
Abstract
Background
Acute otitis externa (AOE) is a common condition encountered in primary care. Evidence-based guidelines recommend topical antimicrobial therapy as first-line treatment for uncomplicated disease regardless of diabetes status. However, clinicians may escalate treatment in patients with diabetes because of concern for necrotizing otitis externa (NOE), a rare but potentially life-threatening complication. This study aimed to evaluate whether diabetes status influences systemic antibiotic use in uncomplicated acute otitis externa and to assess factors associated with treatment decisions.
Methods
A cross-sectional survey was distributed to primary care clinicians participating in a multi-state primary care practice-based research collaborative, comprising physicians, nurse practitioners, and physician associates within the specialties of family medicine, general pediatrics, and general internal medicine. The survey instrument asked clinicians what they would select as first-line treatment for uncomplicated AOE in patients with and without diabetes mellitus (DM). It also assessed factors influencing management decisions as well as confidence in identifying NOE. The primary outcome was whether the clinician reported they would use systemic antibiotics for treatment of AOE, comparing treatment decisions using relative risk (RR) with 95% confidence intervals (CI) for antibiotic exposure given the presence of DM.
Results
Out of 257 invitations, 58 respondents completed the survey (22.6%). Systemic antibiotics were selected more frequently when DM was present (19.0%) compared with when DM was absent (5.2%), resulting in a significantly increased likelihood of reported systemic antibiotic use (RR = 3.67; 95% CI, 1.08–12.47; p = 0.043). Clinician confidence in identifying NOE varied, with most respondents reporting only slight or moderate confidence.
Conclusions
Primary care clinicians reported substantially higher use of systemic antibiotics when managing uncomplicated AOE in patients with DM, representing nearly a fourfold increase in antibiotic exposure despite guideline recommendations favoring topical therapy alone. These findings highlight practice variation which may be driven by concern for necrotizing otitis externa, underscoring opportunities to improve antibiotic stewardship and clinician confidence in risk stratification.
Keywords
Introduction
Acute otitis externa (AOE) is one of the most common ear conditions encountered in primary care, urgent care, and emergency medicine, resulting in substantial discomfort, lost productivity, and healthcare utilization among adults.1-4 High-quality evidence and multiple professional guidelines consistently support topical antimicrobial therapy, with or without corticosteroids, as first-line treatment for uncomplicated AOE.1,3-7 Systemic antibiotics provide no added benefit in uncomplicated disease and are associated with increased adverse effects, antimicrobial resistance, and healthcare costs.1,3-8
Management decisions become more complex in adults with diabetes mellitus. Diabetes is a well-established risk factor for necrotizing (malignant) otitis externa (NOE), a rare but potentially life-threatening infection characterized by extension beyond the external auditory canal into the skull base.1,9-13 Early NOE can initially resemble uncomplicated AOE, and subtle findings such as persistent otalgia, granulation tissue, or cranial nerve involvement may be absent early in the disease course.1,9-13 This overlap creates clinical tension: while uncomplicated AOE in patients with diabetes responds effectively to topical therapy alone, clinicians may escalate treatment out of concern for occult or evolving NOE, particularly when glycemic control is suboptimal or additional immunocompromising factors are present.1,3,5,14,15 Necrotizing otitis externa remains rare, with estimated incidence rates ranging from approximately 1 to 2 cases per million annually, though risk is higher among older adults with diabetes.10,11
Despite these concerns, existing evidence-based guidelines do not recommend routine escalation of therapy for uncomplicated AOE based solely on diabetes status.1,3,9 Current recommendations reserve systemic antibiotics for cases with extension beyond the ear canal, systemic illness, or severe immunosuppression, noting that diabetes alone does not justify deviation from topical therapy.1,3-5 However, the relative rarity of NOE, limitations in high-quality prospective data, and the potentially devastating consequences of missed diagnosis contribute to persistent uncertainty in clinical practice. In the absence of clear, diabetes-specific guidance, clinicians may rely on individual judgment rather than standardized recommendations, resulting in wide variation in management strategies.
Provider Choice of Systemic Antibiotic Use by Diabetes Status

Any systemic antibiotic exposure defined as systemic antibiotics alone or in combination with topical therapy. Percentages reflect responses for each clinical scenario; each clinician evaluated both diabetes and non-diabetes scenarios.
Methods
This cross-sectional study used a voluntary, anonymous online survey distributed to primary care clinicians, including attending physicians, residents, nurse practitioners, and physician associates. Clinicians were recruited through a multi-state primary care practice-based research collaborative comprising physicians, residents, nurse practitioners, and physician associates practicing in the specialties of family medicine, pediatrics, and internal medicine. The survey was distributed to 257 clinicians included on the collaborative participant list. Initial distribution occurred on October 31, 2025, with up to three reminder emails sent to nonresponders on November 7, November 14, and November 21, 2025. No incentives were offered for participation.
