
Abstract
Background:
Minimally invasive approaches have become a feature of cardiac surgery. We compared the outcomes of atrial septal defect closure through either a right thoracotomy or a median sternotomy in adults.
Methods:
Patients who underwent atrial septal defect closure of ostium secundum defects through either a right thoracotomy (n = 14) or a median sternotomy (n = 7) were analyzed. The atrial septal defect was closed with cardiac arrest of the ascending aorta clamped under a cardiopulmonary bypass in both groups.
Results:
The preoperative characteristics of the two groups did not significantly differ. The durations of cardiopulmonary bypass and of cardiac arrest were significantly longer, but the amount of intraoperative blood loss was significantly lower, in the right thoracotomy than in the median sternotomy group. The early postoperative course did not significantly differ between the groups, whereas postoperative minor complications developed in three and two patients in the right thoracotomy and median sternotomy groups, respectively.
Conclusion:
The outcomes of atrial septal defect closure through a right thoracotomy and a median sternotomy were comparable, suggesting that right thoracotomy is a safe and effective alternative to median sternotomy for atrial septal defect closure in adults.
Introduction
A median sternotomy (MS) is the gold standard approach to cardiac surgery. However, minimally invasive approaches have become a feature of cardiac surgery and are established for all types of surgery. A minimally invasive approach with a right thoracotomy (RT) might be less appropriate for extended surgical exposure or complicated cardiac procedures than an MS approach. However, the advantages of decreased invasiveness or a better cosmetic aspect are attractive, especially for atrial septal defect (ASD) closure after relatively simple surgical procedures in patients who are relatively younger than those who undergo other types of cardiac surgery.1,2 We evaluated whether or not RT can serve as an alternative to MS for ASD closure in adults.
Materials and methods
Patients
We retrospectively reviewed 21 adult patients with solitary secundum ASDs that required surgery with ASD closures between October 2004 and April 2013. Patients who underwent concomitant revascularization and procedures for arrhythmia or valvulopathy were excluded. Patients with severe atherosclerosis and concomitant congenital cardiac anomalies such as partial anomalous pulmonary venous drainage detected by enhanced computed tomography were also excluded. The included patients were allocated to groups according to whether they underwent ASD closure through an RT (n = 14) or an MS (n = 7). We then compared their preoperative characteristics of age, sex, body surface area, presence or absence of symptoms, smoking habits, comorbidities, rhythm on electrocardiogram on admission, systolic and mean pulmonary arterial pressures, ratio of systemic to pulmonary blood flow (Qp/Qs), intraoperative factors, site of arterial inflow, duration of cardiopulmonary bypass (CPB) and cardiac arrest, direct or patch closure of ASD, blood loss, early postoperative outcomes, period of intubation, duration of intensive care unit (ICU) stay and hospitalization, total amount and the duration of blood drainage, maximum white blood cell (WBC) counts, levels of C-reactive protein, mortality, morbidity and postoperative echocardiography to assess residual ASD shunt flow. The Gifu University Institutional Review Board for Clinical Research approved the study, without the need for informed consent.
Surgical technique
Secundum ASD was closed under CPB with cardiac arrest in both groups. Patients mainly selected the approach based on explanations from surgeons, whereas MS was preferred for patients with comorbid moderate atherosclerosis of the aorta or arterial stenosis of arteriosclerosis obliterans.
