
Abstract
This study investigated the association between Internet addiction (IA) and suicidal ideation (SI) among Chinese adolescents, focusing on sex differences and the interactive roles of childhood trauma and depressive symptoms. A large-scale multicenter survey involving 24,470 students (mean age = 14.37 ± 1.52 years; 48.40 percent female) from three Chinese cities was conducted using standardized instruments to assess IA, SI, childhood trauma, and depression. Logistic regression and interaction analyses showed that IA was significantly associated with a higher likelihood of SI, with stronger associations observed among female adolescents. Childhood trauma and depressive symptoms significantly moderated the IA–SI relationship (interaction odds ratio [OR] = 6.81/6.88). However, stratified analysis showed that the association between IA and SI was stronger among adolescents without childhood trauma (OR = 3.38) than among those with childhood trauma (OR = 2.63), and the association was also stronger among adolescents without depressive symptoms (OR = 2.88) compared to those with depressive symptoms (OR = 1.80). These differences were primarily attributed to the higher baseline risk of SI among adolescents with childhood trauma and depressive symptoms, which attenuated the relative effect of IA. This effect was more pronounced during early adolescence. These findings suggest that IA may represent a potentially modifiable behavioral risk factor for SI in adolescents, particularly among females. The results highlight the importance of integrating digital behavior and mental health factors in adolescent suicide risk prevention, with a focus on comprehensive intervention strategies for adolescents with psychological vulnerabilities.
Introduction
With the rapid development of digital technologies, the Internet has become an indispensable part of daily life. Among adolescents in China, the Internet usage has reached 94.9 percent. 1 Internet addiction (IA) is generally defined as excessive and poorly controlled engagement in Internet-based activities that leads to functional impairment or psychological distress. 2 It is estimated to affect 8.1–26.5 percent of Chinese adolescents (aged 10–24 years).3–5 Internet gaming disorder, a specific form of problematic online behavior, was formally recognized in the 11th edition of the International Classification of Diseases in 2018. 6 This recognition highlights growing global concern regarding problematic online behaviors and their public health implications.
IA has been linked to various psychological problems and adverse outcomes, 7 among which suicide has attracted particular attention due to its severe consequences. Suicide is now the second leading cause of death among adolescents worldwide. 8 Suicidal ideation (SI) is the strongest predictor of suicidal behavior. 9 Studies indicate that 15–24 percent of Chinese adolescents (most under 18 years of age; mean age ≈ 15 years), have experienced SI, underscoring its substantial prevalence during adolescence.10,11
However, the association between IA and SI remains inconsistent. Some studies have reported a positive association,12,13 whereas others have found no significant relationship. 14 One potential explanation is that previous studies often relied on binary classifications of IA without considering its severity spectrum. Emerging evidence suggests that only severe IA increases the risk of SI. 15 These inconsistent findings highlight the need for large-scale studies examine the association between different levels of IA severity and SI.
The biological–psychosocial model of suicide provides a comprehensive framework, emphasizing the interplay of multiple risk factors. 16 Within this model, childhood trauma and depressive symptoms are recognized as key distal and proximal factors, respectively.17,18 In addition, childhood trauma and depressive symptoms may also influence adolescents’ Internet use. Some studies have indicated that individuals who have experienced childhood trauma or have depressive symptoms tend to exhibit more severe IA.19,20 However, it remains unclear whether IA interacts with these factors in influencing SI.
Sex differences have been observed, with IA being more prevalent among males and SI being more common among females.21,22 Prior research suggests that the pathways linking IA to SI may differ by sex. Female adolescents with IA may be more susceptible to internalizing pathways, such as depression, social comparison, and emotional dysregulation, all of which are strongly linked to SI. 23 In contrast, males with IA tend to exhibit higher impulsivity, externalizing behaviors, and gaming-related risk tendencies. These factors may contribute to alternative pathways leading to SI. 24 These differences suggest that the IA–SI association may vary by sex; however, this issue remains insufficiently explored.
Guided by the biopsychosocial model of suicide, 16 this study examined SI as the outcome of interacting behavioral, psychological, and contextual factors. IA was conceptualized as a potentially modifiable behavioral risk factor, whereas childhood trauma and depressive symptoms represent psychological vulnerability. These two variables were examined as moderators to assess whether the IA–SI association varies across different levels of vulnerability. Sex and age were included given established developmental and sex differences in IA and SI, and family and demographic characteristics were treated as covariates to account for potential confounding. This framework allows for the assessment of both the independent association between IA and SI and its variation across key subgroups.
