
Abstract
Asthma is a common chronic condition in childhood. Household secondhand smoke exposure (SHSe) from caregiver smoking is a major, modifiable contributor to poor asthma control. Previous reviews of SHSe interventions have focused broadly on indoor environmental or health outcomes for the general population. The impact of such interventions on pediatric asthma has yet to be systematically reviewed. We aimed to synthesize evidence regarding the effectiveness of caregiver secondhand smoke interventions for improving pediatric asthma outcomes and identify gaps to guide future intervention research. Following Joanna Briggs Institute methods and Preferred Reporting Items for Systematic Reviews and Meta-Analyses standards, we systematically searched PubMed, PsycINFO, CINAHL, Web of Science, and EMBASE. Eligible studies had no publication date restrictions, tested an intervention targeting household SHSe, and reported pediatric asthma-related outcomes. Randomized and quasi-experimental designs were included. Reviewers independently screened records, extracted data, and assessed risk of bias using the Cochrane Risk of Bias tools for randomized and nonrandomized trials. Of 9,832 records screened, 14 studies spanning 13 distinct interventions met the inclusion criteria. Except for 1 study with a single-group pretest–posttest design, all studies were randomized controlled trials. Overall risk of bias was low to moderate, with only 1 study deemed to be at critical risk. Interventions were typically home-based, delivered by health professionals, and incorporated asthma or SHSe education. Nine included a behavioral counseling component, and 6 incorporated caregiver feedback on SHSe. Six interventions improved subjective asthma indicators, such as symptom control, functional status, and unscheduled health care utilization; objective lung function improvements were not found. Behaviorally focused interventions that integrated caregiver feedback with education had the greatest success in reducing short-term SHSe and improving pediatric asthma outcomes. Evidence for long-term benefits remains poor. Lack of homogeneity in intervention content, measurement, and follow-up periods limits comparability. Future longitudinal trials with standardized measurement tools and diverse racial, ethnic, and socioeconomic populations are warranted.
Introduction
Asthma is most common chronic respiratory disease among youth worldwide and is associated with considerable morbidity and mortality.1,2 Poorly controlled asthma places a significant burden on quality of life, negatively impacting youth mental health, 3 academic performance, 4 and sleep.5,6 When persistent or undertreated, pediatric asthma can contribute to the burden of disease in adulthood, 7 with recent evidence linking childhood asthma and adverse lung-function trajectories to long-term cardiovascular and respiratory complications. 8
It is well established that secondhand smoke exposure (SHSe) from combustible tobacco products is associated with poor asthma control in youth, including exacerbated symptoms and asthma medication use, worse pulmonary function, and increased asthma-related health care utilization.9–11 Caregiver smoking at home is a significant source of SHSe among children,12–14 making SHSe an important modifiable risk factor for pediatric asthma. Despite this, there is a dearth of research systematically reviewing interventions targeting this factor. Previous reviews have focused on children in general and not specifically on those with asthma;15–18 of these, only 1 review included a study on asthma, and the impact of the intervention on asthma was not synthesized. 18 Other reviews have focused on indoor environmental pollutants more broadly.19,20
To the best of our knowledge, no review has evaluated the impact of caregiver-focused household SHSe interventions on pediatric asthma outcomes, representing a critical knowledge gap. This study aimed to systematically review and qualitatively synthesize the literature on the impact of interventions to reduce SHSe in households on pediatric asthma outcomes.
Methods
This systematic review followed the Joanna Briggs Institute (JBI) Guidelines for Systematic Reviews, 21 and was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 22 An a priori protocol was registered in PROSPERO (CRD42024542071). Due to heterogeneity in study design, outcome measures, and reporting practices, a quantitative meta-analysis was not conducted, and findings were synthesized narratively.
Data sources and search strategy
We systematically searched PubMed (pubmed.gov), PsycINFO (EBSCO), CINAHL (EBSCO), Web of Science, and EMBASE (Elsevier) using a predefined, iteratively developed search strategy in collaboration with a librarian to increase the rigor of the search (see Appendix A). A search strategy was first developed for PubMed using the database’s Medical Subject Headings controlled vocabulary terms and key terms. The final PubMed search strategy was then adapted with support from a librarian for the remaining 4 databases. We conducted our initial search on May 10, 2024, with no restrictions on the date of publication. Given the time elapsed between the initial search and article preparation, an updated search was conducted on October 3, 2025, covering studies published from May 10, 2024, onward. To ensure literature saturation, we conducted ascendency and descendancy searches (i.e., searches of the reference lists of each included study and the citations of included studies, respectively). 23
Eligibility criteria
Studies were included in this review if they met the following criteria: an intervention targeting in-home SHSe (eg, smoking bans) was tested; asthma outcomes were reported (eg, asthma symptoms, asthma-related health care utilization); and the study was peer-reviewed and available in English. We included randomized controlled trials, pragmatic trials, and quasi-experimental trials. To improve generalizability, our search was not limited to studies conducted in the United States. Gray literature was excluded to maintain consistency in methodological rigor and reporting standards across included studies. While this approach may limit the inclusion of unpublished findings, it enhances the comparability and quality of evidence synthesized in this review.
Study selection and screening
We imported search results into EndNote, a citation manager library, to identify and remove duplicate records. An EndNote file containing all the unique records from our search was exported. The resulting file was then uploaded into Covidence (https://www.covidence.org), a web-based literature review software. Covidence was used to facilitate all phases of screening, full-text review, and data extraction.
All 6 authors participated in the review process. Titles and abstracts were independently screened by 2 reviewers, with discrepancies resolved through team discussion and consensus. Full-text articles were then independently reviewed by 2 authors, with disagreements resolved by the full team to determine final inclusion for data extraction.
