
Abstract
Background:
Early-life viral lower respiratory tract infections (LRTIs), particularly those caused by respiratory syncytial virus (RSV) and human rhinovirus (HRV), are major contributors to pediatric morbidity and are strongly linked to asthma. RSV causes about 3.6 million hospitalizations and 100,000 deaths annually in children under 5, mainly in low- and middle-income countries. RSV peaks in infancy, while HRV has more impact later in childhood. Mechanisms include viral epithelial injury, genetic susceptibility (e.g., 17q21 variants), and environmental factors (e.g., allergic sensitization). Together, these raise asthma risk. Diagnosis is difficult due to overlapping presentations and reliance on molecular tests. Preventive strategies include maternal RSV vaccination, long-acting monoclonal antibodies such as nirsevimab and palivizumab, and pediatric vaccine candidates. Strategies to limit allergic sensitization may lower HRV-related asthma risk. Long-term effects include persistent wheeze and asthma, making early life a crucial window for prevention.
Methods:
This review summarizes current evidence on the epidemiology, mechanisms, and long-term impact of early viral LRTIs.
Results:
It highlights molecular and immunological endotypes of virus-induced asthma and explores the influence of genetic, epigenetic, and microbial factors. Emerging diagnostic tools and preventive strategies—including vaccines, monoclonal antibodies, environmental interventions, and microbiome-targeted therapies—are also discussed as means to reduce the global pediatric asthma burden and improve respiratory health.
Keywords
Introduction
Childhood respiratory diseases represent a major global health challenge, with viral lower respiratory tract infections (LRTIs) caused predominantly by respiratory syncytial virus (RSV) and human rhinovirus (HRV) contributing substantially to morbidity and hospitalization worldwide.1–3 These infections occur during a critical window of lung and immune system development, during which virus-induced epithelial injury and host immune responses can exert long-lasting effects on respiratory health.4,5 RSV is the leading cause of severe respiratory infection in infancy, infecting nearly all children by the age of 2 years, and early-life RSV infection has been consistently associated with recurrent wheezing and an increased risk of childhood asthma.6,7 Similarly, HRV infections during the first 3 years of life are important triggers for asthma onset, particularly in children with underlying genetic susceptibility or early wheezing phenotypes.8–10 In this review, “endotypes” refer to asthma subtypes defined by distinct underlying molecular and immunological mechanisms rather than clinical features alone.
Other respiratory viruses, including human metapneumovirus, influenza viruses, coronaviruses, and adenovirus, can also cause LRTIs in infancy and early childhood. However, RSV and HRV have the strongest and most consistently demonstrated associations with subsequent recurrent wheeze and asthma development, and therefore remain the primary focus of this review. 3
The pathogenesis of virus-associated asthma reflects complex interactions among viral replication, airway epithelial disruption, host genetic predisposition, and environmental exposures such as allergic sensitization.5,9,10 These factors do not act in isolation; viral infections in early life can alter epithelial development and immune programming, leading to persistent changes in barrier integrity and immune regulation that extend beyond the acute illness. 4 As a result, these alterations increase vulnerability to aeroallergens and environmental pollutants and contribute to the onset and severity of asthma later in childhood.10–12 This challenge is especially pronounced in low-resource settings, where access to diagnostics and preventive interventions is limited.13–15
This review examines current evidence on the epidemiology, pathogenesis, and long-term respiratory consequences of early-life RSV and HRV infections. It also discusses emerging diagnostic approaches, preventive strategies such as monoclonal antibodies and vaccines, and future directions to reduce childhood asthma and improve pediatric respiratory outcomes.