Materials and Methods
Participants and data collection
Data were collected between June and August 2024 using a multicenter cluster sampling design. Secondary school students were recruited from 28 schools in three regions of China: Wuyuan, Yantai, and Rizhao. Paper-based questionnaires were administered during class meetings and completed under researcher supervision. Participation was voluntary, and written informed consent was obtained from both students and their parents/guardians.
The questionnaire took ∼15 minutes to complete. Of the 25,382 questionnaires distributed, 912 were excluded because of substantial missing data, inconsistent responses, or nonresponse. A total of 24,470 valid questionnaires were retained, yielding a valid response rate of 96.4 percent. The final sample had a mean age of 14.37 years (standard deviation [SD] = 1.52), and 48.40 percent were female.
A predefined suicide risk management protocol was implemented. Students screening positive for SI received further assessment, and those at elevated risk were referred to school psychological services or appropriate professional institutions for follow-up support. All participants were provided with information on available mental health resources. The study was approved by the affiliated institution’s Research Ethics Committee (2024-R-157).
Measures
Demographic information
A self-designed questionnaire was used to collect socioeconomic, family, and demographic information, including sex, age, grade, academic performance, personality, residence, family economic status, parental marital status, parental education level, and only-child status.
Internet addiction
IA severity was assessed using Young’s Internet Addiction Test, a 20-item scale rated on a 5-point Likert scale ranging from 1 (rarely) to 5 (always). 25 The Chinese version has been validated among Chinese adolescents (Cronbach’s α = 0.93). 26 Total scores range from 0 to 100: below 40 means no addiction, 40–59 mild, 60–79 moderate, and 80 or above severe. A cutoff of 50 was used to identify IA (Cronbach’s α = 0.913).
Childhood trauma
Childhood trauma was assessed using the Chinese version of the Childhood Trauma Questionnaire-Short Form, which has been validated among Chinese adolescents. 27 The questionnaire contains 25 items rated on a 5-point Likert scale ranging from 1 (never) to 5 (always). The questionnaire includes 25 items rated from 1 (never) to 5 (always). Total scores range from 25 to 125, with higher scores indicating more severe trauma. A score above 45 indicates high trauma (Cronbach’s α = 0.847).
Depressive symptoms
Depressive symptoms were assessed using the Children’s Depression Inventory (CDI), which was designed for children and adolescents. 28 The Chinese version has been validated among Chinese children and adolescents (Cronbach’s α = 0.88). 29 The CDI includes 27 items rated on a 0–2 scale, with higher scores indicating more severe depressive symptoms. A cutoff score of 19 was used to identify depressive symptoms. To avoid overlap with the SI outcome, Item 9, which assesses SI, was excluded from the CDI total score in this study (Cronbach’s α = 0.889).
Suicidal ideation
SI was assessed using Item 9 of the CDI: 0 = I do not have thoughts of suicide; 1 = I have thought about suicide, but I would never act on it; and 2 = I might commit suicide. Adolescents who scored “1” or “2” were classified as having SI. Item 9 is widely used in adolescent research and has been validated as a measure of SI.30,31
Statistical analysis
Descriptive analysis
Descriptive analyses were performed using SPSS version 27.0. Categorical variables were summarized as frequencies and percentages, whereas continuous variables were summarized as means and standard deviations. Differences between participants with and without SI, and between males and females, were examined using χ2 tests or two-tailed independent samples t-tests after assessing normality.
Binary logistic regression analysis
Binary logistic regression was performed to examine the association between IA and SI, with results reported as odds ratios (ORs) and 95 percent confidence intervals (CIs). Analyses were conducted in the total sample and further stratified by age group (10–14 vs. 15–19 years) to assess developmental differences in the IA–SI association. A hierarchical modeling strategy was applied with three progressively adjusted models.
Covariates were selected based on prior evidence and the biopsychosocial framework of suicide, with the aim of accounting for demographic, family/contextual, and psychological factors that may confound the association between IA and SI. Model 1 adjusted for demographic characteristics (sex, age, grade, academic performance, and personality). Model 2 further adjusted for family socioeconomic and environmental variables (family economic status, residence, parental marital status, only-child status, and parental education level). Model 3 additionally included childhood trauma and depressive symptoms as key psychological factors to evaluate whether the IA–SI association remained after accounting for these variables.
