
Abstract
Introduction
Dens fractures are cervical spine injuries with high morbidity and mortality in the elderly. Many patients require discharge to rehabilitation facilities or skilled nursing care, which impacts patient recovery, healthcare system resource allocation, and prognosis. This study evaluated the effect of trauma center level designation on discharge disposition in patients with dens fractures.
Materials and Methods
We conducted a retrospective study using data from a Texas State Trauma Registry from 2020 to 2022. Patient demographics, injury characteristics, and outcomes were queried in patients with dens fractures. Discharge home was defined as home discharge with or without home health services. Non-home discharge (NHD) was defined as discharge to another facility. Differences in discharge disposition were analyzed using adjusted binary and multinomial logistic regressions with 95% confidence intervals. Baseline characteristics were analyzed with chi-square and Kruskal-Wallis tests with post-hoc Dunn test for pairwise comparisons.
Results
A total of 904 patients were included. After excluding patients who died during hospitalization or were discharged to locations not included in the analysis (e.g., against medical advice, jail, or psychiatric facilities), 433 (52.9%) patients were discharged home while 385 (47.1%) patients had a NHD. Patients treated at level II trauma centers were almost twice as likely to have a NHD compared to patients who were treated at a level I (OR=1.98; 95% CI, 1.39-2.83; p<0.001). Lower-level trauma centers combined (levels II to IV) also had higher odds of a NHD compared to patients who were treated at a level I trauma center (OR=2.03, 95% CI, 1.47-2.79; p<0.001). These findings remained significant when patients discharged from the ED without inpatient admission were excluded (OR=1.52; 95% CI, 1.08-2.14; p=0.016).
Discussion
Patients with dens fractures treated at Level I trauma centers were significantly more likely to undergo home discharge than those treated at lower-level centers. Trauma center level may play an important role in discharge outcomes for this high-risk population. Further research is needed to identify specific practices contributing to this difference in discharge disposition.
Keywords
Introduction
Dens fractures represent the most common cervical spine injury in the geriatric population.1,2 These injuries, whether managed nonoperatively or operatively, are associated with significant morbidity, prolonged recovery, and a high likelihood of functional decline.3-9 Within the United States, many affected patients ultimately require discharge to rehabilitation facilities or skilled nursing care.10-13 As the elderly population continues to rise, the incidence of dens fractures and overall burden on the healthcare system is also expected to rise. 13 In this context, understanding the factors that influence discharge disposition has become increasingly important. Discharge destination has been shown to be a predictor of post-injury function, resource utilization, and long-term prognosis.14-16 Optimizing discharge planning not only has implications on patient recovery but also impacts resource allocation and healthcare systems.17,18
Trauma center designation reflects graduated differences in institutional capability. Level I and Level II trauma centers are equipped with on-call orthopaedic and neurosurgical services, enabling timely management of spinal trauma.19,20 In contrast, Level III and IV trauma centers do not require orthopaedic or neurosurgery spine coverage, which may limit their ability to manage spine injuries. While Level I and Level II trauma centers have spine coverage available, Level I trauma centers treat a higher volume of complex injuries, have more specialized resources and structured care pathways, and have greater experience managing high-acuity spinal conditions including dens fractures.21,22 Prior studies have documented improved outcomes for spinal cord injury patients treated at Level I centers compared to lower-level centers. 22 Other studies in broader trauma populations have similarly reported associations between higher trauma center designation and increased likelihood of post-acute care placement, suggesting that institutional resources and care pathways may influence discharge disposition beyond the severity of injury.23,24 Additionally, higher rates of discharge to skilled nursing facilities (SNFs) has been observed in trauma centers compared to non-trauma hospitals for patients with dens fractures. 11 However, there is no literature to our knowledge that evaluates the effect of trauma center level on overall discharge disposition in patients with dens fractures.
The purpose of this study was to examine whether the trauma level designation influenced discharge disposition in patients with dens fractures treated in Texas trauma centers from 2020-2022. We hypothesized that patients treated at Level I trauma centers would have higher rates of routine discharge home compared to those treated at Level II, III, or IV trauma centers.
