
Abstract
Background
Despite the potential of mobile health applications for diabetes self-management, patient adoption rates remain low. Understanding patient perspectives is crucial for developing effective and user-friendly solutions that can improve diabetes self-care and education.
Objective
This study aimed to explore Malaysian patients’ perspectives on the use of mobile health applications for diabetes self-management.
Methods
Qualitative study using semi-structured interviews was conducted with 16 diabetes patients across Malaysia. Interviews were conducted via video conferencing, recorded, transcribed, and analysed using thematic analysis. Participants ranged in age from 24 to 70 years with diabetes duration from 6 to 27 years.
Results
Five key themes emerged: (1) limited adoption and awareness, (2) barriers to use, (3) localization and personalization needs, (4) healthcare system integration gaps, and (5) support preferences. Patients expressed interest in mobile health applications but faced significant barriers including economic constraints, technical difficulties, and behavioural challenges. Key desired features included automated glucose monitoring, localized food databases, educational content, and seamless communication with healthcare providers.
Conclusion
While patients recognize the potential benefits of mobile health applications for diabetes self-management, successful implementation requires addressing economic barriers, improving digital literacy, developing culturally appropriate content, and ensuring seamless integration with clinical care. Future development should prioritize user-friendly interfaces, affordability, and comprehensive support features that align with patients’ daily management needs.
Introduction
Diabetes mellitus affects 589 million adults globally, representing a significant public health challenge requiring comprehensive self-management strategies. 1 Mobile health (mHealth) applications have emerged as promising tools for supporting diabetes self-management, offering features such as glucose monitoring, dietary tracking, medication reminders, and educational resources. 2 These technologies have demonstrated worldwide efficacy in improving glycemic outcomes through glucose tracking, medication reminders, diet and exercise guidance, and enhanced patient-provider communication. Despite their potential benefits and proven effectiveness, adoption rates of diabetes-specific mHealth applications remain disappointingly low globally and particularly in developing nations.
In Malaysia, the widespread ownership of smartphones has rendered these devices an essential part of daily life, creating unprecedented opportunities for digital health interventions. 3 Malaysia is increasingly digitized with a majority of the population owning smartphones, yet adoption of health applications remains paradoxically low. Research by Sze et al. demonstrates that only about 20% of Malaysians are even familiar with mHealth tools for health management. 4 This knowledge gap is particularly concerning in diabetes care, where a recent survey in northern Malaysia found that only 13.6% of patients with diabetes used mHealth applications, with non-users overwhelmingly citing lack of awareness and technical difficulties as primary barriers. 5 While successful patient-centered development approaches have emerged, such as support web application developed through extensive patient partner engagement throughout the design process, 6 such comprehensive user-involvement methodologies remain uncommon in digital health development. These findings reveal a significant ”knowledge-adoption gap”: even as patients could substantially benefit from these applications, many remain unaware of their existence or lack the skills to utilize them effectively.
The reasons behind this gap are likely multifaceted and culturally specific. A meta-analysis encompassing 13 studies found that, on average, only 35% of individuals with diabetes used mHealth applications to manage their condition globally, despite 57% expressing interest in adopting such tools for future diabetes self-management. 7 Concerningly, 39% of patients lacked confidence in the effectiveness of mHealth applications for managing their diabetes, suggesting significant barriers beyond mere availability. In the Malaysian context, these adoption challenges appear particularly pronounced due to unique cultural and contextual factors.
This study aimed to fill that gap by performing thematic analysis on interview transcripts from Malaysian adults with diabetes. We identified key themes and codes related to knowledge and adoption of diabetes mHealth applications, focusing specifically on barriers between knowledge and usage. Our goal was to inform developers and healthcare providers about cultural, technological, and user-experience factors affecting adoption in Malaysia, with particular emphasis on identifying interconnected self-management needs and practical implementation strategies for the Malaysian healthcare context.