Epidemiology and Public Health Impact
Viral lower respiratory tract infections (LRTIs) in infancy, primarily caused by RSV and HRV, represent a substantial global health burden.1,2,16,17 For example, RSV alone accounts for approximately 3.6 million hospitalizations and nearly 100,000 deaths annually in children under 5, with the highest rates in infants younger than six months and in low- and middle-income countries where access to advanced supportive care is limited.1,2,13,18 In addition, HRV contributes substantially to pediatric respiratory morbidity and wheezing illnesses.3,8–10
Geographic and socioeconomic disparities strongly influence the incidence and outcomes of viral LRTIs.13,19 Specifically, infants from disadvantaged backgrounds experience higher rates of infection and persistent respiratory symptoms due to exposures such as indoor air pollution, secondhand smoke, and substandard housing.13,19 Supporting this, population studies indicate that infants from low-income families can have a substantially higher incidence of lower respiratory illnesses compared with those from wealthier households.13,20 Furthermore, secondhand smoke is a well-established risk factor that exacerbates respiratory symptoms, increases asthma attacks, and impairs lung growth in children.11,20,21
Environmental and social determinants—including biomass fuel use, overcrowding, malnutrition, and limited healthcare access—further increase the risk and severity of viral LRTIs, contributing to both acute morbidity and long-term sequelae such as asthma.13,19,20 Addressing these disparities through public health measures is critical to reducing the global burden of pediatric respiratory disease. Seasonal RSV epidemics create surges in pediatric admissions, particularly in temperate climates during fall and winter.22,23 During and immediately after the COVID-19 pandemic, non-pharmaceutical interventions and altered population immunity led to atypical out-of-season RSV activity, but in many regions, seasonal patterns have largely returned toward pre-pandemic winter peaks.24,25
Pathophysiology and Disease Mechanisms
Early-life RSV and HRV infections trigger complex processes predisposing children to chronic respiratory conditions, especially asthma. Beyond acute bronchiolitis or wheezing, these viruses disrupt lung development by inducing repeated epithelial injury, impairing alveolarization, and triggering inflammatory cascades, leading to long-term structural changes and reduced lung function.4,5,26
At the cellular level, RSV infects airway epithelial cells and spreads from the upper to the lower airways. Disease severity is greater with tobacco smoke, indoor pollutants, or aeroallergen exposure, which intensify inflammation and impair repair.8,10,11,19 Genetics adds further variation. Inflammatory signaling persistence, when unresolved, drives smooth muscle hypertrophy, fibrosis, and goblet-cell metaplasia, sustaining airflow limitation. Neonatal epithelial cells are especially vulnerable; infants who develop asthma often show reduced epithelial integrity and repair. Neonatal RSV models show enlarged alveolar spaces, reduced compliance, and persistent peribronchiolar inflammation resembling chronic asthma.4,5
The immunological response during early infection is equally pivotal. Dendritic cells and group 2 innate lymphoid cells orchestrate a type 2–biased immune response characterized by upregulation of epithelial alarmins such as thymic stromal lymphopoietin and interleukin-33 (IL-33).27,28 These cytokines amplify mucus hypersecretion and airway hyperreactivity during reinfections, thereby establishing a mechanistic link to asthma susceptibility.4,27,28 Severe RSV infections consistently skew immunity toward a Th2 phenotype, with elevated IL-4, IL-5, IL-13, and IL-33, coupled with reduced interferon-γ responses.28,29 This imbalance reinforces airway hyperresponsiveness, goblet-cell hyperplasia, and mucus overproduction.28,29 Such immune polarization highlights the importance of targeting both antiviral and immunomodulatory pathways in prevention strategies. These early immune shifts likely contribute to durable, endotype-specific trajectories (e.g., Th2-high versus mixed or non-Th2 phenotypes).30,31
Host genetic background strongly influences individual susceptibility. Twin and family studies estimate asthma heritability between 36% and 79%, and genome-wide analyses have identified more than 100 associated loci.10,32 Among these, the 17q21 locus—encompassing ORMDL sphingolipid biosynthesis regulator 3 and interleukin 1 receptor-like 1—shows a pathogen-specific association, with a strong and reproducible link to early-life HRV-induced wheezing and subsequent asthma.7,8,10,32 In contrast, associations with RSV appear indirect, relating primarily to asthma development following severe RSV bronchiolitis rather than to RSV susceptibility or severity, and direct mechanistic links remain limited. 6 HRV therefore acts not in isolation but through interactions with host genetics to drive persistent asthma trajectories. Differences in genetic association between RSV and HRV should not be overinterpreted, as available evidence is largely observational and reflects interactions among infection timing, disease severity, allergic sensitization, and asthma susceptibility rather than direct virus-specific genetic effects.6,8,9,33 Additional loci linked to immunoglobulin E-mediated atopy, epithelial barrier function, and innate immunity further underscore the multifactorial nature of risk.10,32
Allergic sensitization substantially modifies virus–asthma relationships in a pathogen-specific manner. In a high-risk birth cohort, early-life wheezing with HRV during the first 3 years, particularly in children with aeroallergen sensitization by 1 year of age, was associated with markedly increased odds of asthma persisting into adolescence, indicating a synergistic interaction between HRV infection and atopy.7,8,10,32 By contrast, population-based studies of RSV show that timing and severity of infant RSV infection, rather than early allergic sensitization, are more strongly linked to later asthma; infants who remained uninfected with RSV in the first year of life had a substantially lower risk of asthma at preschool age than those infected in infancy.18,33 Together, these findings support a model in which HRV-driven asthma risk is amplified by early allergic sensitization, whereas for RSV, the severity and timing of infection are key determinants of long-term outcomes.