Materials and Methods
The Acute Traumatic Injury Registry is one of four registries within the Emergency Medical Services and Trauma Registries (EMSTR), a statewide surveillance system maintained by the Texas Department of State Health Services. The EMSTR collects reportable event data from emergency medical services (EMS), hospitals, and rehabilitation facilities across Texas. This comprehensive registry contains over five million patient records annually. 25 For this study, patient data from the Acute Traumatic Injury Registry were queried from January 1, 2020, to December 31, 2022. All data were deidentified. Institutional Review Board (IRB) approval was not required, in accordance with applicable ethical and regulatory guidelines.
Cohort Selection
Patients with acute dens fractures of all ages were identified from the Acute Traumatic Injury Registry within the EMSTR using the following International Classification of Diseases, 10th edition (ICD-10) codes: S12.110A (anterior displaced Type II dens fracture, initial encounter for closed fracture), S12.111A (posterior displaced Type II dens fracture, initial encounter for closed fracture), S12.112A (nondisplaced Type II dens fracture, initial encounter for closed fracture), S12.120A (other displaced dens fracture, initial encounter for closed fracture), and S12.121A (other nondisplaced dens fracture, initial encounter for closed fracture). For all identified patients, data on demographics, injury characteristics, emergency department disposition, and hospital discharge disposition were extracted. Patients were excluded if their hospital discharge disposition or hospital trauma level was not recorded. To avoid duplicate entries and ensure completeness of outcome data, patients whose final disposition was a transfer to another hospital were excluded from the analysis while transferred-in patients were retained and analyzed at the receiving facility.
Hospital Trauma Level and Discharge Disposition Comparison
The trauma level of the treating hospital for each patient encounter was recorded as Level I, Level II, Level III, Level IV, or unknown. For the purposes of this analysis, patients treated at hospitals with an unknown trauma level were excluded. Discharge disposition was categorized as either home discharge or non-home discharge (NHD). A NHD was defined as discharge to another care facility including hospice, inpatient rehab facilities (IRF), skilled nursing facilities (SNF), or other care facilities. Long-term care facilities, intermediate care facilities, and short-term hospitals were combined into a single category for regression analyses due to small sample sizes in each individual group. Patients discharged against medical advice (AMA), to law enforcement, jail, or psychiatric units were excluded from the disposition analysis.
To account for potential bias related to transfer patterns, a secondary analysis was performed to compare discharge disposition among patients who were admitted to the hospital. Level III and IV trauma centers may not have on-call spine surgeons, which may necessitate transferring patients to level I or II trauma centers for appropriate care. This could lead to a higher proportion of patients discharged directly from the emergency department. This analysis was limited to patients admitted to the hospital in order to more accurately assess discharge disposition among patients requiring inpatient care. The relationship between hospital trauma level and NHD was analyzed using an adjusted binomial logistic regression to assess the likelihood of NHD across Level I, II, III, and IV trauma center designations. The regression model was adjusted for age, sex, race, Medicare status, injury severity score (ISS), diabetes, functional dependent status, and smoking.
Statistical Analysis
Baseline characteristics were summarized using medians for continuous variables and percentages for categorical variables. Continuous variables were assessed for normality using the Shapiro-Wilk test and compared with Kruskal-Wallis tests with post-hoc Dunn test for pairwise comparisons. Categorical variables were analyzed using chi-square tests. To account for multiple comparisons in baseline characteristic analyses, a Bonferroni correction was applied. A Bonferroni-adjusted p-value of less than 0.05 was considered statistically significant for differences in baseline characteristics and comorbidities. An unadjusted p-value of 0.05 was considered significant for all other statistical analyses.
In addition to the adjusted binomial logistic regression of home discharge vs NHD, we also conducted a multinomial logistic regression to model the odds of each specific discharge disposition (SNF, IRF, Hospice, and Other care facility) relative to the reference outcome of home discharge. Level I trauma centers were specified as the reference group compared to the other trauma centers. This regression model was also adjusted for age, sex, race, Medicare status, injury severity score (ISS), diabetes, functional dependent status, and smoking. Statistical analyses and modeling were performed using Python (Python Software Foundation, Wilmington, DE). Figures and tables were made using Microsoft Excel (Microsoft Corporation, Redmond, WA) and GraphPad Prism (GraphPad Software, San Diego, CA).
