
Abstract
Introduction
Proximal femur fractures are common in older adults and are associated with high morbidity and mortality. Bone cement augmentation during intramedullary nailing has been reported to improve implant stability; however, its clinical utility and safety in Japan remain unclear.
Materials and Methods
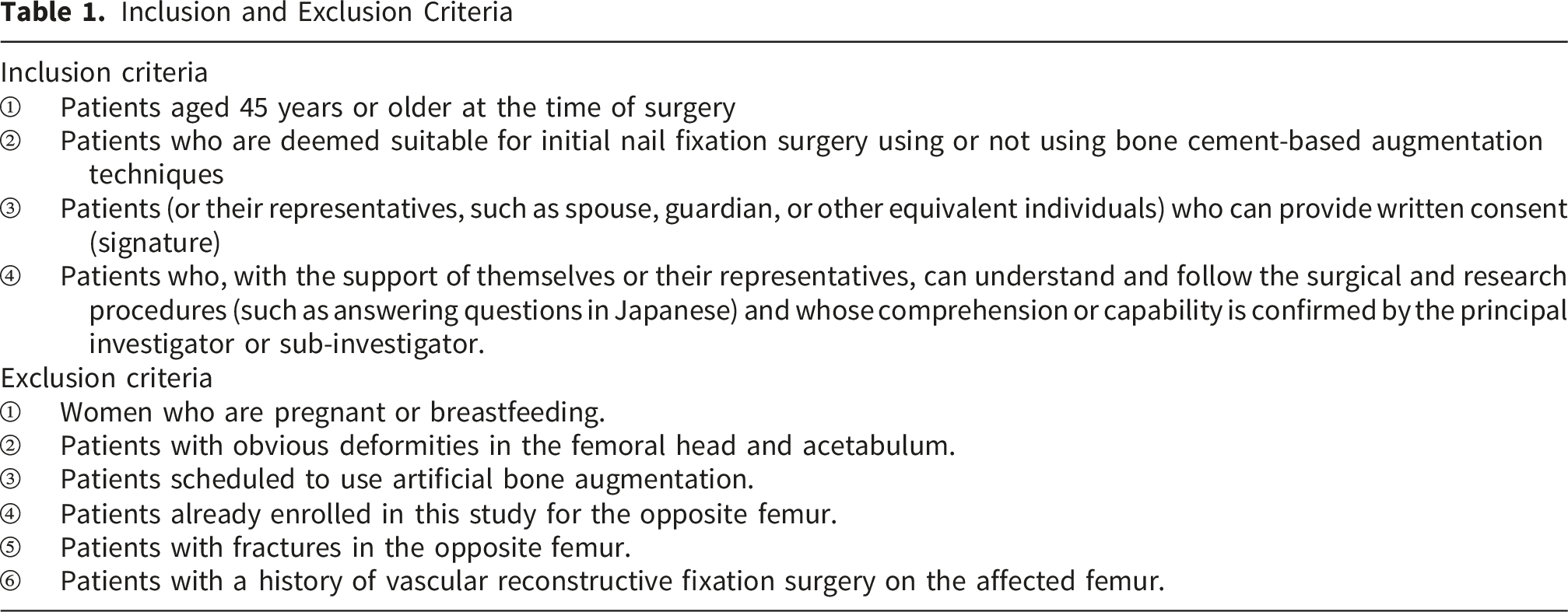
This multicenter prospective observational study included patients aged ≥45 years who underwent intramedullary nailing for trochanteric or basicervical femoral fractures between May 1, 2021, and July 31, 2023. Cement augmentation was applied exclusively to patients aged ≥60 years. Femoral neck fractures were excluded. Patients were treated with cement augmentation (CA group) or without augmentation (N group). The primary outcome was screw cut-out within 6 months postoperatively. Secondary outcomes included sliding distance (>5 mm), reoperation, nonunion, postoperative infection, and other complications. Group comparisons were performed using two-sided statistical tests with p < 0.05 considered significant.