Although severe early-life RSV and HRV infections are consistently associated with increased risk of recurrent wheeze and asthma, it remains uncertain to what extent these infections act as causal drivers versus markers of underlying susceptibility.8,9,18 Available data suggest that illness severity, shared genetic predisposition, and environmental exposures may be at least as important as viral etiology, and randomized or quasi-experimental studies capable of definitively separating causality from association remain limited.6,8,33 Similarly, current asthma endotyping and phenotyping frameworks, which largely emphasize Th2 biomarkers and eosinophilic inflammation, do not fully capture the spectrum of post-viral asthma, particularly non-Th2 or mixed inflammatory endotypes.27,32,34,35
These mechanistic steps are supported by human cohort observations linking early viral exposures to later wheeze and asthma. Birth cohort and longitudinal studies have shown that severe RSV bronchiolitis in infancy is associated with an increased risk of recurrent wheeze and childhood asthma,6,18,33 while recurrent HRV-associated wheezing illnesses in the first years of life—especially in children with early allergic sensitization—strongly predict persistent asthma into later childhood and adolescence.7,8 Consistent with these clinical trajectories, human studies report patterns of type 2–skewed inflammation and related biomarkers in subsets of infants and children following early viral LRTIs, supporting the concept that early epithelial injury and alarmin-driven immune programming contribute to durable, heterogeneous asthma endotypes as summarized in Figure 1.27,28,32

Molecular and immunological pathways linking early-life viral infection to asthma endotypes. Early-life respiratory syncytial virus (RSV) and human rhinovirus (HRV) infections damage airway epithelium, leading to the release of alarmins such as thymic stromal lymphopoietin (TSLP) and interleukin-33 (IL-33). These cytokines activate dendritic cells and innate lymphoid cells, driving differentiation of naïve CD4+ T cells into Th2 and Th17 subsets. The Th2 pathway promotes eosinophilic inflammation through IL-4, IL-5, and IL-13, contributing to allergic asthma. The Th17 pathway induces IL-17 and epithelial IL-8 production, recruiting neutrophils and contributing to non-Th2 asthma phenotypes. Genetic susceptibility loci (e.g., 17q21), epigenetic modifications, and virus-induced microbiome alterations regulate these immune pathways and contribute to asthma heterogeneity. Created with BioRender.com.
