
Abstract
Objective
This systematic review aimed to evaluate and compare three major types of digital cognitive assessment tools—digitized traditional tests, newly developed digital tools, and digital biomarkers. It also explored their validity, feasibility, and potential integration into community-based healthcare, along with clinical utility and implementation challenges.
Methods
A search of nine electronic databases (July 2024) was conducted following PRISMA guidelines. Eligible studies included those reporting diagnostic accuracy and practical application of digital cognitive assessment tools or biomarkers. Data were narratively synthesized, and diagnostic accuracy metrics such as sensitivity, specificity, and area under the curve (AUC) were extracted. The review was prospectively registered in PROSPERO (CRD42024564512).
Results
A total of 48 studies involving older adults with or at risk of cognitive impairment were included. These studies evaluated digital cognitive tools or biomarkers and reported diagnostic performance comparison with established tests or clinical diagnosis across clinical, community, and home settings. Approaches were categorized into digitized traditional tests (AUC: 0.65–1.0), newly developed digital cognitive tools (AUC: 0.75–0.94), and digital biomarkers (AUC: 0.59–0.95). Although diagnostic accuracy was generally promising, most studies were conducted in controlled settings with limited longitudinal or real-world validation. Evidence supporting the role of community-based healthcare professionals, such as nurses, remains limited; however, self-administered and remote assessments indicate potential for future community-based implementation. Future validation in real-world, community-based settings is essential before widespread implementation.
Conclusions
Digital cognitive assessments and biomarkers offer valuable opportunities to enhance early screening and continuous monitoring of cognitive impairment. Based on these findings, we suggest that selection between digitized traditional tests and newly developed tools should be tailored to specific context, with digital biomarkers serving as complementary tools to strengthen cognitive assessment, particularly in community-based nursing practice. Policymakers and healthcare organizations should establish guidelines to safe and effective adoption of digital cognitive tools in community and clinical settings.
Keywords
Introduction
The global prevalence of dementia is increasing, with South Korea alone recording nearly 890,000 dementia patients aged 65 years and older in 2021, an increase of nearly 50,000 cases per year. 1 Dementia not only impacts cognitive and functional abilities but also imposes significant economic and psychological burdens on families and healthcare systems. Early detection plays a critical role in slowing dementia progression and improving patient outcomes, demanding convenient and effective methods of cognitive testing. 2
Historical neuropsychological measures including the Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA) have served as the gold standard for cognitive screening. 3 These tests, however, need expert clinicians, are time-consuming, and are often insensitive to early symptoms of cognitive decline.4,5 Moreover, the suboptimal uptake of screening tests reported above in national dementia screening programs (only 16.6% of eligible individuals underwent screening through public health centers in 2015 6 ) suggests the necessity of improving access to cognitive assessments and increasing their usability to populations.
Several systematic reviews have previously examined digital cognitive assessments, focusing mainly on specific modalities such as mobile-based or AI-assisted tools.7,8 However, few have integrated a comparative evaluation across digitized traditional tests, newly developed digital tools, and digital biomarkers. The present review addresses this gap by synthesizing and contrasting these three categories to provide a comprehensive overview of current evidence.
Traditional neuropsychological tests, although used as a popular standard screening tool, pose a number of concerns in community settings. These evaluations usually involve trained specialists, are time-intensive, and may not be accessible to seniors with limited mobility or geographical barriers.2,4,5 It is also the case that their sensitivity to more modest/early-stage cognitive deterioration is restricted, particularly when administered as single time-point assessments.9,10 Prior systematic reviews investigated digital cognitive assessment tools that typically focused on particular modalities, including mobile-based applications and artificial intelligence-enabled systems.7,8 But these reviews also have missed combining different categories of digital approaches and have lacked the assessment of diagnostic accuracy and of whether/when it is feasible in the real-world. This underscores a major gap in the literature, especially for the use of these tools in community healthcare environments. Digital biomarkers, defined as objective and quantifiable physiological and behavioral data obtained via digital devices, are considered an important complement to traditional cognitive evaluations.11,12 They are clinically relevant because they capture continuous, real-life data, allowing for the early detection of subtle cognitive changes not detected using traditional tests. 13 Such advantages make digital biomarkers an effective tool for improving early screening and long-time monitoring of cognitive outcomes.
Digital cognitive assessment tools have emerged as promising alternatives to address the limitations of traditional methods. These tools utilize mobile applications, artificial intelligence (AI)-assisted scoring, and adaptive testing to provide automated, scalable, and precise cognitive evaluations.14,15 Moreover, self-administered remote-testing methods improve accessibility, particularly for older adults in community settings where medical resources are limited. 16 In addition to these digital cognitive assessment tools, digital biomarkers are defined as objective, quantifiable physiological and behavioral data collected through digital devices such as smartphones, wearable sensors, and computer-based platforms.11,12 In the context of cognitive assessment, these biomarkers enable the detection of subtle changes in cognitive function through real-world interactions and passive data collection. For example, studies included in this review have shown that speech and language features, such as pauses and semantic complexity, can serve as early indicators of cognitive decline.17,18 In addition, motor and behavioral patterns, including gait characteristics such as turn velocity and stride length, have demonstrated predictive value for cognitive impairment. 19 Activity-based monitoring using smart home environments has also been effective in identifying changes in daily living patterns associated with cognitive decline. 20 These characteristics highlight the potential of digital biomarkers for continuous, non-invasive, and ecologically valid monitoring of cognitive function in real-world settings. Traditional neuropsychological assessments are limited by being time-consuming, requiring trained personnel, and lacking scalability, reinforcing the need for innovative digital approaches.2,4,5 Recent evidence indicates that AI-driven multimodal biomarkers achieve higher sensitivity than conventional cognitive screening tools for early Alzheimer’s detection. AI-driven multimodal biomarkers have shown superior performance for early Alzheimer’s detection compared with conventional cognitive test. 21
In this review, traditional neuropsychological tests refer to paper-based cognitive assessments that have been digitized with minimal procedural modification. Digital cognitive assessment tools denote newly developed computerized or mobile-based instruments designed to measure cognitive functions through novel interfaces. Digital biomarkers, in contrast, involve passive or active data derived from sensors, wearables, or device interactions that serve as indirect indicators of cognitive function.
Recent studies have expanded the scope of digital assessments using AI and multimodal data integration, demonstrating improved predictive validity for early Alzheimer’s detection.22,23 Furthermore, updated systematic reviews highlight the growing importance of digital biomarkers in community-based cognitive health monitoring. 24 Despite these advances, several challenges remain regarding the implementation of digital cognitive assessments in real-world settings. Score discrepancies between digital- and paper-based tests, variations in digital literacy among older adults, and the need for standardized scoring frameworks must be addressed to ensure reliability. 25 Although digital cognitive assessments and biomarkers hold promise, their practical feasibility and effectiveness in community healthcare settings require further evaluation.