Results
A total of 300 patients were analyzed (CA, n=97; N, n=203; mean age 86.8 years). No cut-out occurred in the CA group, whereas four cases (1.9%) occurred in the N group (p = 0.12). Sliding distance >5 mm was observed in 2 patients (2.0%) in the CA group and 12 patients (5.9%) in the N group (p = 0.108). Postoperative complications occurred in 2 patients (2.1%) in the CA group and 12 patients (5.9%) in the N group (p = 0.12). No cement-related adverse events were observed.
Conclusions
Cement augmentation during intramedullary nailing was safe and showed numerically lower rates of cut-out and excessive sliding compared with non-augmented fixation. Although statistical significance was not reached, these findings suggest a potential clinical role in elderly patients at high risk of fixation failure. Randomized controlled trials are warranted.
1. Introduction
Owing to the rapid aging of the global population, proximal femur fractures have become one of the most common and serious injuries among older adults. The reported 1-year mortality after such fractures ranges from 10% to 30%, reflecting their major clinical and socioeconomic impact.1,2 Early surgical fixation and prompt mobilization are essential for survival, functional recovery, and prevention of complications.
Intramedullary nailing is widely used for trochanteric and basicervical femoral fractures, and secure fixation of the femoral head element is crucial for maintaining fracture stability and enabling early weight-bearing. However, in elderly patients with osteoporosis, reduced bone quality weakens implant anchorage and increases the risk of mechanical failure such as screw cut-out or excessive sliding, which may lead to pain, delayed rehabilitation, and the need for revision surgery. 3
Bone cement augmentation using polymethylmethacrylate (PMMA) has been introduced to improve the fixation strength of femoral head elements. Several clinical and biomechanical studies from Western countries have demonstrated improved rotational stability and reduced cut-out rates with cement augmentation. Recent cohort studies have also reported potential benefits in early postoperative mobility and mechanical stability when cement augmentation is used in elderly patients with unstable trochanteric fractures.
In routine clinical practice, however, the decision to use cement augmentation is influenced by multiple factors, including patient age, bone quality, fracture pattern, and the surgeon’s assessment of fixation stability. In Japan, cement augmentation is not indicated for true femoral neck fractures but is increasingly considered for elderly patients with trochanteric or basicervical fractures at high risk of fixation failure. Despite its growing use, real-world multicenter data evaluating its effectiveness and safety in Japan remain limited.4-6
Therefore, we conducted a multicenter prospective observational study to evaluate the clinical utility and safety of bone cement augmentation in intramedullary nailing for proximal femur fractures in elderly patients. We compared outcomes between patients treated with and without cement augmentation, using cut-out as the primary outcome and sliding distance and postoperative complications as secondary outcomes.
2. Materials and Methods
2.1. Study Design and Participants
This was a multicenter, prospective observational cohort study conducted in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. The study was performed at five participating hospitals in Japan, including tertiary care centers and regional core hospitals that routinely provide surgical treatment for proximal femur fractures in elderly patients.
All surgeries were performed by board-certified orthopedic surgeons or senior orthopedic residents under direct supervision, following standard institutional protocols for intramedullary nailing. The choice of using bone cement augmentation or not was made by the treating surgeon based on routine clinical judgment, reflecting real-world clinical practice rather than randomized allocation.
