
Abstract
Introduction:
Oral mite anaphylaxis (OMA) is an uncommon form of food-induced anaphylaxis caused by ingestion of foods contaminated with house dust mites. Exercise may act as a cofactor, sometimes mimicking food-dependent exercise-induced anaphylaxis (FDEIA).
Case Presentation:
We describe a 14-year-old boy with atopic dermatitis, allergic rhinitis, and mild asthma who experienced three episodes of anaphylaxis. Each reaction occurred 30–60 min after eating wheat-based foods, followed by physical activities such as football or basketball. Symptoms started with urticaria and progressed to cough and abdominal pain. Notably, he tolerated the same foods in the absence of exercise. Skin prick testing and specific IgE showed strong sensitization to Dermatophagoides pteronyssinus and Dermatophagoides farinae, but not to wheat. Multiplex component testing confirmed broad mite sensitization. Evaluation for primary immunodeficiency was unremarkable. The patient was prescribed an epinephrine auto-injector, and asthma therapy was optimized with budesonide/formoterol. Over 6 months of follow-up, no further episodes occurred, asthma control improved (Asthma Control Test score 24–25), and rhinitis symptoms subsided with intranasal antihistamines.
Discussion:
The clinical picture, together with negative wheat-specific IgE and strong mite sensitization, supported OMA rather than classical food allergy or FDEIA. Component-resolved diagnostics were especially helpful in confirming the diagnosis.
Conclusion:
This case underlines the importance of considering OMA in children with exercise-related anaphylaxis after wheat-based meals, particularly in patients who may initially appear to have idiopathic anaphylaxis. Careful history, use of CRD, and close follow-up are essential. Education, asthma control, and preventive measures remain key to reducing recurrence risk.
Introduction
Oral mite anaphylaxis (OMA), also known as “pancake syndrome,” is a rare but important cause of food-induced anaphylaxis. It is triggered by ingestion of foods contaminated with house dust or storage mites, most commonly Dermatophagoides pteronyssinus, Dermatophagoides farinae, and Blomia tropicalis. OMA was first described by Erben et al., who reported anaphylaxis after the ingestion of mite-contaminated pancakes 1 and further characterized and termed “pancake syndrome” by Sánchez-Borges et al. 2
Allergenic proteins from mites are heat-stable and can cause reactions even after cooking. Although OMA has been predominantly reported in tropical and subtropical climates, cases are increasingly being recognized in temperate regions.3–5 Symptoms typically occur within 1–2 h of ingestion and may involve the skin, respiratory, and gastrointestinal systems. Physical exertion after ingestion can lower the reaction threshold, mimicking food-dependent exercise-induced anaphylaxis (FDEIA). Differentiating OMA from other forms of anaphylaxis is essential to prevent misdiagnosis and guide management.
Case Presentation
A 14-year-old boy with a history of atopic dermatitis, moderate-to-severe persistent allergic rhinitis, and mild asthma since the age of 7 was referred to our clinic for evaluation for subcutaneous immunotherapy. He was born at term without neonatal complications, and his past medical history was unremarkable. His father, however, had idiopathic pulmonary fibrosis with an underlying genetic predisposition related to an Mucin-5B (MUC5B) mutation and died due to disease progression, while his brother has asthma. There was no parental consanguinity.
Over the previous two years, the patient had experienced three distinct anaphylactic episodes. Each episode occurred 30–60 min after ingestion of wheat-based foods—hamburger, lahmacun (a traditional Turkish flatbread topped with spiced minced meat), or bread—followed by 15–30 min of intense physical activity (football or basketball). Symptoms consistently began with generalized pruritic urticaria, followed by coughing/dyspnea and abdominal pain. Importantly, the patient tolerated these foods without symptoms when not followed by exercise. During the first anaphylactic episode, the patient was admitted to the emergency department and treated with intramuscular epinephrine, intravenous corticosteroids, and intravenous antihistamines, and showed a full recovery. In the second and third episodes, the patient self-administered the epinephrine auto-injector at home before presenting to the emergency department, where intravenous corticosteroids and antihistamines were administered. Symptoms resolved completely after treatment (Fig. 1).
