
Abstract
Background:
Pediatricians support families in establishing healthy behaviors, yet there is limited information on valid and pragmatic questionnaires for assessing weight-related health behaviors in early childhood (≤24 months). The objective of this review is to summarize the evidence on parent-reported measures of weight-related health behaviors and/or parenting practices (e.g., feeding practices, dietary intake, sleep duration/routine, physical activity/sedentary behavior, and screen time) in early childhood.
Methods:
We conducted a scoping review by searching MEDLINE, Embase, PsycINFO, CINAHL, Web of Science, and Cochrane from inception to May 2025 (Open Science Framework Protocol https://doi.org/10.17605/OSF.IO/ME5KW). Articles included were peer reviewed, original research, published in English, and parent-reported measures of weight-related health behaviors in early childhood that reported psychometric results and/or were used in primary care. Trained reviewers systematically extracted details on the setting, questionnaire, and psychometrics. Findings were summarized using descriptive analysis.
Results:
Our search yielded 26,642 articles with a final data set of 223 articles. Of the 100 unique questionnaires identified, most (90%) assessed parents’ feeding practices and/or children’s dietary intake; few assessed sleep duration/routine (13%), screen time (13%), and/or physical activity/sedentary behavior (12%). Of the 52 articles describing questionnaires used in primary care, 35% reported psychometric analyses.
Conclusions:
Most questionnaires measuring weight-related health behaviors in early childhood assessed parent feeding practices and/or children’s dietary intake. Few questionnaires used in primary care reported psychometric results. Comprehensive, valid, reliable, and pragmatic questionnaires of health behaviors in early childhood are needed in the primary care settings to standardize screening for obesity risk in early childhood.
Introduction
Based on estimates from the 2021–2023 US National Health and Nutrition Examination Survey, 8.1% of children younger than 24 months had high weight-for-length (≥97.7th percentile on the World Health Organization [WHO] growth charts) and 14.9% of 2- to 5-year olds had obesity (≥95th percentile on the
The multifactorial etiology of childhood obesity as a result from a combination of genetic predisposition and environmental exposures, including social inequities, is well established. 16 Improving modifiable risk factors within a family’s locus of control, such as parenting practices and health behaviors, may help to mitigate risk and prevent the development of childhood obesity.17–20 Primary care clinicians (PCCs) have a unique opportunity and responsibility to support families in establishing healthy behaviors and parenting practices as they are being formed within the complex socioecological contexts. The American Academy of Pediatrics (AAP) Bright Futures “Periodicity Schedule” recommends 11 well-child care visits between the ages of 0 and 24 months. 21 Core elements of these well-child care visits include screening and anticipatory guidance to address growth trajectories, well-being, development, parenting practices, mental and behavioral health, and social drivers of health. During a well-child visit, PCCs are expected to deliver a large amount of health advice in a limited amount of time (the average patient–pediatrician interaction in the United States is approximately 15–18 minutes per preventive appointment).22,23
Valid and pragmatic screening questionnaires are widely available and in prevalent use in primary care to assess early childhood development and social drivers of health.24,25 Yet, information is limited on valid and pragmatic questionnaires for assessing weight-related health behaviors and/or parenting practices (e.g., feeding practices, dietary intake, sleep duration/routine, physical activity/sedentary behavior, and screen time) in early childhood (0 to ≤24 months). Filling this gap is essential because screening for weight-related health behaviors in early childhood may help to identify young children who are at risk for developing obesity and provide an opportunity for PCCs to counsel and connect families to interventions. Early childhood is a time of rapid development for children and parents’ behaviors need to adapt in response. 26 Interventions that support individual-level behavior change of both the parent and the child may have an influence on modifiable weight-related health behaviors.26–28
This scoping review was designed to guide decision makers seeking questionnaires for use in pediatric primary care to evaluate health behaviors and parenting practices related to obesity risk in early childhood. The purpose of this scoping review was to comprehensively explore the body of evidence on questionnaires that measure weight-related health behaviors and/or parenting practices in early childhood (0 to ≤24 months), summarize the evidence, identify gaps in knowledge, and inform future research.29–31 Considering that implementation of questionnaires in primary care settings requires balancing feasibility, acceptability, and validity, our objectives for this review were to identify parent-reported questionnaires to assess weight-related health behaviors and/or parenting practices in early childhood that (a) reported psychometric results; and/or (b) primary care settings utilized for routine screening. Identifying questionnaires with psychometrics results utilized in any setting can provide resources for decision makers about valid/reliable screening questionnaires, while identifying questionnaires utilized in primary care may identify pragmatic tools successfully implemented in primary care settings.
