
Abstract
Background:
Transient wheezers are preschool children with recurrent wheezing that resolves by age 6 years. In cases of frequent or severe exacerbations, maintenance inhaled corticosteroid (ICS) therapy is often required. This study evaluated the time to ICS cessation and identified factors associated with delayed cessation.
Materials and Methods:
This retrospective study included children under 5 years with >3 wheezing episodes per year who received ICS therapy. The duration of ICS treatment was calculated from the initiation to the cessation of ICS use. Successful ICS cessation was defined as the absence of wheezing following discontinuation of ICS, with follow-up until at least 7 years of age. The primary outcome was time to ICS cessation, estimated using a time to event curve. Factors associated with time to ICS cessation were identified using a Weibull accelerated failure time model.
Results:
A total of 162 children were enrolled. The mean ages (SD) at ICS initiation and cessation were 2.7 (1.1) and 4.1 (1.1) years, respectively. The median time to achieve ICS cessation was 16.1 months. Compared with children aged >3 years, those aged <2 years had more than twice the time to ICS cessation (time ratio [TR] 2.01, 95% confidence interval [CI] 1.62–2.49). In addition, the presence of non-allergic rhinitis (NAR) was associated with a TR of 1.38 (95% CI: 1.09–1.76), suggesting that these children required 38% longer to discontinue ICS therapy than those without rhinitis.
Conclusion:
Among transient wheezers requiring ICS therapy, the median time to successful cessation was 16.1 months and may represent a potential upper-bound estimate. The observed time to ICS cessation likely reflects physician-driven decision-making. Younger age and NAR were associated with delayed ICS discontinuation. These findings provide real-world evidence on ICS treatment trajectories in children whose wheezing ultimately resolves and support the development of evidence-based guidelines to optimize ICS discontinuation.
Introduction
Wheezing is a common symptom in preschool children requiring medical consultation. The prevalence of preschool wheezing varies by region. A European cohort study reported that the prevalence of wheezing in 4-year-old children ranged from 9.82% in Greece to 55.37% in Spain. 1 In Asia, the prevalence is 22.4% in Korean children aged 3–6 years 2 and 30.47% in Sri Lankan children. 3 Despite its frequency, limited evidence exists on the pathophysiology and treatment of wheezing in preschool children owing to the heterogeneity among affected children. The Global Initiative for Asthma guidelines recommend a 3-month trial of low-dose inhaled corticosteroid (ICS) therapy for preschoolers with recurrent wheezing. 4 After the trial, physicians determine whether to continue or discontinue ICS, with treatment duration tailored to individual clinical characteristics. Evidence suggests that low-to-moderate doses of ICS improve symptoms and reduce exacerbation in children with a classical asthma phenotype, characterized by atopic disease and allergic sensitization. 5 These children often require ICS therapy for symptomatic control until at least 6 years of age (persistent wheezers). Conversely, transient wheezers, comprising 50%–60% of preschool wheezers, experience symptom resolution without controller medications before the age of 6 years. 6 Transient wheezers commonly develop exacerbations triggered by viral upper respiratory tract infections (URIs). Studies indicate that intermittent high-dose ICS administration during URI can shorten symptom duration and reduce bronchodilator use.7,8 However, the routine use of daily ICS remains controversial, as it does not significantly reduce the frequency or severity of wheezing episodes, and evidence remains lacking for its use in preventing and managing of wheezing among preschool children.7,9 For example, 1 guideline recommends maintenance ICS for children with persistent or recurrent wheezing or severe exacerbations, but the optimal treatment duration is unclear. 10
The classification of “transient wheezer” is a retrospective epidemiological construct that can only be determined after longitudinal follow-up. At the time of clinical decision-making, clinicians cannot predict whether a child will follow a transient or persistent wheezing trajectory. Consequently, decisions regarding the initiation and duration of ICS therapy are based on the presenting clinical phenotype, commonly viral-triggered wheezing, rather than on a future epidemiological classification. In clinical practice, the duration of ICS therapy varies considerably, and evidence regarding the optimal duration and factors associated with its discontinuation remains limited. To address this gap, this study aimed to evaluate the time to successful ICS cessation and identify factors associated with delayed cessation in a cohort of children who were followed longitudinally and later classified as transient wheezers. Understanding the real-world duration of ICS use in this population may provide evidence to support further research and help inform future clinical guidelines regarding the rationale for ICS therapy in these children.
Methods
Study design
This retrospective study was conducted at the Pediatric Pulmonology and Allergy Clinic of Songklanagarind Hospital, Prince of Songkla University, Southern Thailand. Throughout the study period, there were 2–3 pulmonologists and 2–3 allergists practicing at the hospital. Patient data were retrieved from the hospital database using the International Classification of Diseases (10th Revision) and hospital drug codes. Patient recruitment involved (1) identifying children aged <5 years who visited the clinic between 2006 and 2021 with diagnoses of J45 asthma, J459 unspecified asthma, J458 mixed asthma, J451 non-allergic asthma, or R062 wheezing and who were prescribed ICSs; (2) excluding children with bronchopulmonary dysplasia or heart or neuromuscular diseases; (3) excluding children requiring ICS treatment for persistent wheezing after the age of 6 years. A manual chart review was subsequently conducted to identify children classified as transient wheezers based on the following criteria: (1) age <5 years having more than 3 wheezing episodes per year; (2) successfully discontinued ICS by 6 years of age; and (3) no wheezing episodes after age 7 years, as confirmed during subsequent hospital visits for unrelated conditions where wheezing was explicitly noted to be absent.