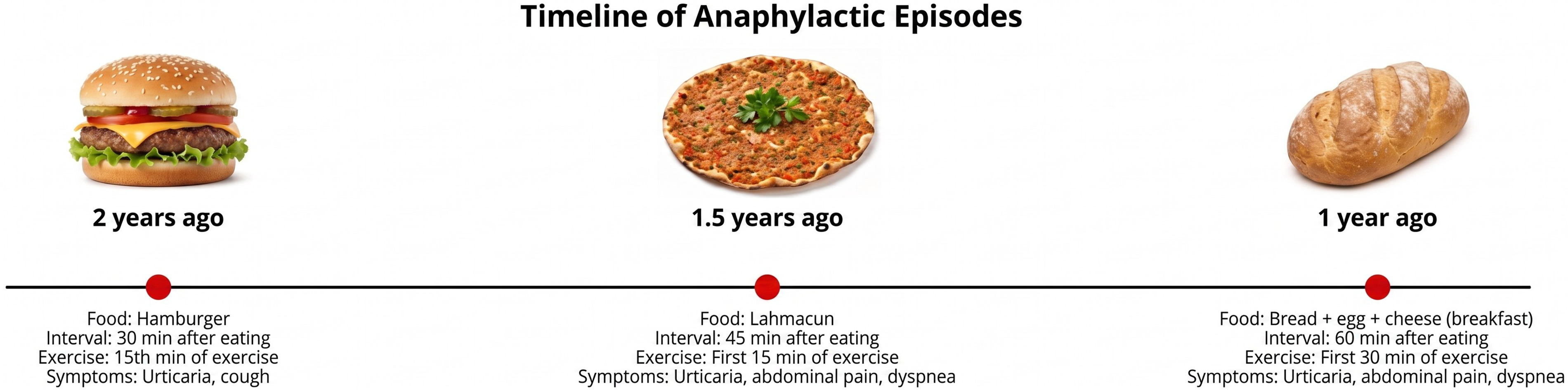
Timeline of anaphylactic episodes.
The food was commercially prepared, except for the bread episode, when the patient also consumed homemade dishes. His brother, who has similar allergic sensitizations, had never experienced similar reactions.
Between episodes, the patient exhibited persistent nasal congestion, sneezing, and moderate atopic dermatitis. Asthma control was suboptimal at presentation, with an Asthma Control Test (ACT) score of 20 and spirometry showing a reduced FEV1/FVC ratio (z-score –3.33 SDS, corresponding to approximately 74% of predicted). Controller therapy was escalated from inhaled fluticasone to a budesonide/formoterol combination.
Skin prick testing revealed strong sensitization to D. farinae (13 mm), D. pteronyssinus (9 mm), cat dander (10 mm), and dog dander (5 mm). Specific IgE was markedly elevated for D. farinae (80 kU/L) and D. pteronyssinus (>100 kU/L) but was negative for wheat. Baseline serum tryptase was 5.38 µg/L. Given the recurrent anaphylactic episodes with no clear food allergen and the initial consideration of idiopathic anaphylaxis, a multiplex component-resolved diagnostic test (ALEX2, Allergy Explorer 2) was performed. ALEX2 confirmed strong reactivity to multiple mite components, including Der f 2 (42 kU/L), Der p 2 (45 kU/L), Der p 5 (33 kU/L), Der p 7 (15 kU/L), Der p 21 (40 kU/L), Der p 23 (27 kU/L), and Blo t 5 (0.33 kU/L), while all tested food allergens were negative, including ω-5 gliadin (Tri a 19), the major marker of wheat-dependent exercise-induced anaphylaxis (WDEIA). Total serum IgE was markedly elevated (2,500 IU/mL). The patient’s Hyper-IgE Syndrome (HIES) score was calculated as 19, which did not support a diagnosis of HIES. Given the patient’s severe atopic dermatitis, an evaluation for primary immunodeficiency was performed; however, complete blood counts, lymphocyte subsets, and immunoglobulin levels were within normal limits, effectively ruling out an associated immunodeficiency.
The patient and his family were educated on the diagnosis of OMA, the importance of proper food storage, avoidance of long-term room-temperature storage of flour-based products, and the role of exercise as a reaction cofactor. He was prescribed an epinephrine auto-injector and trained in its use. Subcutaneous immunotherapy for house dust mite allergy was planned but only to be initiated after the exclusion of underlying genetic conditions and upon sustained asthma control, given the increased risk of systemic reactions in patients with uncontrolled asthma.
Subsequently, the patient was followed for six months after diagnosis. No further anaphylactic episodes were reported during this period; asthma control improved significantly, with ACT scores rising to 24–25 under combination therapy with budesonide/formoterol; allergic rhinitis symptoms improved markedly with azelastine and fluticasone combination intranasal therapy. This favorable outcome underscores the importance of optimizing comorbid allergic disease management and providing appropriate education and preventive strategies to reduce the risk of recurrence.
After genetic testing revealed no MUC5B mutation and asthma control was realized with optimized therapy during follow-up, subcutaneous immunotherapy (SCIT) for house dust mite allergy was initiated.
Discussion
Our patient presented with recurrent anaphylaxis following ingestion of wheat-based foods, but only when followed by exercise. The consistent absence of symptoms when consuming the same foods without exertion suggested a cofactor-dependent reaction. Since being first reported by Erben et al. 1 and subsequently by Sánchez-Borges et al., 2 OMA has been increasingly recognized, mainly in tropical countries but also in temperate regions.3–5 Strong sensitization to multiple house dust mite components, combined with negative wheat-specific IgE, supported a diagnosis of OMA rather than IgE-mediated wheat allergy or classic FDEIA.