Subgroup analysis
Subgroup analyses were conducted to explore whether the IA–SI association differed by sex. Sex differences were assessed using ORs. To provide developmental context, additional analyses were performed within age groups (10–14 vs. 15–19 years) to examine sex differences separately across early and late adolescence.
Interaction analysis
Using the cutoff value, the study examined the interactive effects of IA with childhood trauma and depressive symptoms on SI separately and plotted the corresponding trend maps. Interaction analysis was also analyzed by age group.
Results
A total of 24,470 adolescents participated in the study (mean age = 14.37 ± 1.52 years), including 12,626 males (51.60 percent) and 11,844 females (48.40 percent). Among the sample, the prevalence of IA was 19.4 percent. In addition, 42.1 percent reported experiencing SI, 19.1 percent had a history of childhood trauma, and 27.5 percent exhibited depressive symptoms. The sample was divided into four IA severity groups: no addiction (n = 14,281, 58.4 percent), mild addiction (n = 8,660, 35.4 percent), moderate addiction (n = 1,367, 5.6 percent), and severe addiction (n = 162, 0.7 percent) (Table 1).
Characteristics of Participants (n, %)

Logistic regression results showed that IA severity was significantly associated with SI (Table 2). The adjusted odds ratios (aORs) changed only slightly from Model 1 to Model 2 (e.g., mild: 3.06–2.99; moderate: 7.68–7.44; severe: 10.62–10.26). However, after further adjustment for childhood trauma and depressive symptoms in Model 3, the associations were attenuated, with aORs decreasing to 2.14, 3.28, and 3.29 for mild, moderate, and severe IA, respectively. This association remained consistent across age groups.
Relationships Between Internet Addiction and Suicidal Ideation
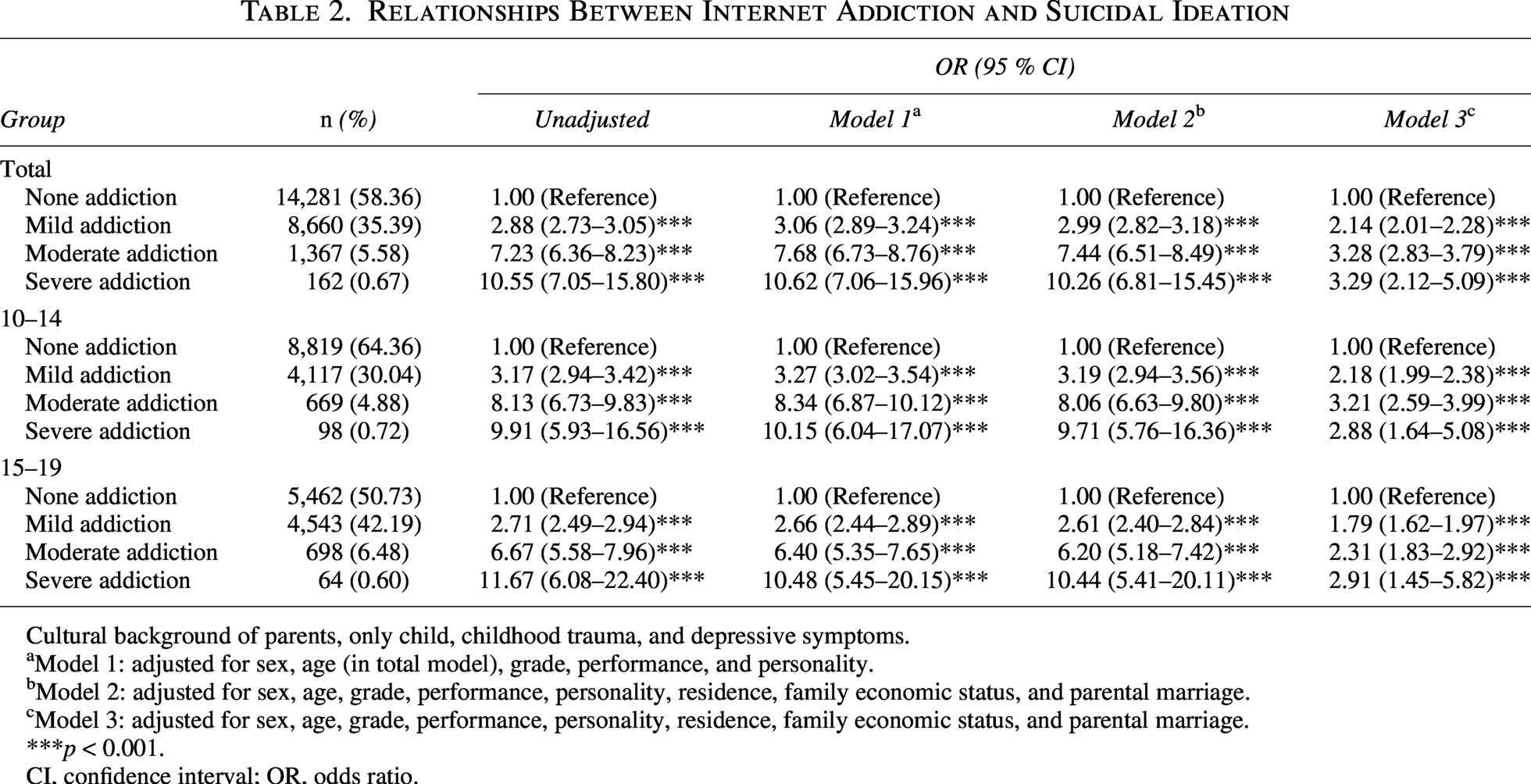
Cultural background of parents, only child, childhood trauma, and depressive symptoms.
