
Abstract
Background
Hip fractures are among the most common osteoporotic injuries in older adults, and early identification of high-risk individuals is essential for their prevention. Although dual-energy X-ray absorptiometry (DEXA) remains the standard method for measuring bone mineral density (BMD), access to this modality is limited in many regions. The deltoid tuberosity index (DTI), which is measured on proximal humeral images and visible on routine chest radiographs, may be a simple and accessible indicator of systemic osteoporosis.
Methods
This retrospective study included 1,012 patients aged ≥60 years who underwent surgery for hip fractures and had preoperative chest radiographs suitable for DTI measurement. The normal DEXA group consisted of 75 individuals with normal BMD (DEXA T-score ≥ –1.0) who had chest or shoulder radiographs taken within 6 months of their DEXA scan. DTI measurements were independently performed by two observers. Interobserver and intraobserver reliabilities were analyzed using intraclass correlation coefficients (ICC). Group comparisons, age-related associations, and receiver operating characteristic (ROC) analyses were conducted to evaluate the predictive performance of DTI.
Results
DTI was measurable in 74.7% of chest radiographs. The hip-fracture group showed significantly lower DTI values than the normal DEXA group (mean, 1.294; p<0.001). The measurement reproducibility was excellent, with inter- and intraobserver ICC values of 0.95. ROC analysis demonstrated strong discrimination for predicting hip fracture (AUC=0.903). The optimal cutoff value was 1.377, corresponding to 84.6% sensitivity and 86.7% specificity.
Conclusions
DTI is a simple, reliable, and easily obtainable measurement from routine chest radiographs and is strongly associated with hip fractures and systemic osteoporosis. Its high reproducibility and diagnostic performance highlight its potential as an opportunistic screening tool, particularly in settings with limited access to DEXA.
Keywords
Background
Hip fractures are among the most common fractures in the older population.1,2 In addition to posing a significant risk of mortality, they lead to long-term morbidity.3,4 Even with successful treatment, hip fractures result in long-term functional limitations, loss of independence, and a substantial burden on patients, caregivers, and healthcare systems.5-7 With an aging population, this burden is projected to increase in the future. 8 Therefore, developing strategies to prevent hip fractures is crucial, as osteoporosis represents one of their major underlying risk factors. 9 Although dual-energy X-ray absorptiometry (DEXA) is the gold standard for assessing osteoporosis, its worldwide use is limited by factors such as device availability and cost. 10 Therefore, various studies have proposed practical, affordable, and widely applicable radiological markers for diagnosing osteoporosis.11,12
Many studies have shown a correlation between proximal femoral cortical thickness index measurements and systemic osteoporosis.13,14 However, hip radiographs are not frequently obtained outside of arthrosis and trauma, limiting their use in incidental screening for osteoporosis. The most frequently obtained radiograph, both in older adults and the general population, is chest radiography. 15 The deltoid tuberosity index (DTI) is a parameter that can be evaluated in this regard. It indicates regional bone mineral density and is primarily used to determine the treatment of proximal humeral fractures, another type of osteoporotic fracture. 16 There are also studies demonstrating its relationship with systemic osteoporosis.17,18
In studies on DTI, images were obtained from humerus radiographs. The measured area is often cross-sectioned on chest X-rays, suggesting that DTI measurements may be possible. Nearly all hip fractures require surgical treatment, and a chest radiograph is often obtained during preoperative preparations. In our study, we aimed to obtain a cutoff value for hip fracture risk and osteoporosis by performing DTI measurements on the chest X-rays of these patients. DTI may serve as an opportunistic tool to help identify patients who may benefit from further osteoporosis evaluation, particularly in regions with limited access to DEXA devices.
Methods
Following approval from the local ethics committee, this study was conducted in accordance with the principles of the Declaration of Helsinki, using retrospective data collection through the hospital automation system. Preoperative chest radiographs of 1,354 patients aged 60 and older who underwent hip fracture surgery at our hospital between January 1, 2019, and June 30, 2024, were reviewed. A total of 1,012 patients with a proximal humerus suitable for DTI measurements were included in the study. The normal DEXA group consisted of 75 individuals who underwent DEXA examination during the same period, had a T-score ≥ -1.0, and had normal bone mineral density. 19 After a comprehensive scan of the patients’ radiological image archives, patients who underwent proximal humerus imaging within 6 months before or after the DEXA scan date were included.
Data Collection
Demographic data, including age and sex, were obtained from the hospital automation system. Clinical and radiological data related to the index hip fracture were retrieved from the institutional imaging and medical record databases. Only data corresponding to the first unilateral hip fracture event were used for analysis.