Respondent Characteristics and Survey Responses (n = 58)

AOE = acute otitis externa; ENT = otolaryngology; ID = infectious disease.
*Respondents could select more than one option; percentages for multi-select items do not sum to 100%.
The survey instrument was developed using an iterative process with evidence of content and response process validity obtained through cognitive pretesting. A diverse group of primary care clinicians, including physicians, nurse practitioners, and physician associates, reviewed the survey across multiple rounds. Seven primary care clinicians affiliated with the practice-based research collaborative provided feedback on clarity, relevance, and interpretability. The survey was revised iteratively until further pretesting did not yield additional substantive changes.
The primary outcome measure was treatment modality selected for AOE in patients with diabetes compared with those without diabetes. Treatment options were categorized as (1) topical antibiotics, (2) topical antibiotics with steroids, (3) systemic antibiotics, (4) combination therapy, or (5) other. Clinician confidence in recognizing NOE was assessed using a 5-level Likert-type scale.
Descriptive statistics were used to summarize responses. Because each respondent evaluated both clinical scenarios, paired comparisons were assessed using McNemar testing for the primary binary outcome. For the primary binary outcome of any systemic antibiotic exposure versus no exposure, relative risk (RR) with 95% confidence intervals was selected as the primary effect measure. Comparisons between diabetes and no diabetes scenarios were performed using Fisher exact test with statistical significance defined as p < 0.05.
Results
A total of 58 clinicians completed the survey. Respondents represented a range of experience levels, including early career clinicians and those with more than 20 years of practice experience.
Clinicians reported a higher likelihood of selecting systemic antibiotic therapy for uncomplicated acute otitis externa when diabetes mellitus was present. Any systemic antibiotic exposure (systemic antibiotics alone or in combination with topical therapy) was selected for 19.0% (11/58) of patients with diabetes compared with 5.2% (3/58) of patients without diabetes (Table 2; Figure 1). This corresponded to a significantly increased probability of systemic antibiotic exposure in the presence of diabetes (relative risk [RR] = 3.67; 95% CI, 1.08–12.47; p = 0.043). In addition to antibiotic escalation, some clinicians indicated they would obtain laboratory assessment of glycemic control or arrange closer clinical follow-up for patients with diabetes. The distribution of systemic antibiotic use by diabetes status is shown in Table 1, while the full distribution of first-line treatment selections is illustrated in Figure 1. Reported first-line treatment choices for uncomplicated acute otitis externa by diabetes status
Clinicians reported varying frequencies of encountering acute otitis externa in practice. The majority of respondents (56%, n = 32) encountered AOE at least once per month but less than weekly, while 27% (n = 15) encountered AOE at least once per year but less than monthly. Seventeen percent (n = 10) reported seeing AOE at least once per week.
Clinician confidence in identifying necrotizing otitis externa varied substantially (Figure 2). Forty percent (n = 23) of respondents reported being slightly confident, 30% (n = 17) moderately confident, and 16% (n = 9) not at all confident. Lower clinician confidence appeared to coincide with higher rates of systemic antibiotic selection, although this relationship was not formally tested. Confidence in identifying necrotizing otitis externa (NOE)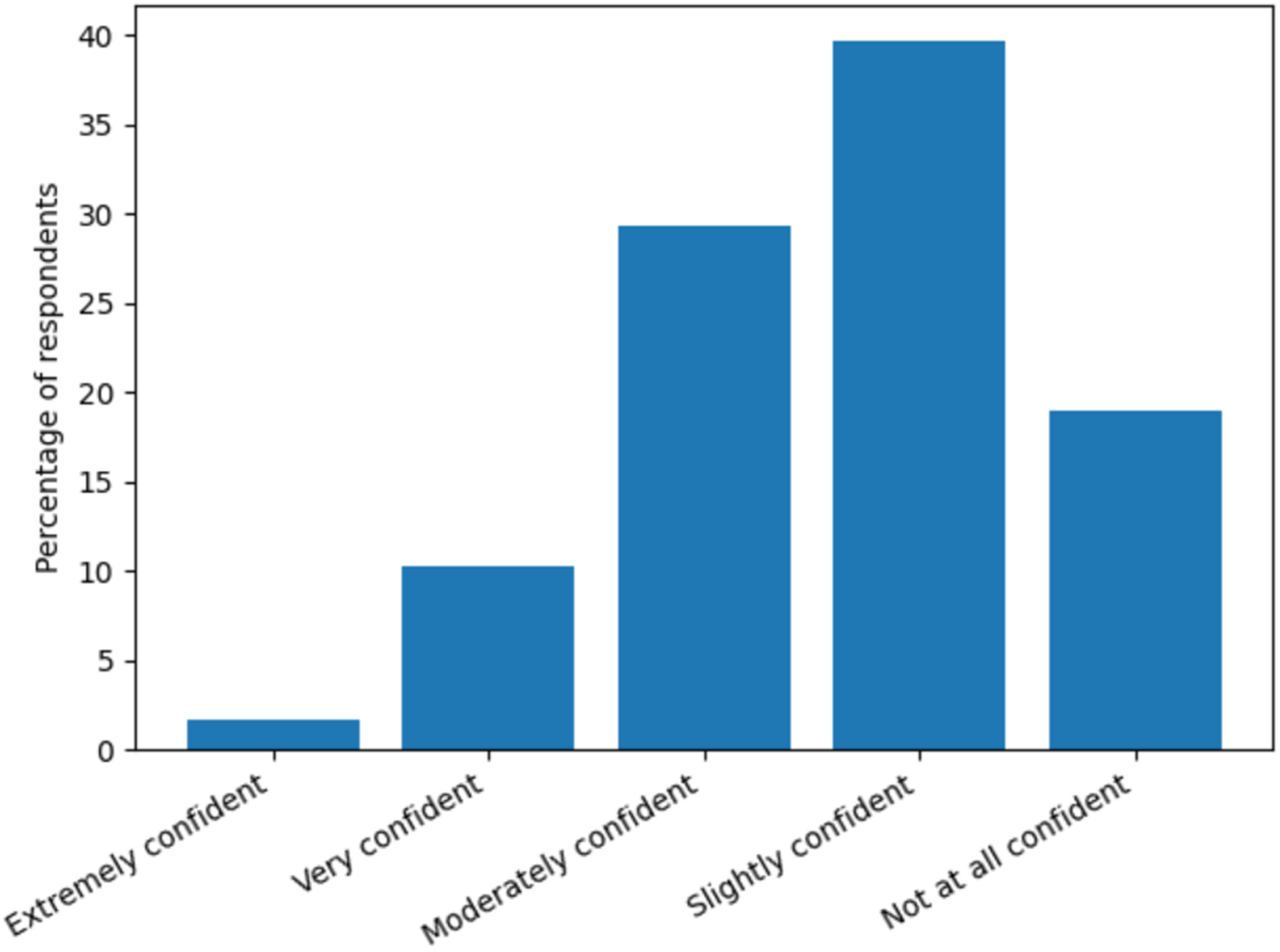