Model 1: adjusted for sex, age (in total model), grade, performance, and personality.
Model 2: adjusted for sex, age, grade, performance, personality, residence, family economic status, and parental marriage.
Model 3: adjusted for sex, age, grade, performance, personality, residence, family economic status, and parental marriage.
***p < 0.001.
CI, confidence interval; OR, odds ratio.
Subgroup analyses indicated that IA was associated with SI in both males and females after adjustment for covariates (Table 3). In the overall sample, females exhibited higher aORs than males across all IA severity levels (mild: 2.27 vs. 1.99; moderate: 4.10 vs. 2.88; severe: 6.42 vs. 2.61), with sex differences observed in the mild and moderate addiction groups. Age-stratified analyses similarly showed generally higher aORs among females than males (10–14 years: mild 2.53 vs. 1.93, moderate 3.79 vs. 2.94, severe 3.79 vs. 2.46; 15–19 years: mild 2.07 vs. 2.07, moderate 4.37 vs. 2.89, severe 17.00 vs. 2.85). However, sex differences in early adolescence were primarily evident in the mild addiction group (2.53 vs. 1.93, p < 0.001), whereas no sex differences were observed in late adolescence (p > 0.05).
Relationships Between Internet Addiction and Suicidal Ideation by Sex
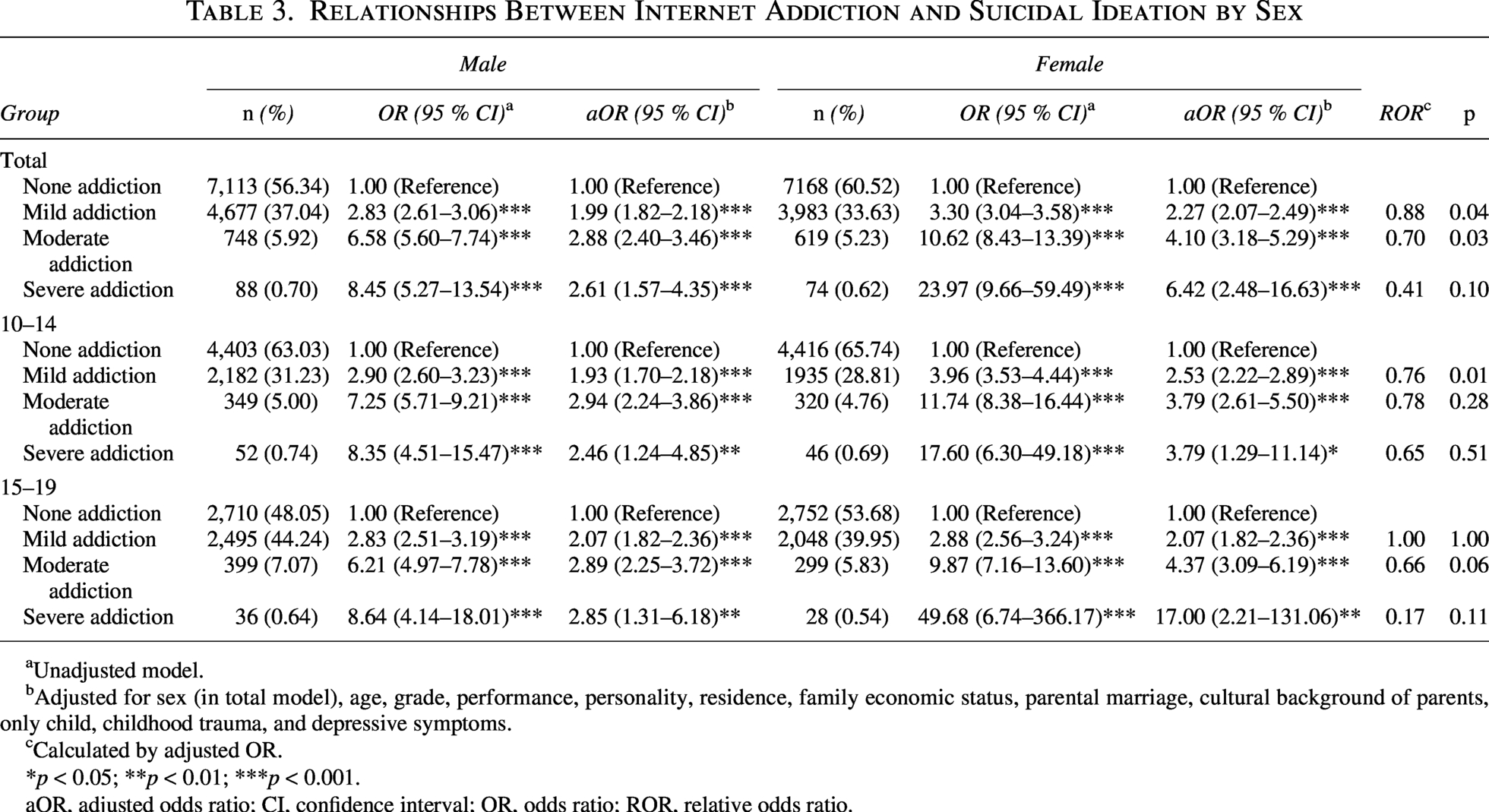
Unadjusted model.