Data extraction
Data extraction took place from July 29, 2024, to February 13, 2025. Two authors independently extracted data in Covidence using a form developed iteratively as a team. The data extraction form included (1) study characteristics (first author’s last name, publication year, location, funding source); (2) study design details (sample size, inclusion and exclusion criteria, study design, follow-up duration, primary and secondary outcomes); (3) participant age and sex; (4) SHSe intervention and control intervention details (setting, format, delivery method, intervention content); (5) asthma and SHSe outcomes assessed and how they were measured; (6) impact of the intervention on asthma and SHSe outcomes; and (7) study limitations. All discrepancies in the data extracted were resolved by team consensus.
Risk of bias
Two authors independently assessed the validity and robustness of each study using the Cochrane Risk of Bias 2.0 (RoB2) 24 tool for randomized trials and the Risk of Bias in Non-randomized Studies of Interventions, Version 2 (ROBINS-I V2) 25 tool for nonrandomized trials. Randomized trials were scored on 5 domains of bias: (1) the randomization process; (2) deviations from the intended interventions; (3) missing data; (4) measurement of the outcomes; and (5) selection of reported results. Non-randomized trials were scored on 7 domains of bias: (1) confounding; (2) classification of interventions; (3) selection of participants into the study (or into the analysis); (4) deviations from intended interventions; (5) missing data; (6) measurement of the outcome; and (7) selection of the reported result. Domain scores were then used to determine an overall risk of bias rating, which was calculated using predefined algorithms provided by each respective tool. Discrepancies were resolved as a team until consensus was achieved. Randomized trials were categorized as having low, some, or high risk, and non-randomized trials as low, moderate, serious, or critical risk.
Results
Study identification
Figure 1 illustrates the study selection process. A total of 9,832 unique records were identified and screened at the title and abstract level, of which 40 were deemed eligible for full-text review. Of these, 26 articles were excluded for the following reasons: not assessing asthma outcomes (n = 16); interventions not focused on SHSe (n = 5); absence of analysis of asthma outcomes (n = 2); protocol-only publications (n = 2); and duplicate records (n = 1).
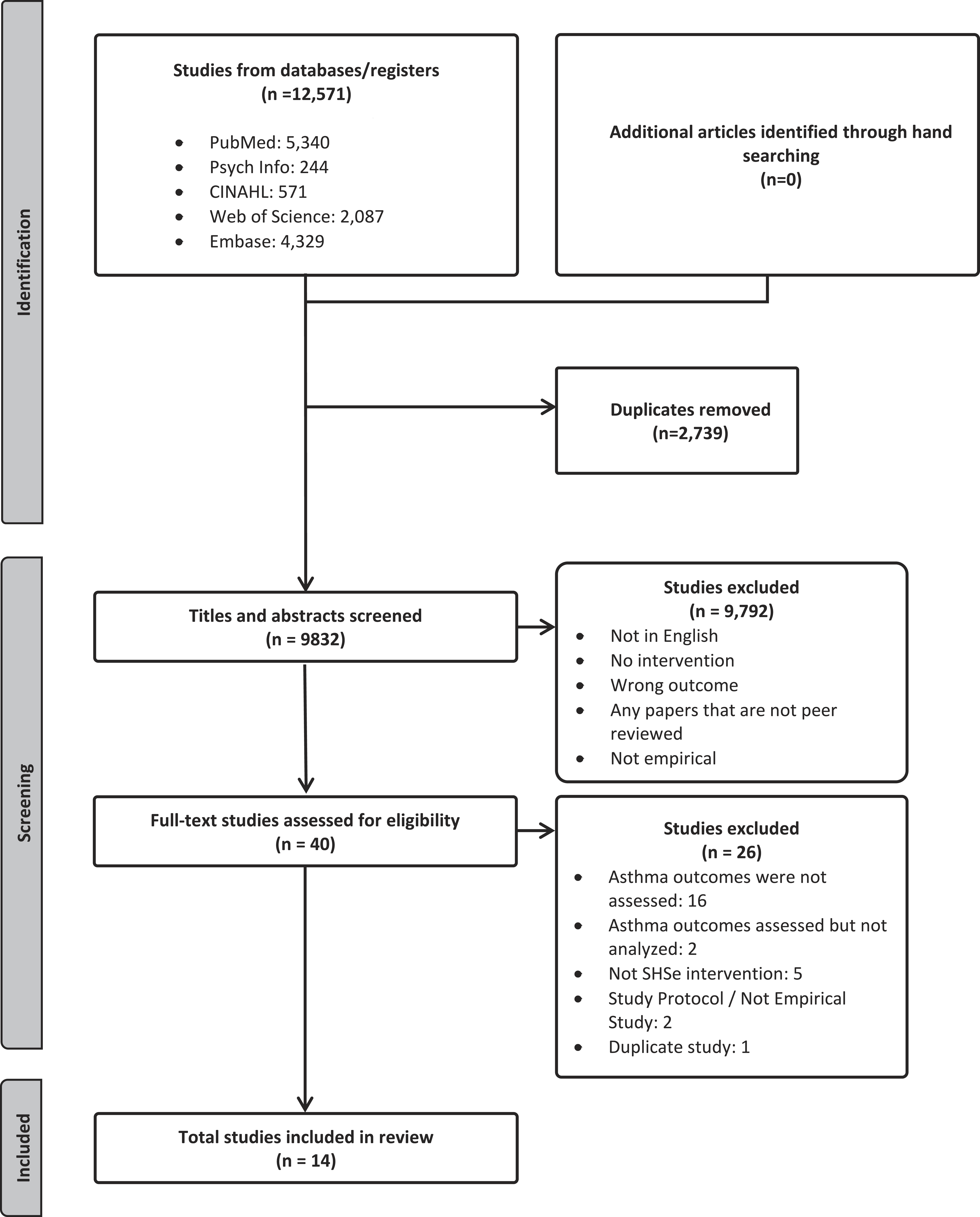
PRISMA flow diagram illustrating the literature search. Note. CINAHL stands for Cumulative Index to Nursing and Allied Health Literature. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Among the 14 studies identified, 13 distinct interventions were represented, all targeting pediatric asthma. Four interventions were evaluated across multiple publications: (1) the Childhood Asthma Prevention Study in both interim 26 and postintervention analyses 27 ; (2) an in-person counseling and education program at 1 month 28 and 3 years 29 post-intervention; (3) the Lowering Environmental Tobacco Smoke (LET’S Manage Asthma) intervention in 2 studies30,31; and (4) the Precaution Adoption Model intervention, evaluated both as the primary intervention 32 and as a control condition. 33
Study designs
With the exception of 1, single-group pretest–posttest study design, 34 all studies used 2- or 3-arm individual-level randomized controlled trial (RCT) designs.26–33,35–39 Sample sizes ranged from 58 39 to 560 participants 33 (Table 1).