Community nurses play a critical role in bridging this accessibility gap by incorporating digital cognitive assessments into routine home visits and community health programs. However, visiting nursing services face structural and operational challenges, including limited resources, administrative burdens, and role ambiguity.26,27 To enhance early detection and intervention, an integrated community-based cognitive function-monitoring system that leverages digital cognitive assessment and biomarkers should be developed.
This systematic review aims to evaluate and compare different types of digital cognitive assessment tools and examine their validity, feasibility, and potential integration into community-based healthcare. Specifically, this review assessed (a) the validity of digital adaptations of traditional neuropsychological tests, (b) the advantages and limitations of newly developed digital cognitive assessment tools, and (c) the emerging role of digital biomarkers in cognitive function monitoring.
Although previous studies have explored digital approaches for cognitive assessment, existing systematic reviews have often focused on specific tools or technologies without comprehensively integrating multiple domains, such as digitized neuropsychological tests, newly developed digital tools, and digital biomarkers.15,16 In addition, limited attention has been given to the combined evaluation of diagnostic accuracy and practical feasibility, particularly in community-based settings. Therefore, a more integrative and practice-oriented review is needed.
Methods
This systematic review was conducted and reported in accordance with the PRISMA 2020 guidelines and was prospectively registered in the PROSPERO database (registration number: CRD42024564512). In addition, the PRISMA checklist has been included as an appendix to enhance methodological transparency and reproducibility.
The research question was developed using the PICOS framework, including Population (older adults with or at risk of cognitive impairment), Intervention (digital cognitive assessment tools and digital biomarkers), Comparator (traditional cognitive tests or clinical diagnosis), Outcomes (diagnostic accuracy and feasibility), and Study design (observational and diagnostic accuracy studies).
The data search was conducted over a period of five days, from July 24, 2024 to July 29, 2024. An updated literature search was conducted in March and April 2026 using the same databases and search strategy to identify any newly published studies. No additional studies met the inclusion criteria for this review. A comprehensive search was conducted across nine electronic databases, including MEDLINE, Embase, Cochrane Library, CINAHL, PsycINFO, RISS, KISS, KMbase, and KoreaMed. The search strategies combined controlled vocabulary and relevant keywords related to cognitive impairment (such as “dementia,” “mild cognitive impairment,” and “cognitive dysfunction”), cognitive assessments (such as “neuropsychological tests” and “cognitive screening”), and digital technologies (such as “digital health,” “mobile applications,” and “digital biomarkers”). The search strategy combined controlled vocabulary (e.g., MeSH terms such as “Cognitive Dysfunction” and “Dementia”) and free-text keywords (e.g., cognitive, dysfunction, impairment, Alzheimer*), using Boolean operators (AND, OR) to ensure comprehensive retrieval across multiple fields.
Most of the included studies were cross-sectional in design. Longitudinal or interventional studies were not included, as the primary objective of this review was to examine the validity and applicability of digital cognitive screening tools rather than intervention effects or longitudinal change trajectories. This criterion was defined a priori to ensure transparency in study design selection.
Eligibility criteria and selection procedure
This systematic review included studies that evaluated digital cognitive assessment tools for older adults with a focus on their validity and applicability. The inclusion criteria were as follows: (a) studies involving older adults, including those with mixed-age samples where older participants were the primary focus; (b) studies using digital cognitive assessment tools; and (c) studies that assessed diagnostic performance for identifying cognitive impairment. Review articles, study protocols, nonhuman studies, and studies unrelated to cognitive assessment were excluded.
However, direct evidence for nurse-led or community-based implementation of these tools remains limited. Self-administered and remote monitoring options have demonstrated growing feasibility, offering valuable opportunities for continuous cognitive screening in community-dwelling older adults. Future research should prioritize usability testing among older adults, training programs for nurses, and the acceptability of digital devices among healthcare professionals.
All retrieved studies were reviewed according to the predefined selection and exclusion criteria, and duplicate studies were removed using a bibliographic management program (EndNote 20). After removing duplicate literature in the first round of selection and exclusion, we excluded literature unrelated to the research topic by looking at the title and abstract. If it was difficult to judge whether a study was suitable for selection, the full manuscript text was reviewed. In the second selection/exclusion process, the full text of the literature selected in the first step was reviewed, and literature suitable for the research topic of this study was selected. Two researchers independently evaluated the literature search and selection processes. If the opinions of the researchers were not in agreement for literature selection, a consensus was reached through discussion.
Data extraction
We extracted data regarding the characteristics of the included studies (such as study design, sample size, and participant demographics), intervention details (including the type of digital cognitive assessment and setting), and outcomes of interest.
The primary outcomes of interest included measures of diagnostic validity, such as sensitivity, specificity, and area under the curve (AUC). In addition, extracted data included the statistical associations with traditional cognitive tests, such as correlation coefficients and score differences between digital and conventional assessments. Furthermore, information related to feasibility of the tools was collected, including self-administration formats and the general utility rates.
Study risk of bias assessment
Due to methodological heterogeneity, only a narrative synthesis was conducted rather than a meta-analysis.
The risk of bias was assessed using the Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) tool for studies that evaluated outcomes related to diagnostic accuracy. Two reviewers independently evaluated each study across the following four domains: patient selection, index test, reference standard, and flow and timing. Discrepancies were resolved by discussion or consultation with a third reviewer. Data extraction and quality appraisal were independently performed by two reviewers to ensure consistency and reduce bias. Discrepancies were resolved through discussion and consensus, with inter-rater agreement assessed using Cohen’s kappa coefficient to confirm reliability of the review process.
Synthesis method
We conducted a narrative synthesis owing to heterogeneity in study designs, participant characteristics, assessment tools, and reported outcomes. The studies were grouped into three categories based on the type of digital cognitive assessment tool used: (a) digital adaptations of traditional neuropsychological tests; (b) newly developed digital cognitive assessments; and (c) cognitive assessments using digital biomarkers. The first category included studies that digitized well-established neuropsychological tests. The second category comprised newly developed digital assessments that are not direct digital versions of traditional tests. The third category included studies that used digital biomarkers to assess cognitive function in a continuous and unobtrusive manner.
Within each category, the key findings related to diagnostic performance, feasibility, and unique technological features were summarized. Results are presented in descriptive tables and synthesized narratively to highlight similarities, differences, and notable trends across studies.
