
Abstract


Introduction:
Robotic Partial nephrectomies (PNs) for early-stage renal tumors have become increasingly popular in comparison to laparoscopic nephrectomy, for their shorter warm ischemia time, lower rates of conversion to open surgery, and higher preservation of renal function. However, vascular injury during PN is a potentially disastrous complication with limited literature on its specific management. We present a PN case to depict the role of co-piloting between the primary surgeon and assistant for minimizing intraoperative blood loss.
Methods:
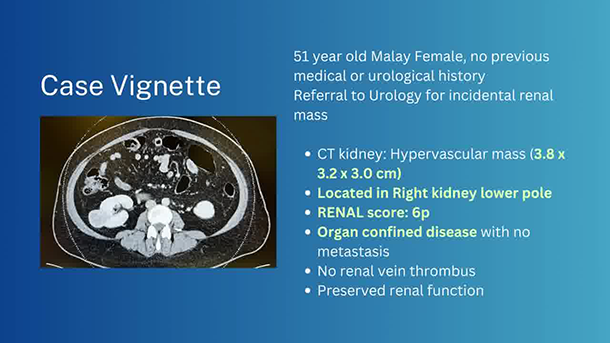
We present events during a single robotic right PN for a 3.8 cm R kidney confined lesion performed by a Urology consultant and a single assistant (Urology registrar).
Results:
Intraoperatively, varying degrees of intraoperative bleeding were encountered, most notably an inadvertent tear of the renal vein during hilar dissection. We describe a systematic step-wise approach when venous bleeding is encountered: increasing pneumoperitoneum, combined effort to ensure adequate visualization, tamponade with gauze, use of clips, and suture repair of the affected vessel. The patient had a smooth postoperative journey; follow-up computed tomography scans showed no development of pseudoaneurysm or recurrence, and renal function was preserved.
Discussion:
Teamwork between the surgeon and assistant is critical to minimize complications and blood loss intraoperatively. The process starts pre-operatively with careful review of imaging. Cultivating the habit of regular communication mitigates uncertainty in approaching intraoperative bleeding. Patient safety is paramount, so conversion to open surgery should not be considered as a failure by the surgical team.
Patient Consent Statement:
All authors have received and archived patient consent for video recording/publication in advance of video recording of the procedure.
We do not have any commercial associations during the last 2 years. We do not have any conflict of interest in connection with the video.
Runtime of video: 5 mins 4 secs