A direct comparison of RSV and HRV features is presented in Table 1, which summarizes their epidemiological, pathogenic, and immunological differences. This comparison highlights that RSV is strongly linked to severe bronchiolitis in early infancy, whereas HRV is more closely associated with wheezing episodes in later childhood and with asthma risk in children who have underlying allergic sensitization or specific genetic backgrounds.7,8,10,32
Comparison of Respiratory Syncytial Virus and Human Rhinovirus in Early-Life Lower Respiratory Tract Infections and Asthma Risk
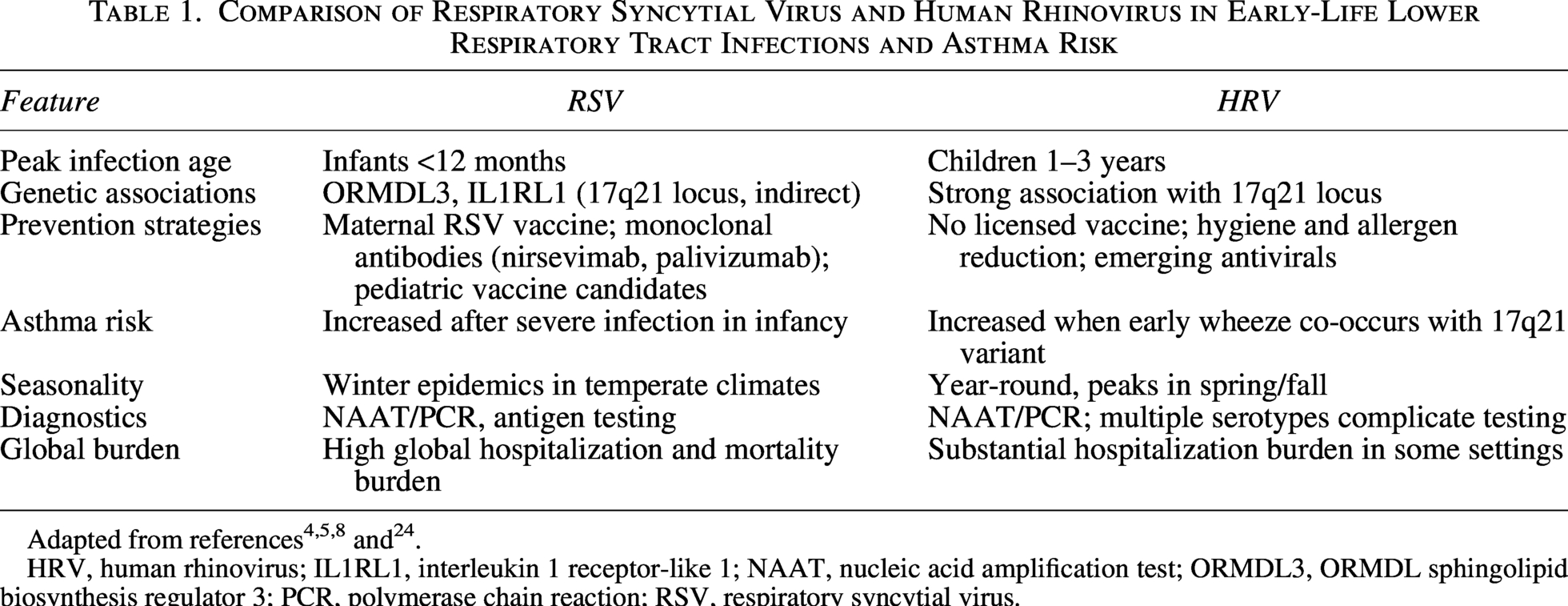
HRV, human rhinovirus; IL1RL1, interleukin 1 receptor-like 1; NAAT, nucleic acid amplification test; ORMDL3, ORMDL sphingolipid biosynthesis regulator 3; PCR, polymerase chain reaction; RSV, respiratory syncytial virus.
Epigenetic modifications—including DNA methylation, histone remodeling, and microRNA regulation—further refine gene–environment interactions by reprogramming immune and epithelial cells in response to viral, allergen, or pollutant exposures.10,32,36 These modifications act as molecular “memory marks,” sustaining the effects of early exposures to viruses, allergens, or pollutants. For example, altered methylation at loci within 17q21 or cytokine gene promoters can maintain a pro-inflammatory or Th2-skewed immune profile long after acute infection has resolved.32,36 Epigenetic programming therefore provides a mechanistic link between transient viral insults and persistent asthma endotypes.10,32
Early-life viral infections also reshape the airway microbiome, which plays a central role in calibrating immune responses. A balanced microbial community supports tolerance, whereas virus-induced dysbiosis—such as enrichment of Streptococcus or Moraxella—is associated with recurrent wheeze and increased asthma risk.37–39 Virus–bacteria interactions are bidirectional: bacteria can enhance viral replication by damaging epithelial barriers, while viruses alter the ecological niche to favor bacterial overgrowth.36,38,40 These interactions highlight that pathogens should not be studied in isolation, as disease trajectories are shaped by the combined influence of microbial consortia and host factors. Longitudinal, integrative studies that track children from birth through early life are needed to clarify causal relationships between viral infections, immune programming, and microbiome alterations.4,41
Prevention Strategies
Preventing asthma following early-life RSV and HRV infections requires a multi-layered approach that integrates immunization, environmental interventions, microbiome modulation, and strategies to overcome systemic barriers to care.42–45 These approaches are most effective when implemented in combination, with particular emphasis on high-risk and underserved populations.13,20
Current emerging vaccines
Pediatric RSV vaccine candidates—including live-attenuated, subunit, and mRNA platforms—are advancing rapidly in clinical development, with several demonstrating robust immunogenicity and favorable safety profiles.42,46,47 Live-attenuated vaccines induce mucosal immunity in infants, while protein-based and mRNA platforms provide scalable options suitable for combination strategies.42,46 Maternal RSV vaccination reduces infant illness via transplacental antibody transfer and offers immediate neonatal protection during the highest-risk period. 48 This approach bridges the gap until infant-directed vaccines achieve optimal coverage.