Adjusted for sex (in total model), age, grade, performance, personality, residence, family economic status, parental marriage, cultural background of parents, only child, childhood trauma, and depressive symptoms.
Calculated by adjusted OR.
*p < 0.05; **p < 0.01; ***p < 0.001.
aOR, adjusted odds ratio; CI, confidence interval; OR, odds ratio; ROR, relative odds ratio.
Moderation analyses showed that childhood trauma and depressive symptoms influenced the association between IA and SI (Table 4). The IA–SI association was larger among adolescents without childhood trauma (OR = 3.38 vs. 2.63) and without depressive symptoms (OR = 2.88 vs. 1.80). As shown in Figure 1, adolescents with childhood trauma or depressive symptoms had a higher prevalence of SI across all IA severity levels, indicating a higher baseline risk in these psychologically vulnerable groups. However, the increase in SI prevalence across IA severity levels appeared steeper among adolescents without childhood trauma or depressive symptoms, suggesting a stronger relative IA–SI association in these lower baseline-risk groups. These findings support a subadditive interaction pattern, in which the relative contribution of IA appears attenuated among adolescents with elevated baseline SI risk. Interaction estimates indicated that the joint presence of IA and these psychological factors was associated with a higher risk than IA alone (interaction OR = 6.81/6.88), with stronger interaction patterns observed in early adolescence.