The primary factors influencing treatment decisions for patients with diabetes were diverse. Nearly half of respondents (47%, n = 27) cited patient-specific factors such as glycemic control and comorbidities as the most important determinants of management, while 30% (n = 17) identified clinical guidelines or protocols as their primary influence. A smaller proportion (15%, n = 9) reported relying primarily on personal clinical experience or other factors.
Discussion
In this cross-sectional survey of primary care clinicians, diabetes mellitus was associated with significantly increased risk of systemic antibiotic use for uncomplicated acute otitis externa. Although topical therapy remained the most selected first-line treatment in both patient scenarios, clinicians were substantially more likely to select systemic antibiotics when diabetes was present. This finding is a meaningful deviation from evidence-based guidelines, which recommend topical antimicrobial therapy alone for uncomplicated AOE regardless of diabetes status.1,3-5 This pattern may reflect risk-averse decision-making influenced by concern for missing rare but serious complications such as necrotizing otitis externa. Given the high prevalence of diabetes in primary care, small deviations from guideline-concordant management may result in substantial cumulative antibiotic exposure at the population level. 16
The observed treatment escalation likely reflects clinician concern for necrotizing otitis externa (NOE), a rare but potentially life-threatening complication that occurs disproportionately in individuals with diabetes. Population-based studies have consistently demonstrated an elevated risk of NOE among patients with diabetes, particularly in older adults and those with poor glycemic control.1,3,9-13,17 However, current guidelines explicitly advise against routine systemic antibiotic use in uncomplicated AOE based solely on diabetes status, reserving escalation for cases with extension beyond the external auditory canal, systemic illness, or severe immunosuppression.1,3-5 The tension between guideline recommendations and perceived clinical risk likely contributes to variability in practice. These findings may reflect risk-averse decision-making in the setting of diagnostic uncertainty, where concern for rare but severe outcomes such as necrotizing otitis externa may drive overtreatment despite guideline recommendations.18,19
Clinician confidence in identifying necrotizing otitis externa varied widely in this study, with a substantial proportion of respondents reporting low confidence in recognizing early clinical signs. Because early NOE can present subtly and overlap with uncomplicated AOE, diagnostic uncertainty may prompt clinicians to adopt a more conservative or risk-averse treatment approach, particularly in patients with diabetes.20-22 This variability in confidence may partially explain the observed escalation in systemic antibiotic use despite guideline recommendations. The observed variability in clinician confidence may play an important role in treatment decisions. Lower confidence in recognizing early features of necrotizing otitis externa may contribute to increased use of systemic antibiotics as a precautionary strategy. This suggests that improving clinician confidence through targeted education may reduce unnecessary treatment escalation.