Ethics approval was obtained from the Ethics Committee of the Faculty of Medicine, Prince of Songkla University, Thailand (approval no. REC 65-517-1-1). A waiver for obtaining informed consent was granted for this study due to the de-identification of patient data.
Data collection
Data pertaining to the after variables were recorded: age, sex, perinatal oxygen use within 7 days of birth, atopic history, exposure to smoking, pet ownership, day care attendance, parental asthma, blood eosinophil count, aeroallergen sensitization, and ICS treatment duration.
Outcome measurement
ICS treatment duration was defined as the time between ICS initiation and cessation. The primary outcome was the time to ICS cessation, and the secondary outcome was factors associated with delayed cessation.
Definitions
Allergic rhinitis (AR) was defined as recurrent or persistent rhinitis symptoms (sneezing and/or itchy nose or a runny or blocked nose) with aeroallergen sensitization.
Non-allergic rhinitis (NAR) was defined with the same symptoms as above, without aeroallergen sensitization. Unspecified rhinitis (UR) was defined with the same symptoms as above, with unknown sensitization status. Atopic dermatitis (AD) was diagnosed by a physician based on chronic or recurrent skin lesions.
Skin prick testing (SPT) was used to evaluate 12 standardized common aeroallergens, including grass pollen (Johnson grass, acacia, and careless weeds), molds (Alternaria, Aspergillus mix, and Candida albicans), pets (cat pelt and dog epithelium), and insects (Dermatophagoides pteronyssinus, D. farinae, American cockroach, and German cockroach). Tests with histamine for positive control and glycerin for negative control were also performed. A mean wheal diameter with a value greater than that of the negative control by at least 3 mm was considered test-positive.
Successfully discontinued ICS was defined by no wheezing for at least 1 year after ICS cessation.
Statistical analysis
Analyses were performed using R software version 4.4.1 (R Foundation for Statistical Computing, Vienna, Austria). Descriptive data are presented as percentage, mean (standard deviations, SD), or median (interquartile range, IQR). ICS treatment duration was analyzed to determine time to cessation and was illustrated using a time to event curve. Sensitivity analyses were performed by reclassifying participants with missing data under best- and worst-case assumptions, and time-to-event analyses were repeated to assess robustness. Univariate analysis for factors associated with time to cessation of ICS was performed. Wilcoxon rank-sum test or Kruskal–Wallis test was applied to compare groups based on categorical variables. Multivariate analysis to identify associated factors of time to ICS cessation was conducted using a Weibull accelerated failure time (AFT) model. Statistical significance was set at P < 0.05.
Results
Patient characteristics
Figure 1 presents the study design and flow diagram. Of the 1,666 patients initially identified, those with underlying diseases or persistent wheezing beyond 6 years of age were excluded. Among the remaining 913 children, 38 had wheezing fewer than 3 times per year, 713 had unknown wheezing status after 7 years of age and were excluded. The final analysis included 162 children, all of whom had subsequent hospital visits for other medical conditions, confirming the absence of further wheezing. The mean (SD) age at the last visit was 11.2 (3.7) years (range, 7–23 years).