Characteristics of Participants and Study Settings
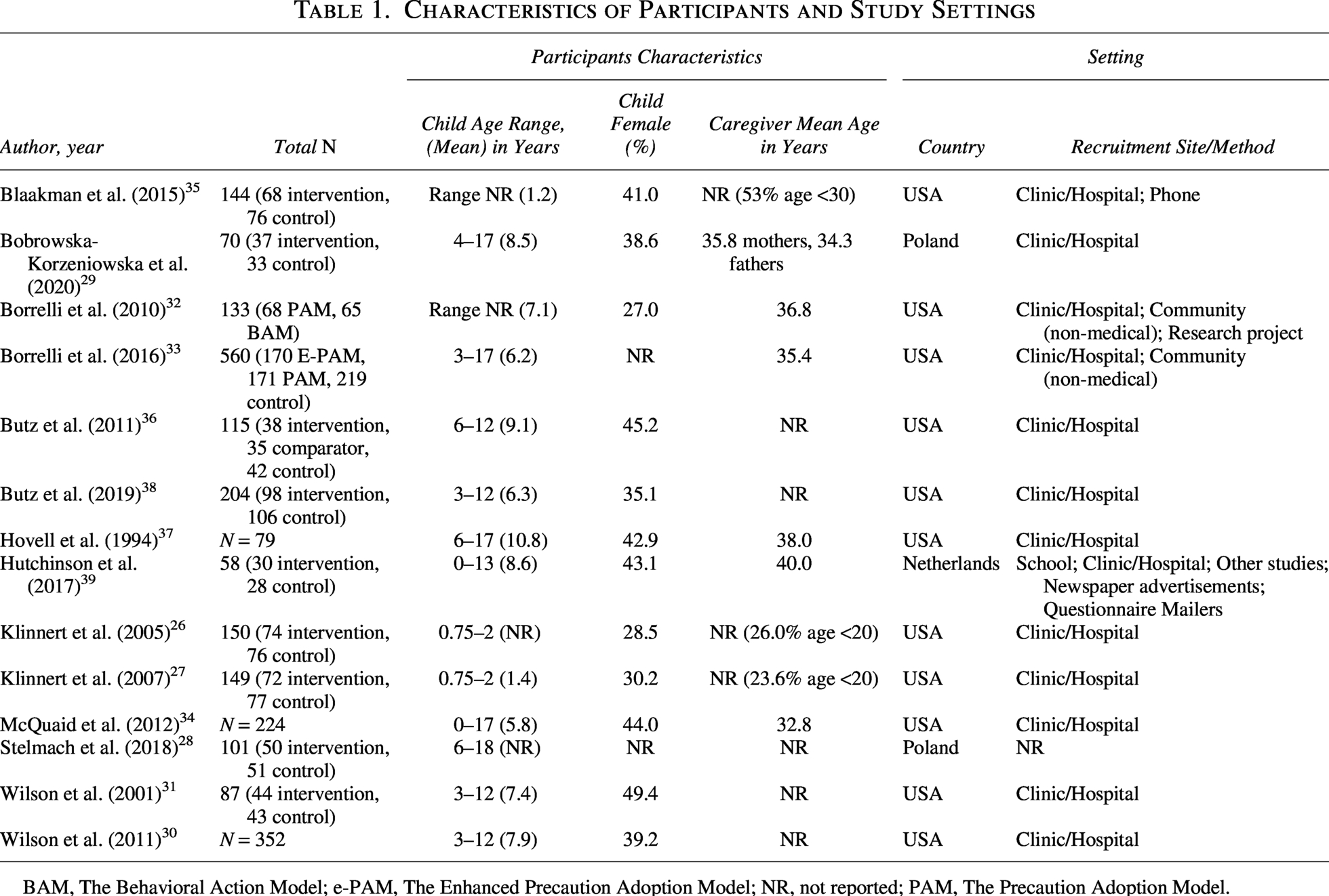
BAM, The Behavioral Action Model; e-PAM, The Enhanced Precaution Adoption Model; NR, not reported; PAM, The Precaution Adoption Model.
Intervention characteristics
All interventions were delivered to individual primary caregivers or to individual families. Nurses led sessions for 6 interventions.26,27,30,31,34–36,38 The remaining interventions were delivered by allergists, 29 health educators, 32 counselors, 39 or were unspecified.29,33,37 Individual sessions lasted between 1029,40 and 60 min. 39 Eight interventions were delivered in homes,26,27,32–36,39 of which 3 also included phone calls.32,33,35 Three interventions were delivered during clinic or hospital visits.29–31,37 One intervention utilized both home and clinic visits. 38
Interventions were comprised of 1 35 to 18 26 sessions. Among the 10 studies that reported intervention duration, time varied substantially from 5 weeks30,31,36,38 to 3 years. 29 Klinnert et al. 26 was the most participation-intensive intervention, with 18 home visits over 12 months and an average session length of 53 min.