Most reported cases of OMA involve foods stored for prolonged periods at room temperature, allowing mite proliferation. 4 In our case, although the food was commercially prepared, contamination could have occurred during production or storage prior to consumption. Wheat-related augmentation-dependent entities, namely wheat anaphylaxis dependent on augmentation factors (WANDA), could not be definitively excluded, as purified gluten or isolated wheat protein challenge tests were not available. This represents one of the main limitations of our case. 6 The absence of similar reactions in the patient’s atopic sibling highlights the variable clinical expression of mite sensitization. We attempted to obtain the flour used during the episodes for microscopic evaluation of mite contamination. However, the family had already discarded the homemade flour used during the third episode, and it was not possible to access the flours used in the first two episodes since they were commercially prepared, and a significant time had already passed. Therefore, direct demonstration of mite contamination could not be performed, which represents another limitation of our case.
Asthma control plays a critical role in anaphylaxis outcomes, as poor control is a well-recognized risk factor for increased severity and fatality in allergic reactions.7,8 In our patient, asthma control was initially suboptimal, with reduced lung function and persistent symptoms. Following escalation to a combination of inhaled corticosteroid/long-acting β2-agonist regimen, both symptom control and ACT scores improved significantly. This clinical course underscores the importance of assessing and optimizing comorbid allergic diseases, particularly asthma, as part of comprehensive anaphylaxis management. Optimizing asthma not only reduces background airway inflammation but may also lower the risk of severe outcomes during future anaphylactic episodes.
In patients presenting with recurrent anaphylaxis initially considered idiopathic after standard allergy work-up, the early adoption of component-resolved diagnostics (CRD) is crucial to uncover hidden or unconventional allergen sources and to refine the etiological diagnosis. CRD provided crucial diagnostic clarity in this case: It confirmed broad sensitization to multiple house dust mite components (Der f 2, Der p 2, Der p 5, Der p 7, Der p 21, Der p 23), consistent with clinically significant mite allergy. Importantly, all tested food allergens, including Tri a 19—the major marker of WDEIA 9 —were negative. This molecular profile allowed us to confidently move away from primary wheat allergy and supported mite-contaminated food ingestion as the most plausible explanation for the patient’s reactions. By demonstrating extensive mite sensitization while major wheat-related molecular markers were absent, CRD offered a clear diagnostic advantage over conventional testing and helped refine the etiological assessment in a patient who initially appeared to have idiopathic anaphylaxis.
Notably, all anaphylactic episodes required emergency management. The first was treated in the emergency department with intramuscular epinephrine, intravenous corticosteroids, and antihistamines, while in the latter two episodes, the patient self-administered the epinephrine auto-injector at home prior to additional treatment in the emergency department. These observations underscore the importance of immediate recognition and prompt epinephrine use in OMA-related anaphylaxis.
Differential diagnosis included primary wheat allergy, WDEIA, WANDA, and idiopathic anaphylaxis. In primary wheat allergies, symptoms typically occur after any ingestion, regardless of cofactors, and wheat-specific IgE is positive. WANDA represents augmentation factor-dependent wheat-related reactions; however, in our case, the lack of purified gluten or isolated wheat protein challenge testing precluded definitive assessment of these entities. Idiopathic anaphylaxis remains a diagnosis of exclusion when no clear trigger is identified. Importantly, CRD did not reveal any sensitization to molecular food allergens commonly implicated in idiopathic anaphylaxis, further supporting a defined allergen-driven mechanism rather than a truly idiopathic process.
Preventive strategies for OMA include refrigeration or freezing of flour-based products, avoiding long-term room-temperature storage, and educating patients on prompt recognition and treatment of symptoms. 4 Given the potential severity, patients should always carry and be trained to use an epinephrine auto-injector.
Conclusion
This case highlights OMA as an important diagnostic consideration in children presenting with cofactor-dependent anaphylaxis after wheat-based food ingestion. A detailed dietary and activity history, combined with CRD, is essential for accurate diagnosis, particularly in patients who may initially appear to have idiopathic anaphylaxis. In selected patients with coexisting asthma and/or allergic rhinitis, SCIT may be considered once stable disease control is ensured, to support long-term management and symptom control. Optimizing asthma control, educating patients in preventive measures, and ensuring epinephrine auto-injector availability are critical in preventing future episodes. The absence of new episodes over a six-month follow-up period would appear to underscore the effectiveness of these preventive strategies in real-life clinical practice.
Ethics Approval and Informed Consent for Publication
Ethical approval was not required for this case report in accordance with local legislation and institutional requirements. Written informed consent for publication was obtained from the patient’s parents.
Availability of Data and Materials
The datasets analyzed during the current study are not publicly available because they are patient-specific data, but are available from the corresponding author upon reasonable request.
Authors’ Contributions
S.A.: Conceptualization, data curation, investigation, writing—original draft, visualization. A.S.: Investigation, writing—review and editing. M.Ö.: Investigation, writing—review and editing. S.E.: Investigation, writing—review and editing. Ç.A.: Conceptualization, investigation, supervision, methodology, writing—review and editing. P.G.: Conceptualization, investigation, supervision, methodology, writing—review and editing. All the authors approved the final version of the article.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.