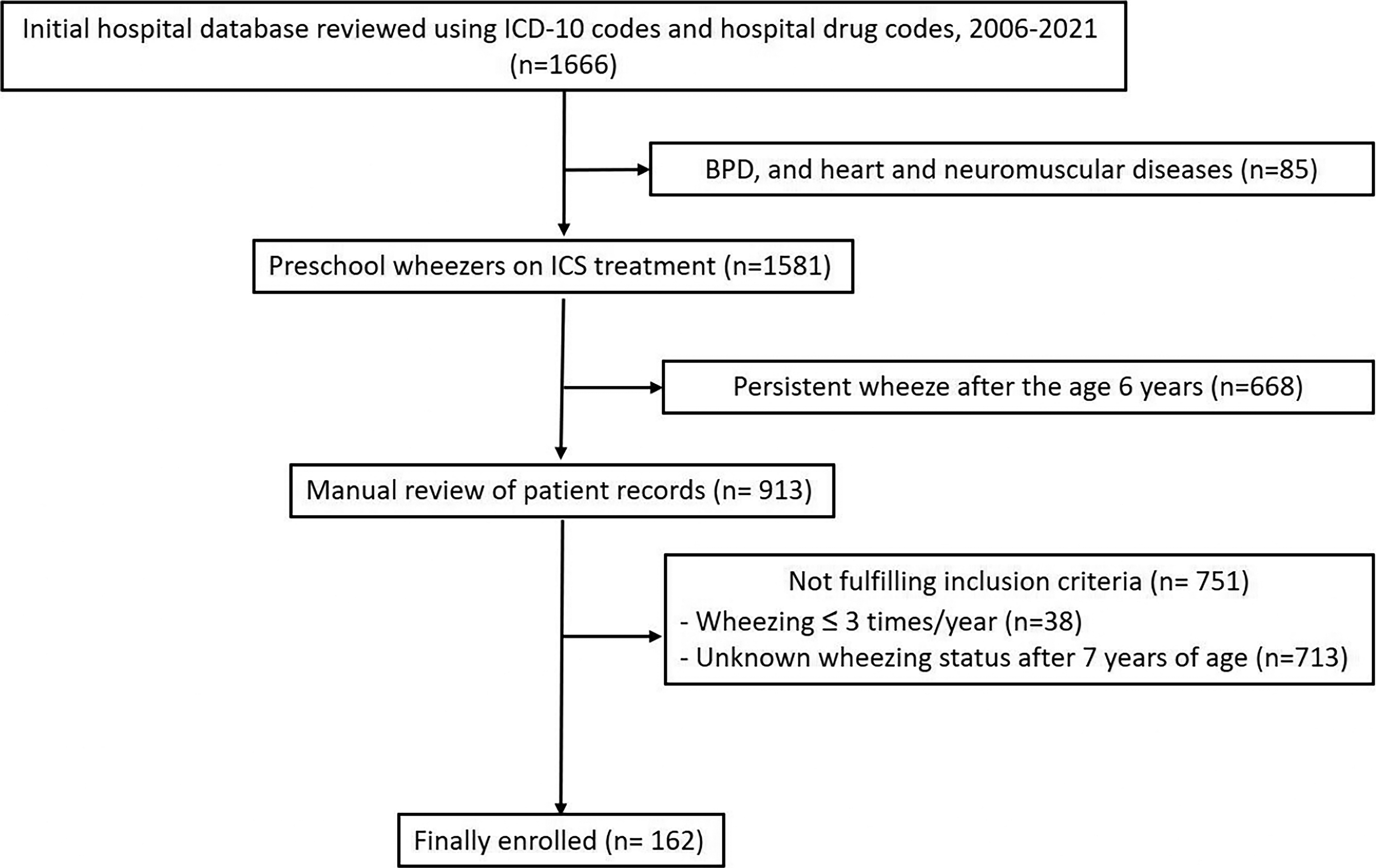
Study design and flow diagram. BPD, bronchopulmonary dysplasia; ICD-10, Intxernational Classification of Diseases, Tenth Revision; ICS, inhaled corticosteroid.
We further examined the excluded children. Among the 713 children with unknown wheezing status after 7 years of age, 139 had documented successful cessation of ICS before age 6, whereas the remaining 574 were lost to follow-up during ICS therapy and had insufficient baseline data. To evaluate potential selection bias due to incomplete follow-up, we compared baseline characteristics between the 139 excluded children and the 162 enrolled transient wheezers. The age at initiation and cessation of ICS was significantly younger in the excluded children, and the prevalence of AD was lower than in the enrolled participants. No significant differences were observed in other baseline characteristics. (Table 1)
Demographic and Characteristics of Enrolled Participants and Excluded Participants
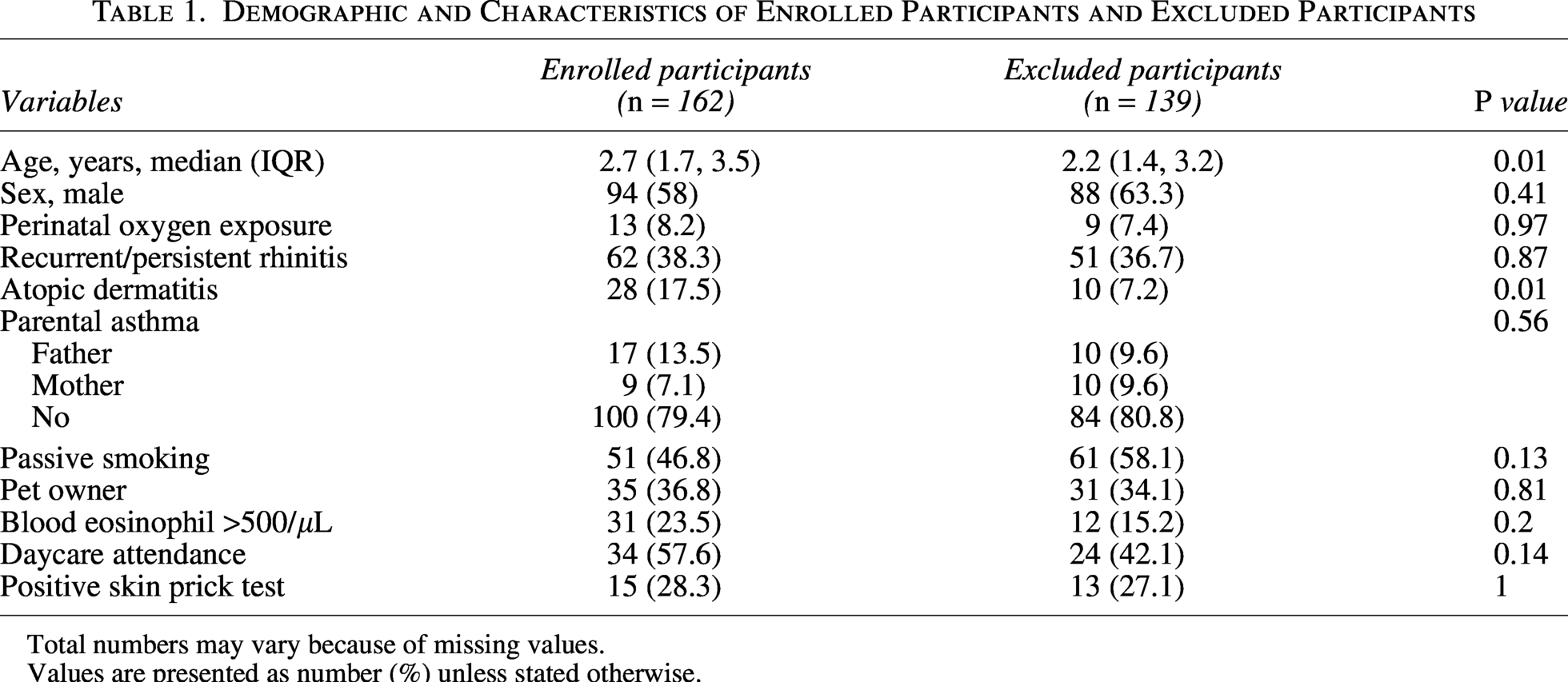
Total numbers may vary because of missing values.
Values are presented as number (%) unless stated otherwise.
ICS prescription patterns
