
Abstract
Objective
Long COVID (LC) refers to the long-term symptoms occurring after SARS-CoV-2 infection and resolution of the initial disease prodrome. While LC is increasingly recognized, knowledge about its biomarkers is still limited. This study examines imaging findings in 18F-FDG PET-CT scans in 40 patients with LC from an academic LC Clinic, for potential imaging biomarkers.
Methods
This study included patients aged 18 and older with confirmed positive SARS-CoV-2 PCR test and at least 28 days post-symptom onset. 18F-FDG PET-CT scans were performed, and brain metabolic activity was compared to a control database to generate Z-scores. Participants were grouped based on their clinical phenotype and Z-scores of different brain regions were analyzed using t-tests.
Results
The study group was mainly female (70%), with a median age of 53 years, and predominantly non-Hispanic White (90%). Most had pre-existing conditions such as gastrointestinal, cardiovascular, endocrine, and psychiatric disorders. The findings showed significant cerebral hypometabolism in 29 patients with fatigue and post-exertional malaise (PEM), particularly in the left sensorimotor cortex (p=0.0253) and bilateral primary visual cortex (right: p=0.0096, left: p=0.0016), which persisted up to two years after infection.
Conclusions
In summary, this study identified persistent cerebral hypometabolism in LC patients, especially those with fatigue with PEM, up to two years post-infection. These results suggest that 18F-FDG PET-CT could be a valuable tool for diagnosing and managing LC. Further research is essential to confirm these findings and improve treatment strategies for patients with LC.
Introduction
Long COVID (LC), or ‘Post-acute Sequelae of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infection (PASC),' is a complex condition marked by persistent and severe symptoms following a SARS-CoV-2 infection. 1 It is estimated that between 10% to 48% of individuals recovering from acute Coronavirus Disease 2019 (COVID-19) experience prolonged symptoms, irrespective of the severity of the initial infection.1-5 These symptoms include fatigue, dyspnea, cognitive issues, joint pain, palpitations, myalgia, disturbances in smell and taste, cough, headaches, gastrointestinal changes, and cardiac problems. 6 LC is not confined to individuals who required intensive care unit admission; it also manifests in those with milder forms of the disease. 7 These symptoms underscore the intricate nature of this condition, emphasizing the need for additional research and clinical guidance to effectively diagnose and treat this challenging illness.
Despite the recognition of LC over the past few years, there remains a substantial dearth of reliable and accessible biomarkers. Recent studies on patients with LC demonstrate elevated inflammatory biomarkers post-initial infection, however there is still limited data on imaging biomarkers. 8 Emerging insights into immune profiling, neurohormonal signaling, and residual SARS-CoV-2 substrates are yet to transition to clinical applications.1,9-14 Though imaging has some utility in acute COVID-19, particularly pulmonary radiographs and CT scans, standard imaging generally has limited utility in LC, aligning with other infection-associated chronic illness15-24 This absence of objective abnormalities can be frustrating for patients and clinicians, despite the evident impact on quality of life.1,25-27
Advanced imaging has presented new opportunities for understanding LC. Brain MRI studies conducted via a UK biobank have shown compelling evidence of gray matter changes, tissue damage, and a reduction in global brain size following COVID-19 infection, and functional MRI studies on patients who have had COVID-19 have exhibited decreased functional activity in multiple brain regions.28-30 Several recent studies have demonstrated white matter changes on MRI in patients with LC with cognitive changes, as well as changes in cerebral blood flow and altered brain connectivity.31-36 Recent functional neuroimaging utilizing functional MRI (fMRI) and positron emission tomography (PET) technology has revealed signs of neuroinflammation in populations affected by conditions such as fibromyalgia (FM) and myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS).37-39 In one study, two patients with confirmed cognitive symptoms and brain fog underwent neuropsychological tests. Cerebral 18F-FDG PET scans indicated dysfunction in the cingulate cortex, despite normal MRI results. Patient 1 displayed widespread hypometabolic regions, affecting the cingulate cortex, precuneus, and other cortical areas, while patient 2 exhibited localized dysfunction in the cingulate cortex. This underscores the significance of exploring metabolic abnormalities in understanding cognitive symptoms when conventional imaging appears normal. 7 Another study described significant hypometabolism of patients with LC on 18 F-FDG PET scans obtained within the first 6 months of persistent symptoms (on average 97 days post infection). 40 Hypometabolic findings were also noted in whole-body 18F-PET-CTs conducted in 13 participants with LC in Italy, four of whom were also found to have persistent lung damage. 21