Methodology
Study design
A qualitative descriptive study was conducted using semi-structured interviews to explore the experiences of diabetes patients’ with mobile health applications. No specific theoretical framework was adopted. This approach was selected to capture rich, contextual data about patient perspectives and experiences without imposing predefined theoretical assumptions. Mobile health applications in this study refer to smartphone-based software applications used by diabetes mellitus patients to support self-management activities, including but not limited to blood glucose recording, diet and physical activity tracking, medication reminders, educational resources, and data visualization. Given the nature of this qualitative study and its focus on patient perspectives, no restriction was placed on the type of mobile health application used. Both device linked (such as glucometers, continuous glucose monitoring systems, or blood pressure monitors) and non-device linked applications were included, as long as participants perceived these technologies as part of their mobile app–supported diabetes management experience. The emphasis of the study was on users’ perceptions and experiences rather than on technical evaluation of devices or software performance. The study was conducted from June 2023 to September 2023 in Hospital Pulau Pinang, Malaysia.
Interview guide development
A comprehensive literature review was conducted using electronic databases (Scopus, Google Scholar, and PubMed) by PCL, YHO, CS, NNZ and SWWT from January to June 2022 to identify qualitative studies in English that explored patients’ perspectives on mobile health applications. Articles on qualitative study or interview of patients on the perspective, usability, experience and satisfaction of mobile health applications were included for item generation for the development of interview guide. The search strategy used subject terms and keywords that included: ”mobile health” or ”mhealth” or ”mobile app*” and ”qualitative” or ”interview” and ”patient” and ”perspective” or ”experience” or ”satisfaction” or ”usability”. Additionally, the reference lists of all included articles were manually screened to identify additional studies that met the inclusion criteria.
This systematic approach aimed to generate items for the qualitative study based on existing evidence. A total of 34 studies were assessed for eligibility, and 24 studies were excluded due to no question (17 studies), not qualitative study (4 studies), German language (1 study), and not mobile application (2 studies). Ten studies8–17 comprising a total of 71 questions, along with additional expert input, were included for item generation.
The nominal group technique was utilized by a panel of six experts to evaluate each item for relevance, representativeness, applicability to the local Malaysian context, and significance for diabetes patients’ self-management. Key thematic areas were identified to gather comprehensive information about mobile applications for diabetes management. Twenty-two questions were excluded due to duplication, and 41 questions were unable to reach consensus among experts. Consequently, eight questions were initially designed for the qualitative inquiry.
Content and face validation
The qualitative questions drafted were validated through both the content validation and the face validation processes. Content validation was carried out by a panel of eight experts with experience in digital health and diabetes patient care, including two endocrinologists, two family medicine specialists, three pharmacists and one engineer. Experts assessed the relevance, importance, and clarity of each item using a 4-point scale (4 = very relevant/important/clear; 1 = very not relevant/important/unclear). The validity was assessed using the item-level content validity index (I-CVI), 18 with scores greater than 0.83 considered acceptable. 19 Based on expert feedback, items were revised or removed, resulting in a second draft.
Face validation of the revised questionnaire was performed with five patients with diabetes mellitus aged 18 years and older who owned smartphones. Participants were recruited in person at the Diabetes and Endocrine Clinic, Hospital Pulau Pinang. Patients rated each item for relevance and clarity using the same 4-point scale. The I-CVI was calculated, with a value of 1.0 indicating excellent validity. Based on patient input, the questionnaire was further refined, resulting in a final version consisting of six questions.
Final interview guide
The validated interview guide consisted of six main questions: 1. Do you use any healthcare-related mobile applications? 2. Do you use any diabetes-related mobile applications? • If yes, proceed to questions 3 and 4 • If no, skip to question 5 3. Does the mobile application help you to manage your diabetes better? 4. Is there any feature in the mobile application that you feel does not help with your diabetes management? 5. Is there any barrier to use the mobile health application? 6. Is there any feature that you would like to have in the mobile application to better manage your diabetes?
Setting and participants
Participants were recruited from the Diabetes and Endocrine Clinic, Hospital Pulau Pinang, Malaysia. Inclusion criteria included: • adults aged ≥18 years, • confirmed diagnosis of diabetes mellitus (Type 1 or Type 2), • diabetes duration ≥6 months, • ability to communicate in English or Malay, • ownership of a smartphone.