Ten interventions incorporated individual counseling techniques (Table 2). Among these, the most commonly used technique, adopted by 5 interventions, was motivational interviewing.32,33,35,38,39 Three interventions used a cognitive-behavioral approach,26,27,34,35 while 2 employed other behavioral techniques, including behavioral modification 37 and stage-of-change-based counseling.30,31 Seven interventions incorporated general asthma education.26,27,32–35,38 None of the interventions specifically included a pharmacotherapy component for smoking cessation. However, Borrelli et al.32,33 offered 8 weeks of transdermal nicotine patches (TNP) to caregiver participants who expressed readiness to quit during or after the intervention.
Study Characteristics
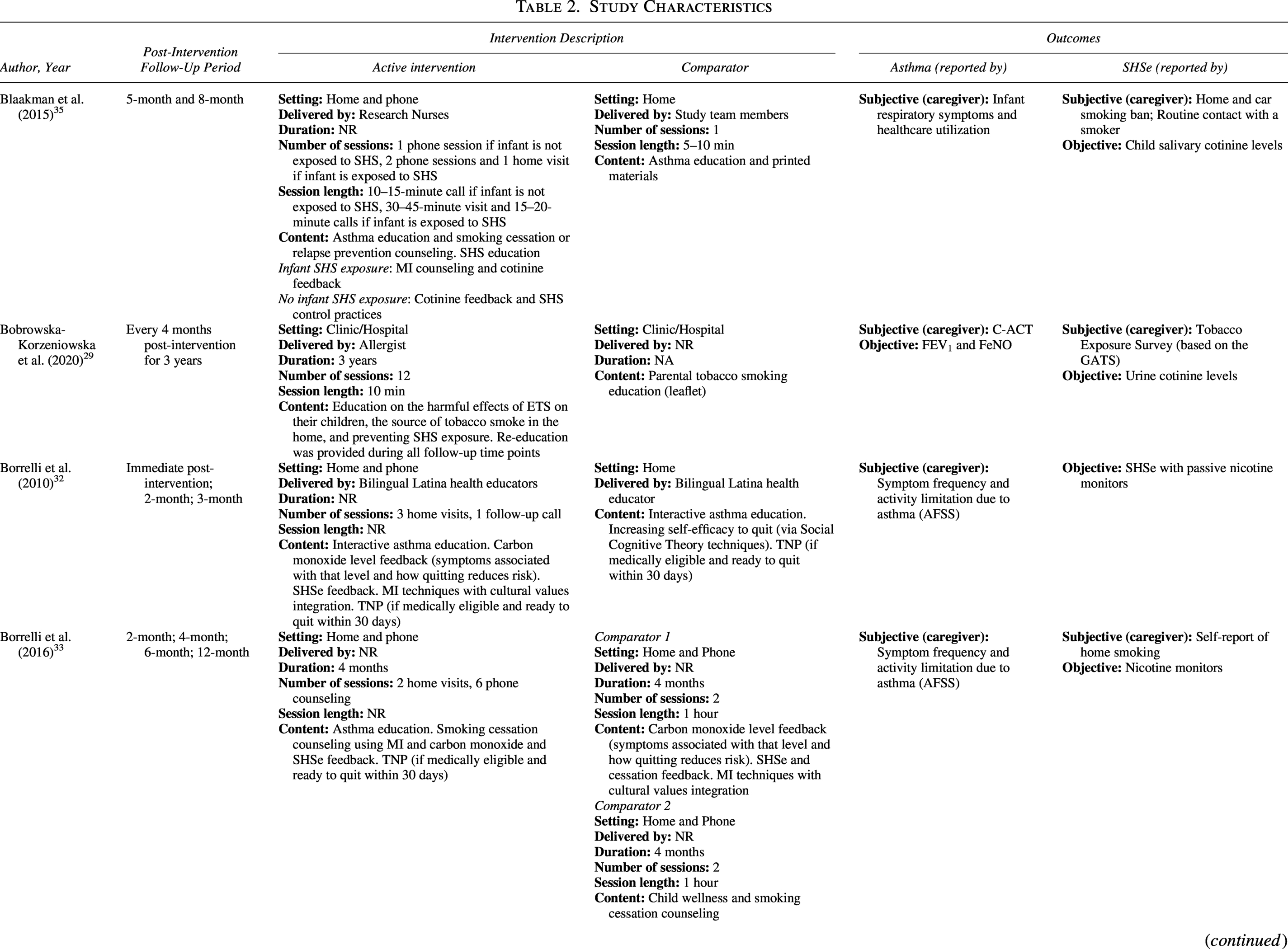
Note: All studies utilized an individual-level RCT design, except for McQuaid et al., 2012, which implemented a single-group, pretest–posttest design.
AFSS, Asthma Functional Severity Scale; BAM, The Behavioral Action Model; C-ACT, Childhood Asthma Control Test; CCR, cotinine/creatinine ratio; ED, emergency department; ETS, environmental tobacco smoke; e-PAM, The Enhanced Precaution Adoption Model; FAMSS, Family Asthma Management Scale Scale; FEV1: forced expiratory volume in 1 second; FeNO, fractional exhaled nitric oxide; FSII, Functional Status II Scale; GATS, Global Adult Tobacco Survey; HEPA, high-efficiency particulate air; IOS, impulse oscillometry; MI, motivational interviewing; NA, not applicable, NR, not reported; PACQLQ, Pediatric Asthma Caregiver’s Quality of Life Questionnaire; PAM, The Precaution Adoption Model; PCP, primary care provider; RCT, randomized controlled trial; ROI, return on investment; SHS, secondhand smoke; SHSe, secondhand smoke exposure; TNP, transdermal nicotine patch.
Participants
Studies were conducted primarily in the United States, with 2 in Poland28,29 and 1 in the Netherlands. 39 Participants were recruited from clinic or hospital settings in all but one study. 28 In addition to recruiting from clinics and hospitals, Hutchinson et al. 39 also recruited participants from schools and additional channels, including newspaper advertising and mailers.