Results
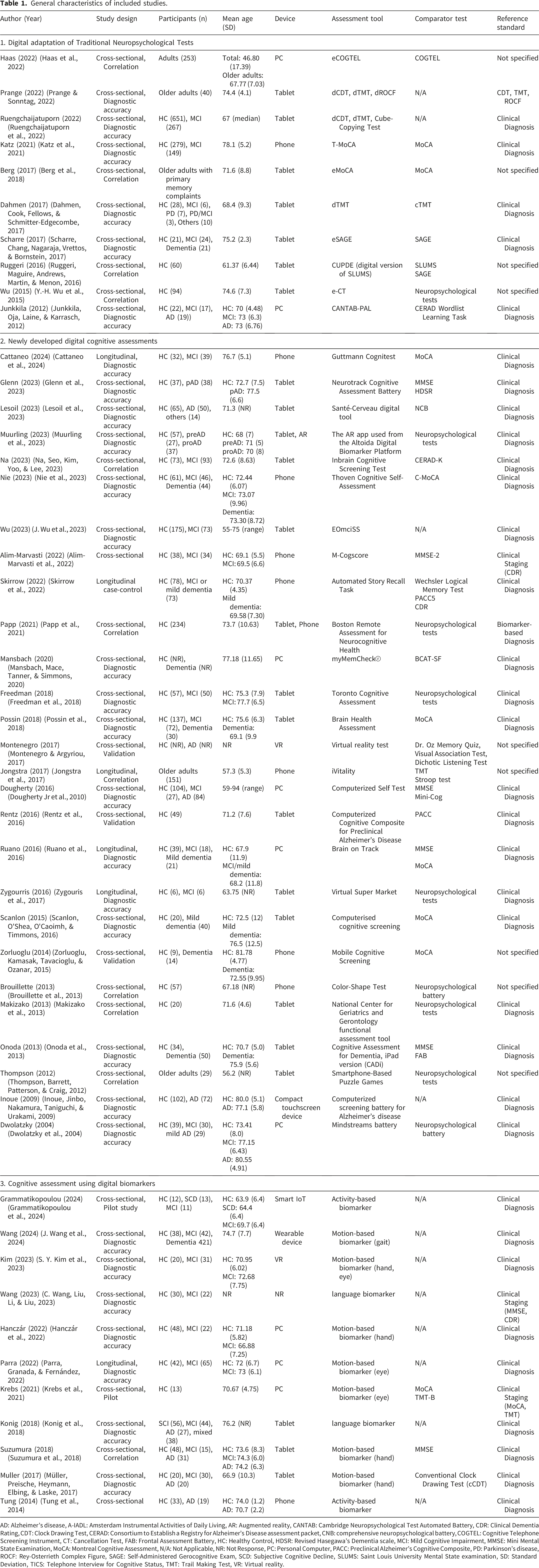
A total of 48 studies examining various digital cognitive assessment tools for older adults were included in this systematic review (Figure 1). The general characteristics of the included studies are summarized in Table 1. The included studies were published between 2004 and 2024, with the majority employing a cross-sectional design (n=42) and a few (n=6) following a longitudinal approach. The sample sizes varied significantly, ranging from as few as 13 participants in pilot studies to over 900 participants in large-scale studies. The mean age of participants for each study was in the older adult range, with most studies focusing on individuals aged 60 and above, although some included younger adults for comparison. The participants were categorized into different cognitive status groups: healthy controls (HC), mild cognitive impairment (MCI), and dementia. Some studies further classified individuals into preclinical cognitive decline stages or specific conditions, such as subjective cognitive decline (SCD) and Parkinson’s disease (PD)-related cognitive impairment. Most studies were conducted in high-income countries with limited representation of diverse ethnic or socioeconomic groups. Flow chart of the study selection process. General characteristics of included studies. AD: Alzheimer’s disease, A-IADL: Amsterdam Instrumental Activities of Daily Living, AR: Augmented reality, CANTAB: Cambridge Neuropsychological Test Automated Battery, CDR: Clinical Dementia Rating, CDT: Clock Drawing Test, CERAD: Consortium to Establish a Registry for Alzheimer’s Disease assessment packet, CNB: comprehensive neuropsychological battery, COGTEL: Cognitive Telephone Screening Instrument, CT: Cancellation Test, FAB: Frontal Assessment Battery, HC: Healthy Control, HDSR: Revised Hasegawa’s Dementia scale, MCI: Mild Cognitive Impairment, MMSE: Mini Mental State Examination, MoCA: Montreal Cognitive Assessment, N/A: Not Applicable, NR: Not Response, PC: Personal Computer, PACC: Preclinical Alzheimer’s Cognitive Composite, PD: Parkinson’s disease, ROCF: Rey-Osterrieth Complex Figure, SAGE: Self-Administered Gerocognitive Exam, SCD: Subjective Cognitive Decline, SLUMS: Saint Louis University Mental State examination, SD: Standard Deviation, TICS: Telephone Interview for Cognitive Status, TMT: Trail Making Test, VR: Virtual reality.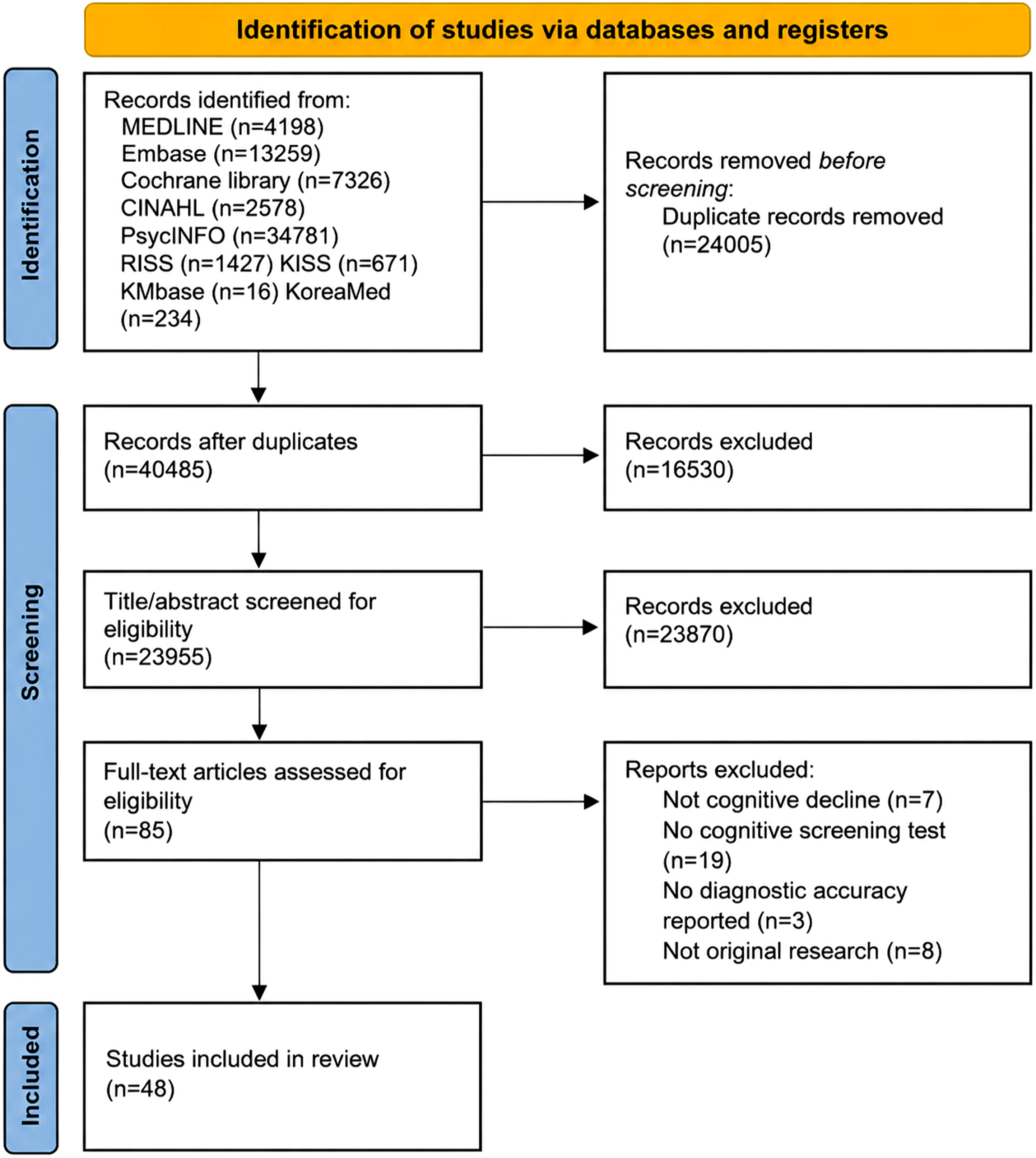
Tablets were the most frequently used devices for cognitive assessments, followed by smartphones and computers. Some studies also incorporated immersive technologies such as virtual reality (VR), augmented reality (AR), or wearable devices to facilitate real-time or continuous cognitive monitoring. In terms of validation, most studies relied on clinical diagnoses established through expert evaluation or standardized diagnostic criteria as the primary reference standard. In addition, many studies compared digital assessments to widely accepted cognitive screening tools such as the MoCA, MMSE, and the Consortium to Establish a Registry for Alzheimer’s Disease Neuropsychological Assessment Battery (CERAD-NAB) to assess their diagnostic accuracy.