All children received daily ICS therapy using either budesonide or fluticasone via a metered-dose inhaler with valved holding chambers at low to medium doses. Among the 162 children, 143 (88.3%) received ICS continuously until complete cessation. In the remaining 19 children (11.7%), ICS was temporarily discontinued for a short period but was later resumed to control wheezing.
Time to ICS cessation
Among the 162 enrolled transient wheezers, the median time to ICS cessation was 16.1 months (95% confidence interval [CI], 13.8–19.5). The cumulative probability of ICS cessation is shown in Figure 2.
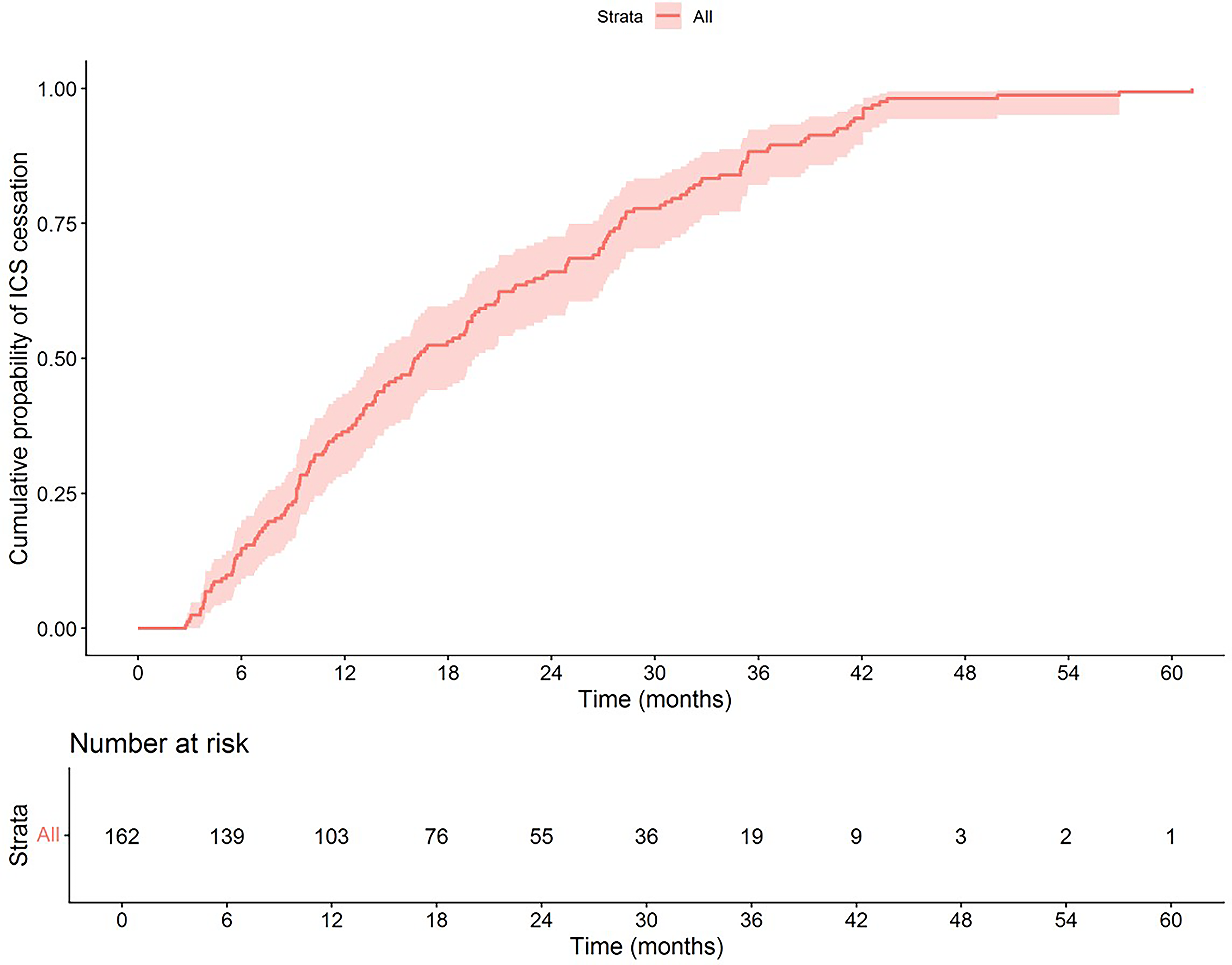
Time to cessation of inhaled corticosteroids (ICS) in a cohort of preschool children with transient wheezing (n = 162). The y-axis shows the cumulative probability of ICS cessation, and the x-axis represents time since ICS initiation. The curve depicts the cumulative proportion of children who achieved ICS discontinuation over time.
To evaluate the impact of the 139 excluded wheezers, sensitivity analyses were conducted using extreme-case assumptions. In the best-case scenario, all 139 children were assumed to be transient wheezers and were included in the enrolled group. The