Study Population/Patient Selection
The inclusion criteria were age > 60 years and hip fractures resulting from simple falls. Data were used only for the date of the unilateral hip fracture. A formal a priori power analysis was not conducted for this study. Instead, the sample size was determined by the total number of eligible patients who underwent hip fracture surgery during the predefined study period and had preoperative chest radiographs suitable for DTI measurement. Given the initial uncertainty regarding the feasibility of DTI measurements on standard chest radiographs, all available data were included to maximize statistical power. The high rate of measurability (74.7%) resulted in a final sample size that was sufficient to detect significant differences between the groups. Patients with pathological fractures, fractures related to primary bone tumors or metastatic disease, and periprosthetic fractures were excluded from the study. Patients with previous implants in the proximal humerus that interfered with DTI measurement or resulted in unclear measurement margins were also excluded. In patients who sustained bilateral hip fractures during the study period, only the first fracture was included in the analysis; cases with bilateral fractures without available imaging records for the initial fracture were excluded.
DTI Measurement
The DTI was measured using the ratio of the outer cortical diameter to the inner endosteal diameter at the level where the cortices were parallel, just proximal to the deltoid tuberosity of the humerus (Figure 1). In sections where the deltoid tuberosity was not prominent due to rotation, measurements were taken at the approximate location of the deltoid tuberosity, where the cortex and medulla widths were 2 cm parallel. Patients with previous implants in the same location and unclear measurement margins were excluded from the study. The measurements were performed electronically using a PACS archiving and communication system. Measurements were performed independently by two orthopedic surgeons, and the average value from the two observers was used in the analyses for each case. Measurement of the Deltoid Tuberosity Index (DTI): DTI is calculated by dividing the outer cortical diameter (A) by the inner endosteal diameter (B) at the level where the humeral cortices run parallel just proximal to the deltoid tuberosity (DTI = A/B)
Intermeasurement Reliability Analysis
The reliability of DTI measurements was analyzed using two complementary approaches. In a subset of 40 randomly selected patients, both observers performed two repeated measurements, allowing calculation of intraobserver and interobserver intraclass correlation coefficients (ICC) values using two-way ANOVA models. Because each of the two observers also performed a single DTI measurement for all patients included in the study (n=1012), a second interobserver ICC analysis was performed on the full dataset to validate observer agreement at the population level.
Statistical Analysis
The distribution of continuous variables was assessed using the Shapiro–Wilk test. Variables that did not show a normal distribution were reported as median (IQR) or mean ± standard deviation. The Mann–Whitney U test was used for intergroup comparisons. The relationships between the variables were analyzed using Spearman’s correlation test. Receiver operating characteristic (ROC) analysis was performed with hip fracture as the positive outcome. Since lower DTI values indicate higher fracture risk, inverse DTI (1/DTI) was used so that higher test values corresponded to higher probability of hip fracture. AUC, sensitivity, specificity, and optimal threshold values (Youden’s index) were calculated. A p-value < 0.05 was considered statistically significant in all tests.
Results
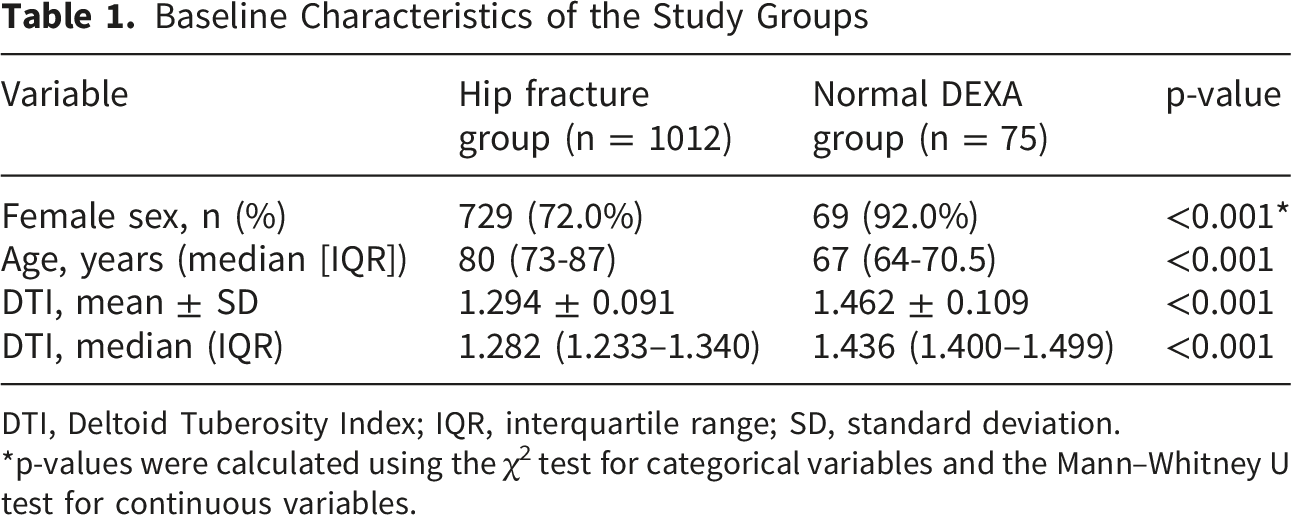
Of the 1,354 patients who underwent surgery for hip fractures, DTI values were measured in 1,012 patients from the evaluated chest X-rays, representing 74.7% of these patients. The normal DEXA group comprised 75 individuals who underwent normal dual-energy DEXA measurements. The DTI distributions between the groups were not normal (Shapiro–Wilk test, p<0.001). Therefore, nonparametric tests were used for comparison. DEXA also revealed a female predominance (72% in the hip fracture group and 92% in the normal DEXA group).