Results
Baseline Characteristics
Between 2020 and 2022, a total of 453,369 patients were recorded in the Acute Traumatic Injury Registry. Of these patients, 1,013 patients with dens fractures were identified. After excluding 109 patients due to missing or unknown trauma center level (n = 108) or missing discharge disposition (n = 1), 904 patients were included in the analysis (Figure 1). Among these patients, 312 patients (34.5%) were admitted to the intensive care unit (ICU). The overall in-hospital mortality rate was 8.2%. There were no statistically significant differences for in-hospital mortality between the trauma center levels (p = 0.075). The median age of the cohort of all patients with dens fractures was 79 years and 78.6% of the patients analyzed were 65 years or older. Flowchart with hospital disposition for patients with dens fractures
Baseline Demographics Between Patients at Various Trauma Levels
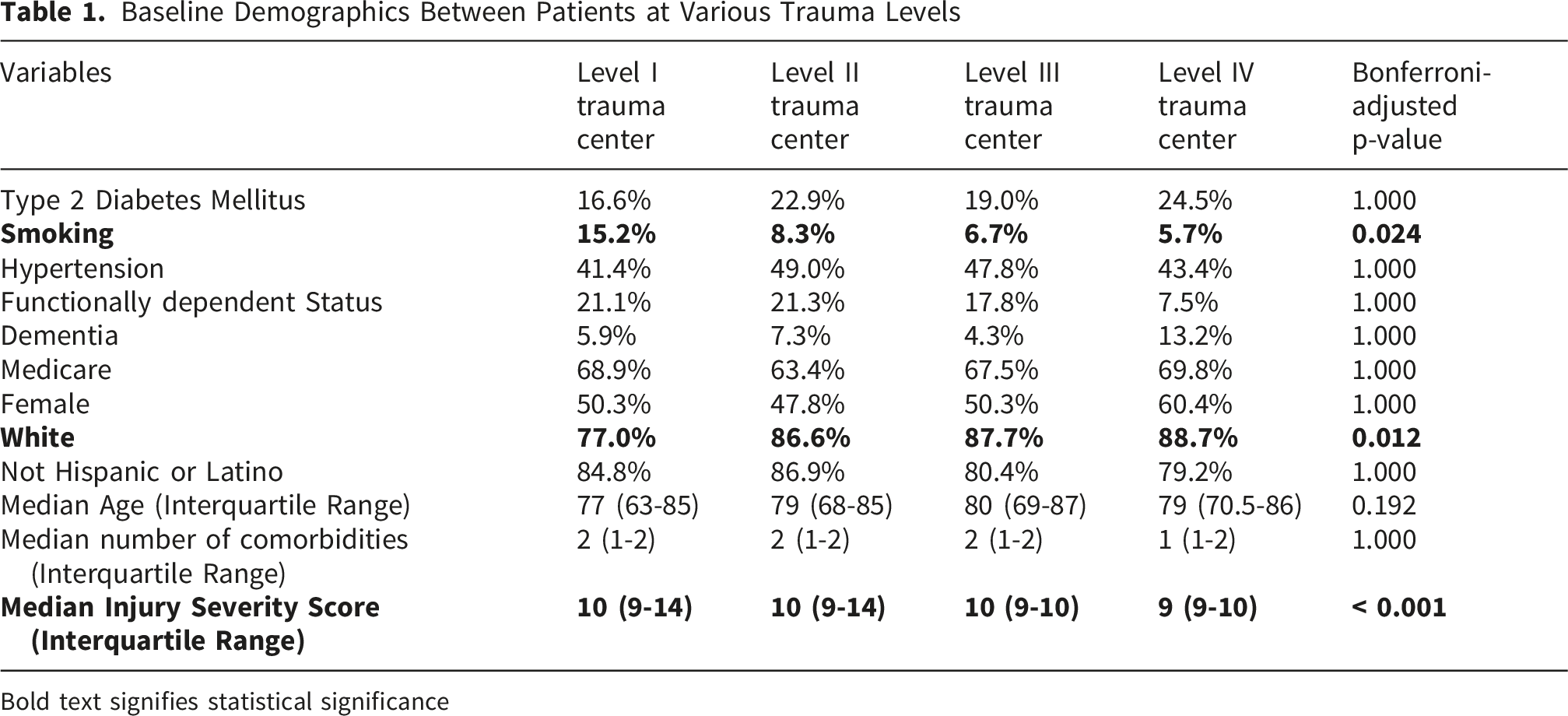
Bold text signifies statistical significance
Hospital Disposition
Effect of Hospital Trauma Level on Discharge Disposition
Discharge Disposition Compared With Trauma Center Level

After adjusting for covariates, patients treated at Level II trauma centers were almost twice as likely to undergo NHD compared to those treated at Level I centers (OR = 1.98, 95% CI, 1.39-2.83; p-value < 0.001). Patients treated at Level III (OR = 1.79, 95% CI, 1.17-2.75; p-value = 0.008) and Level IV trauma centers (OR = 3.89, 