To address the burgeoning number of patients with LC during the first year of the COVID-19 pandemic, our institution established a specialized LC Clinic.Comprising of a multidisciplinary team, including physicians, scientists, nurses, and therapists, the clinic aims to cater to the diverse needs of individuals grappling with persistent symptoms post-recovery from COVID-19. Building upon our prior investigation involving a 59-year-old female patient with LC with normal MRI findings but abnormal 18F-FDG PET-CT brain imaging, 41 our present study outlines the 18F-FDG PET scans of 40 participants with LC seen and diagnosed in our clinic. Due to abnormal functional neuroimaging findings observed in conditions sharing symptomatic similarities, such as ME/CFS and fibromyalgia (FM), our research was centered around brain PET scans seeking to identify distinctive patterns that could serve as diagnostic or therapeutic biomarkers in patients with LC.
Methods
This was an observational cohort study conducted between December 2021 and February 2023. Approval was obtained from the institutional review board (IRB) with additional review by the Radiology overview committee to ensure appropriate risk reduction in the study protocol with IRB number 21-002870. Written informed consent was obtained from all participating subjects prior to study initiation. Study inclusion criteria were defined as age ≥18 years, having a documented positive SARS-CoV-2 PCR test, and being ≥28 days after onset of symptoms or date of test if initially asymptomatic with no upper limit of illness duration. Participants who reported being pregnant were excluded. A total of 46 study participants were subsequently invited to undergo 18F-FDG PET-CT of the brain through the LC Clinic, of which 45 proceeded with testing. Participants were divided into the primary phenotypes used in the LC Clinic - fatigue, orthostasis, and myalgia/arthralgia correlating to the known post-infectious conditions ME/CFS, postural orthostatic tachycardia syndrome (POTS), and FM, respectively.
18F-FDG PET-CT scans utilized in this study were performed at the same campus of the LC Clinic. Following a standard protocol, images were reconstructed using standard procedures and attenuation correction using CT-based attenuation map. Per our institutional standard, the 18F-FDG activity at the pons was used as the standard for normalization of the other areas of the brain, which is based on data suggesting that the metabolic activity of the pons is not significantly affected by aging or neurodegenerative diseases. 42 Using the pons as the reference point, additional post-processing was performed to create Z-score maps comparing each scan to an age- and gender-matched normal control database (Cortex ID software, GE Healthcare).
Data was supplemented with previously collected demographic and laboratory results and did not require additional testing beyond the 18F-FDG PET imaging. Data was deidentified using study-specific identification numbers assigned to individual participants. Data was stored on the secure institutional server and accessed only by individuals conducting and performing analysis for the study.
Statistical Analysis
Participants were grouped according to whether fatigue with post-exertional malaise was a predominant feature of their LC (fatigue with PEM; LC-PEM) or if it was not (non-PEM). The Z-scores were analyzed for normality using Shapiro-Wilk test and then using an ANOVA t-test with repeated measures and Bonferroni correction for multiple comparisons and p-values were considered significant if <0.05.
Results
A total of 45 PET-CTs were performed with the current the research protocol. One participant was excluded as they were found to have metastatic brain cancer from a known malignancy predating their COVID illness. Four were referred to a separate registry as they had predominantly POTS symptoms with a positive tilt table test (Figure 1). As with our prior studies, the population was female-predominant with 31 participants being female (70%). Ages ranged from 26 to 78 with a median age of 53 years with an interquartile range of 18.5 years. The majority of participants were non-Hispanic White (36/40; 90%). Demographic data and clinical phenotypes are outlined in Table 1. Patient flow diagram Demographics and Comorbidities of Current Study Population *median. **interquartile range (IQR).