While we imposed no age restrictions on our search, all included studies assessed pediatric asthma outcomes, with the mean age of child participants ranging from 1.2 35 to 10.8 years. 37 For the 2 studies in which mean age was not reported, child participant ages ranged from 0.75 to 2 years 26 and 6 to 18 years. 28 Only half of the studies reported race and ethnicity data for their child participants.26,27,30,31,35–37
All studies except two26,27 focused on children and adolescents with an asthma diagnosis. Klinnert et al.26,27 designed their intervention to prevent asthma among infants with wheeze; therefore, a clinical asthma diagnosis was a study outcome rather than an inclusion criterion.
Risk-of-bias
Of the 13 RCTs identified, 8 were classified as having a low risk of bias,30–33,35,36,38,39 and 5 were identified as having some risk (Table 3).26–29,37 Poorer scores were the result of limited or missing information (eg, no study plan/research protocol) in older clinical trials26,27,37 and insufficient methodological details included in brief reports. 28 The single-group pretest–posttest study by McQuaid et al. was classified as having critical risk as a result of uncontrolled confounding. 34 No studies were excluded due to their risk.
Outcomes assessed
Asthma
All 14 studies assessed asthma outcomes subjectively through child, caregiver, or provider report (Table 2). Seven studies assessed asthma-related health care utilization.26,30,31,34–36,38 Other dimensions of subjective asthma control included symptom-free days and nights,31,36,38 activity limitations,31–34,36 respiratory complaints,35,39 and night awakenings, 31 which were assessed using questionnaire items written by the investigators. Of the 5 studies that utilized validated instruments, 2 used the Childhood Asthma Control Test (C-ACT),28,29 1 used the Functional Status II, 39 and 2 used the Asthma Functional Severity Scale.32,33 Only 3 studies measured medication use subjectively.26,30,38
Lung function was objectively assessed in 6 studies,27–29,31,37,39 with the most common measure being forced expiratory volume in the first second of expiration (FEV1).28,29,31,37 Other measurement techniques utilized were fractional exhaled nitric oxide28,29 and impulse oscillometry. 27
Secondhand smoke exposure
With only 1 exception, 27 all studies assessed child SHSe (Table 2). Subjective outcomes were measured in 6 studies through caregiver self-report.29,33,35–37,39 Measures included: caregiver-reported child smoke exposure in the home33,37,39; reported implementation of a home and car smoking ban 35 ; reported contact with a smoker 35 ; and reported smoking frequency and location in and around the home. 36 Bobrowska-Korzeniowska et al. 29 evaluated exposure using a caregiver-reported questionnaire based on the Global Adult Tobacco Survey.
Objective SHSe outcomes were assessed in all but one study, 27 with the most common objective measures being urine cotinine levels26,28–31,36,39 followed by salivary cotinine levels.35,38
Study heterogeneity
Intervention characteristics
Considerable heterogeneity was observed across the 13 interventions, particularly in reporting core intervention components. Four studies did not report total intervention duration,32,34,35,38 and 2 did not specify delivery personnel (eg, nurses, interventionists, research staff).33,37 Only 5 interventions reported session length,26,27,29,35,36,39 limiting comparisons of intervention intensity and delivery frequency.
Intervention participation and adherence
Reporting metrics for intervention participation and adherence were varied across studies (Table 4). When reported (6 of 14 studies reviewed), session participation and attendance were relatively high, ranging from 66% to 98% per session.30,33 One study reported a median attendance rate of 83.3% across intervention sessions. 26 Another study reported 83% participation in at least 3 of its 6 sessions. Three studies reported that 90%, 82%, and 89% of participants, respectively, attended at least 1 session.31,32,35
Risk of Bias Assessment of the Included Randomized Trials
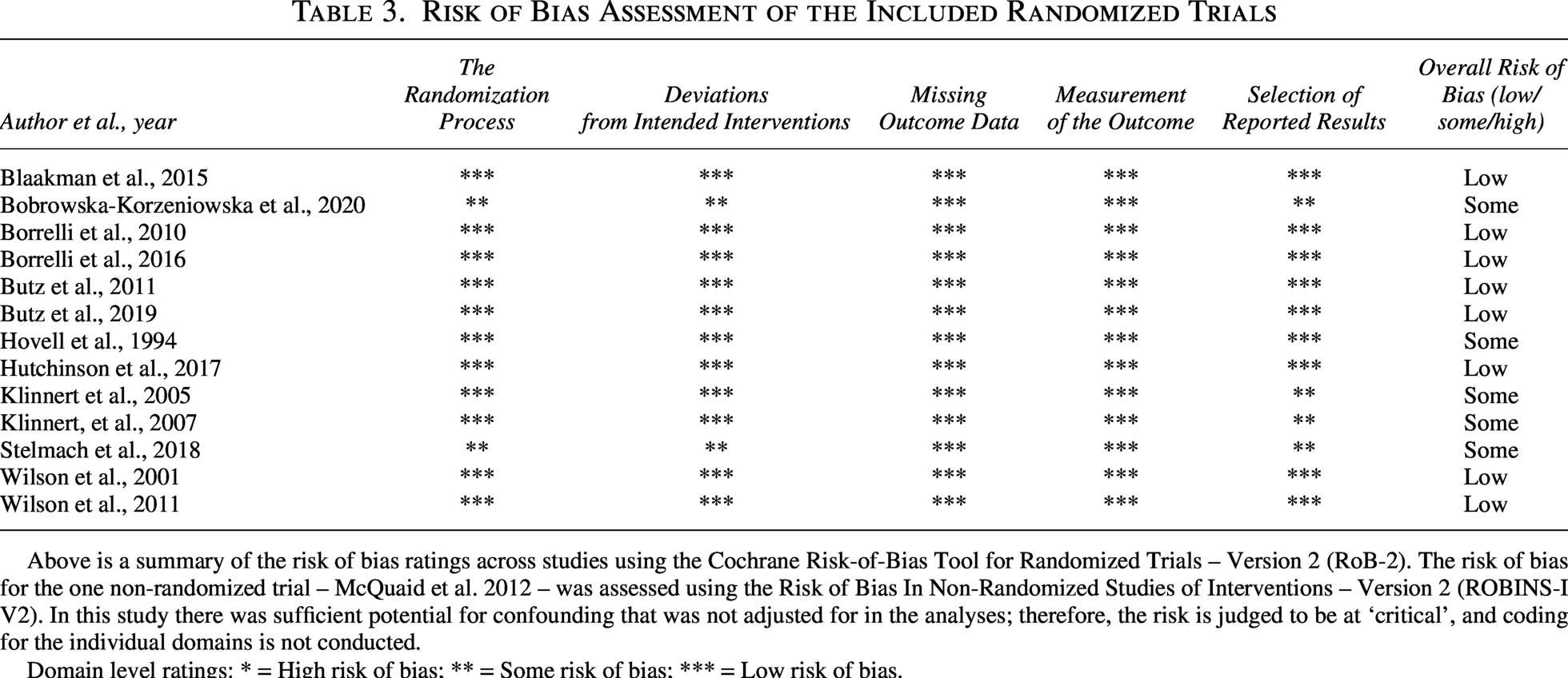
Above is a summary of the risk of bias ratings across studies using the Cochrane Risk-of-Bias Tool for Randomized Trials – Version 2 (RoB-2). The risk of bias for the one non-randomized trial – McQuaid et al. 2012 – was assessed using the Risk of Bias In Non-Randomized Studies of Interventions – Version 2 (ROBINS-I V2). In this study there was sufficient potential for confounding that was not adjusted for in the analyses; therefore, the risk is judged to be at ‘critical’, and coding for the individual domains is not conducted.