Differentiating between long-term asthma risk reduction and short-term prevention of severe RSV disease is crucial. Although maternal vaccination and monoclonal antibodies have proven effective in lowering acute morbidity and severe RSV-related hospitalizations,48,49 it remains unclear how they will affect the development of long-term asthma. Available data suggest that preventing severe RSV infection during infancy may reduce the risk of asthma and recurrent wheezing,6,33 but confounding variables such as shared genetic susceptibility and environmental exposures limit the ability to draw firm conclusions regarding causality.8,9,18 Separating the prevention of acute infection from the modulation of chronic asthma pathways therefore remains a major challenge, as emphasized in prior reviews.
Monoclonal antibodies have become a cornerstone of passive immunization. Nirsevimab has demonstrated significant efficacy against severe RSV disease in both preterm and term infants, offering single-dose seasonal protection.48,49 These advances expand preventive coverage beyond the limited eligibility criteria of earlier agents such as palivizumab.48,49 In the United States, average wholesale price estimates have historically been several thousand US dollars per vial for palivizumab, with estimates exceeding 2,000 USD for a 50-mg vial and 4,000 USD for a 100-mg vial, which has limited its use to narrowly defined high-risk groups. 50 By contrast, nirsevimab is supplied as 50-mg and 100-mg prefilled syringes with an average wholesale price of approximately 594 USD for either dose, representing a substantial per-dose reduction relative to palivizumab and improving the feasibility of broader infant prophylaxis programs.50–52 However, ensuring equitable access in low- and middle-income countries remains a major challenge, given the disproportionate RSV burden in these regions.1,2,18
In contrast, HRV prevention remains limited due to the virus’s antigenic diversity and the large number of circulating serotypes.53,54 Vaccine development efforts focus on conserved capsid epitopes, including computationally designed multi-epitope candidates, 55 while antiviral therapies targeting viral proteases and replication machinery are under investigation.56,57 Despite these advances, practical HRV vaccines are not yet available, underscoring a key gap in preventive strategies for HRV-associated asthma.53–55,57
Public health measures to reduce exposure
Environmental and behavioral interventions remain critical to reducing the burden of viral LRTIs and their downstream consequences. Indoor allergen exposure, tobacco smoke, and socioeconomic barriers consistently worsen disease severity and increase the likelihood of chronic respiratory sequelae.11,19–21 Foundational preventive measures include allergen avoidance, smoke-free homes, improved ventilation, and reduction of household crowding.11,19,21
Nutritional interventions also play an important role. Breastfeeding provides passive immunoglobulins and bioactive molecules that support immune maturation and reduce the severity of viral illness.19,20,44 Vitamin D supplementation has been shown to improve epithelial barrier function and immune regulation, 44 while maternal omega-3 fatty acid supplementation during pregnancy has been associated with reduced asthma risk in offspring. 58 Community-based approaches—including school hygiene programs, parental education, and culturally tailored awareness campaigns—further reduce viral transmission and promote early care-seeking behavior.59,60
Microbiome-targeted interventions
The gut and airway microbiomes are increasingly recognized as key regulators of immune development, tolerance, and antiviral defense.45,61 Early dysbiosis—whether driven by viral infections, antibiotic exposure, or environmental factors—can promote exaggerated immune activation and long-term asthma susceptibility.39,45,62 Probiotic and synbiotic supplementation may enhance epithelial barrier integrity, modulate cytokine production, and strengthen regulatory T-cell responses, although results across studies remain inconsistent.39,45,63
Emerging precision approaches that integrate metagenomics, metabolomics, and other multi-omics platforms may enable targeted modulation of microbial networks in high-risk infants.36,64 While these strategies remain experimental, they represent a promising frontier for individualized prevention of virus-associated asthma.