Baseline health characteristics and vaccination history were also explored. The most common pre-existing categories of medical conditions were gastrointestinal (most commonly irritable bowel syndrome and gallbladder disease), cardiovascular (most commonly high blood pressure and high cholesterol), endocrinology (most commonly thyroid disease and hysterectomy/oophorectomy), and psychiatric (most commonly depression and anxiety), allergies, and obesity (Table 1).
Of the participants with LC who had a PET-CT scan performed, 29 (73%) had LC-PEM (defined as increase in symptoms or onset of new symptoms following exertion, often after a characteristic 24-hour delay 43 ) and 11 (27%) did not. Length of time from initial COVID-19 symptoms or diagnosis to PET imaging study ranged from 17 to 149 weeks, with a median duration of 62 weeks (IQR 49 weeks). The average number of weeks until scan was 63 weeks (IQR 39.5 weeks) in those with LC- PEM versus 62 weeks (IQR 57 weeks) in those in the non-PEM group, which was not statistically significant (p=0.46).
Distribution of Cerebral Metabolism in Participants With Fatigue With PEM Versus Those Without PEM
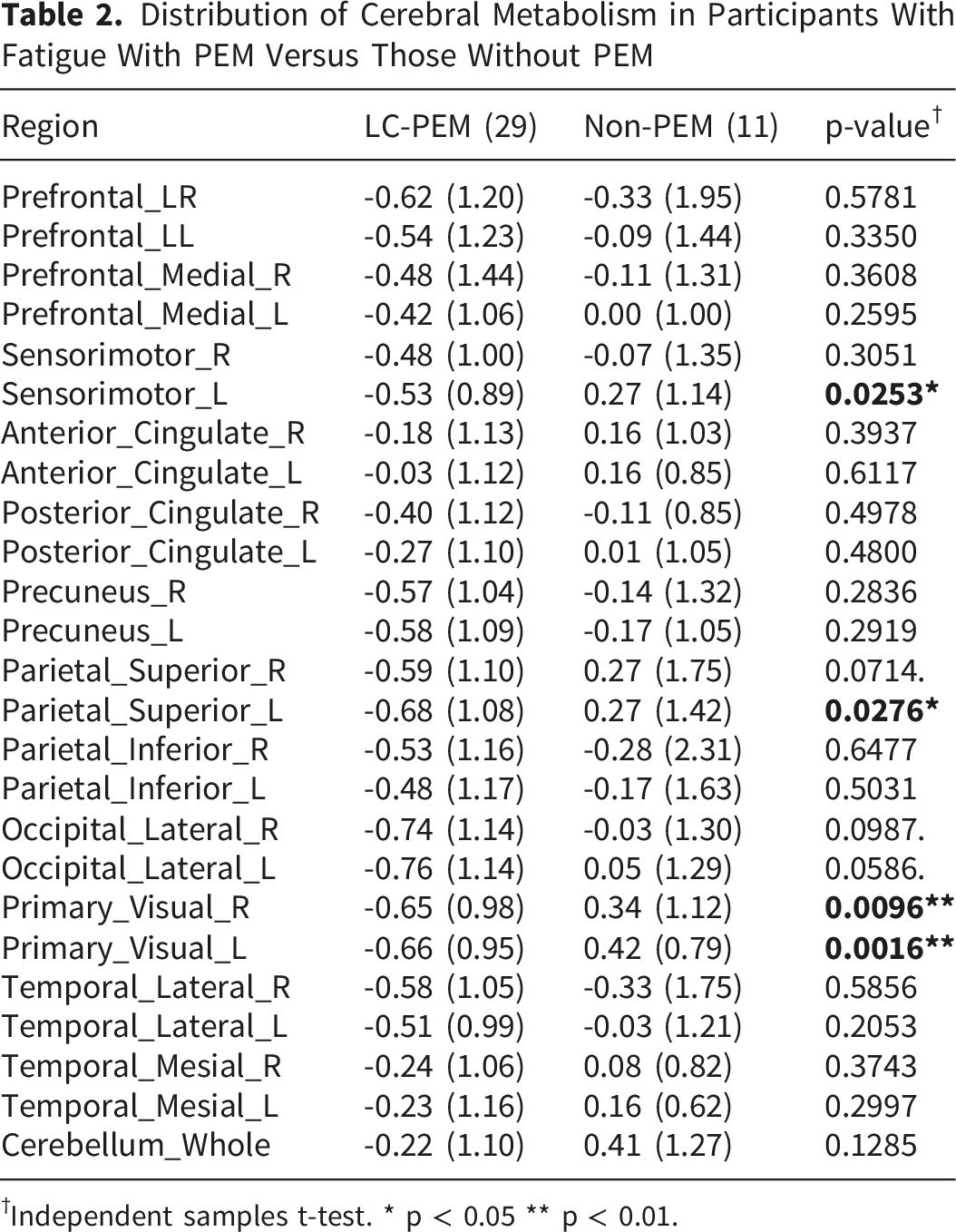
†Independent samples t-test. * p < 0.05 ** p < 0.01.

Representative 18F-FDG PET scan for a patient with Long COVID showing cerebral hypometabolism. The scan above shows the unprocessed 18F-FDG PET scan of the brain, and the below image has been processed to demonstrate the comparison to the age- and gender-matched normal database using the pons to normalize the comparison. This scan shows near global hypometabolism particularly pronounced in the occipital lobes, correlating with the participant’s symptoms of cognitive dysfunction and fatigue with post exertional malaise
Discussion
Here we report our findings of abnormal 18F-FDG PET-CT scans in patients with LC, highlighting their potential utility as a diagnostic tool for patients with LC, particularly those with a significant fatigue and PEM component. While many studies have investigated persistent symptoms and clinical manifestations in individuals recovering from acute COVID-19, the role of imaging in understanding the underlying pathophysiology of LC has remained largely underexplored. This study utilizes the population seen in a specialized LC clinic