95% CI, 1.86-8.12; p-value < 0.001) also had increased odds of NHD compared to patients treated at Level 1 trauma centers. When Levels II, III, and IV trauma centers were combined, the odds of a NHD remained significantly higher compared to Level I centers (OR = 2.03, 95% CI, 1.47-2.79; p-value < 0.001). These findings are summarized in Figure 2. Effect of Hospital Trauma Level on Non-Home Discharge From Hospital in Dens Fractures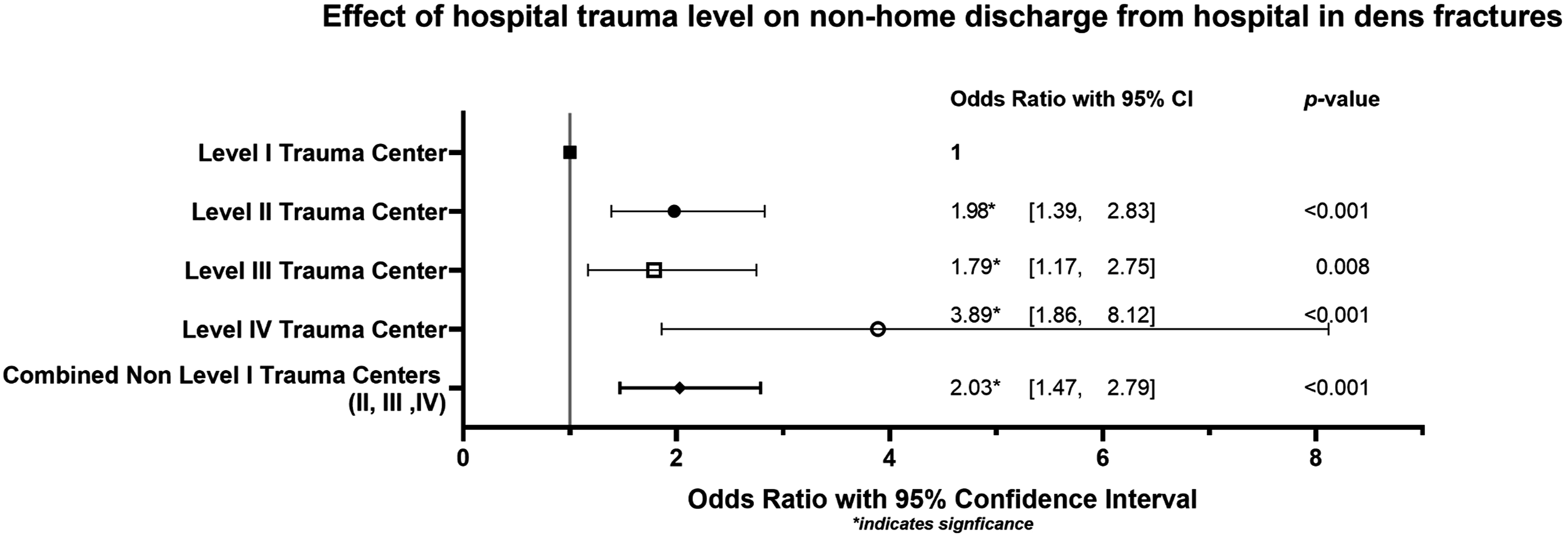
Multinomial Logistic Regression of Discharge Destination Compared to Home for Varying Trauma Center Levels Compared to Level I Trauma Centers

Bold text signifies statistical significance
A subgroup analysis was conducted comparing discharge disposition by hospital trauma level among patients who were admitted to the hospital, excluding those discharged directly from the ED without an inpatient stay. In this cohort, patients treated at Level II (OR = 1.46; 95% CI, 1.00-2.12; p = 0.049) and Level IV trauma centers (OR = 3.15; 95% CI, 1.44-6.89.; p = 0.004) remained significantly more likely to experience a NHD compared to those treated at Level I trauma centers. There was no statistically significant difference between NHD for Level I and Level III trauma centers (OR = 1.38; 95% CI, 0.88-2.17; p = 0.164). Collectively, patients treated at Levels II, III, and IV trauma centers also demonstrated a higher risk of NHD compared to those at Level I centers (OR 1.52; 95% CI, 1.08-2.14; p = 0.016).