Domain level ratings: * = High risk of bias; ** = Some risk of bias; *** = Low risk of bias.
Intervention Effects
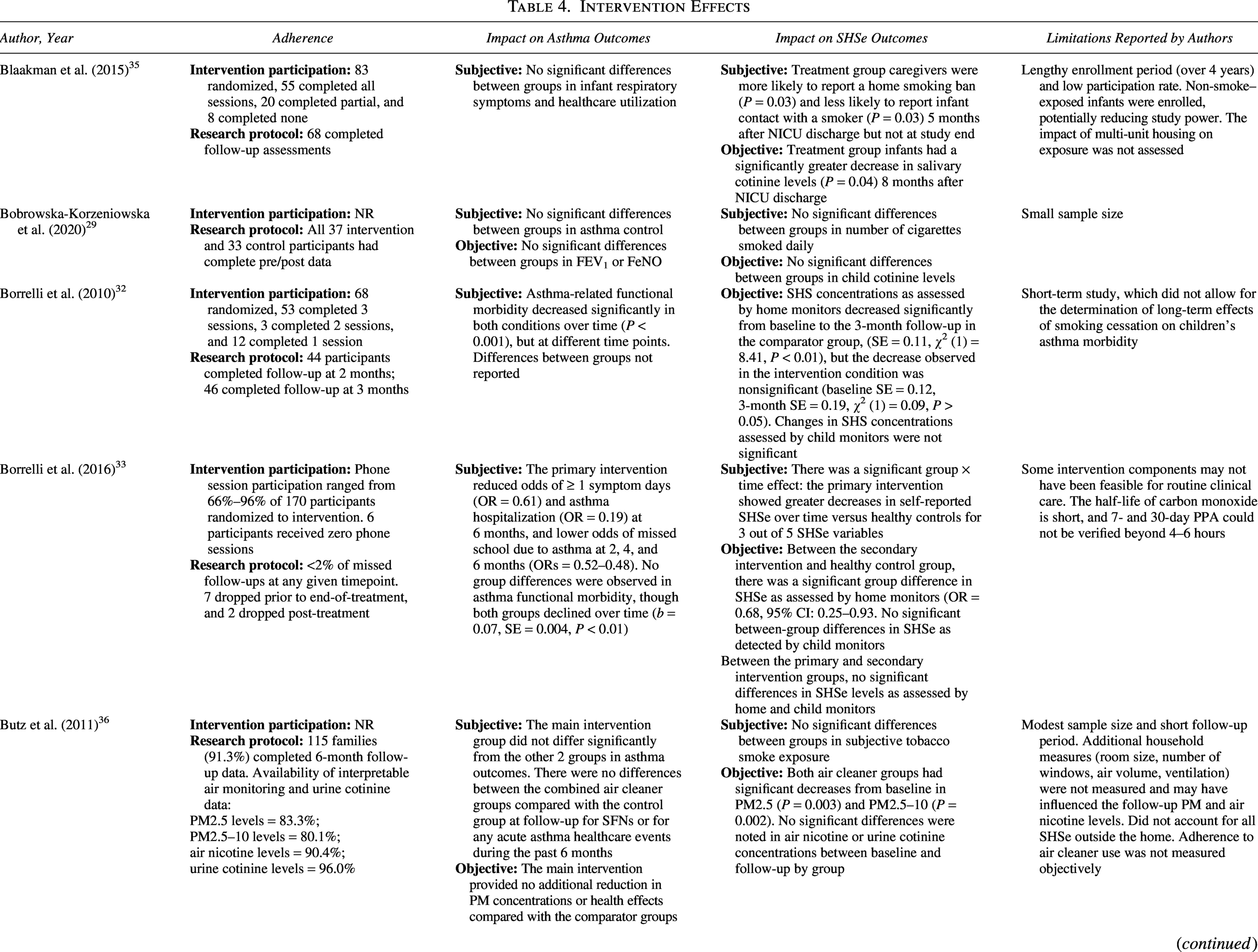
C-ACT, Childhood Asthma Control Test; CI, confidence interval; ED, emergency department; ETS, environmental tobacco smoke; FeNO, fractional exhaled nitric oxide; FEV1, forced expiratory volume in 1 second; FSII, Functional Status II Scale; HC, healthy controls; HR, hazard ratio; lnCCR, natural logarithm of the cotinine to creatinine ratio; NICU, neonatal intensive care unit; NR, not reported; OR, odds ratio; PM, particulate matter; PPA, point prevalence abstinence; PACQLQ, Pediatric Asthma Caregiver’s Quality of Life Questionnaire; PEF, peak expiratory force; PS, passive smoking; QoL, quality of life; SD, standard deviation; SE, standard error; SFD, symptom-free days; SFN, symptom-free nights; SHS, secondhand smoke; SHSe, secondhand smoke exposure.