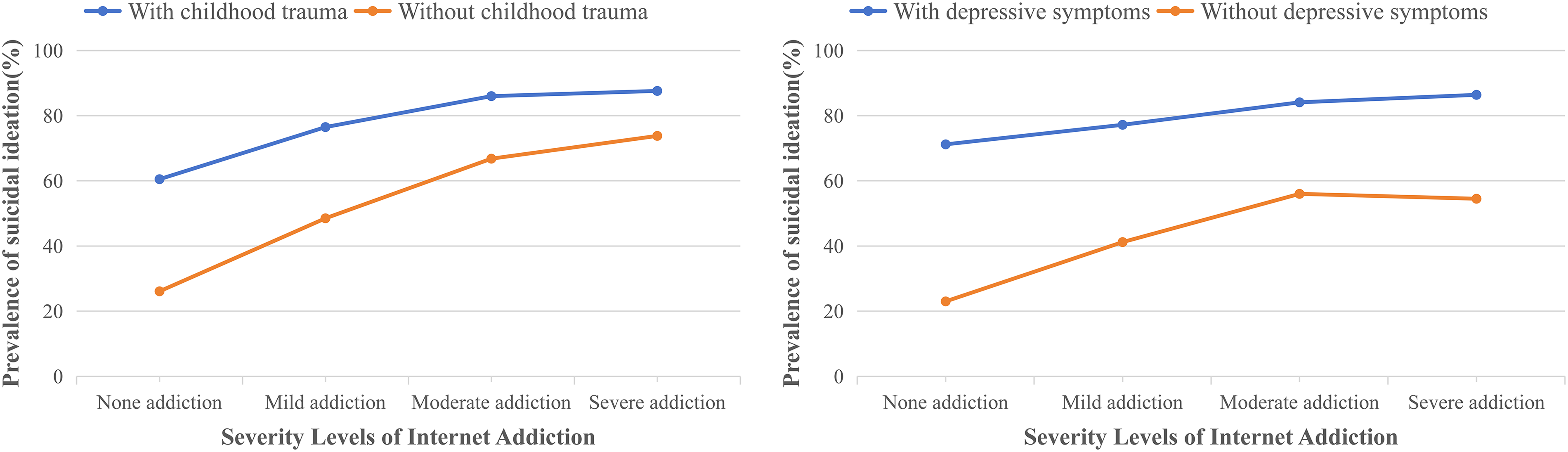
Association between severity levels of Internet addiction and suicidal ideation in adolescents.
Interaction and Stratified Analysis Between Internet Addiction and Suicidal Ideation
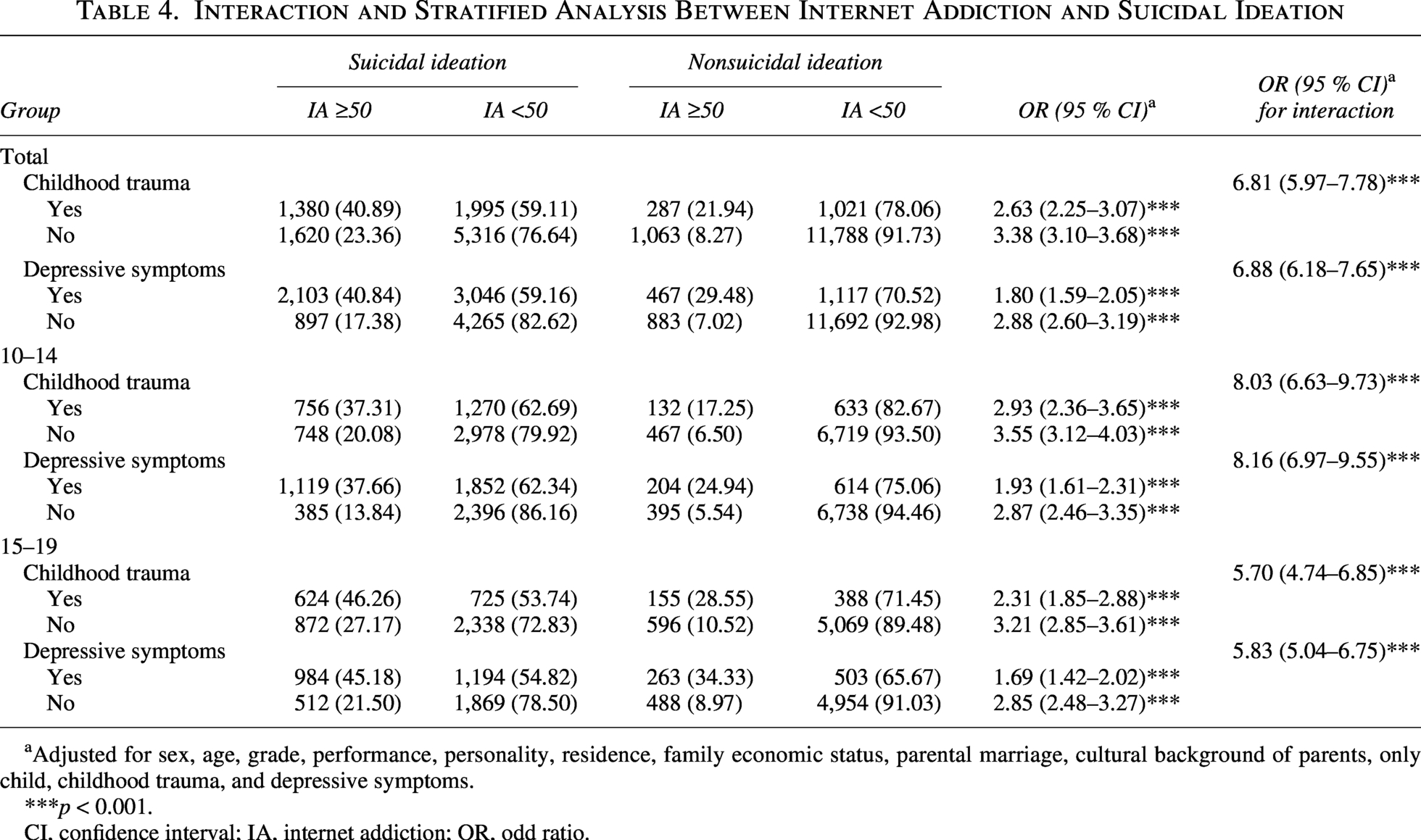
Adjusted for sex, age, grade, performance, personality, residence, family economic status, parental marriage, cultural background of parents, only child, childhood trauma, and depressive symptoms.
