-related information on short-video platforms will require joint efforts from healthcare professionals, patients, platform operators, and regulatory bodies.
Supplemental material
Supplemental material - Quality and reliability of online health information on benign paroxysmal positional vertigo in TikTok and Bilibili short videos: A cross-sectional content analysis
Supplemental material for Quality and reliability of online health information on benign paroxysmal positional vertigo in TikTok and Bilibili short videos: A cross-sectional content analysis by Feng Zhu, Jing Deng, Yao Sun, Jianyun Ma, Guoqi Sima and Ru Chen in Digital Health.
Supplemental material
Supplemental material - Quality and reliability of online health information on benign paroxysmal positional vertigo in TikTok and Bilibili short videos: A cross-sectional content analysis
Supplemental material for Quality and reliability of online health information on benign paroxysmal positional vertigo in TikTok and Bilibili short videos: A cross-sectional content analysis by Feng Zhu, Jing Deng, Yao Sun, Jianyun Ma, Guoqi Sima and Ru Chen in Digital Health.
Supplemental material
Supplemental material - Quality and reliability of online health information on benign paroxysmal positional vertigo in TikTok and Bilibili short videos: A cross-sectional content analysis
Supplemental material for Quality and reliability of online health information on benign paroxysmal positional vertigo in TikTok and Bilibili short videos: A cross-sectional content analysis by Feng Zhu, Jing Deng, Yao Sun, Jianyun Ma, Guoqi Sima and Ru Chen in Digital Health.
Supplemental material
Supplemental material - Quality and reliability of online health information on benign paroxysmal positional vertigo in TikTok and Bilibili short videos: A cross-sectional content analysis
Supplemental material for Quality and reliability of online health information on benign paroxysmal positional vertigo in TikTok and Bilibili short videos: A cross-sectional content analysis by Feng Zhu, Jing Deng, Yao Sun, Jianyun Ma, Guoqi Sima and Ru Chen in Digital Health.
Footnotes
Acknowledgments
The authors thank the colleagues who contributed to data collection and analysis, and appreciate the valuable suggestions provided by peers during manuscript revision.
Ethical considerations
This study is a secondary analysis of publicly available short-video content. It involves no patient data, human specimens, animal experiments, or user interaction. No personally identifiable information was collected and results are reported in aggregate. Under our institutional policy, such public-data research is exempt from review; therefore, ethics approval and informed consent were not required.
Consent to participate
This study involved publicly available short-video content and did not include any human participants, identifiable personal information, or direct interaction with users. Therefore, informed consent was not required.
Author contributions
FZ: Conceptualization, Methodology, Data curation, Formal analysis, Visualization, Writing – original draft. JD: Data curation, Validation, Writing – review & editing. YS: Data curation, Writing – review & editing. JM: Project administration, Administrative support. GS: Conceptualization, Validation, Supervision, Writing – review & editing. RC: Conceptualization, Validation, Supervision, Writing – review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grant from the Key Support Project of Jiaxing (no. 2023-FC-004). The funder had no role in the study design, data collection, data analysis, decision to publish, or preparation of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are included in this article and its supplementary materials. Analytical materials (e.g., R packages or scripts) are available from the corresponding author upon reasonable request.
Guarantor
RC is the guarantor.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.