CPB was established in the RT group via inflow from the femoral artery, and unilateral femoral venous cannulation into inferior vena cava was concurrent with RT through the fourth or occasionally the third intercostal space. Inflow from the femoral artery consisted of unilateral and occasionally bilateral cannulation if the arterial diameter was small, and a prosthetic graft had recently been anastomosed to the femoral artery. Pericardiotomy and cannulation of the superior vena cava then proceeded through RT under CPB. In the MS group, CPB was established via ascending aortic and bicaval cannulation. The ASD was closed directly or with an autologous pericardial patch after achieving cardioplegic arrest with a clamped ascending aorta in both groups. Surgeons intraoperatively determined the closure procedure based mainly on the size of the ASD. The right atriotomy was closed under cardiac arrest in the RT group and under a beating heart after aortic declamping in the MS group. The left atrium was kept filled with blood, while the ASD was closed and the closure was finally completed with lung expansion performed by anesthesiologists. Thereafter, de-airing from the aortic root cannula was maintained until micro bubbles disappeared on transesophageal echocardiography. These techniques proceeded under carbon dioxide infiltration. The 19-Fr drainage tubes were placed in the pericardium and right pleural space of the RT group and in the pericardium and post-sternum space of the MS group.
Statistical analysis
Data were statistically analyzed using SPSS Statistics 21 software (SPSS, Chicago, IL, USA). Values are expressed as means ± standard deviations or as frequencies and proportions. Quantitative parametric and non-parametric data were compared using an unpaired Student’s t-test and the Mann–Whitney U-test, respectively. Categorical variables were compared using the χ2 or Fisher’s exact test. The p values of <0.05 were considered significant.
Results
Table 1 shows the preoperative characteristics of the patients. Age, sex, body surface area, presence or absence of symptoms, smoking habits, hypertension, hyperlipidemia, diabetes mellitus and renal dysfunction did not significantly differ between the two groups. One patient in the RT group developed moderate iron deficiency anemia after gastrectomy for gastric carcinoma, and another who had chronic hypoxia associated with pulmonary hypertension was using home oxygenation therapy (HOT). All patients upon admission had sinus rhythm, whereas some had a history of paroxysmal supraventricular arrhythmia. The results of a hemodynamic study showed that the preoperative maximum and mean pulmonary arterial pressures (31 ± 9 vs 26 ± 13, ns, and 19 ± 5 vs 18 ± 10, ns, respectively) and Qp/Qs (2.76 ± 0.60 vs 2.21 ± 0.75, ns) did not significantly differ between the groups.
Preoperative characteristics of the patients.

BSA: body surface area; GR: gastrectomy; HOT: home oxygenation therapy; MS: median sternotomy; PAP: pulmonary arterial pressure; Qp/Qs: ratio of systemic to pulmonary blood flow; RT: right thoracotomy; SR: sinus rhythm.
Table 2 shows the intraoperative factors. The durations of CPB and cardiac arrest were longer in the RT group than in the MS group (105 ± 32 min vs 45 ± 16 min, p < 0.001; and 45 ± 17 min vs 23 ± 9 min, p = 0.004, respectively). The site of arterial inflow was the femoral artery in 10 patients, of which 5 were bilateral, and a prosthetic graft was anastomosed to the femoral artery in 4 patients in the RT group. None of the patients were converted from RT to MS. Significantly less intraoperative blood was lost by the RT group than the MS group (89 ± 53 mL vs 209 ± 142 mL, p = 0.01). Autologous blood from all but two patients in the RT group was routinely preserved. These two patients required homologous blood transfusion due to chronic iron deficiency anemia and chronic hypoxia.
Intraoperative factors.

ASD: atrial septal defect; CPB: cardiopulmonary bypass; RT: right thoracotomy; MS: median sternotomy.
Table 3 shows the early postoperative outcomes. Intubation was significantly longer in the RT group than in the MS group (4.0 ± 4.6 h vs 1.7 ± 3.7 h, p = 0.038). However, the length of stay in the ICU and hospitalization, as well as the total amount and duration of blood drainage, did not significantly differ between the two groups. Laboratory findings revealed no significant differences between WBC counts and levels of C-reactive protein between the two groups. Although postoperative paroxysmal atrial fibrillation occurred in one and two patients in the RT and MS groups, respectively, the difference did not reach statistical significance. Life-threatening postoperative complications such as aortic dissection, limb ischemia or cerebral infarction did not arise in either group. Postoperative echocardiography confirmed the absence of residual shunt flow in all patients. All of our patients remained alive and were discharged home without complications.