1. Digital adaptation of traditional neuropsychological tests
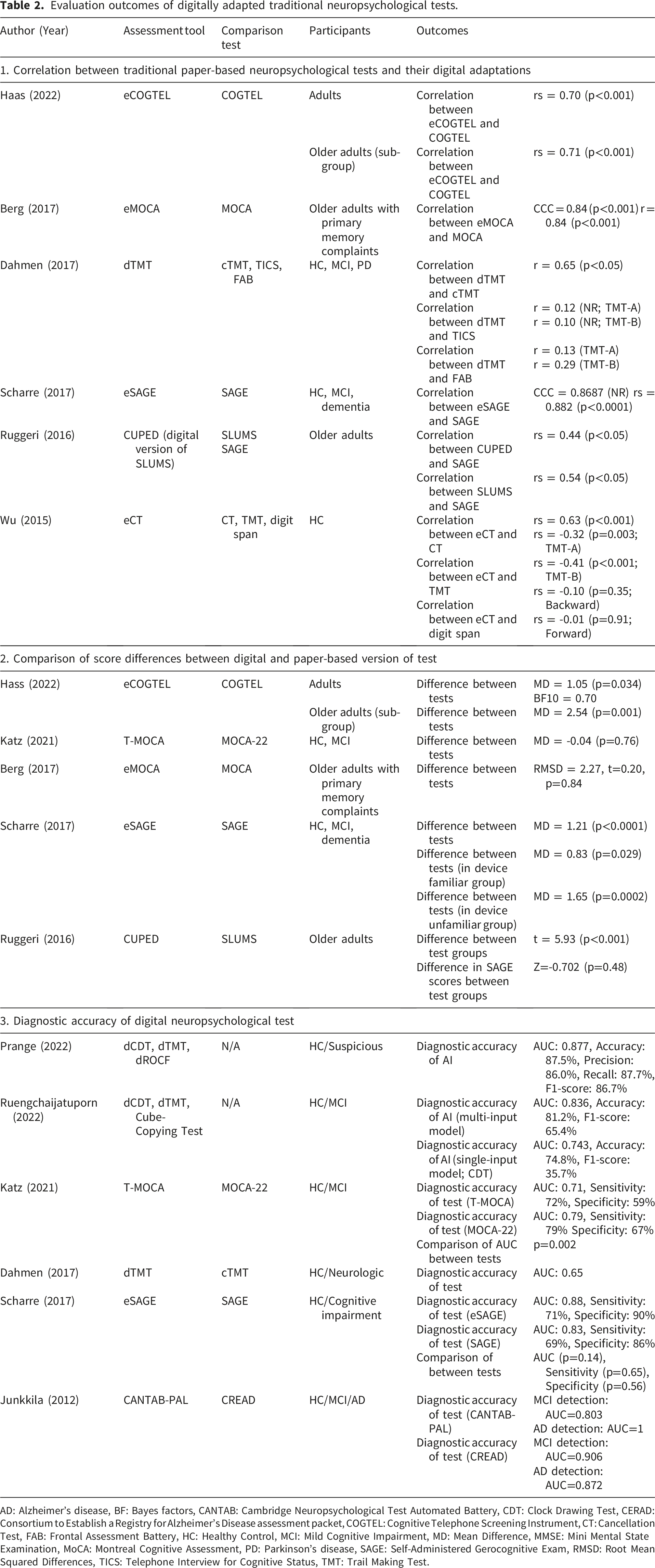
Evaluation outcomes of digitally adapted traditional neuropsychological tests.
AD: Alzheimer’s disease, BF: Bayes factors, CANTAB: Cambridge Neuropsychological Test Automated Battery, CDT: Clock Drawing Test, CERAD: Consortium to Establish a Registry for Alzheimer’s Disease assessment packet, COGTEL: Cognitive Telephone Screening Instrument, CT: Cancellation Test, FAB: Frontal Assessment Battery, HC: Healthy Control, MCI: Mild Cognitive Impairment, MD: Mean Difference, MMSE: Mini Mental State Examination, MoCA: Montreal Cognitive Assessment, PD: Parkinson’s disease, SAGE: Self-Administered Gerocognitive Exam, RMSD: Root Mean Squared Differences, TICS: Telephone Interview for Cognitive Status, TMT: Trail Making Test.
1.1. Correlation between traditional paper-based neuropsychological tests and their digital adaptations
Six studies examined the correlations between traditional paper-based neuropsychological tests and digital adaptation.25,28–32 Among these, five specifically assessed the direct correlation between the same tests in both formats. The studies reported either Pearson’s or Spearman’s correlation coefficients ranging from 0.63 to 0.84. Additionally, some studies investigated the correlation between digital cognitive tests and other traditional assessments.29,32 The correlations between digital TMT and TICS (Telephone Interview for Cognitive Status), as well as FAB (Frontal Assessment Battery), ranged from 0.10 to 0.29, reflecting a weak correlation. 29 Another study 32 examined the relationship between eCT and both the TMT and Digit span tests, showing a moderate association for eCT-TMT, whereas the correlation with Digit span remained weak.