time to event analysis yielded a median time to ICS cessation of 16.4 months (95% CI: 14.6–19.1), which was comparable to the primary analysis. In the worst-case scenario, all 139 children were assumed to have persistent wheezing and were excluded from the enrolled transient wheezer group. Under this assumption, the median time to ICS cessation was unchanged from the primary analysis.
Associated factors for time to ICS cessation
In univariate analysis, a longer duration of ICS use was observed in younger children and in those with NAR and UR compared with children without rhinitis (Table 2). As the UR group may introduce heterogeneity, given that it could include either NAR or AR due to the absence of SPT results, this raises the possibility of misclassification bias. Therefore, a sensitivity analysis excluding the UR group was performed, and the association between NAR and longer time to ICS cessation remained significant. To further minimize potential misclassification bias, subsequent analyses were restricted to patients with confirmed SPT results. Multivariable analysis included age, NAR, and variables with borderline significance in univariate analyses (eosinophil count, pet ownership, and SPT status) (Table 2). In the multivariable AFT model, compared with children older than 3 years, the time ratio (TR) for discontinuation of ICS was 2.01 (95% CI: 1.62–2.49) for children younger than 2 years and 1.7 (95% CI: 1.35, 2.13) for those aged 2–3 years, indicating more than twice the time to ICS cessation among children younger than 2 years. Additionally, the presence of NAR was associated with a TR of 1.38 (95% CI: 1.09–1.76), indicating that these children required 38% longer to stop ICS treatment than those without rhinitis. (Table 3)
Univariate Analysis for Factors Associated with Time to Cessation of Inhaled Corticosteroids (n = 162)
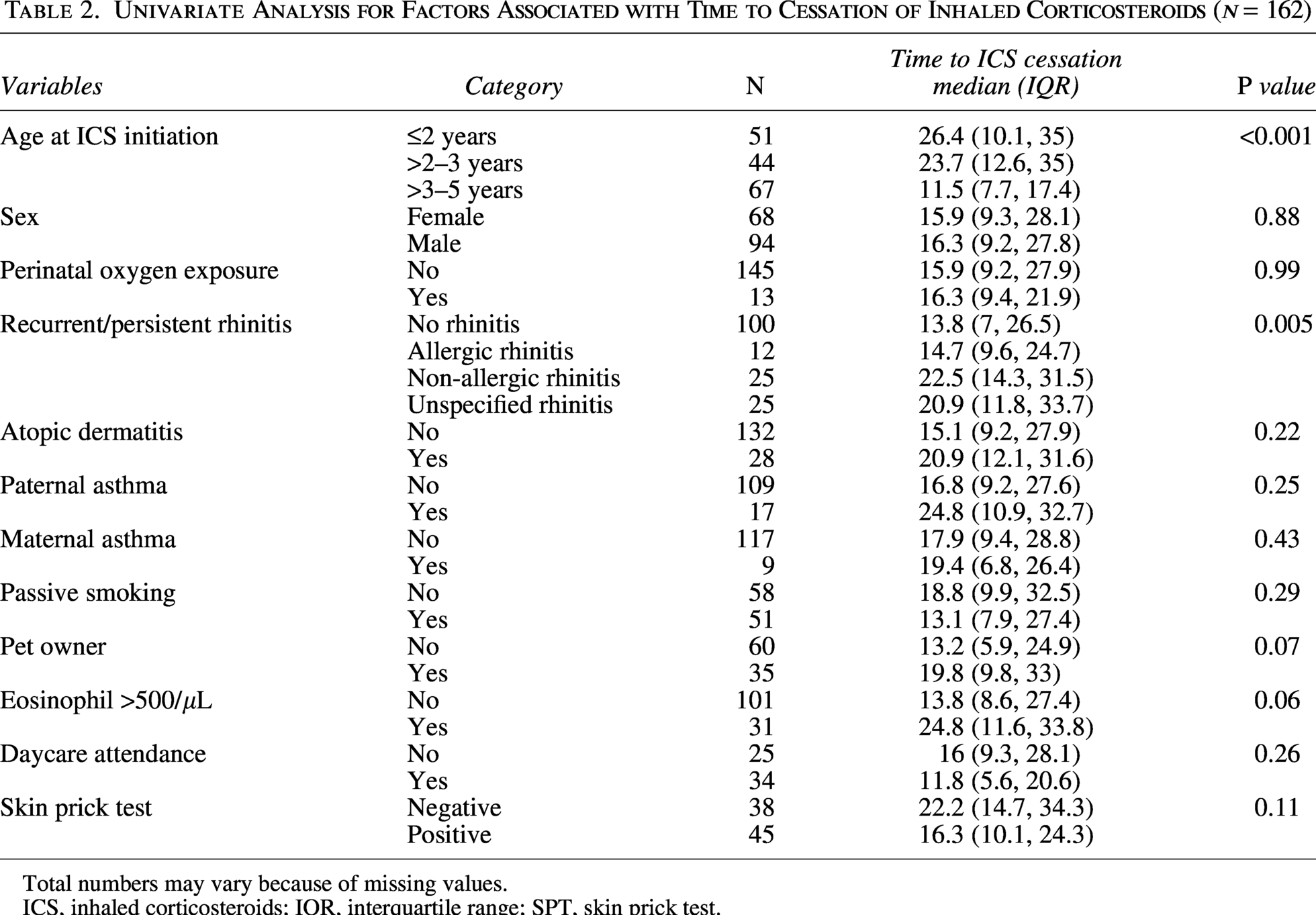
Total numbers may vary because of missing values.
ICS, inhaled corticosteroids; IQR, interquartile range; SPT, skin prick test.
Multivariate Analysis for Factors Associated with Time to Cessation of Inhaled Corticosteroids Using a Weibull Accelerated Failure Time Model
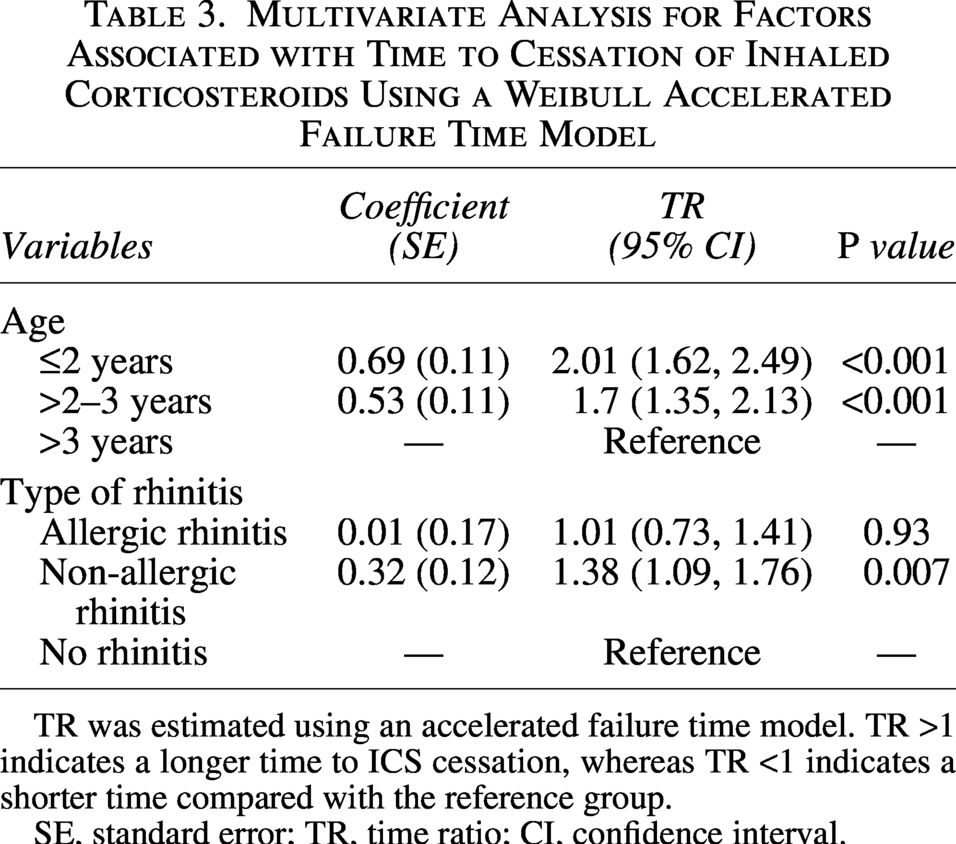
TR was estimated using an accelerated failure time model. TR >1 indicates a longer time to ICS cessation, whereas TR <1 indicates a shorter time compared with the reference group.