Adjusted Odds Ratios From Logistic Regression on Non-home Discharge

Bold text signifies statistical significance
Discussion
Our study demonstrates that patients treated for dens fractures at Level I trauma centers were significantly more likely to undergo home discharge compared to those treated at other trauma centers, confirming our initial hypothesis. This association remained even after including only patients requiring inpatient care. We further characterized the different discharge dispositions following dens fractures and showed that this difference in NHD between Level I and non-Level I trauma centers is driven by significantly higher rates of discharge to SNFs, IRFs, and hospice. While we are unable to determine why there are higher rates of home discharge for Level I trauma centers versus other trauma centers in our present study, we speculate that the observed differences may be related to differences in institutional resources and care pathways.
Baseline characteristics and demographics were generally similar across all trauma center levels, although patients at Level I centers had a significantly higher prevalence of smokers. Level I and Level II trauma centers also had a significantly greater initial ISS compared to lower level trauma centers. Both smoking and higher ISS are established risk factors for adverse outcomes in dens fractures.3,27-29 Johnstone et al identified ISS as an independent predictor of mortality and discharge to SNFs in this population. 11 Despite treating a clinically more complex and at-risk cohort, our study demonstrated that Level I trauma centers achieved higher rates of home discharge, which may reflect differences in care coordination, among other institutional factors.
The 8.2% in-hospital mortality rate and 34.5% ICU admission rate in our cohort is consistent with prior literature with White et al reporting a 6.2% in-hospital mortality rate. 30 ICU admission rates have been reported between 40% and 46% following dens fractures in multiple studies.31-33 Dens fractures represent high-acuity injuries that may benefit from multidisciplinary management, given the complexity of management and the need for individualized approaches based on patient and injury characteristics.33,34,35 While non-level I trauma centers also provide multidisciplinary care, they may have more limited access to subspecialty services involved in the care of patients with dens fractures. 20 Level I trauma centers can provide comprehensive care with immediate access to orthopaedic and neurosurgical specialists, geriatrics, physical and occupational therapy, rehabilitation services, and critical care teams.19,20,36,37 Prior studies have documented improved outcomes for spinal cord injury patients treated at Level I centers compared to lower-level centers. 22 Other studies in trauma populations have similarly reported associations between higher trauma center designation and increased likelihood of post-acute care placement, suggesting that institutional resources and care pathways may influence discharge disposition beyond the severity of injury.23,24 Higher patient volumes at Level I centers may contribute to greater familiarity with spinal injury protocols and standardized care pathways that enhance patient outcomes. 21 Adequate institutional resources and early comprehensive care may partially explain discharge disposition following dens fractures. Daniels et al estimated the cost of treating C2 fractures, predominantly involving the dens, to exceed annual charges of over $1.5 billion as of 2010.1,17 As healthcare is increasingly aiming to prioritize value-based care, understanding treatment pathways that optimize resource utilization and patient outcomes is paramount. 38
Almost half of the patients in our study experienced a non-home discharge, with 20.6% discharged to SNFs. These findings align with reported SNF discharge rates after dens fractures, ranging from 19% to 42%.22,24,39 While previous literature has primarily evaluated discharge to SNFs, our study is the first to include NHD destinations such as IRFs, hospice, and other care facilities reflecting the significant and variable ongoing care needs after hospital discharge. 39 These results emphasize the morbidity and prolonged recovery associated with dens fractures. Our findings further demonstrate that the likelihood of these NHD, particularly to skilled nursing and inpatient rehab facilities varies significantly based on trauma center level. While the overall pattern of increasing non-home discharge across trauma levels was consistent, the smaller sample size for Level IV trauma centers and less common non-home discharge destinations, such as hospice or other care facilities, may limit our conclusions. The wide confidence intervals indicate instability and these findings should be approached with caution.