Intervention effects
Asthma outcomes
The effectiveness of interventions in improving asthma outcomes was mixed (Table 4). Six studies reported significant differences across various dimensions of subjective asthma outcomes, which included functional morbidity, 32 frequency of symptom days, 33 asthma hospitalizations or acute care medical visits,31,33 missed school due to asthma, 33 asthma symptoms,27,37 and use of steroid bursts. 26 In the asthma prevention trial among wheezing infants, the odds of developing asthma by age 4 were 3 times lower in the intervention group than in the control group (P = .04). 27 Eight studies found no improvements in subjective28–30,35,36,38,39 or objective28,29,34,39 asthma outcomes.
Secondhand smoke exposure outcomes
Across the 6 studies assessing subjective SHSe outcomes through caregiver self-report,29,33,35–37,39 3 showed positive results.33,35,37 Two of 3 studies assessing caregiver-reported home exposure favored the intervention group.33,37 One study found short-term increases in reported home smoking bans (P = 0.03) and decreased likelihood of infant contact with a smoker (P = 0.03) among the treatment group, though these differences were not maintained after the active study intervention period. 35 Smoking frequency and location 36 and the number of cigarettes smoked daily 29 did not differ significantly between treatment groups.
Of the 9 studies objectively assessing SHSe, 3 reported positive outcomes,26,35,37 2 were mixed,32,33 and 4 found no between-group differences28,29,36,39 (Table 4). Klinnert et al. 26 reported significantly lower cotinine levels in intervention participants compared with controls (P = 0.02), with a greater decrease found among low psychologically resourced families (P = 0.01). Similarly, Hovell et al. 37 found a significant decrease in all sources of home environmental tobacco smoke (ETS) in the intervention group compared with the monitoring control group (F[4,148] = 3.71, P < 0.01) and the treatment-as-usual group (F[4,164] = 3.75, P < 0.01). One infant-focused intervention reduced salivary cotinine at follow-up in the intervention group (P = 0.04). 35 Objective outcomes from 2 studies yielded mixed results: home-monitor data from 1 trial showed a significant decrease at 3-month follow-up, but only in the control condition (standard error = 0.11, χ2(1) = 8.41, P < 0.01), 32 while another trial found significant group differences between the secondary intervention and healthy control group (OR = 0.68, 95% confidence interval [CI]: 0.25–0.93), but not between the primary intervention and secondary intervention. 33
Subgroup analyses
Five studies conducted subgroup analyses. Borrelli et al. conducted post hoc comparisons between SHSe reduction and smoking status (quitters versus nonquitters); results indicated significant reductions in subjective (P < 0.05) and objective (χ2(1) = 6.01, P = 0.014) SHSe among nonquitters in the control group compared with the intervention group. 32 According to the authors, these unexpected findings may have been the result of nonquitter control participants taking additional measures to reduce SHSe at home in lieu of quitting. The Butz et al. trial of a home-based environmental control intervention found fewer asthma emergency health care utilizations among a subgroup of intervention children with no SHSe at home (P = 0.04), but not among children with SHSe at home (P = 0.53). 38 Results of McQuaid et al.’s single-arm financial return on investment (ROI) study found positive ROI (+106.9) for children younger than 6 years, negative ROI (−150.3) for children 6–18 years old, and negligible ROI for moderate/severe persistent asthma (+6.9%). 34
Multivariate analyses were conducted in 2 studies assessing the LET’S Manage Asthma Intervention. Findings from the 2001 study found that the interaction between the intervention group and high-risk status was significantly associated with reduced nicotine levels care (β = −0.994; 95% CI, −1.810 to −0.178; P = 0.017). Among the high-risk subgroup, the intervention was associated with significantly lower urine cotinine levels at 6 months follow-up (P = 0.02) compared with usual care. 31 Findings from the 2011 study indicated that intervention efficacy was significantly moderated by child baseline risk status (β = −0.994; 95% CI, −1.810 to −0.178; P = 0.017); children classified as high-risk in the intervention group showed significantly lower follow-up nicotine levels compared with those receiving usual care (β = 1.068; 95% CI, −1.816 to −0.319; P = 0.006). 30
Characteristics of effective interventions
Key differences emerged between the 4 successful interventions and the 9 that showed no significant impact. Specifically, programs with sessions relatively close together (1–3 weeks apart)26,27,31 were more likely to yield significant asthma or SHSe improvements compared with those with lengthier times between sessions (eg, 1 month apart or more). All but one intervention 31 employed a multicomponent approach, specifically integrating biomarker or environmental feedback with behavioral counseling for caregivers. Providing caregivers feedback on child cotinine concentrations, carbon monoxide levels, SHSe, and environmental allergens in the home proved particularly effective, as across 8 studies that utilized this component, 5 yielded favorable asthma or SHSe outcomes.26,27,33,35,37 Interventions delivered through both home and phone sessions32,33,35 were more successful in improving asthma symptoms and SHSe outcomes32,33,35 compared with those delivered in the home alone.34,36,37,39
Discussion
The results of our findings were mixed. Across 13 interventions, 6 resulted in improved subjective asthma outcomes, including report of symptom-free days, asthma functional severity, and reduced emergency care visits. In contrast, interventions assessing objective asthma outcomes found no improvements. The salience of caregiver-observed asthma symptoms may offer one explanation for favorable subjective-to-objective asthma outcomes. In addition, objective measures were collected relatively infrequently and thus limited to a single time point, whereas subjective measures were captured over time to provide a more robust temporal sequence of asthma symptoms.