Addressing barriers to immunization and preventive care
The impact of vaccines and monoclonal antibodies is constrained by socioeconomic disparities, vaccine hesitancy, and logistical challenges.13,20,49 In many low- and middle-income countries, limited healthcare infrastructure and out-of-pocket costs hinder access to preventive interventions, while inequities persist even in high-income settings.13,20,49 Integrating maternal and pediatric immunization into routine care, employing culturally tailored communication strategies to address hesitancy, and investing in supply chains and workforce training are critical for equitable delivery.49,60
Surveillance systems are essential for monitoring vaccine effectiveness and adapting immunization policies to shifting viral epidemiology.18,49 Strengthening surveillance and delivery platforms will maximize the population-level impact of preventive strategies.
In resource-limited settings, practical priorities include integrating maternal RSV vaccination and infant monoclonal antibodies into existing antenatal visits and childhood immunization schedules, empowering nurses and community health workers to deliver these interventions, and using simplified eligibility criteria to avoid missing high-risk infants.49,60 Pooled procurement mechanisms, tiered pricing agreements, and inclusion of RSV vaccines and monoclonal antibodies on national essential medicines lists can help reduce out-of-pocket costs. 49 Investments in cold-chain infrastructure, oxygen delivery systems, and pulse oximetry, along with embedding RSV surveillance into existing pneumonia or influenza platforms, are also critical to ensure that innovations reach children at greatest risk.13,18,49
Diagnosis and Surveillance
Diagnostic challenges in low-resource settings
The diagnosis of early-life viral LRTIs is not merely a matter of pathogen identification but a critical determinant of subsequent clinical management, resource allocation, and long-term outcomes. Gold-standard molecular methods such as reverse transcription polymerase chain reaction (RT-PCR) and multiplex PCR achieve sensitivities and specificities exceeding 90% for most respiratory viruses, making them indispensable in high-income settings for accurate diagnosis and surveillance.2,65 However, their reliance on advanced laboratory infrastructure, continuous electricity, and trained personnel limits their use in many low- and middle-income countries.13,14,65
In such settings, clinicians frequently rely on syndromic diagnosis based on nonspecific clinical features such as wheeze, tachypnea, or hypoxemia, or on rapid diagnostic tests.13,65 While rapid diagnostic tests offer speed and portability, their sensitivity varies widely, 64 leading to false-negative results that delay appropriate care and false-positive results that misdirect limited resources. This diagnostic uncertainty contributes to inappropriate antibiotic use, estimated to occur in a substantial proportion of pediatric viral LRTIs,13,15 and hampers effective infection control in hospital settings.
Advances in point-of-care diagnostics
Recent technological innovations aim to overcome infrastructure limitations by reducing turnaround time and dependence on centralized laboratories. Isothermal amplification methods, including loop-mediated isothermal amplification and recombinase polymerase amplification, enable nucleic acid detection at constant temperatures, eliminating the need for thermal cyclers.13,65 Cartridge-based platforms integrate sample preparation, amplification, and detection into closed systems suitable for use in low-resource environments. 13
Emerging clustered regularly interspaced short palindromic repeats-based assays offer single-nucleotide specificity and the ability to detect viral subtypes without complex instrumentation. 13 Additional platforms, including nanoparticle-enhanced lateral flow tests, microfluidic devices, and biosensors, provide portability and multiplexing capacity.13,65 Collectively, these advances move diagnostics closer to the point of care and may democratize access to reliable viral testing across diverse healthcare settings.