2.2. Participants
Inclusion and Exclusion Criteria
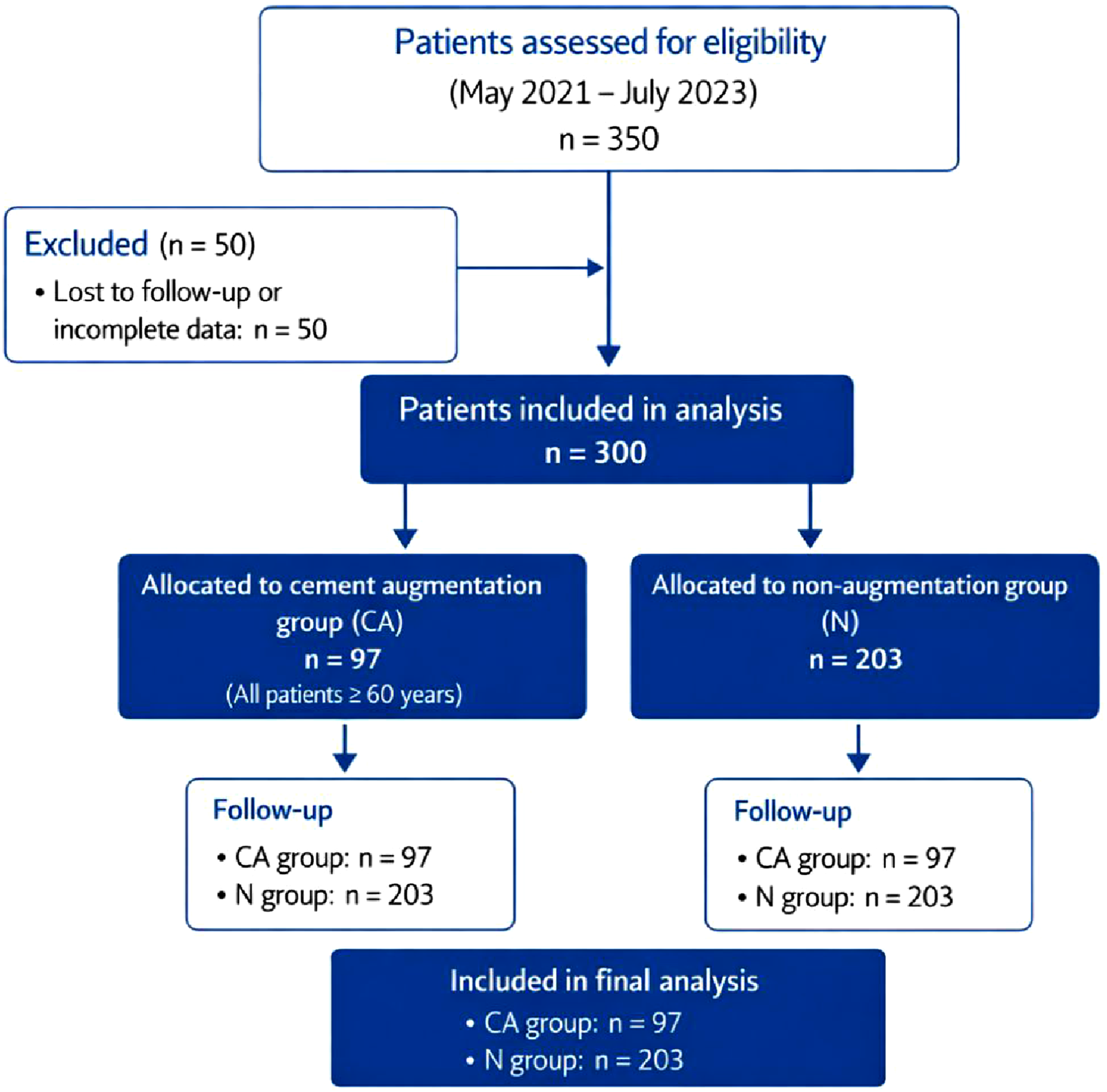
Flow diagram of patient selection, exclusion, and allocation to the cement augmentation (CA) and non-augmentation (N) groups
2.3. Exposure
The exposure of interest was the use of polymethylmethacrylate (PMMA) bone cement augmentation delivered through a fenestrated femoral head element of the Trochanteric Femoral Nail Advanced (TFNA) system during intramedullary nailing.
2.4. Outcomes
The primary outcome was screw cut-out within 6 months after surgery. Secondary outcomes included sliding distance, reoperation, nonunion, infection, and perioperative complications. Sliding distance was defined as >5 mm collapse of the head–neck segment relative to the femoral shaft, measured on standardized anteroposterior radiographs. All radiographs and CT images were anonymized and centrally reviewed. Fractures were classified using the Evans, Ikuta, and Ochi systems.
2.5. Statistical Analysis
Continuous variables were compared using the Student’s t-test or Mann–Whitney U test as appropriate. Categorical variables were compared using the chi-square test or Fisher’s exact test. A two-sided p-value < 0.05 was considered statistically significant. Because this elderly population was expected to have incomplete follow-up, the study protocol was designed to prospectively capture key outcomes during hospitalization and scheduled visits. Analyses were performed using available data without imputation. An a priori power analysis was performed based on an expected clinically meaningful difference in cut-out rates between groups (10% vs 5%), with a two-sided α level of 0.05 and 80% statistical power.