1.2. Comparison of score differences between digital and paper-based version of test
Five studies compared the score differences between the digital and paper-based versions of the cognitive assessments.25,28,30,31,33 However, the findings were heterogeneous, with three studies reporting significant differences between the two versions, and two studies reporting no meaningful differences.
Regarding additional analyses, one study categorized the participants into familiar and unfamiliar groups based on their level of device familiarity. 30 Although the difference between the groups was not statistically significant, the mean difference (MD) was 0.82. Another study conducted additional analyses focusing on older adults. 25 Although the overall mean difference between the eCOGTEL and COGTEL scores was 1.05, this difference was more pronounced in the older adult subgroup, in which the MD increased to 2.54.
1.3. Diagnostic accuracy of digital neuropsychological test
Six studies evaluated the diagnostic accuracy of neuropsychological tests.29,30,33–36 Among these, four studies focused on the diagnostic performance of the tests themselves, while two assessed the diagnostic accuracy of AI models using these neuropsychological tests. AI-related studies were published in 2022, whereas test-based studies were conducted between 2017 and 2021. Four studies investigated the distinction between healthy controls and patients with MCI, whereas three studies classified between healthy controls and individuals with suspected cognitive impairment.
Across all studies, the AUC values ranged from 0.65 to 1, indicating moderate to high diagnostic accuracy. The sensitivity ranged from 62.5% to 87.5%, whereas the specificity varied from 59% to 90%. Of the two studies that assessed both digital and traditional tests, one reported that the AUC for the digital test was not significantly different from that of the traditional test (Ref. 30, p = 0.14). In contrast, one study reported superior diagnostic accuracy for the traditional paper-based version. 33 Notably, one study compared the diagnostic performance of multi-input and single-input AI models. 35 The multi-input AI model, using data from three neuropsychological tests, outperformed the single-input model, which relied on only one test across all metrics.
2. Newly developed digital cognitive assessments
Diagnostic accuracy and features of newly developed digital cognitive assessment tools.

AD: Alzheimer’s disease, AUC: Area Under the Curve, AR: Augmented reality, HC: Healthy Control, MCI: Mild Cognitive Impairment, N/A: Not Applicable.
Most newly developed digital cognitive assessments reported diagnostic performance metrics with AUC values ranging from 0.75 to 0.94. Sensitivity ranged from 54% to 100%, while specificity varied from 60% to 100%, indicating a generally high, but variable, accuracy across different studies. Several studies explored the association between digital test scores and conventional cognitive measures. Reported correlation coefficients with established tools such as MoCA, MMSE, and PACC (Preclinical Alzheimer’s Cognitive Composite) ranged from 0.39 to 0.84 (p < 0.05), depending on the statistical method used.
Many of the newly developed digital assessments incorporated distinctive technological features to enhance usability, adaptability, and diagnostic precision. Of the 27 tools reviewed, 18 were designed for self-administration, enabling older adults to complete the assessments independently, often at home. Automated scoring was incorporated into 13 tools, with some offering provider feedback to facilitate the timely interpretation of results. Five tools featured adaptive testing or parallel versions to minimize effects of test practice. Reaction times and other digital biomarkers were integrated into three tools, highlighting their potential to capture subtle performance variations.
Cognitive domain analysis revealed that most newly developed digital cognitive assessments emphasize memory, often in combination with executive function and attention evaluation. Several assessments integrated executive function, attention, and processing speed, highlighting a shift toward broader cognitive profiling. A few tools incorporated reaction time-based tasks or complex cognitive processing paradigms. Thirteen of the 27 assessments adopted composite scores that integrated multiple domains.
3. Cognitive assessment using digital biomarkers
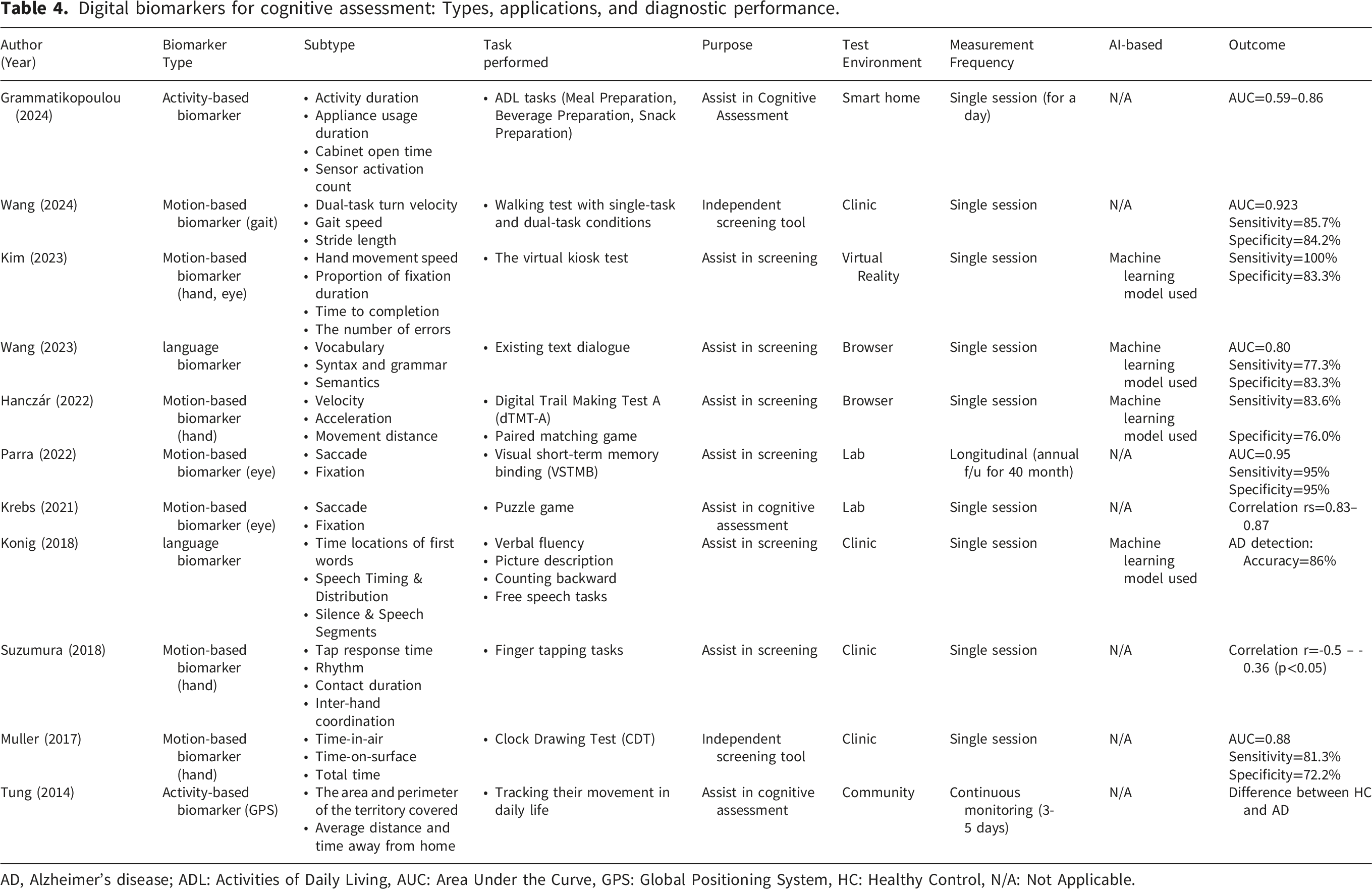
Digital biomarkers for cognitive assessment: Types, applications, and diagnostic performance.