In the hip fracture group, DTI values were found to be 1.294 ± 0.091 (median: 1.282; IQR: 1.233–1.340), while in the normal DEXA group, DTI was found to be 1.462 ± 0.109 (median: 1.436; IQR: 1.400–1.499) (Figure 2). The difference between the two groups was statistically significant when evaluated with the Mann–Whitney U test (U=7370, p<0.001). In the effect size analysis, r=0.354, a moderate difference was found (Figure 3) (Table 1). Distribution of DTI values in the hip fracture and normal DEXA groups. Boxplots represent the median (horizontal line), interquartile range (box), and minimum–maximum values (whiskers). Individual data points are shown as dots. The hip fracture group included n = 1012 patients, and the normal DEXA group included n = 75 individuals Scatter plot comparing the relationship between Age and DTI in the study groups. The Hip Fracture Group (blue) predominantly exhibits lower DTI values compared to the Normal DEXA Group (orange) Baseline Characteristics of the Study Groups DTI, Deltoid Tuberosity Index; IQR, interquartile range; SD, standard deviation. *p-values were calculated using the χ2 test for categorical variables and the Mann–Whitney U test for continuous variables.

The performance of DTI in predicting hip fractures was evaluated using ROC curve analysis. Because lower DTI values were associated with hip fractures, inverse DTI (1/DTI) was used in the analysis so that higher values indicated higher fracture risk. The area under the curve (AUC) was 0.903, demonstrating excellent discriminatory performance.According to the Youden index, the optimal threshold value was 1.377, with a sensitivity of 84.6% and specificity of 86.7% (Figure 4). ROC curve showing the diagnostic performance of DTI
The relationship between age and DTI findings was evaluated separately for the two groups. In the hip fracture group, a significant negative relationship was found between age and DTI (Spearman r = –0.274, p < 0.001). Accordingly, DTI values tended to decrease with increasing age in this group. No significant relationship was found between age and DTI findings in the normal DEXA group (Spearman r = –0.040, p = 0.733) (Figure 3). When examined by sex in the hip fracture group, the mean DTI values were 1.287 and 1.311 in women and men, respectively. DTI values were slightly higher in men than in women, and this difference was statistically significant (Mann–Whitney U = 124.848; p = 0.010).
The reliability subset (n=40) demonstrated excellent intraobserver (ICC=0.96) and interobserver (ICC=0.95) agreement. In the full cohort (n=1012), the interobserver ICC based on single measurements from both observers also showed excellent agreement, confirming high measurement consistency at the population level (ICC=0.92).
Discussion
Hip fractures are among the most common fractures requiring surgical intervention in the older population and often occur after simple, low-energy falls due to underlying osteoporosis. With the increasing older population, effective strategies to prevent hip fractures have become increasingly important. DTI is a parameter measured in the proximal humerus and frequently appears within the field of view of chest radiographs. Because chest radiography is one of the most commonly obtained imaging modalities in older adults due to respiratory conditions, chronic comorbidities, or routine evaluations, this creates a significant advantage for the opportunistic assessment of bone quality. In our study, DTI measurements were feasible in 74.7% of chest radiographs, suggesting that this parameter may be applicable to a broad patient population. Obtaining a practical measurement from a frequently performed radiograph may support the identification of patients at increased risk of osteoporotic hip fractures and facilitate timely preventive strategies. Significant correlations between HU values and systemic bone mineral density have been reported in studies conducted in various anatomical regions, including the proximal femur, lumbar spine, wrist, and proximal humerus.20-23 However, the widespread use of CT for screening is limited due to its high cost and radiation exposure. Cortical thickness ratios measured in the distal radius and metacarpal bones have been shown to be associated with systemic bone density, and the proximal femur cortical thickness index has been reported to predict hip fracture risk.11,13 However, as wrist, hand, and femur radiographs are not routinely obtained in the older population, there are practical limitations to the use of these screening methods.