***p < 0.001.
CI, confidence interval; IA, internet addiction; OR, odd ratio.
It should be noted that the severe addiction group had a small sample size (n = 162), resulting in lower statistical power (75.5 percent). This reduced power may affect the stability of the estimates for this group, and caution is recommended when interpreting the results for severe addiction.
Discussion
This large-scale multicenter study examined the relationship between IA and SI in Chinese adolescents, focusing on sex differences and the moderating roles of childhood trauma and depressive symptoms. IA was significantly associated with SI, particularly among females. Childhood trauma and depressive symptoms were found to moderate the IA–SI relationship, with a stronger association observed during early adolescence. These findings enhance our understanding of how these moderating effects vary across developmental stages and sexes in the context of adolescent suicide risk in China.
IA was independently associated with SI and showed a dose–response relationship, consistent with a recent study. 32 Adolescents with IA typically exhibit poorer self-control and heightened impulsivity, 33 traits that significantly increase the risk of IA. 34 Online communication may promote reduced self-awareness and behavioral inhibition through anonymous interaction. 35 Consequently, repeated exposure to suicide-related content may desensitize adolescents to its negative consequences. 36 In addition, IA may also increase the SI risk by reducing social interactions, leading to loneliness, which is a significant risk factor for SI. 37
This study found a stronger association between IA and SI among females. Previous research suggests that females and males may differ in their patterns of Internet use: Females tend to engage more in social networking and online interaction, whereas males primarily use the Internet for entertainment, particularly online gaming. 38 These differences suggest that female adolescents may be more likely to use online activities to cope with emotional distress or interpersonal difficulties, thereby increasing their vulnerability to IA. 39 Furthermore, some studies suggest that females are more drawn to social or role-playing games, which involve higher emotional engagement and interpersonal interaction. 32 The increasing popularity of sex-neutral or female-oriented online games, such as Honor of Kings and Onmyoji, may therefore expose females to online gaming environments with strong social and emotional components. These environments may involve psychosocial processes such as social interaction, emotional investment, and comparison, 40 which could explain the stronger IA–SI association observed among females, although this remains hypothetical. As the present study did not collect data on specific gaming behaviors, preferences, or Internet use motives, further studies incorporating behavioral surveys are needed to clarify these mechanisms.