AD, Alzheimer’s disease; ADL: Activities of Daily Living, AUC: Area Under the Curve, GPS: Global Positioning System, HC: Healthy Control, N/A: Not Applicable.
3.1. Motion-based digital biomarkers
Motion-based biomarkers were the most commonly studied and included gait, hand-movement, and eye-movement metrics. Assessment of gait parameters, such as turn velocity and stride length, demonstrated strong predictive accuracy for cognitive decline ( 19 ; AUC=0.923). Similarly, hand movements observed during neuropsychological tests, including virtual or digital assessments, demonstrated acceptable accuracy in distinguishing cognitive impairment ( 64 ; AUC=0.88) and significant negative correlations with MMSE scores ( 63 ; r=-0.50 to-0.36, p<0.05). Eye movement biomarkers, characterized by saccades and fixation, were assessed through puzzle and visual memory binding tasks using longitudinal designs ( 66 ; AUC=0.95).
3.2. Language digital biomarkers
Language biomarkers, such as syntax and semantic complexity analysis in speech (17,18), have been explored for cognitive impairment screening (AUC=0.80, Alzheimer’s disease detection accuracy 86%). A study has applied machine learning models to analyze language features and reported high accuracy in distinguishing cognitively impaired individuals from HC. 18
3.3. Active-based digital biomarkers
Activity-based biomarkers included the assessment of daily living tasks and GPS (Global Positioning System) tracking. Smart home monitoring studies 20 utilized sensor-based tracking of household activities. This approach demonstrated moderate to high accuracy in detecting cognitive impairment, with AUC values ranging from 0.59 to 0.86 across different ADL (Activities of Daily Living) tasks. Other studies 65 monitored spatial movement patterns in community settings over multiple days.
Risk of bias assessment
Study quality assessment using QUADAS-2.
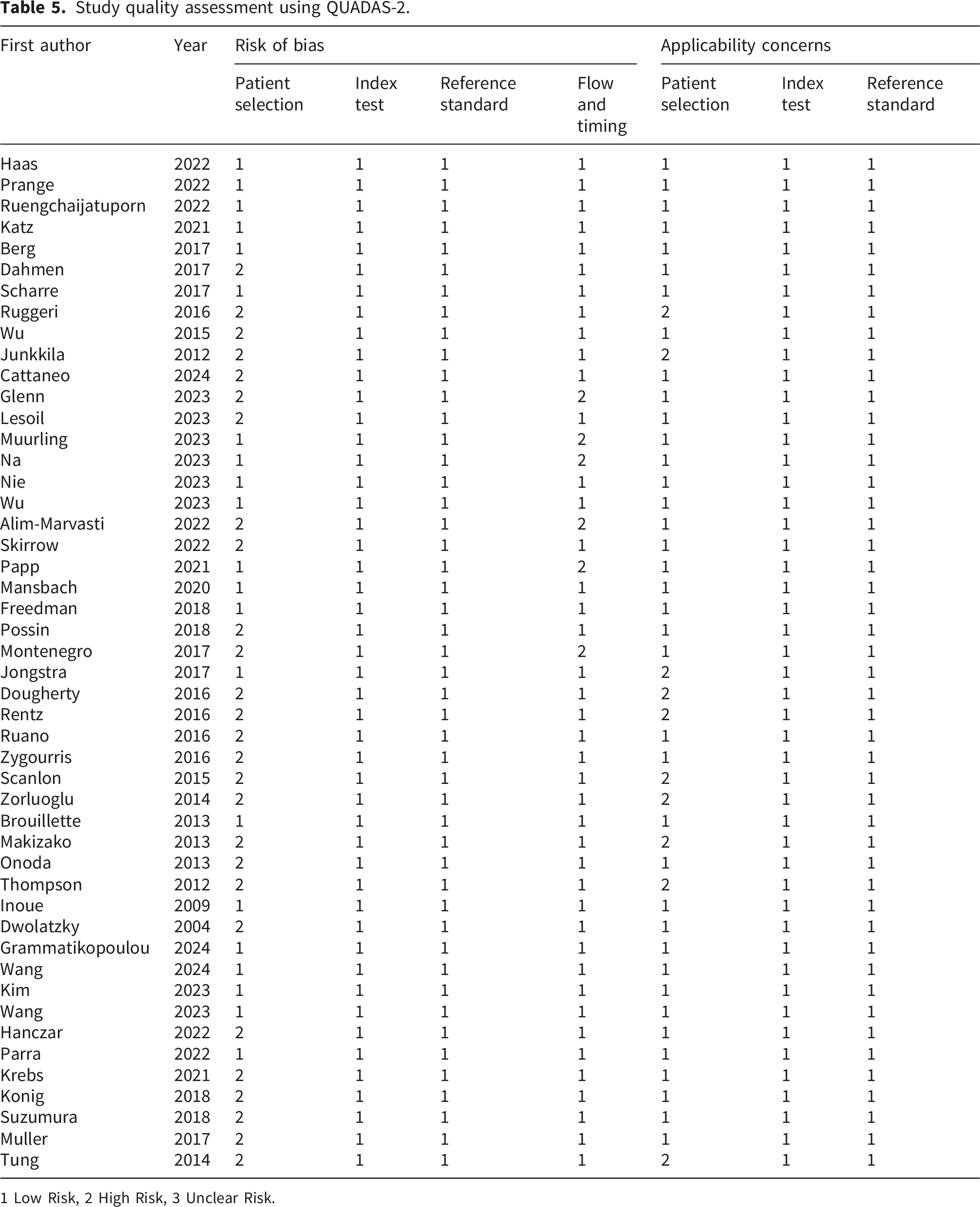
1 Low Risk, 2 High Risk, 3 Unclear Risk.
Discussion
With the increasing adoption of digital cognitive assessment tools, nursing professionals face critical decisions regarding their implementation. Available options include relying on digital adaptations of traditional neuropsychological tests, adopting newly developed digital tools, and integrating cognitive assessments with digital biomarkers. This systematic review evaluated the reliability and applicability of these three approaches and provides foundational insights into the implementation of digital cognitive assessment tools in nursing practice and community-based settings. Specifically, this review aims to support nurses in integrating these tools into clinical practice and community healthcare to ensure effective and accurate cognitive assessments in older adults.