Biomarkers for early detection and prognosis
The diagnostic paradigm is expanding to include host-response profiling. Cytokine signatures—such as elevated IL-6, IL-8, and interferon-inducible protein-10—have been shown to correlate with disease severity, hospitalization duration, and risk of adverse outcomes. 29 Multi-biomarker panels and transcriptomic signatures are under evaluation to stratify risk and support rapid triage, particularly in overcrowded pediatric wards.36,65 These approaches shift diagnostics beyond pathogen identification toward prediction of clinical course and personalized management of viral LRTIs.
Surveillance systems for LRTIs
Robust surveillance systems are essential to guide prevention and treatment strategies.15,18,49 Global surveillance networks provide burden estimates that inform vaccine development, licensure, and public health policy.1,2,15 These data highlight the disproportionate impact of RSV in low- and middle-income countries, where limited access to supportive care contributes to high morbidity and mortality.1,2,18
Prospective cohort studies provide longitudinal insights linking early-life viral infections to chronic outcomes such as recurrent wheeze, asthma, and impaired lung growth.4,18,66 However, many high-burden regions lack sustained diagnostic infrastructure and trained personnel, creating gaps in real-time monitoring.13,15 Strengthening surveillance through integration of molecular diagnostics, digital reporting systems, and workforce training is critical for outbreak detection, preparedness, and long-term planning.15,18,49
Management and Treatment
Standard of care for acute LRTIs
The management of acute viral LRTIs in children is primarily supportive and guided by illness severity.66–68 Core interventions include oxygen supplementation to maintain adequate oxygen saturation, appropriate hydration, antipyretics for fever control, and airway clearance techniques when indicated.67,68 Specific antiviral therapies remain limited. For RSV, ribavirin has demonstrated variable efficacy and is rarely used in routine clinical practice, whereas neuraminidase inhibitors such as oseltamivir are standard for influenza.68,69
Antibiotic stewardship is essential in the management of viral LRTIs.13,70 Antibiotics should be avoided unless bacterial co-infection is suspected or confirmed, and empirical therapy should be guided by local resistance patterns with prompt de-escalation when bacterial infection is excluded.13,70
Personalized medicine approaches
Advances in diagnostics and immunology are enabling more precise management strategies.64,70 Multiplex PCR panels allow simultaneous detection of multiple respiratory viruses, 65 while host transcriptomic profiling can help distinguish viral from bacterial infections, thereby reducing inappropriate antibiotic use.64,70 Respiratory microbiome analyses have identified dysbiosis patterns—such as reduced microbial diversity or Streptococcus dominance—that predispose children to secondary bacterial infections and may serve as predictive markers.37,38,45
Pharmacogenomic and immunogenetic factors are also being investigated to identify children with heightened type 2 immune responses or impaired interferon signaling who may benefit from tailored anti-inflammatory or immunomodulatory interventions.10,32 While these approaches remain largely investigational, they represent an important step toward precision management of virus-associated respiratory disease.
Implementation barriers
Despite advances, significant challenges remain in clinical practice.13,15 Limited availability of rapid molecular diagnostics, seasonal surges that overwhelm pediatric wards, and resource constraints in low- and middle-income countries reduce the effectiveness of both supportive care and advanced therapies.13,15 These barriers contribute to inappropriate antibiotic prescribing, delayed antiviral use, and inconsistent oxygen delivery.13,15,70
Addressing these gaps requires multifaceted solutions, including task-shifting to trained community health workers, equitable immunization programs to reduce seasonal disease burden, and sustained investment in laboratory capacity, oxygen infrastructure, and healthcare workforce development.49,71 Embedding new diagnostic and therapeutic tools into resilient health systems is essential to ensure consistent, high-quality care across diverse settings.
Long-term outcomes and life course implications
Early-life RSV and HRV infections are strongly associated with recurrent wheeze and persistent asthma across childhood and adolescence.6–8,18 Severe RSV bronchiolitis in infancy and HRV-induced wheezing episodes in early childhood represent two of the most robust predictors of subsequent asthma development.6–8,18 Longitudinal cohort studies consistently demonstrate that children hospitalized with RSV during the first year of life have higher rates of recurrent wheeze and physician-diagnosed asthma in preschool and school-age years compared with uninfected peers.6,18,33 Similarly, HRV-associated wheeze in the first 3 years of life, particularly when recurrent, is strongly linked to asthma persistence into adolescence.7,8
Beyond asthma diagnosis, early viral LRTIs exert broader effects on lung growth and respiratory health.4,5,18 Children with severe early-life viral infections often exhibit reduced lung function trajectories, including lower forced expiratory volumes and increased airway hyperresponsiveness that may persist into adulthood.4,5,18,27 These impairments can limit exercise tolerance, increase susceptibility to respiratory infections, and contribute to chronic obstructive airway disease later in life.4,5 The cumulative impact of repeated viral infections during early childhood further amplifies these risks.