Childhood trauma moderated the IA–SI relationship, with a pattern consistent with a subadditive interaction. As shown in Figure 1, adolescents with childhood trauma showed a consistently higher prevalence of SI across all levels of IA severity, indicating an elevated baseline risk for SI in trauma-exposed adolescents. This finding aligns with previous research showing that childhood trauma is a significant risk factor for SI. 41 However, the increase in SI prevalence across IA severity levels was less steep in adolescents with childhood trauma than in those without, indicating that while trauma-exposed adolescents have a higher absolute risk of SI, the incremental effect of IA on SI is smaller in this group. This subadditive interaction may reflect the already elevated baseline risk of SI in trauma-exposed adolescents rather than suggesting that IA is unimportant. Mechanistically, adolescents with trauma exposure may be more likely to rely on online interactions for emotional support, potentially reflecting reduced trust in offline relationships. 42 In this context, excessive Internet use may serve as an avoidant coping strategy for trauma-related distress. Although such use may temporarily reduce negative affect, persistent avoidance may interfere with the development of adaptive coping strategies, reinforce social withdrawal and emotional dysregulation, and ultimately increase vulnerability to SI. 43
Similarly, depressive symptoms moderated the IA–SI relationship, showing a comparable subadditive pattern. Adolescents with depressive symptoms had a significantly higher prevalence of SI across all levels of IA severity, consistent with extensive evidence linking depression to SI. 44 As with childhood trauma, although adolescents with depressive symptoms had a higher baseline prevalence of SI, the increase in SI across IA severity levels was less pronounced in this group compared with those without depressive symptoms. This suggests that the elevated baseline risk associated with depression attenuates the apparent incremental effect of IA on SI. However, this does not imply that IA is negligible in adolescents with depressive symptoms. IA may still contribute to SI through maladaptive coping pathways, as adolescents with depressive symptoms may turn to the Internet to alleviate feelings of sadness, loneliness, or hopelessness. 45 While online engagement may provide temporary relief, excessive reliance on digital reinforcement may worsen emotional dysregulation over time, reduce offline support, and increase hopelessness, further lowering the threshold for SI. 46
The interaction results suggest that childhood trauma and depressive symptoms have a greater impact during early adolescence. This period is crucial for rapid brain development, especially in areas related to emotional regulation and social functions. 47 During this stage, adolescents’ cognitive abilities are still developing, and neural connections are highly sensitive to external influences. 48 Adolescents are also in the process of developing psychological adaptation and coping strategies. 49 As a result, they may lack the resources needed to effectively cope with trauma and negative emotions. Therefore, providing adequate emotional support and mental health resources is crucial to help adolescents build resilience and improve coping mechanisms.
These findings should also be understood within the sociocultural context of China. Chinese adolescents face significant academic pressure and high parental expectations, while family communication is often more reserved. Consequently, their emotional needs may not always be met effectively. In this context, Internet use serves not only as entertainment but also as an important means of emotional regulation, social support, and self-expression. For left-behind children or those with limited offline support, digital environments may play a compensatory role in helping them cope with emotional distress. The social and psychological functions of Internet use among Chinese adolescents may therefore differ from those observed in other cultural settings. This perspective helps explain the observed IA–SI association and underscores the importance of incorporating culturally sensitive prevention strategies.
Although this study provides valuable insights into the IA–SI relationship, it has limitations. First, the cross-sectional design prevents the establishment of causal relationships; therefore, future longitudinal studies are needed. Second, the reliance on self-report questionnaires introduces the potential for social desirability bias, which may affect the accuracy of responses. Third, the small sample size in the severe addiction group (n = 162) resulted in lower statistical power (75.5 percent), which may affect the stability of the estimates for this group. Future research should include larger samples to improve statistical power and ensure more reliable estimates. Finally, although Item 9 of the CDI was used to assess SI,30,31 it is a single-item measure that may not capture the full complexity of SI, including its frequency, severity, and duration. Future studies may benefit from using multi-item or interview-based assessments to provide a more comprehensive understanding of SI.
Conclusions
In conclusion, IA was significantly associated with SI among Chinese adolescents, particularly among females. Childhood trauma and depressive symptoms influenced this association, highlighting the complexity of suicide risk during adolescence. These findings suggest that IA may represent a potentially important behavioral correlate of SI. Integrating digital behavior assessment with psychological screening may support the early identification of at-risk adolescents and contribute to more comprehensive suicide prevention efforts.
Authors’ Contributions
F.Z. and X.X.: Conceptualization, methodology, data curation, formal analysis, investigation, writing—original draft, and writing—review and editing. Z.H.: Methodology, data curation, and investigation. T.F.: Data curation and investigation. J.L.: Investigation and writing—review and editing. Y.Y.: Methodology, investigation, and supervision. L.K.: Conceptualization, data curation, writing—review and editing, and supervision. All authors read and approved the final article.
Footnotes
Acknowledgment
The authors gratefully acknowledge the participating schools, students, and all individuals who contributed to data collection and coordination. The authors also thank all participants for their voluntary participation and the staff for their help with data collection in this study.
Ethics Approval Statement
All procedures were conducted in accordance with relevant laws and institutional guidelines, and approval was obtained from the Ethics Committee of Shandong University School of Nursing and Rehabilitation (2024-R-157).
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. The data are not publicly available due to privacy or ethical restrictions.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was supported by the Shandong Excellent Young Scientists Fund Program (Overseas) (Grant No. 2024HWYQ-010) and the Taishan Scholar Foundation of Shandong Province (Grant No. tsqn202211034).