3. Results
Of the 350 patients aged 45 years or older who underwent surgery for proximal femur fractures at the five participating facilities, 300 were followed up. Among them, 97 patients who received augmentation were included in the case group (the CA group), and 203 patients without augmentation were included in the control group (the N group).
Demographic Data
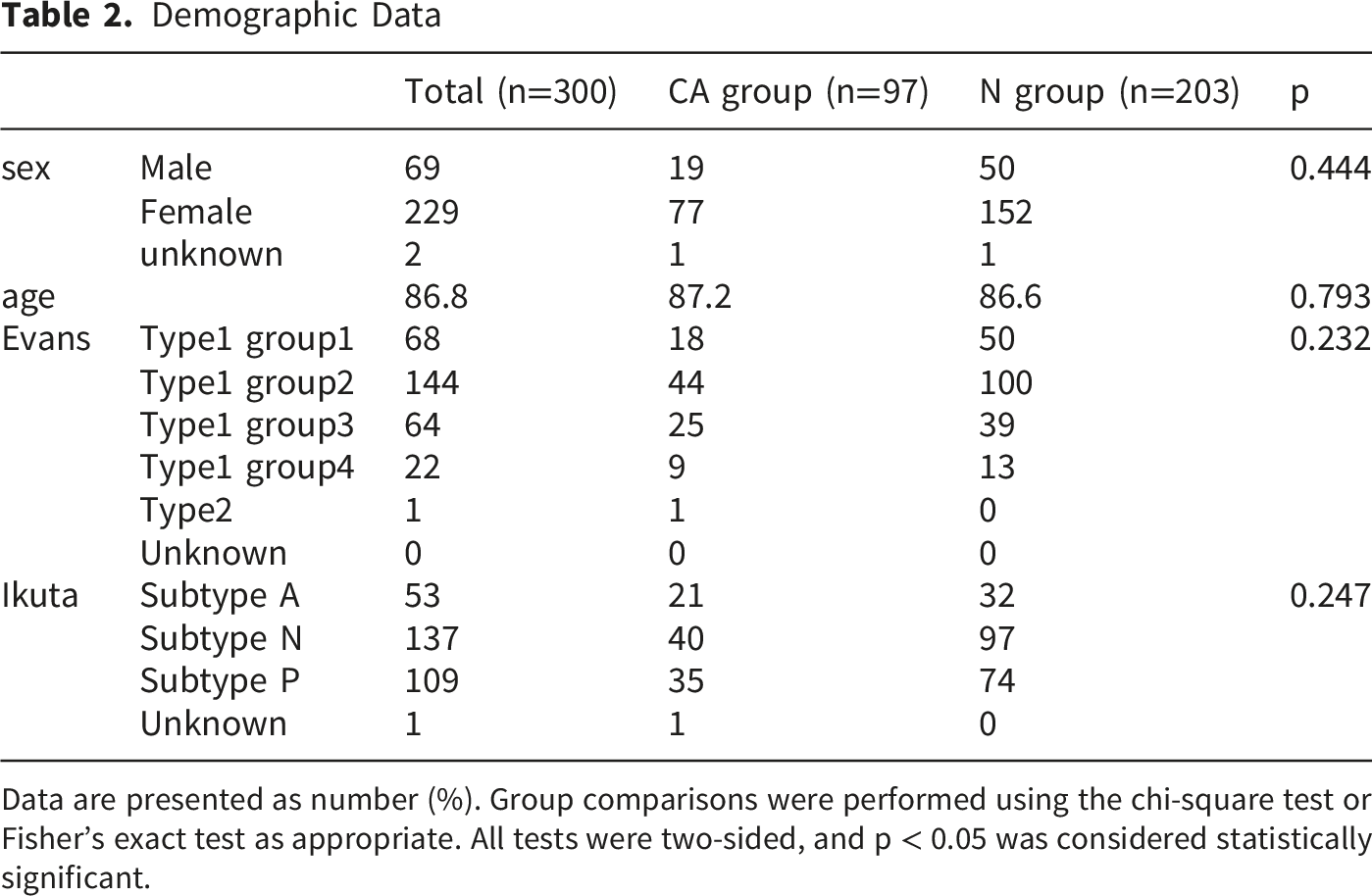
Data are presented as number (%). Group comparisons were performed using the chi-square test or Fisher’s exact test as appropriate. All tests were two-sided, and p < 0.05 was considered statistically significant.