From a clinical and implementation perspective, the observed escalation in systemic antibiotic use is consequential. Systemic antibiotics provide no proven benefit in uncomplicated acute otitis externa and are associated with well-established risks, including adverse drug effects, antimicrobial resistance, and increased health care utilization.1,3-8,23-25 A nearly fourfold increase in systemic antibiotic exposure based solely on diabetes status suggests that a meaningful proportion of patients may be exposed to avoidable harm despite the availability of effective topical therapy. By quantifying this association, the present study moves beyond anecdotal concerns and identifies a clear target for antibiotic stewardship, clinician education, and decision support interventions aimed at reinforcing guideline-concordant management while supporting appropriate escalation when specific high-risk features are present.26-29 A substantial proportion of clinicians (44.8%) selected topical therapies that included corticosteroids, which may reflect additional variation in treatment selection; however, unlike systemic antibiotics, these therapies remain supported in many guideline-based approaches to acute otitis externa.1,3
Several limitations should be considered when interpreting these findings. First, the study relied on self-reported responses to hypothetical clinical scenarios rather than observed prescribing behavior, which may introduce recall bias or social desirability bias. Second, the sample size was modest and drawn from a single practice-based research network, potentially limiting generalizability to other clinical settings. Third, the survey did not assess clinicians’ reasoning in detail or capture whether specific clinical features suggestive of increased NOE risk influenced decision-making. Additionally, vignette-based responses may not fully reflect the complexity of real-world clinical encounters, where access to imaging, laboratory data, and specialist consultation may influence management decisions. Additionally, responses may have been influenced by social desirability bias, as clinicians may have selected treatment options they perceived to be expected or more defensible rather than those reflecting actual practice patterns. Finally, because each respondent evaluated both scenarios, responses were not independent, and future studies could apply paired analytic approaches such as McNemar testing to further refine effect estimates.
Despite these limitations, this study offers novel insight into real-world practice variation in the management of uncomplicated AOE in patients with diabetes. The findings highlight the need for clearer guidance and targeted educational interventions to support clinicians in risk stratification and early recognition of NOE while avoiding unnecessary systemic antibiotic exposure. Future research should include larger, multi-institutional studies and link survey data to de-identified prescribing patterns to better characterize actual clinical behavior. Qualitative studies exploring clinician decision-making and prospective observational designs may further clarify how perceived risk, diagnostic confidence, and patient factors interact to influence treatment escalation.18,19,30 Addressing this gap between perceived risk and evidence-based care represents a critical opportunity to improve antibiotic stewardship while maintaining patient safety.
Conclusion
Primary care clinicians reported significantly higher use of systemic antibiotics when managing uncomplicated acute otitis externa in patients with diabetes mellitus, despite guideline recommendations favoring topical therapy alone. Diabetes status was associated with a nearly fourfold increase in the risk of systemic antibiotic exposure, likely reflecting clinician concern for necrotizing otitis externa and uncertainty in early risk recognition. These findings highlight an important gap between evidence-based guidance and real-world clinical decision-making and underscore the need for clearer risk stratification tools, targeted education, and decision support to promote appropriate antibiotic use while ensuring prompt escalation for patients at true risk of complications.
Supplemental Material
Supplemental Material - Acute Otitis Externa Management in Patients With Diabetes: A Cross-Sectional Survey of Primary Care Clinicians
Supplemental material for Acute Otitis Externa Management in Patients With Diabetes: A Cross-Sectional Survey of Primary Care Clinicians by Brian Burroughs, Parivash Badar, Artika Misra, Nandita Ganne, Janel Tunison and Stephen K Stacey in Journal of Primary Care & Community Health.
Footnotes
Acknowledgments
The authors thank the clinicians who participated in the survey and the practice-based research collaborative for supporting survey distribution.
Ethical Considerations
This study was reviewed by the Mayo Clinic Institutional Review Board and determined to be exempt research under 45 CFR 46.104, Category 2. The IRB application number was 11-004811. Written informed consent was not required because the study was determined to be exempt by the Institutional Review Board. As protected health information was not requested from participants, HIPAA authorization was not required in accordance with 45 CFR 160.103.
Author Contributions
Brian Burroughs contributed to study conception and design, study implementation, data collection, data analysis and interpretation, manuscript drafting, critical revision, and final approval of the manuscript. Parivash Badar contributed to study design, critical revision, and final approval of the manuscript. Artika Misra contributed to study design and final approval of the manuscript. Nandita Ganne contributed to the final approval of the manuscript. Janel Tunison contributed to study implementation and final approval of the manuscript. Stephen K. Stacey contributed to study design, manuscript drafting, critical revision, and final approval of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.