Exclusion criteria included cognitive impairment or severe psychiatric illness affecting ability to participate. Participants were consented face-to-face and appointment was given for individual interview via Cisco WeBex.
Sample size and data saturation
The estimated sample size was 15 patients, based on previous recommendations for qualitative research, 20 or until data saturation was reached. Data collection was closely monitored to identify saturation. No new themes or information emerged between the 10th and 11th participants. To confirm saturation, an additional five interviews were conducted, resulting in a final sample size of 16 patients. This approach aligns with established guidelines for determining sample size adequacy in qualitative research. 21
Data collection
Semi-structured interviews were conducted through Cisco Webex by a single researcher (PC), a pharmacist specializing in diabetes care, to maintain consistency in all interviews. There was no prior relationship between the interviewer and the interviewees. Before each interview, permission to record was obtained from participants. The interviews started with ice-breaking session where demographic data collection, followed by the six qualitative questions, which related to experience, features and functions of mobile applications, and barriers. Each interview lasted approximately 15-25 minutes.
Data management and analysis
The interviews were recorded and supplemented with written notes as needed. Data were transcribed after each interview and annotations were included when relevant to capture behaviors, phonetic transcriptions of dialects, and filler words when relevant to analysis. All transcripts were checked for accuracy by another researcher prior to analysis. NVivo 14 software was utilized for data management and thematic analysis.
The analytical process followed Braun and Clarke’s six-phase framework for thematic analysis
22
: 1. transcripts were read repeatedly to understand the content and familiarize with data, 2. systematic line-by-line coding to generate initial codes, 3. searching for themes, related codes were grouped into broader categories and potential themes using Nvivo’s node and hierarchy functions, 4. reviewing themes, candidate themes were iteratively reviewed for coherence, distinction, support, and clarity, 5. each theme’s essence, scope, and meaning were defined and named concisely and 6. producing the report.