Significant differences in home-based SHSe were observed across 4 interventions, and 2 of these found improvements in both objective and subjective. Of the remaining 2 interventions, 1 found differences in self-reported home exposure but not in home-monitoring data, while the other found differences in cotinine levels alone.
Our findings outline several intervention characteristics associated with improved asthma outcomes and reduced SHSe at home. Most notably, caregiver counseling emerged as a critical driver of effectiveness. Interventions that emphasized skill building, motivational interviewing, and individualized feedback were more likely to show benefits than information-only approaches, which rarely led to lasting reductions in SHSe or asthma outcomes.29,36,38 Furthermore, the delivery modality appeared to influence outcomes. Interventions that combined home visits with phone sessions showed greater success in improving asthma symptoms than those relying solely on home-based delivery. While single-modality home visits were common across the broader sample, the added engagement from phone call follow-ups was a recurring feature of most effective interventions.
Outcome assessment varied considerably. Most studies relied on caregiver-reported asthma symptoms or health care utilization. Only 6 studies used objective asthma measures, and even fewer linked them directly to cotinine-verified reductions in SHSe. The use of different instruments to assess asthma control, such as the C-ACT and investigator-written questionnaires, limited comparability across studies. Most studies measured outcomes only at short-term follow-up points, typically within 6 months, which constrained the ability to assess sustainability. Moreover, intervention adherence and participation rates were inconsistently reported, potentially biasing results due to varying levels of adherence across studies. Significant heterogeneity in the reporting of core intervention characteristics (eg, program duration, session length, and session frequency) further limited comparability.
Although most studies assessed both SHSe and asthma outcomes, reductions in SHSe did not consistently translate into measurable improvements in asthma control. This discrepancy may reflect a combination of factors. Modest SHSe reductions and relatively short follow-up periods may have limited the ability to detect clinically meaningful changes in asthma control. Taken together, the findings suggest that while SHSe-focused interventions are feasible and can influence caregiver behavior, their downstream impact on pediatric asthma outcomes remains limited without continued reinforcement and behavioral support.
Limitations
This review followed rigorous methodological guidance from the JBI and PRISMA, including dual screening, independent data extraction, and use of validated bias assessment tools. The inclusion of both randomized and quasi-experimental studies allowed for a broad assessment of intervention approaches. However, it should be acknowledged that the inclusion of a pretest–posttest study without a control group34 introduces a high risk of results reflecting regression to the mean rather than a true intervention effect. Also, heterogeneity in intervention type, outcome measures, and follow-up precluded meta-analysis and limited our results to qualitative synthesis.
The generalizability of our findings is limited for several reasons. First, while our search strategy was comprehensive and included studies from all countries, it is plausible that eligible studies were missed. The review included only English-language, peer-reviewed articles, possibly excluding relevant gray literature. Most study samples were recruited from clinical or hospital settings, introducing potential selection bias, as these populations may differ from the broader community in their health-seeking behavior. Participation in randomized trials may increase the likelihood of social desirability bias in self-reported outcomes. It is possible that participants’ awareness of being observed, often referred to as the Hawthorne effect, may have further influenced behavior, potentially narrowing the gap between group differences and limiting the external validity of the observed effects.42 In addition, while we did not limit the age of patients with asthma, most studies focused solely on children. Finally, few studies reported participant race, ethnicity, or socioeconomic status, limiting the generalizability of our study to children and adolescents of diverse racial, ethnic, and socioeconomic groups. This also highlights a knowledge gap regarding SHSe interventions.
Implications for practice and research
Future research can clarify the mechanisms linking SHSe reduction to asthma control by utilizing standardized, objective measures. Longitudinal studies with extended follow-up are needed to assess whether short-term reductions in SHSe are sustained and translate into asthma improvements in outcomes such as pulmonary function, health care utilization, and symptom control. As evidenced by trials such as LET’S Manage, children with high-risk asthma can derive the greatest clinical benefit from intensive SHSe reduction efforts. Clinicians can specifically target families of children with persistent or poorly controlled asthma.
Greater inclusion of racially, ethnically, and socioeconomically diverse families is vital, given the disproportionate burden of both asthma and SHSe among low-income and minority populations. To address this need, policy initiatives can prioritize the integration of high-frequency intervention programming into federally qualified health centers and school-based health clinics to reach those most in need. Similarly, governments can ban smoking in subsidized housing or offer SHS education and behaviroral interventions to families with a primary caregiver who smokes. In addition, developing approaches that engage caregivers and adolescents in intervention development can lead to cultural relevance, adherence, and long-term behavior change.
Conclusion
This systematic review provides a novel synthesis of interventions to reduce household SHSe and improve asthma outcomes among children and adolescents. Findings across the 14 studies were mixed. While several interventions improved caregiver behavior and subjective asthma symptoms, these gains rarely translated into improvements in objective lung function (eg, FEV1). The most effective interventions—those improving both SHSe and asthma morbidity—featured high session frequency, multicomponent designs, and hybrid intervention delivery combining home visits with phone counseling or clinic visits. Programs integrating biomarker, environmental, or symptom feedback with motivational interviewing and tailored behavioral planning outperformed information-only approaches, highlighting the importance of individualized caregiver feedback. Clinicians and policymakers should expand services through the delivery of health interventions in community clinics and the implementation of regulations on smoking in public housing to better support high-need populations.
Footnotes
Acknowledgments
The authors thank John Usseglio for his expertise in developing the search strategy and for his support throughout the review process.
Author Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding Information
The authors disclose receipt of the following support for the research, authorship, and/or publication of this article: This work was supported by the National Heart, Lung, and Blood Institute (R61/R33 HL151958; PI: Bruzzese); the content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.