which performs comprehensive multidisciplinary evaluation of participants, incorporating clinical, laboratory, and imaging data to characterize the distinct phenotypes within the LC population, which in turn, direct treatment. Through the addition of the 18F-FDG PET scans of the brain, we gain insight of cerebral hypometabolism as a potential cause of LC symptoms.
Our study demonstrates similar hypometabolic patterns on brain 18F-FDG PET-CT scans to those reported previously, particularly in patients with predominant fatigue symptoms. 40 Our study further characterized this research by delineating specific phenotypes of LC, including LC-PEM, providing information on differences in neuroimaging patterns by symptom cluster phenotype. Our study additionally demonstrates persistence of hypometabolism well beyond 6 months from initial infectious symptoms, with the longest time to PET scan in our population being 4x greater than the previously reported longest duration of symptoms of 155 days to scan. The predominance of cerebral hypometabolism in patients with PEM draws important corollaries to similar changes seen in patients with FM and ME/CFS in prior neuroimaging studies. 22 The correlation of the symptom clusters and cerebral hypometabolism between LC and ME/CFS, particularly in those with PEM, suggests similar underlying pathophysiology.
In our study, we emphasize the abnormalities seen in PET scans among participants with LC, with persistent cerebral hypometabolism demonstrated across multiple phenotypes beyond six months on 18F-FDG PET imaging.40,44 Notably, reported brain fog and cognitive symptoms aligned with the observed dysfunction of the cingulate cortex, which has been linked to episodic memory deficits and abnormal executive and attentional functions. 7 Similarly, hypometabolism has been identified in multiple cortical regions in patients with severe COVID-19 which has been postulated to be related to hypoxia and neuroinflammation.7,44 These studies emphasize the significance of 18F-FDG PET scans in evaluating brain metabolism, particularly the integrity of the cingulate cortex, to guide cognitive remediation in COVID patients developing neurocognitive disorders. The hypometabolism seen in our data correlate with the neurocognitive disorders seen in patients with LC.