The process involved data familiarization, identification of thematic frameworks, indexing, mapping, and interpretation. Transcripts were systematically coded to facilitate organization and analysis of the data. To enhance analytic rigour and reduce researcher bias, the analysis was conducted independently by a psychology lecturer experienced in qualitative research. Throughout the analytic process, emerging codes and themes were discussed with the research team, and discrepancies were resolved through iterative discussion until consensus was achieved. A log consisting of coding decisions, theme development, and analytic memos was maintained to enhance transparency and dependability of the findings.
Results
Interview guide development and validation
Item-Level Content Validity Index (I-CVI) for Expert Validation (n=8 experts).
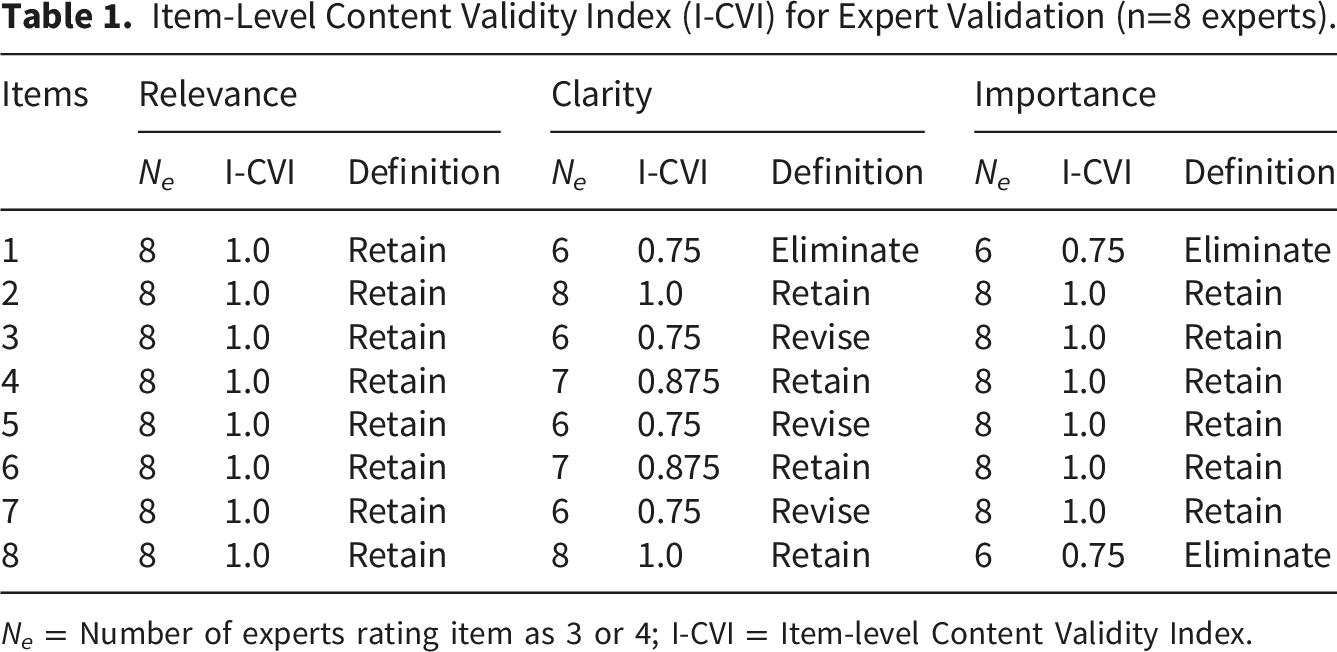
N e = Number of experts rating item as 3 or 4; I-CVI = Item-level Content Validity Index.
For face validation, five diabetes patients (60% female, mean age 50.2 ± 18.0 years, comprising 40% Malay, 40% Chinese, and 20% Indian participants) were recruited. Patients found that the six final qualitative questions were relevant and clear, with I-CVI scores of 1.0 for each item, indicating excellent validity.
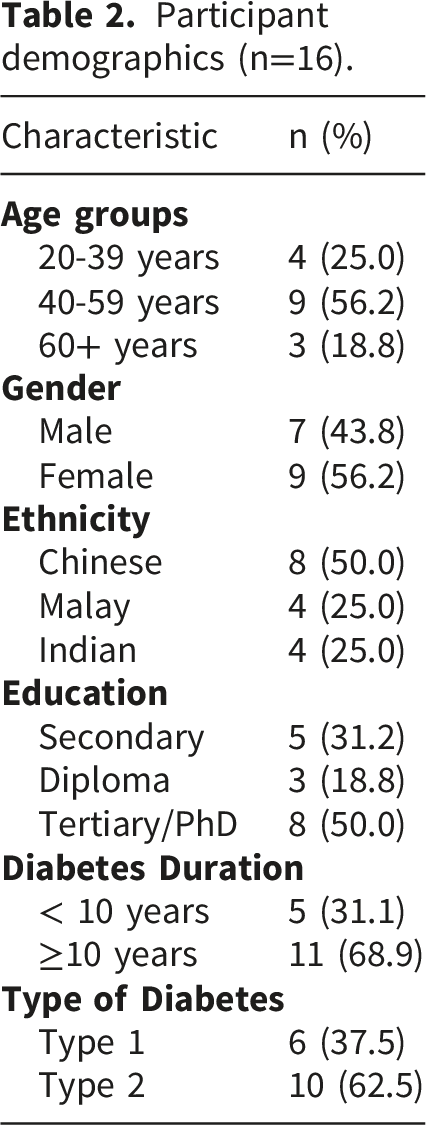
Participant characteristics
Participant demographics (n=16).
Thematic analysis
Thematic analysis revealed five major themes representing patients’ perspectives on mobile health applications for diabetes self-management. These themes are summarized in Figure 1 and include: (1) limited adoption and awareness, (2) barriers to use, (3) localization and personalization needs, (4) healthcare system integration gaps, and (5) support preferences. Summary of themes.
Theme 1: Limited adoption and awareness
Despite widespread ownership of smartphones, patients demonstrated limited participation in diabetes-specific mobile applications. As illustrated in Figure 2, 75% of the participants reported that they had never used diabetes applications, while 18.75% were current users, and 6.25% were former users who had discontinued use. Current status of diabetes app usage.
”Don’t know how to use or download [diabetes apps].”