Various parameters, such as the Tingart and cortical indices, have been previously used to assess regional bone quality in the proximal humerus.24,25 Compared with these measurements, DTI is a more practical method owing to its acquisition from a defined anatomical reference point, ease of application, and high reproducibility. 16 The excellent intra- and inter-user ICC values obtained in our study demonstrate that DTI is a reliable measurement method. Initial DTI studies have shown that this measure reflects the local bone quality in the proximal humerus and can predict the risk of surgical complications.16,26 Spross et al reported that a DTI < 1.4 is associated with low proximal humeral bone mineral density; Handa et al similarly found that DTI values below 1.38 for the femur are associated with osteoporosis.16,17 In our study, the optimal threshold value for predicting hip fracture risk was 1.377, which was consistent with the accepted threshold value of 1.4 in the literature. If the DTI is 1.4 or below, individuals should be evaluated for osteoporosis, and fracture prevention interventions should be planned.
Da Silva et al reported that small differences in humeral rotation can affect DTI values and that the interobserver agreement is only moderate.
27
When a measurement technique is applied correctly, DTI can provide reliable results using a simple measurement method. Although humeral rotation may cause minor variations in absolute DTI measurements, bones with low DTI values reflecting thin cortices remain visually osteoporotic across different projections. Therefore, small rotation-related changes are unlikely to alter the overall risk classification (Figure 5). Representative examples of proximal humerus radiographs from different patients demonstrating increasing DTI values. These images do not represent different rotations of the same patient. (A) DTI = 1.1, (B) DTI = 1.2, (C) DTI = 1.3, (D) DTI = 1.4, and (E) DTI = 1.5
The significant negative correlation observed between age and DTI in the hip fracture group reflects the progressive cortical thinning associated with aging in high-risk individuals. Interestingly, this age-dependent decline was less pronounced in the normal DEXA group, suggesting that DTI captures pathological bone loss beyond physiological aging. Furthermore, although DTI values were higher in men than in women, the absolute difference was small. Given that osteoporosis in men is often underdiagnosed and undertreated, the ability to measure DTI on routinely acquired chest radiographs provides a valuable opportunistic means of patient identification for both sexes. From a clinical perspective, incorporating DTI assessment into routine practice could facilitate earlier patient stratification and guide referrals for DEXA, particularly in older patients where the risk of hip fracture is highest.This study had several limitations. The large proportion of the sample comprising female patients may limit the generalizability of the results to the male population. Another limitation of this study is the lack of an a priori sample size calculation. However, the inclusion of a large cohort (n=1012) and the highly significant differences observed between groups (p < 0.001) suggest that the study possessed adequate statistical power to validate the results. Furthermore, previous studies have reported that DTI measurement values may vary across populations. Therefore, it is important to determine the regional threshold values for DTI in studies conducted across different geographic and ethnic groups.25,28 The retrospective design and single-center nature of our study also limit the generalizability of the findings. Multicenter prospective studies will further clarify the clinical value of DTI in predicting the risk of hip fractures.
Conclusions
This study demonstrates that DTI, which can be measured from routinely obtained chest radiographs, is a robust and reliable radiological parameter associated with osteoporotic hip fractures. Significantly lower DTI values observed in patients with hip fractures, together with the high discriminatory performance in ROC analysis (AUC = 0.903), support its clinical relevance in fracture risk assessment. The identified threshold value of 1.377 is consistent with previously reported reference values, indicating that lower DTI values are associated with increased osteoporosis risk. Given its feasibility on a large proportion of chest radiographs and its high intra- and inter-observer agreement, DTI may serve as an opportunistic aid for identifying patients who may benefit from further osteoporosis evaluation, particularly in settings with limited access to DEXA.
Footnotes
Acknowledgement
The authors declare no acknowledgements.
Ethical Consideration
The study was approved by the local ethics committee (Sincan Training and Research Hospital Scientific Research Ethics Committee BAEK-135 numbered approval) and was conducted in accordance with the principles of the Declaration of Helsinki, using retrospective data collection through the hospital automation system.
Consent for Publication
All authors agreed with the content and all authors gave explicit consent to submit the study.
Author Contributions
The original idea and study design were developed by Nuri Koray Ülgen (NKÜ). Data collection was performed by NKÜ, Nihat Yiğit (NY), and Ünal Demir (ÜD). Radiographic measurements were conducted by NKÜ and ÜD. Statistical analyses were carried out by NKÜ, Ali Said Nazlıgül (ASN), and Arslan Kağan Arslan (AKA). The literature review was undertaken by NKÜ, Sadık Emre Erginoğlu (SEE), and AKA. The initial draft of the manuscript was written by NKÜ, while Mehmet Orçun Akkurt (MOA), Nurettin Mantı (NM), and ASN contributed to critical revision and editing of the manuscript. Overall supervision of the study was provided by MOA. All authors have read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.