SE, standard error; TR, time ratio; CI, confidence interval.
Discussion
This retrospective study conducted at a tertiary hospital analyzed ICS treatment duration in children with transient wheezing to evaluate time to cessation and identify factors linked to delayed cessation. The recruitment method, which excluded preschool wheezers requiring ICS treatment beyond 6 years of age and featured long-term documentation of the absence of wheezing until an average age of 11 years, ensured that the participants predominantly had transient wheezing. To evaluate for potential selection bias, the results of sensitivity analysis found that excluded children initiated and discontinued ICS at a younger age and had a lower prevalence of AD than enrolled participants. Earlier initiation of ICS may reflect earlier onset of wheezing in these children. The lower prevalence of AD may also suggest a lower atopic predisposition in the excluded group. Although these differences suggest potential selection bias, other baseline characteristics were comparable between groups, supporting the overall robustness of the findings. This study shows that the duration of ICS use was relatively long, with a median time to ICS cessation of 16.1 months. However, this observed duration should be interpreted as a potential upper-bound estimate, rather than the minimal treatment duration necessary in routine clinical practice. One possible explanation for the prolonged ICS therapy is that our study population consisted mainly of children with frequent wheezing. This is supported by the enrollment data: out of 875 children with recurrent wheezing, only 162 (18.5%) were included in the study. The excluded children were those who did not continue follow-up at the clinic, possibly because their wheezing had resolved. Therefore, the children who regularly attended follow-ups likely had more severe or frequent symptoms, necessitating prolonged ICS treatment. In real-world clinical practice, without knowledge of a child’s eventual wheezing trajectory, decisions regarding long-term anti-asthma therapy depend on clinical risk factors such as frequent wheezing episodes, prior emergency visits for wheezing, personal allergic diseases, and day-care or kindergarten attendance. 11 However, concerns about potential medication side effects should also be considered, and treatment decisions should involve shared decision-making between physicians and parents.
In terms of ICS prescription patterns, physicians in this study demonstrated a preference for daily ICS regimens over intermittent prescriptions. This pattern mirrored standard asthma management, involving continuous ICS use until symptom control, followed by step-down treatment. Previous research on the efficacy of regular versus intermittent ICS use has yielded inconsistent results. Papi et al. found that regular glucocorticoid inhalation was the most effective treatment for frequent wheezing in preschool children, 12 whereas another study reported that the daily low-dose ICS regimen was not superior to intermittent high-dose regimens in reducing an exacerbation. 13 A systematic review of 29 randomized trials concluded that maintenance ICS therapy reduced exacerbations in preschool wheezers. 14 However, these findings were primarily driven by studies involving children with pronounced asthma features, potentially misrepresenting the efficacy of maintenance ICS in transient wheezers. Our study’s preference for daily ICS may stem from the severity or frequency of wheezing episodes or difficulty distinguishing transient wheezers from those with asthma, for whom daily ICS is preferred. This observed clinical practice, characterized by daily and prolonged ICS use, appears to exceed guideline recommendations, which generally advocate minimal ICS use in preschool wheezers.
This study also provides insights into the factors associated with the time to ICS cessation. In the multivariable analysis, younger age and NAR were significantly associated with longer durations of ICS prescription. The association with younger age may reflect the natural course of early childhood wheezing, which often persists during the preschool years before resolving around 6 years of age. NAR was also identified as an additional factor associated with time to ICS cessation. Based on chart reviews, we found that 38.3% of children had physician-diagnosed AR, which was identified through recurrent or persistent rhinitis symptoms (chronic rhinitis, CR). However, in young children, it is often difficult to distinguish AR from NAR based solely on clinical symptoms. To address this, we classified the children into 3 groups: AR, NAR, and UR, based on their SPT results. We found that NAR and UR were significantly associated with delayed cessation of ICS, while this association was not observed in children with AR. In a sensitivity analysis excluding the UR group, NAR remained significantly associated with a longer time to ICS discontinuation, supporting the consistency of the findings.