Usage was often inconsistent, as PT06 explained: ”Yes. The one record the blood sugar one. Rightest app to record blood sugar, now still got use but forget to update.”
”No barrier, I am not aware of such application. The exercise app also I knew it through friends.”
Similarly, PT10 expressed: ”No barrier, I do not have any exposure regarding mobile health application.”
This limited awareness expanded across education levels and age groups, suggesting inadequate promotion and education about available diabetes health tools within clinical settings.
Theme 2: Barriers to use
The participants identified several obstacles preventing effective use of diabetes-related applications. These barriers can be categorized into economic, technical, and behavioural factors as shown in Figure 3. Barriers to diabetes-related app usage.
”To use the apps, need to get the strips and the strips are expensive so not using.”
PT16 echoed this concern while describing additional access challenges: ”Hard to use as not free, I am traveling now to my in law for prayer and not at home. I used back my old brand of strips as unable to find the strips for this app. Besides, the strips are expensive so I used back my normal old brand.”
Some participants suggested implementing cost-mitigation strategies. PT01 proposed: ”Hopefully we can get discount. Something like reward system…When you go to purchase the new test strips, here we can have some reward, you know, or discount.”
”Not used to the mobile application and I am not good at using mobile phone.”
PT02 highlighted visual challenges:
”My eye sight not good and need magnifying glass. My eyesight is getting poorer and poorer. Larger size font in the app.”
”I think because I am lazy”
Theme 3: Localized and personalized needs
Cultural appropriateness emerged as a critical concern for 42.7% of participants, highlighting the importance of locally relevant features across two main areas namely local food culture compatibility and food intake measurement.
”A lot of the food options there they give us not very applicable to our local diet so not helping to manage diabetes better…Like you go to eat economy rice, the options is not very matching with the food there.”
”…the food in Malaysia is quite different from other countries, so if you are to take photo, it’s quite difficult to judge whether it’s high in calorie or what.”
To address these challenges, participants desired automated food recognition capabilities. PT05 suggested: ”Ideally one more simple one, like nowadays, Taobao can do, you just take photo of what you eat and then it can estimate what you eat. It’s easier to record.”
Theme 4: Healthcare system integration gaps
Integration with clinical care emerged as a significant concern for 50% of participants (8/16).
”I want to ask questions through the mobile apps because we see doctor like every 3 months or 6 months. In between when there’s something we cannot ask questions to the healthcare provider.”
”Not a problem to share information with healthcare providers, what is there to hide.”
PT05 affirmed: ”Of course I am willing to share data with healthcare providers, then if I take the data and then I keep to myself makes no sense, right?”
Theme 5: Support preferences
Patients demonstrated preference for comprehensive applications addressing multiple health management aspects, with various features desired by different participant subgroups across five main categories as shown in Figure 4. Desired features for diabetes-related application.
PT03 requested:
”It will be good if provide education.”
PT09 sought: ”Education regarding cholesterol, blood sugar and high blood pressure.”
”Give alert when blood sugar too low or too high, will be good.”
PT03 wanted: ”The app can inform me when my sugar is very high or very low.”
”I can check blood sugar at anytime and no need to poke. So one that you need to put on your body, sensor.”
”record blood pressure reading, provide education related to diabetes, food chart and exercise.”
PT09 sought comprehensive features: ”record step count. I hope it can record the stress level. The apps need to have records of body weight too and also calendar to key in appointments.”
”Tailored exercise as we have knee and leg pain. Internet has many types of exercise but not sure which exercise is the correct to do.”
PT07 requested: ”Apps suggest exercise like just for exercise for 15 minutes a day.”
Discussion
This study revealed important insights into patients’ perspectives on mobile health applications for diabetes self-management. The findings highlighted a complex landscape where potential benefits were constrained by practical, cultural, and systemic barriers.
Although this study was not guided by a predefined theoretical framework, the findings align with established theories of technology adoption and health behaviour. Participants’ emphasis on convenience, attitude and actual usage towards mobile health application and perceived benefits reflects key constructs of the Technology Acceptance Model. 23 Additionally, themes related to personalized need, support preference and motivation resonated with the Health Belief Model, 24 whereby perceived benefits and reduced barriers influence health-related behaviours. These theoretical linkages support the relevance of the findings and enhance their interpretive depth.