The validity and limitations of digital adaptations of traditional neuropsychological tests
Our systematic review suggests that the digital adaptations of neuropsychological tests maintain a strong correlation with their traditional paper-based counterparts, indicating that digital platforms can reliably replicate core cognitive assessments. Specifically, correlation coefficients ranging from 0.63 to 0.84 confirm the robustness of these digital adaptations. In addition, the diagnostic accuracy of digital neuropsychological tests, as reflected by AUC values ranging from 0.65 to 1.0, further supports their effectiveness in distinguishing between healthy individuals and those with cognitive impairment. Similar findings have been reported in previous studies, with the digital CDT (AUC = 0.87; 67 ) and visual cognitive assessment test (AUC = 0.77; 68 ) demonstrating promising diagnostic accuracy for detecting cognitive impairment. This suggests that digital assessments can serve as viable alternatives to traditional methods, particularly for large-scale screening and remote-testing settings.
However, the differences in scores between the digital and paper-based tests were inconsistent. This highlights the importance of considering various contextual factors when developing digital assessments and suggests that new evaluation standards tailored to digital formats may be necessary. One key factor contributing to this variability is the influence of participant demographics and technological experience. For instance, one study found that individuals unfamiliar with digital devices scored lower on the digital version, with a mean difference of 0.82, although this difference was not statistically significant. 30 Another study focusing on older adults found a larger score discrepancy (MD = 2.54) than the general sample (MD = 1.05; 25 ), suggesting that age-related factors, including digital literacy, motor function, and cognitive adaptability, may disproportionately affect older individuals’ performance on digital tests. This observation aligns with the findings of a previous scoping review, which also emphasized that participant characteristics such as age, education, and prior technology experience can significantly impact performance on mobile cognitive assessments. 7
Considering these discrepancies, several studies have proposed score adjustments to better align digital test scores with traditional assessments.28,30 One approach suggests that applying a 1-point correction to digital test scores may improve comparability. This underscores the critical need to develop new scoring standards and algorithms specifically tailored for digital cognitive assessments rather than directly applying the criteria and benchmarks used for paper-based versions. Thus, while nurses can choose to implement digital adaptations of traditional neuropsychological tests, given their strong correlation and diagnostic accuracy, it is essential to establish appropriate scoring frameworks that ensure valid and reliable assessments in digital formats.
The advantages and challenges of newly developed digital cognitive assessment tools
Newly developed digital cognitive assessments for older adults provide alternatives to traditional neuropsychological tests by enhancing accessibility, reducing the need for professional oversight, and incorporating broader cognitive domains. Consequently, digital assessments may be more suitable for nursing and community-based cognitive screening initiatives. Many newly developed digital cognitive tools offer self-administered testing with automatic scoring and AI-assisted preliminary diagnoses, thereby significantly reducing the need for professional oversight during the early stages of assessment. Moreover, the integration of adaptive testing strengthens the applicability of these tools in nursing practice by tailoring assessments to individual performance levels in real time. This shift enhances accessibility and allows more widespread use in community healthcare settings, including nursing-led initiatives.
In addition to their accessibility, these new digital assessments demonstrate strong diagnostic accuracy. The reported AUC values for these tools range from 0.75 to 0.94, indicating their effectiveness in distinguishing between healthy individuals and those with cognitive impairments. Traditional neuropsychological assessments, including digitized versions, maintain high diagnostic reliability, with previously reported AUC values of 0.65–1.0, supporting their continued relevance alongside newer tools. Compared with previous reviews reporting variable diagnostic accuracy for remote cognitive assessments (sensitivity, 26–100%; specificity, 58–100%; 8 ), the current review included studies with higher sensitivity and specificity (sensitivity = 54-100%, specificity = 60-100%). This improvement may reflect recent technological advancements that enable more stable and user-friendly digital environments, such as tablet- and smartphone-based applications. Enhanced interface design and improved processing capabilities are likely to contribute to minimizing technical limitations and optimizing test performance.
Digital cognitive assessments introduce additional advantages that improve the flexibility and precision of cognitive evaluations. Adaptive testing is a key innovation that dynamically adjusts task difficulty based on individual performance, leading to a more tailored assessment. Although only a few tools currently employ adaptive approaches 14,15,59 this method holds promise for improving the sensitivity to mild cognitive deficits, particularly in populations with diverse baseline measurements. Additionally, digital platforms mitigate common issues associated with traditional assessments, such as practice effects, in which repeated exposure leads to artificial score improvements.45,69 Digital assessments enhance the reliability and validity of cognitive evaluations by incorporating parallel test versions and randomized item sequences.
Another critical advantage of digital cognitive assessments is their ability to evaluate a wider range of cognitive domains than traditional tools. Conventional assessments, such as the MMSE and MoCA, primarily focus on memory, language, and attention, making them effective for detecting moderate-to-severe cognitive impairment, but less sensitive to early cognitive decline. 9 However, identifying subtle cognitive changes in a community setting is important, as early detection enables timely interventions that can slow progression and support independent living. 10 In this context, newly developed digital assessments are especially valuable as they incorporate broader cognitive domains, including executive function, visuospatial abilities, and processing speed, enhancing sensitivity to mild impairments. Their applicability to community-based screening provides nurses with practical tools for identifying at-risk individuals and supporting their cognitive health.
Despite these improvements, some limitations remain for the implementation of digital cognitive assessments, particularly in detecting subtle cognitive changes in real-world settings and accounting for natural performance variability. Cognitive performance fluctuates over time, making it challenging to draw reliable conclusions from a single test. 13 As a result, there is growing recognition of the need for performance-based approaches that capture behavioral trends over time, rather than relying solely on isolated scores. 7 In this context, incorporation of digital biomarkers has been initiated to address the limitations of single-time, score-based cognitive assessments and to provide a more comprehensive understanding of cognitive health.38,40
The emerging role of digital biomarkers as complementary tools for cognitive function monitoring
Through our examination of digital biomarker studies, we found that motion-, language-, and activity-based biomarkers are commonly used to detect cognitive impairment. Diagnostic accuracy varied across studies, with activity biomarkers demonstrating AUC values between 0.59 and 0.86, while eye-tracking biomarkers achieved AUC values up to 0.95 in specific visual tasks. Although biomarker utilization for cognitive assessments has increased, validation studies are limited. As shown in Table 4, most studies were conducted in controlled environments such as clinics and laboratories, often as single-session assessments, with only a few 66 incorporating longitudinal or real-world designs. These limitations highlight the need for further studies to establish the clinical utility of digital biomarkers in daily clinical settings.
Home- and community-based assessments offer greater potential for scalability and for continuous cognitive monitoring in clinical settings. Technologies such as smart homes and wearable sensors enhance accessibility, particularly for older adults facing barriers to frequent clinic visits.20,70 Previous studies demonstrated the feasibility of IoT-based systems for monitoring daily activities and behavioral patterns in home environments 71 supporting their potential for cognitive health management. Community nurses can enhance the use of these technologies by providing patient education and participating in home-based assessments.72,73 Nurses can also assist with digital biomarker data interpretation to guide personalized care and facilitate early referrals when appropriate. However, it is important to note that direct empirical evidence supporting the role of community health professionals, such as nurses, in implementing digital cognitive assessments tools remain limited. Most of the included studies focused on tool validation in controlled or clinical environments rather than real-world, nurse-led applications. Therefore, while the potential role of nurses in facilitating digital cognitive screening and monitoring is promising, further research is required to establish their effectiveness and practical applicability in community-based settings.