Complication Occurrence
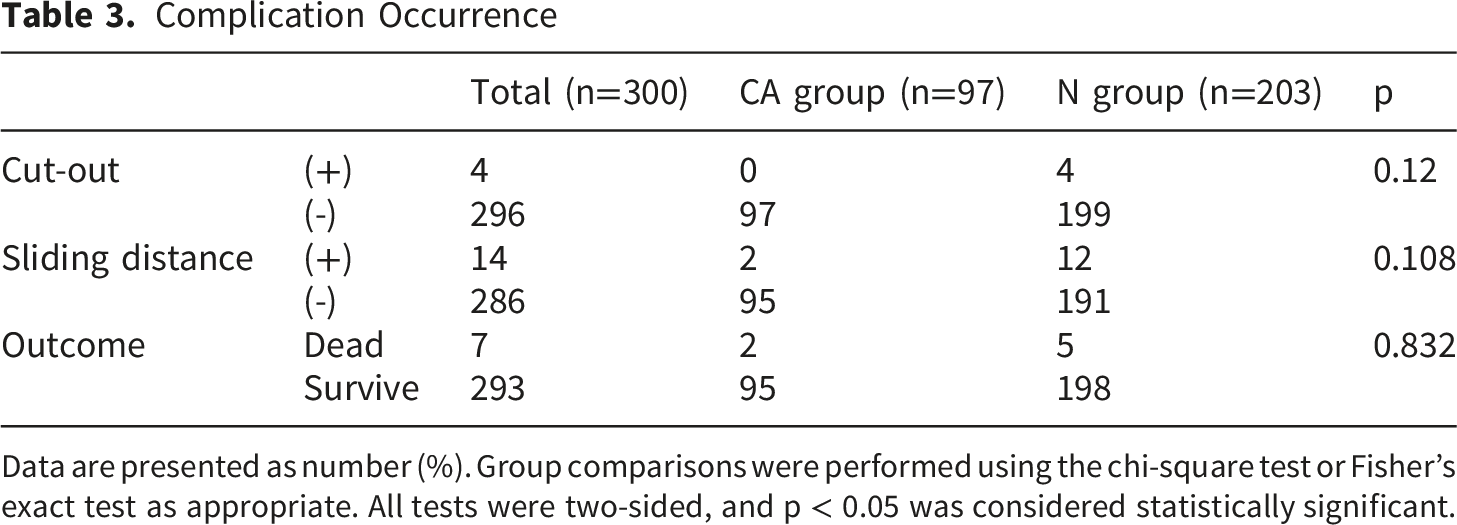
Data are presented as number (%). Group comparisons were performed using the chi-square test or Fisher’s exact test as appropriate. All tests were two-sided, and p < 0.05 was considered statistically significant.
Comparison in the Evans Classification Type 1 Groups 1 and 2
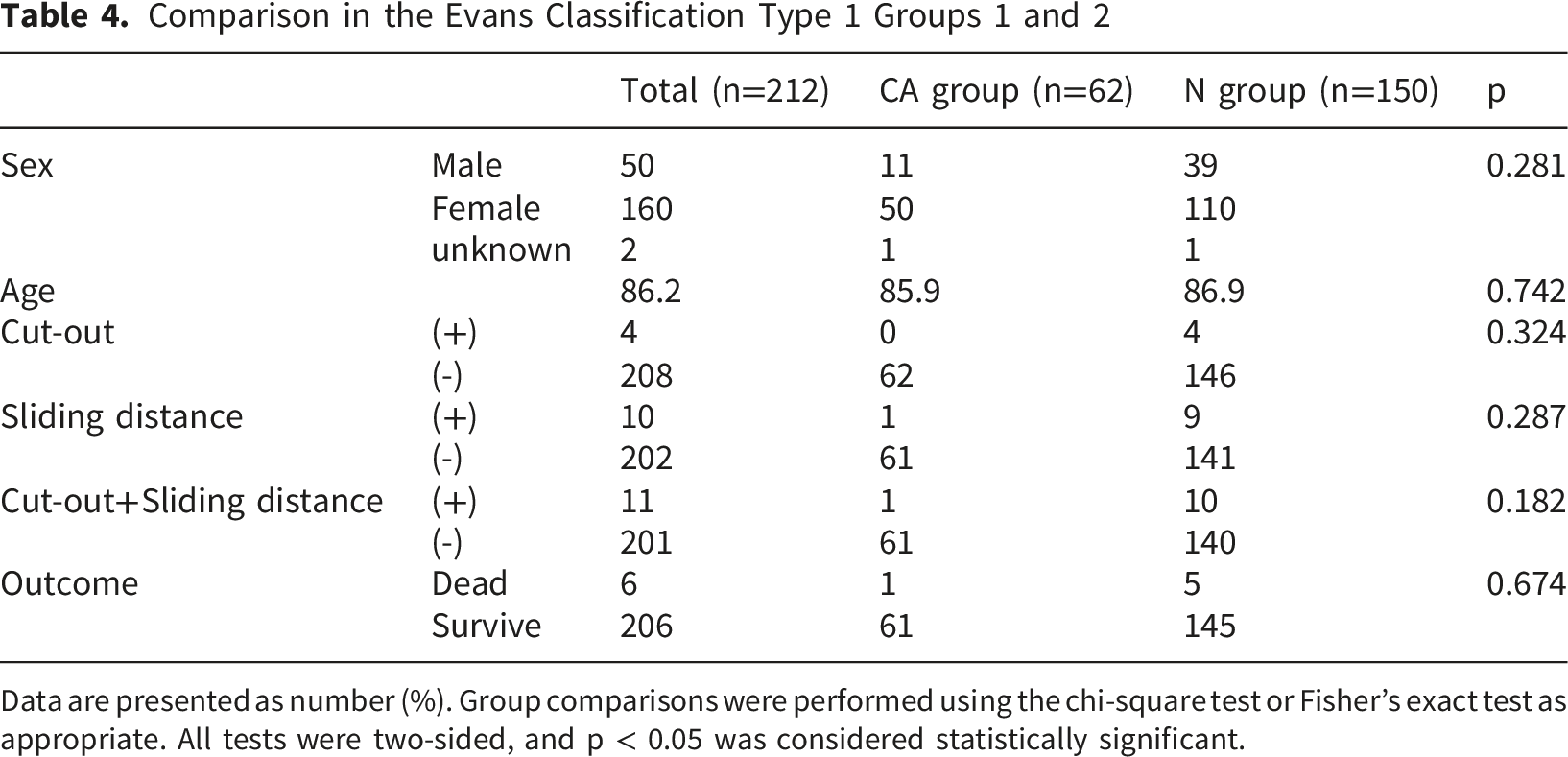
Data are presented as number (%). Group comparisons were performed using the chi-square test or Fisher’s exact test as appropriate. All tests were two-sided, and p < 0.05 was considered statistically significant.
Comparison in the Evans Classification Type 1 Groups 3 and 4
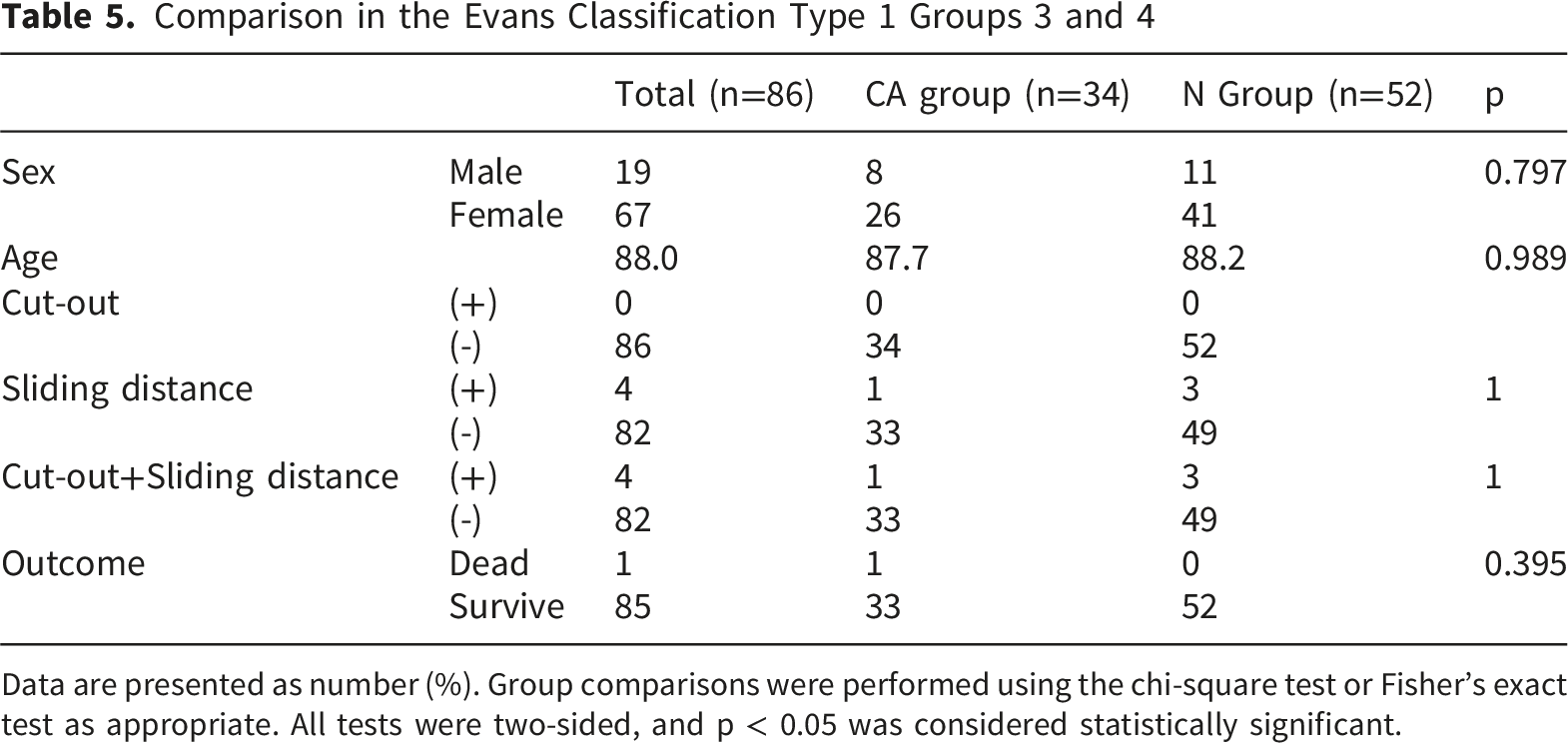
Data are presented as number (%). Group comparisons were performed using the chi-square test or Fisher’s exact test as appropriate. All tests were two-sided, and p < 0.05 was considered statistically significant.