The limited adoption despite widespread smartphone ownership suggests that availability alone is insufficient for meaningful engagement. This finding was consistent with studies conducted in Malaysia that reported low adoption rate and lack of awareness which reflected that digital health might be at the infancy stage in Malaysia.4,5 Economic barriers, particularly test strip costs, represent a significant obstacle that technology solutions must address. This finding aligns with broader literature on health technology adoption in resource-constrained environments.
The emphasis on localization and cultural appropriateness reflects the global challenge of developing universally applicable health technologies. Malaysian patients’ struggles with Western-oriented food databases and portion measurements which were impractical for daily use. This underscore the need for culturally specific development approaches as “one size fits all” approach might fail to meet the needs of diverse population. A study conducted in India that evaluated 11 mobile health applications reinforced the importance of cultural and linguistic adaptation in diabetes self-management tools. Applications that provided calorie and dietary information aligned with local food practices and delivered in familiar languages demonstrated higher levels of user engagement. 25 This finding has implications for application development, suggesting that databases must be populated with locally relevant content in order to be more effective in supporting sustained use and meaningful self-management behaviours as compared to non-localized applications. Our qualitative findings complement quantitative app evaluation studies that have used standardized rating instruments.
Integration challenges reveal gaps between technological capabilities and healthcare system realities. Technology illiteracy posed as barriers to adoption of such technologies. In this study, participants represented diverse ethnicities, age groups and both Type 1 and Type 2 diabetes mellitus. While participants generally acknowledged the potential benefits of adopting mobile health applications in supporting their diabetes care, older adult participants expressed concerns regarding confidence in using this technology. This finding was consistent with previous studies which reported older adults and individuals with low health and digital literacy had difficulties adopting mobile health applications.26,27 This highlighted the importance of simple, user friendly design which is adaptable to patients’ varying age digital competence levels to improve the uptake and sustainability of this technology in diabetes management. A study conducted in Singapore with participants aged 40 to 69 years also emphasized on simple and automatic application features. 2
Patients’ desire for communication with healthcare providers indicates that effective applications must function as bridges between patients and clinical care rather than standalone solutions. Selen and Polat 28 demonstrated that structured digital interventions can effectively bridge these gaps when properly implemented. Such integration enabled better clinical care and individualized feedback and recommendations from healthcare professionals. Evidence from randomized controlled trial supported this perspective as glycaemic control improved with interactive mobile health application in diabetes management which facilitated timely interventions and data sharing with healthcare professionals. 29
The comprehensive support preferences suggest that patients view diabetes management holistically, expecting applications to address multiple aspects of their health and daily life. This perspective challenges developers to create integrated solutions rather than single-purpose applications.
Despite limited current usage, participants demonstrated clear understanding of desired features and potential benefits, suggesting readiness for adoption if barriers were addressed.
Limitations
This study’s strength lies in its patient-centered approach, capturing diverse perspectives across age, education, and ethnicity. The qualitative methodology allowed deep exploration of experiences and preferences that quantitative studies might miss. Our sample included both users and non-users of diabetes apps, providing comprehensive insights into adoption barriers.
Several limitations should be acknowledged. The sample was limited to smartphone owners, potentially excluding perspectives from those facing more fundamental digital access barriers. Recruitment through a single urban healthcare facility may have biased toward more engaged patients and limits generalizability both within the Malaysian context and to those in remote areas who may face different technological and infrastructure challenges. However, efforts were made to enhance the contextual relevance and validity of the study. The interview guide was validated by experts from different geographical locations in Malaysia who had experience managing diabetes patients from both urban and rural settings with different levels of resources. This process ensured that the questions were comprehensible for different types of patients.
The study’s focus on a single country limits broader generalizability, though findings likely resonate with countries facing comparable digital health adoption challenges. Caution should be exercised when extrapolating the findings to countries where the healthcare delivery systems and technology accessibility might differ significantly. Variation in health beliefs, digital literacy, accessibility to healthcare and patient-healthcare professionals relationship might also influence the perception of mobile health applications.