Our study does have several important limitations. The absence of longitudinal 18F-FDG PET assessments makes it difficult to comment on the persistence of findings within a single individual and hence reduces the internal validity of our findings and does not allow for any correlation with clinical progression for use as a therapeutic biomarker. The comparisons were made to an existing national age- and gender-matched normal control database which predated the COVID pandemic. As a result, the comparison group is by definition not Long COVID specific and does present the potential that other confounders could have been missed. There are also potential considerations related to reproducibility of our findings as all participants were tested at the Rochester campus, which does raise concerns about the generalizability to patients with limited access to care. As a result of the single-center cohort, this may result in limitations in data extrapolation to other geographic and ethnic areas, but the similarity to the findings demonstrated in other studies is very reassuring.7,40,44 There are also limitations in generalizability of our data as neither our study or other contemporary studies have included patients with LC and severe PEM as these patients are often homebound and unable to come in for testing. Data is conflicted as to whether the pons is metabolically involved in patients with LC, but were the pons to be metabolically involved, it would be an inappropriate comparison for normalization, affecting the geographic location, magnitude, and direction of effect. This will need to be confirmed in future studies. Lastly, given that we simultaneously performed multiple comparisons between brain regions, there is a recognized potential for false positives. Future studies in this arena would benefit from either comparison of a smaller number of variables defined a priori based on the existing literature or using a statistical method for multiple comparisons such as the Bonferroni correction. Despite these limitations, this study does have several strengths including a well-defined and well-phenotyped participant group and consistent imaging practices, which provides a robust foundation for future research endeavors in the complex landscape of LC.
These findings do provide the foundation for future investigation. One potential direction involves evaluating the utility of cerebral 18F-FDG PET-CT scans as a therapeutic biomarker to evaluate responses to treatment in patients with LC based on distinct neuroimaging patterns. By understanding how these patterns evolve with different interventions, we could tailor more effective and targeted therapeutic strategies. Furthermore, our study prompts the investigation of 18F-FDG PET-CT neuroimaging as a potential diagnostic biomarker for LC. By establishing a biomarker for LC, patients who are struggling with this ‘invisible illness’ could be diagnosed quickly and easily prompting early access to interventions, thereby improving outcomes and patient experience. Identification of key areas of the brain which are involved in LC may offer glimpses into potential pathophysiology, which may allow for development of targeted therapies. Future directions for this research will also include use of novel nuclear medicine isotopes including [11C]ER-176 which is specifically targeted to detect glial inflammation. 45
Conclusion
This study reports persistent cerebral hypometabolism on 18F-FDG PET-CT in a highly phenotyped cohort of 40 participants seen in a Long COVID clinic. These changes have been previously reported in the literature at 6 months post COVID-19 infection, but our data shows that this cerebral hypometabolism persists 2 years post COVID-19 infection. Our study additionally redemonstrates the correlation with fatigue and PEM as a predominant symptom. Further studies are recommended to validate the potential use of 18F-FDG PET-CT as a diagnostic and therapeutic biomarker for participants with LC.
Footnotes
Acknowledgments
The PCOCC study team would like to thank the Division of General Internal Medicine for their support of this project, our research coordinator team Shawn Fokken, Jennifer Hanson, and Megan Erickson for their significant investment of the time and effort into our LC Research. This work was funded in part by Mayo Clinic Department of Medicine, Division of General Internal Medicine. Finally, a special thanks to all study participants - without their participation, this study would not have been possible.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This work was supported by the Division of General Internal Medicine at the Mayo Clinic in Rochester, MN and the GHR Foundation in Minneapolis, MN. RTH is a paid consultant for Nestle. The remaining authors report no conflicts of interest.