Digital biomarkers have another unique advantage. 11 They can provide continuous, non-invasive assessments. 11 Rather than being an indication of a condition, digital biomarkers are passive tracking that allow you to obtain insights into your cognitive performance over time rather than relying on single-session, score-based tests. 13 However, Koo and Vizer (2019) recognized that longitudinal follow-up of behavioral trends may improve the capability for cognitive impairment detection in the early stages of cognitive deterioration. With the support of local community-based healthcare professionals, digital biomarkers hold great promise into the future for promoting proactive and preventive cognitive health strategies in elderly populations.
Nevertheless, although the new digital biomarkers offer significant benefits, they are still not ready to replace existing cognitive tests. They should rather act as adjunctive tools to complement traditional tests in terms of early detection and long-term monitoring. Most studies assessing these digital biomarkers were aimed at supporting cognitive screening rather than providing independent diagnostic capabilities. Longitudinal and practical studies in practical community contexts are needed to confirm the clinical utility of digital biomarkers.
Implications for integrated cognitive assessment strategies in nursing practice
This systematic review assessed strengths and limitations in digitizing traditional neuropsychological tests and developing new cognitive assessments. Even with developments in these approaches, they fall short of sensitivity to subtle cognitive changes and their application in the real world. As digital biomarkers evolve, there are avenues to integrate these platforms with digital cognitive tests that support continuous cognitive monitoring, greater access, and the early detection of cognitive decline in ways that are especially relevant in home- and community-based settings.
Community and public health nurses can be key practitioners to increase the linkage of digital cognitive assessment tools to nursing practice. In real-world settings, these tools may be part of nurses’ routine health checkups, home visits, and chronic disease management programs to assist patients with evidence about cognitive screening early on. Nurses should develop training programs to enhance their digital literacy and ability to administer, interpret and follow up assessment results. Additionally, as early detection and intervention becomes possible as an essential tool of the future, the collaboration between nurses, primary physicians, and ICT specialists may generate an interdisciplinary model of early detection and intervention. For instance, traditional community nurses may apply self-administered digital screening techniques to recognize vulnerable older adults, educate them on promoting cognitive health and refer these patients with early-onset decline for additional assessment. Nurse-led digital screening-type initiatives can improve accessible care at the community level.
Inspired by the insights these researchers obtained, we propose that whether traditional test/digital cognitive assessment should be digitized or developed should be a sensitive matter according to the person’s particular needs and the specific context to use it. Either way, nurses have a vital role to play in introducing these digital tools as part of routine cognitive screening and long-term monitoring. Digital biomarkers in conjunction with cognitive assessment tools may help nursing professionals identify cognitive decline sooner and take prompt action at the clinical and community levels. While additional studies are needed for corroboration of clinical utility, implementation of these combined strategies in nursing-led cognitive health programming with these strategies can improve dementia prevention and management at the patient level in nursing and the community level, with some clinical utility, only empirical work will help clarify.
It might be useful for future studies to use novel biomedical and data-driven approaches paired with digital cognitive assessment technologies at an advanced age to enrich already known biomarker methodologies in the cognitive fields with a focus on improving early detection, as well as ongoing measurement of cognitive impairment and monitoring. Recent findings have illustrated the promise of sophisticated biomarker systems and multidisciplinary technological approaches to enhance diagnostic accuracy and address the current constraints in the scope of its real-world application.74,75 Incorporating these approaches may also enhance the clinical utility and scalability of digital cognitive screening in community-based settings. Moreover, new biomedical technologies—including nanocarrier-based systems to bypass blood-brain barrier limitations—could represent adjunctive prospects to augment the sensitivity and ecological validity of cognitive assessment strategies. While these technologies have mostly been studied in therapeutic settings, their linkage with digital health interventions might assist in more accurate and continuous surveillance of neurological disorders. Nevertheless, issues of the safety, biocompatibility and clinical scale are important, requiring translational research. 75
Limitation
The majority of included studies have been carried out in controlled laboratory or clinical settings, and without rigorous real-world or longitudinal designs, the review notes. Further, his methodological limitation highlights an important gap in the current literature that merits future validation studies in community-based and naturalistic settings to guarantee ecological validity and applicability of digital cognitive assessments in practice, There are some limitations of this study. The included studies were widely heterogeneous regarding the population, assessment environment, and type of digital cognitive tool and thus might have restricted the generalization of the findings. The study designs also limited the applicability of the findings: most studies were performed in controlled environments and had small numbers of experimental subjects with no longitudinal examination. While we noted potential involvement of community nurses in the implementation of digital cognitive assessments and biomarkers, more empirical studies regarding the participation of these practitioners are still lacking in the literature. Future validation studies in real community-based settings need to be conducted before these tools can be put into practice. Policy frameworks should address the safe use, data governance, and system-level implementation of digital cognitive assessment tools in healthcare practice. Lastly, the review may have been subject to publication bias, being only comprised of peer-reviewed articles that were published in nine electronic databases.
Conclusions
This systematic review examined the validity and applicability of digital cognitive assessment approaches, including traditional digitized tests, newly developed digital tools, and digital biomarkers. Although each method offers distinct advantages, limitations remain regarding sensitivity to subtle cognitive changes and applicability in real-world settings. Based on these findings, we suggest that the choice between digitizing existing tests and developing new assessments should be tailored to specific contexts, with digital biomarkers serving as complementary tools to enhance continuous monitoring and early detection. Policymakers and healthcare organizations should establish guidelines to support the safe, equitable, and effective adoption of digital cognitive tools in community and clinical settings. Further research is needed to establish the clinical utility of these approaches, particularly longitudinal studies in community settings. Notably, more extensive and real-world validation studies done in community-based populations need to be conducted before nationwide implementation. Before these technologies can be integrated into routine care, large-scale validation studies across diverse real-world populations are needed. Utilizing digital cognitive assessment strategies in nursing practice may pave the way for more proactive cognitive care for older adults.
Footnotes
Acknowledgements
This work was supported by the National Research Foundation of Korea(NRF) grant funded by the Korea government(MSIT) (RS-2026-25489560).
Ethical considerations
This study is a systematic review and was exempt from ethical approval by the Gachon University Institutional Review Board (IRB). The exemption approval number is 1044396-202408-HR-138-01.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Gachon University research fund of 2024(GCU-202403980001) and National Research Foundation of Korea(NRF) (RS-2026-25489560).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Trail Registration
This systematic review is registered in PROSPERO (Registration No: CRD42024564512, registered on July 2, 2024)