We did not evaluate specific apps in detail, preventing assessment of how different design approaches influence user experience. Future research should combine qualitative insights with usability testing of specific applications. Moreover, the mobile health applications defined in this study was broad to reflect real-world use and user experiences. Few participants in the study had experiences with mobile application that were linked to external monitoring device such as RightestTM application that was linked with glucometer. Hence, some perceptions described by participants might have been influenced by the usability, reliability and availability of device-related components, rather than the application alone. There was a total of 16 and 19 diabetes-related mobile applications downloadable from Apple Apps and Google Play Store in Malaysia, respectively. Most of these applications were standalone applications focusing on self-recording of blood glucose levels, medications, diet and physical activities. Most available applications were internationally developed rather than locally tailored, and only a limited number offered integration with external monitoring devices. 30 This app landscape may have shaped participants’ expectations and experiences of mobile health applications, particularly in terms of cultural relevance, language suitability, and technological sophistication. As such, participants’ views largely reflect interactions with basic, non-integrated applications commonly accessible in Malaysia, which should be considered when interpreting the findings. Future research should combine qualitative insights with usability testing of specific applications and explicitly distinguish between app-specific features and device-related factors as well as examine user experiences with locally developed mobile application. While this study focused exclusively on patient perspectives, healthcare providers’ perspectives on AI-based mobile applications for diabetes education and behavioral management have been explored in complementary research, 31 revealing provider concerns about accessibility, data privacy, and the need for human interaction alongside AI support.
Conclusion
This study reveals significant gaps between the potential of mobile health applications for diabetes management and their current real-world implementation. Despite recognizing potential benefits, patients face multiple barriers to adoption and sustained use, including economic constraints, usability challenges, and misalignment with local contexts and clinical care patterns.
Patients recognize substantial potential in mobile health applications for diabetes self-management but face significant barriers to adoption and effective use. Successful implementation requires addressing economic constraints, improving digital literacy, developing culturally appropriate content, and ensuring seamless integration with clinical care systems. Focus should be placed on developing simple, user-friendly, and equipped with multilingual options. Education, awareness programs and support initiatives should be integrated into routine clinical care to improve digital literacy and ensure usability across diverse populations in Malaysia. In addition, healthcare professionals should actively engage with patients through mobile health applications, providing timely clinical intervention to build trust towards this technology. Affordability should be prioritized, with policy makers and developers working together to subsidize the costs while ensuring culturally and linguistically appropriate features that promote equitable access across all socioeconomic levels.
Future research should focus on quantifying the impact of addressing these barriers on adoption rates and health outcomes, while exploring optimal integration strategies with existing healthcare systems. Future mobile health applications for diabetes care development should be holistic with comprehensive features, user-friendly interfaces, affordable pricing models, and synchronization with diverse cultures and linguistics to ensure broader accessibility and adoption. By prioritizing patient perspectives and needs, mobile health applications for diabetes can achieve their potential to improve self-management and health outcomes.
Footnotes
Acknowledgements
This work was supported by the Fundamental Research Grant Scheme (FRGS/1/2023/ICT02/USM/02/3), Ministry of Higher Education, Malaysia. We thank the Director General of Health, Ministry of Health Malaysia for the permission to publish this article.
Ethical considerations
This research is registered in the National Medical Research Register, Malaysia (NMRR ID-22-02846-I21) and approved by the Medical Research Ethics Committee, Ministry of Health, Malaysia.
Consent to participate
All participants received an information sheet and written informed consent was obtained. All research procedures were conducted according to ICH-GCP and other regulatory requirements.
Authors contributions
PCL contributed to study conception, design, material preparation, data collection, analysis, and writing and review of manuscript.
HZ contributed to study conception, design, writing, and review of manuscript.
YWC contributed to study conception, design, analysis, writing, and reviewing of manuscript.
YHO, CS, NNZ and SWWT contributed equally to this work including material preparation, analysis, writing, and review of manuscript.
All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was supported by the Ministry of Higher Education (MOHE), Malaysia through the Fundamental Research Grant Scheme FRGS/1/2023/ICT02/USM/02/3.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.