NAR is a condition that irritates the nasal passages, leading to inflammation and nasal symptoms, and diagnosis is usually made upon exclusion of an AR. 15 Studies in children with CR have shown that the proportions of NAR and AR differ among studies. Research conducted in Thai children found that among those under 4 years of age with CR, AR occurred more frequently than NAR (71% versus 29%). 16 In contrast, a study in Singapore reported that NAR was more commonly observed than AR in children under 2 years old with CR, accounting for 66.6% of all cases. The proportion of NAR decreased to 41.8% at ages 2–6 years and to 15% after age 6. 17 Regarding the connection between upper and lower airway diseases, AR is an inflammatory condition involving the nasal passages and paranasal sinuses. It is well established that patients with AR exhibit lower airway hyper-responsiveness, which can result in recurrent wheezing and a prolonged course of illness. 18 Although the link between NAR and wheezing symptoms is not well established, studies demonstrated that children with concomitant AR or NAR exhibit comparable frequencies of wheezing or asthma symptoms, irrespective of age.17,19 This suggests that inflammation triggered by non-allergic factors (such as smoke exposure, air pollution, infection, and weather changes 20 ), as seen in NAR, may also contribute to lower airway inflammation and lead to recurrent wheezing. However, despite the known link between NAR and recurrent wheezing, the observed association between NAR and prolonged ICS duration in our study should not be interpreted as causal. NAR classification relied on negative SPT results, yet a substantial proportion of children in this cohort did not undergo SPT. Moreover, aeroallergen sensitization is age-dependent and relatively uncommon in very young children, which may limit accurate rhinitis classification. Alternatively, persistent upper airway symptoms in children with recurrent wheezing may influence clinicians’ decisions to continue ICS therapy, potentially contributing to the observed association.
The rationale for using the AFT model for analysis is that the probability of ICS cessation is not constant over time, suggesting that time-to-event analysis is appropriate for modeling this outcome. Additionally, various clinical and demographic factors may influence both the likelihood and timing of cessation. In light of these considerations, we selected the AFT model, which enables direct interpretation of covariate effects on the time scale and does not rely on the proportional hazards assumption required by the Cox model. The Weibull distribution was selected because it accommodates monotonic hazard functions consistent with the observed cessation pattern, and it provided the best fit compared with alternative parametric distributions based on goodness-of-fit criteria.
This study has limitations owing to its retrospective design, including missing data for key variables. First, SPT, which predicts atopic wheezing through early sensitization to food and aeroallergens, 21 was performed in only 32.7% of participants. Lack of SPT limits the confirmation of transient wheezers among our study participants, for whom SPT should typically be negative. 22 In addition, the absence of SPT in many children with rhinitis symptoms, resulting in a large group classified as UR. The missing data mechanism is likely consistent with a missing-at-random pattern, as the performance of SPT depended on clinical indications and physician decision-making rather than random assignment. Second, daycare attendance data were available for only 36.4% of children. Daycare attendance increases the risk of respiratory infections, which can trigger wheezing, potentially prolonging the time to ICS use. Third, the absence of standardized local ICS treatment guidelines may have resulted in variation in the decisions among clinicians regarding the initiation, cessation, and resumption of ICS, potentially affecting treatment duration. Therefore, the time to ICS cessation observed in this study is likely a physician-driven outcome influenced by prescribing practices, rather than a pure reflection of disease remission. In addition, the findings describe patterns of ICS discontinuation within a retrospectively defined subgroup rather than identifying predictors applicable at treatment initiation. Because transient wheezers were classified post hoc based on long-term outcomes, the analysis is inherently subject to selection bias and limited causal inference. Fourth, as it was conducted in a single-center, tertiary-care setting, the generalizability of the findings to other settings, particularly primary care, where most preschool wheezers are managed, may be limited. Despite these limitations, this study provides valuable insights, as no previous study has examined the real-world practice regarding the time to ICS cessation in transient wheezers. In addition, the study is novel in determining factors associated with delayed ICS cessation.
In conclusion, among transient wheezers requiring ICS therapy, the median time to successful cessation was 16.1 months. This should be considered as a potential upper-bound estimate. The observed time to ICS cessation likely reflects physician-driven prescribing patterns. Younger age and concomitant NAR were associated with delayed discontinuation. These findings characterize real-world patterns of ICS use in children whose wheezing ultimately resolves and should be interpreted as descriptive rather than predictive. Prospective studies are needed to determine whether clinical factors can guide individualized decisions on ICS duration. In parallel, the development of evidence-based guidelines to optimize ICS discontinuation is warranted.
Authors’ Contributions
N.T. and W.A. designed the research study. N.T., W.A., and K.S. performed the research. K.R., K.S., and P.P. provided help and advice on the research. N.T. and W.A. wrote the article. K.S., K.R., K.S., and P.P. reviewed and edited the article. All authors read and approved the final article.
Ethics Approval and Consent to Participate
Ethics approval was obtained from the Ethics Committee of the Faculty of Medicine, Prince of Songkla University, Thailand (approval no. REC 65-517-1-1). A waiver for obtaining informed consent was granted for this study due to the de-identification of patient data. All procedures were performed in accordance with the ethical standards of the Institutional Review Board and The Declaration of Helsinki, and its later amendments or comparable ethical standards.
Footnotes
Author Disclosure Statement
There are no conflicts of interest to declare.
Funding Information
No funding was received for this article.