Socioeconomic and environmental factors critically shape long-term outcomes.13,19,20 Children from low-income households or those exposed to tobacco smoke, indoor air pollution, and overcrowded living conditions experience higher infection severity and poorer recovery.11,13,19 Limited access to early diagnosis, preventive interventions, and follow-up care further exacerbates disparities in respiratory outcomes.13,15,20 As a result, virus-associated asthma contributes to a cycle of health inequity that extends across the life course, emphasizing the need for early, equitable preventive strategies.
Future directions
Future progress in reducing virus-associated asthma risk will depend on integrating advances in basic science, translational research, and public health implementation. A key priority is the refinement of molecular and immunological endotypes that distinguish children who are most likely to progress from early viral infection to chronic asthma.10,27,32,34,35 Multi-omics approaches—including genomics, epigenomics, transcriptomics, proteomics, and microbiomics—offer unprecedented opportunities to define these endotypes and to identify predictive biomarkers during infancy.32,36,41,64
Longitudinal birth cohorts with detailed viral surveillance and extended follow-up into adolescence and adulthood will be essential to disentangle causality from shared susceptibility.4,41 Such studies can clarify whether preventing or attenuating early viral infections modifies long-term asthma trajectories or whether viral LRTIs primarily unmask underlying predisposition.8,9,33 Randomized trials of preventive interventions, including maternal vaccination and monoclonal antibodies, with long-term respiratory outcomes as predefined endpoints will be particularly informative.42,48,49,72
Implementation science must also play a central role.13,49 Even the most effective vaccines and diagnostics will have limited impact without equitable delivery.13,20,49 Future strategies should prioritize integration of RSV vaccines and monoclonal antibodies into routine maternal and pediatric care, expansion of point-of-care diagnostics in low-resource settings, and strengthening of surveillance systems to guide policy decisions.15,18,49 Community engagement and culturally tailored communication will be critical to addressing vaccine hesitancy and ensuring uptake. 60
Conclusion
Early-life viral LRTIs, particularly those caused by RSV and HRV, are major contributors to the global burden of childhood asthma.1–3 These infections intersect with genetic susceptibility,10,32 epigenetic programming,32,36 immune maturation,27,28 and microbiome development37–39 to shape long-term respiratory health. Advances in preventive strategies—including maternal vaccination,42,48 long-acting monoclonal antibodies,48,49,72 and emerging pediatric vaccines42,46—offer promising opportunities to reduce severe disease and potentially modify asthma risk.42,48,49 However, the extent to which these interventions prevent long-term asthma remains an active area of investigation.6,8,33
Integrating molecular endotyping with accessible diagnostic and preventive approaches is essential to identify high-risk children early and to deliver effective interventions across diverse healthcare settings.10,27,32,34 Addressing social and environmental determinants of health alongside biomedical innovation will be critical to reducing disparities and improving respiratory outcomes worldwide.11,13,19,20
Authors’ Contributions
S.A.: Conceptualization, methodology, investigation, writing—original draft, project administration. S.M.: Investigation, writing—review and editing. M.Y.: Investigation, writing—review and editing. A.A.: Resources, writing—review and editing. All the authors approved the final article.
Ethics Statement
Ethical review and approval were not required for this study in accordance with local legislation and institutional requirements. Written informed consent was not required as this is a narrative review of existing literature.
Data Availability Statement
No new data were generated or analyzed in this study.
Footnotes
Acknowledgments
The authors thank colleagues and mentors for their insights and contributions to the conceptualization of this work.
Author Disclosure Statement
The authors declare no commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
No financial support was received for the research, authorship, and/or publication of this article.