Early postoperative outcomes.
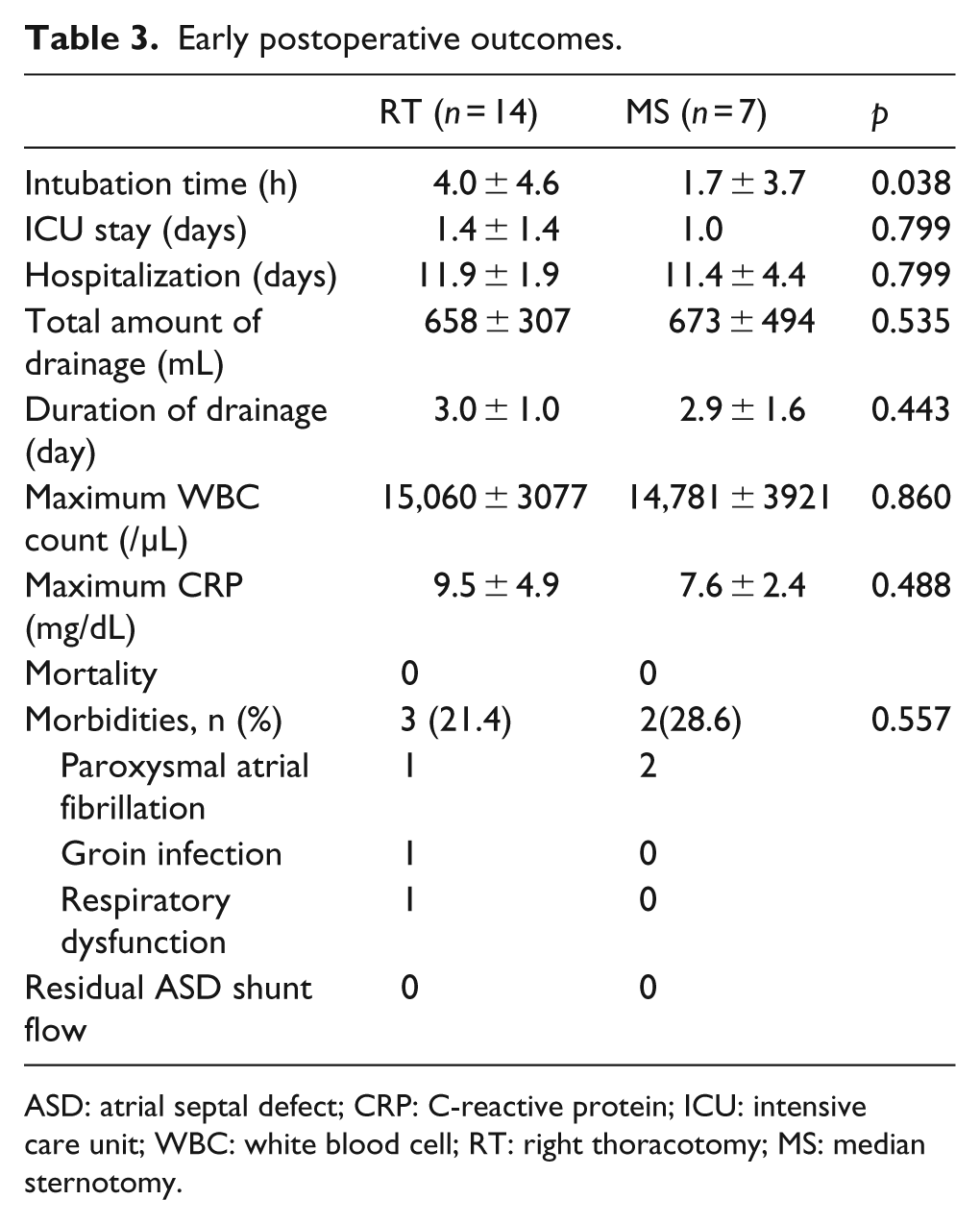
ASD: atrial septal defect; CRP: C-reactive protein; ICU: intensive care unit; WBC: white blood cell; RT: right thoracotomy; MS: median sternotomy.