There were 14 cases of postoperative complications, with 2 cases in the CA group and 12 cases in the N group (2.1% vs. 5.9%, p = 0.12). There were 7 deaths: 2 in the CA group and 5 in the N group (2.1% vs. 2.5%; p = 0.832). No adverse events related to the cement augmentation were observed in the CA group.
4. Discussion
In this study, among the 97 patients who received cement augmentation, no cases of cut-out were observed. In the group without cement augmentation, four cases (1.9%) had a cut-out, while no significant differences in patient backgrounds were found between the groups. Previous reports indicate that the cut-out rate for proximal femoral fractures ranges from 1.6–5.3% or 1.0–6.9%.7,8 Cut-out often requires screw removal or additional surgery, causing physical and emotional stress in patients, as well as increased medical costs. 9 Therefore, preventing cut-outs is crucial in the surgical treatment of proximal femoral fractures. 10
Factors that contribute to cut-out include surgical factors such as implant placement and fracture alignment and patient-related factors such as poor bone quality.11,12 Although surgical factors can be improved using medical techniques, it is difficult to influence patient-related factors, particularly in urgent cases. Proximal femoral fractures are more common in women, particularly after menopause, due to the rapid decrease in bone density. Women have approximately twice the risk of fractures compared to men, making bone quality a major concern for many patients. 13 Cement augmentation improves the stability of the implant by injecting polymethylmethacrylate (PMMA) bone cement into the femoral head, which enhances the rotational stability and resistance to cut-out. 14 In this study, the overall cut-out rate was low, and no cut-out was observed in the augmentation group.