A strength of our study is that it includes data from a large, multi-year database, with a 904 patient sample treated across multiple trauma centers within Texas. This sample captured a wide range of practice settings and outcomes, which may enhance the external validity and generalizability of our findings. Additionally, our study characterizes specific NHD dispositions, which provides increased context on patient discharge outcomes following dens fractures.
However, our study has several limitations. The retrospective design restricts our ability to infer causation and limits our conclusions to associations. The reliance on trauma registry data introduces potential biases related to coding accuracy and completeness. Misclassification or inaccurate reporting of injury severity, comorbidities, or discharge disposition may impact our results. Due to lack of hospital-level identifiers within the dataset, we were unable to account for clustering of patients by treating hospital. This may underestimate standard error and increase chances of type I error. We were not able to directly measure information regarding care coordination, institutional resources, and multidisciplinary service involvement. Our proposed explanations underlying the observed differences in discharge disposition are speculative and cannot be directly evaluated. We were unable to longitudinally track individual patients across hospitals, limiting our assessment of inter-hospital transfers or repatriation. The inclusion of transferred-in patients and exclusion of transferred-out patients was done to mitigate duplicate data entries. However, this may bias our results, as outcomes reflect only the final treating hospital rather than the full care trajectory. Patients with more severe injuries may die, which introduces survivorship bias to our results for discharge disposition. Our analysis of discharge outcomes focuses on the cohort of patients who survived their initial hospitalization, and conclusions are limited to this population. While there was no statistically significant difference in functional dependent status between patients in various trauma centers, the database did not include validated measures of baseline functional status, frailty, complete comorbidity indices, or BMI. We were unable to determine operative versus non operative treatment, neurologic status, baseline residence, or fracture severity. These variables are relevant to discharge disposition and represent potential confounders in our analysis.34,35 Additionally, our study population is confined to trauma patients within Texas, which may limit generalizability to other regions with different healthcare infrastructures and patient demographics.
Conclusion
In conclusion, our findings indicate that patients with dens fractures treated at Level I trauma centers were significantly more likely to have home discharge compared to those treated at lower-level trauma centers. These results suggest that Level I trauma centers may positively influence discharge disposition, despite treating more at-risk patient populations. Further research is needed to identify specific protocols and practices at Level I centers that may be responsible for this disposition, which may help guide discharge optimization across trauma systems of varying levels in the future.
Footnotes
Ethical Considerations
This review was exempt from Institutional Review Board approval given its retrospective nature and lack of patient-identifiable information.
Consent to Participate
Not applicable as this study was a retrospective database study.
Author Contributions
Andrew Ni, MD contributed to conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, software, visualization, writing – original draft, and writing - review & editing. Doha Hussien, MD contributed to conceptualization, investigation, methodology, writing – original draft, and writing – review and editing. Abhi Rashiwala, MD contributed to investigation, methodology, writing – review & editing. Victoria Vargas, BS contributed to validation, data curation, writing – original draft, and writing – review and editing. Nasa Xu, MD contributed to conceptualization, data curation, formal analysis, writing – original draft. Jason McCartney, MD contributed to validation, writing – review & editing. Ralph Zachary Garza, MD contributed to supervision and project administration.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ralph Zachary Garza MD: Received payment for expert testimony from Texas Medical Legal Consultants, Medical Cost Contain, IMS Legal Services, and miscellaneous law firms. Owns stock or stock options in Bridgepoint MD.
Data Availability Statement
The data underlying this article are from the Acute Traumatic Injury Registry from the Emergency Medical Services and Trauma Registries (EMSTR) from the years 2020 to 2022. This data is maintained by the Texas Department of State Health Services. This data is available from the corresponding author upon reasonable request, subject to the data provider’s access restrictions.
Trial Registration
Not applicable. This study was not a prospective clinical trial and was not registered.