Discussion
ASDs should be closed in adults,3,4 and the postoperative outcomes of this type of adult congenital cardiac surgery are good. 5 MS has been the gold standard approach in cardiac surgery because almost all aspects of the heart can be reached and complex measures such as revascularization, valve surgery and procedures for arrhythmia can be executed. However, an MS requires a large surgical wound around the sternum that can cause bleeding from bone marrow that occasionally requires blood transfusion and results in mediastinitis, which is often a critical complication although ASD itself is not a critical disease. In contrast, minimally invasive approaches have become a feature of cardiac and other types of surgery.6,7 Minimally invasive cardiac surgery delivers the benefits of smaller, less painful wounds, shorter hospital stay, more rapid postoperative recovery and cost reductions. 1 Preferable results of minimally invasive ASD closure have been reported,1,2 and Vida et al. 8 obtained excellent cosmetic results. In addition, a thoracotomy without either a partial or a full sternotomy could help patients with non-fatal ASD to avoid critical postoperative complications such as mediastinitis.
Minimally invasive approaches through an RT seem to have some limitations compared with MS. They might be inadequate for extended surgical exposure or complicated concomitant cardiac procedures such as coronary, valve, aortic and arrhythmia surgery. Cerebral infarction due to retrograde perfusion using inflow from the femoral artery must be avoided especially when the aorta is atherosclerotic, and peripheral arterial cannulation is associated with a risk of aortic dissection and lower limb ischemia. 9
We prefer both inflow from the femoral artery and inferior vena caval drainage from the femoral vein in order to avoid the interruption of the surgical field by the cannulae through thoracotomy and thoracotomy becoming larger. And then, we preoperatively assessed the aorta using enhanced computed tomography to prevent cerebral infarction and avoided the RT approach when atherosclerosis was evident. Chang et al. 2 described the importance of de-airing, which we also applied. We previously cannulated the femoral artery for inflow, but bilateral cannulation was occasionally required because of a small femoral artery diameter. However, the prosthetic root anastomosed to the unilateral femoral artery has recently been used to maintain sufficient flow and prevent aortic dissection associated with cannulation maneuvers. Although the groin incision became infected in one patient in the RT group, life-threatening postoperative complications such as cerebral infarction, aortic dissection and limb ischemia did not arise in our patients.
ASDs were often combined with other congenital cardiac anomalies such as partial anomalous pulmonary venous drainage and persistent left superior vena cava. We preoperatively evaluated such anomalies by echocardiography and multidetector computed tomography that offers excellent and reliable spatial resolution. 10
We evaluated whether or not RT can serve as an alternative to MS for closing ASD in adults. Pericardiotomy and cannulation of the superior vena cava through the RT proceeded after CPB was established via the femoral arteries and unilateral femoral veins, which prolonged the CPB in the RT group compared with the MS group. The right atriotomy was closed while maintaining cardiac arrest in the RT group, whereas closure proceeded under a beating heart after aortic declamping in the MS group. Therefore, cardiac arrest was more prolonged in the RT group compared with the MS group. However, less blood was lost during procedures in the RT group than in the MS group, but other peri- and postoperative factors did not significantly differ between the two groups. This suggested that the thoracotomy approach might be less invasive and that the postoperative courses of ASD closure through an RT and an MS are quite similar.
This study has some limitations. It was not a randomized prospective design, and only the early postoperative outcomes of a small patient cohort were available. A randomized prospective study of long-term outcomes among a large patient cohort is needed. In conclusion, the comparable outcomes of ASD closure between RT and MS in this series suggested that RT could be a safe and effective alternative to MS for ASD closure in adults.
Footnotes
Acknowledgements
Presented at the Annual Scientific Meeting of the International Society for Minimally Invasive Cardiothoracic Surgery, 12–15 June 2013, Prague, Czech Republic.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.