Patients with proximal femoral fractures often experience various postoperative complications, making prevention crucial. Early surgery and mobilization are essential, and the fracture must be firmly stabilized to enable early weight bearing. Cut-out is one of the most critical postoperative complications; however, excessive sliding distance, which can cause pain and instability at the fracture site, is also problematic. These issues can hinder rehabilitation and make it more difficult for patients to resume daily activities. This study suggests that cement augmentation may help prevent excessive sliding distance by providing strong fixation between the implant and the femoral head. Biomechanical studies have shown that cement augmentation increases the resistance of both screws and blades, which lowers the cut-out rate.15,16 Although this study did not directly evaluate early functional outcomes, reduced sliding distance may contribute to improved rehabilitation. Because this was an observational study, the decision to use cement augmentation was not randomized and may have been influenced by factors such as age, sex, fracture type, and bone quality. Although baseline characteristics were similar between groups, residual confounding cannot be excluded. Nevertheless, this multicenter prospective design reflects real-world practice in Japan and provides clinically relevant evidence regarding the effectiveness and safety of cement augmentation in elderly patients at high risk of fixation failure.
Bone cement syndrome (BCS) is a serious complication associated with the use of PMMA bone cement. BCS can cause sudden hypoxia, low blood pressure, and loss of consciousness, and, in some cases, cardiac arrest. 17 In this study, no adverse events were observed in the 97 patients who underwent cement augmentation. Proximal femoral fractures primarily affect elderly patients, especially those aged ≥ 65 years. The rate of fractures increases with age owing to the progression of osteoporosis and muscle weakness, with even minor falls leading to fractures. According to Orimo, the incidence of proximal femur fractures in Japan has risen with aging, especially among women aged > 75 years. 18 In this study, the average patient age was 86.8 years, and even minor complications could have been serious. This study’s secondary aim was to assess the safety of cement augmentation. No adverse events were noted during surgery, likely due to careful injection technique, slow pressurization, and vigilant anesthetic monitoring.
The main limitation of this study is its observational nature, which may introduce selection bias regarding the choice of cement augmentation. Moreover, the surgical techniques may not have been consistent across facilities. However, we obtained informed consent from all patients, and the study was prospectively conducted at multiple facilities. No significant differences in patient backgrounds were found between the augmentation and non-augmentation groups, suggesting that our evaluation of the cut-out rate, sliding distance occurrence, and complication rate is more reliable than retrospective single-facility studies.
Although an a priori power analysis was performed, this study was designed as a prospective observational cohort study rather than a randomized controlled trial. However, the results suggest a potential role of cement augmentation in reducing the risk of cut-outs. Future prospective interventional studies with controlled surgical techniques are planned to confirm the effectiveness of cement augmentation.
5. Conclusion
This study’s findings suggest that bone cement augmentation with intramedullary nailing may be associated with improved mechanical stability and a reduced risk of complications in elderly patients. While further research and clinical trials are crucial, this method shows promise as a valuable treatment option for the future.
Footnotes
Acknowledgements
We thank Ayaka Suganami for her writing assistance.
Ethical Considerations
This study was approved by the Ethics Committee of Yokohama City University Hospital (Approval No. B210100012).
Consent to Participate
Patients provided informed consent to participate. Written informed consent was obtained from all participants.
Consent for Publication
Informed consent for publication was obtained from the participants or their legally authorized representatives. Non-essential identifying details have been omitted to protect the privacy of the participants. The authors hold written informed consent.
Author Contributions
Masahiro Matsumoto: Conceptualization, data collection, manuscript drafting, corresponding author. Hyonmin Choe: Study design, data analysis, manuscript revision. Naomi Kobayashi: Data interpretation, supervision. Kazuyoshi Yamamoto: Clinical data collection, critical revision. Kousuke Matsuo: Clinical data collection, validation. Hiroyuki Makita: Clinical data collection, supervision. Daisuke Enomoto: Data acquisition, investigation. Yuta Hieda: Data analysis, validation. Yutaka Inaba: Supervision, critical review of manuscript. All authors reviewed and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Johnson & Johnson K.K.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.