Methods
This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols Extension for Scoping Reviews (PRISMA-ScR) and the guidance suggested by the Joanna Briggs Institute and the Arksey and O’Malley framework for conducting scoping reviews.29–31 The PRISMA-ScR checklist and explanation were used throughout the process. Our scoping review protocol was registered in Open Science Framework, https://doi.org/10.17605/OSF.IO/ME5KW, a free, open platform to support research and enable collaboration throughout a life cycle. 32 Search results were pooled in EndNote™ 20 (Clarivate, Philadelphia, USA, and London, UK), a citation manager software, and deduplicated. This set was uploaded into Covidence (Veritas Health Innovation, Melbourne, Australia), a software program that facilitates the management of articles and the screening of references by multiple reviewers.
Selection of Weight-Related Health Behaviors and/or Parenting Practices
We first defined the set of weight-related health behaviors and/or parenting practices by building upon work led by members of our study team at the AAP Institute for Healthy Childhood Weight to describe risk factors for obesity in early life. AAP policy and clinical reports identify that (a) parent feeding practices; (b) dietary/nutrition intake; (c) sleep duration/routine; (d) physical activity/sedentary behavior; and (e) screen time as weight-related health behaviors associated with the development of pediatric obesity were published and served as the foundation for this work.33–36 Our study team consisting of national experts in childhood obesity reviewed the list of behaviors for completeness and achieved consensus before commencing with the scoping review.
Eligibility Criteria
This scoping review included articles reporting on questionnaires utilized to assess parent-reported weight-related health behaviors and/or parenting practices in early childhood that reported psychometric results and/or were utilized in primary care. The questionnaires included an assessment of the following: (a) parent-reported feeding practices, and/or (b) parent report of the child’s dietary intake, and/or (c) sleep duration/routine, and/or (d) physical activity/sedentary behavior, and/or (e) screen time (Supplementary Table S1). The respondent who completed the questionnaire was either a parent, primary caregiver, or guardian responsible for taking care of a child age 0 to ≤24 months who herein is referred to as parent.
This review included any peer-reviewed research published in English, included human subjects, and utilized questionnaires of weight-related health behaviors and/or parenting practices in early childhood (0 to ≤24 months). There were no restrictions to country or population, participants’ demographic variables, recruitment or sampling strategies, date of publication, or research setting (e.g., hospitals, workplaces, community-based organizations).
Articles were excluded if they did not include children age 0 to ≤24 months, were conference abstracts, systematic and narrative reviews of the literature, and/or were: (a) a diagnostic test or observation (e.g., not parent-reported), (b) only included data collected by a diary/log, (c) assessed objective nutritional status or weight status, or (d) assessed behavioral problems and/or disordered sleeping.
Information Sources
To identify relevant literature, the following databases were searched on July 22, 2022, and updated on May 14, 2025: MEDLINE (Ovid), Embase (Ovid), PsycINFO (Ovid), CINAHL Complete, Web of Science Core Collection, and both the Cochrane Database of Systematic Reviews and CENTRAL (Clinical Trials Database) in Cochrane Library.
Search
An experienced medical librarian (M.C.F.) engaged in the development of our methodology ran a medical subject heading (MeSH) analysis of known key articles provided by the research team (mesh.med.yale.edu) and completed scoping searches of each database. An iterative process was used to translate and refine the searches. To maximize sensitivity, the formal search used controlled vocabulary terms and synonymous free-text words. The search strategy (Supplementary Table S2) was peer reviewed by a second librarian, not otherwise associated with the project, using the PRESS standard. 37 The citation chaser software program was utilized to check for additional relevant cited and citing articles using the included studies. 38
Selection of Sources of Evidence
Title and abstract screening
Before independent screening, we ensured interrater reliability (IRR) using Cohen’s kappa statistic.39,40 A random sample of titles and abstracts were screened by all reviewers (M.S., J.L., M.T., A.E.S., K.S., S.V.L., C.F.A., K.A.B., and C.C.C.) for inclusion or exclusion. 30 Discrepancies between reviewers were resolved through discussion, screening expectations were adjusted accordingly, and IRR was reassessed. 30 This process was repeated in which a total of 60 randomly selected titles and abstracts were screened, and an IRR of ≥0.80 was established for all reviewers. 30 Once an agreement on the screening process was met (IRR ≥0.80), each title and abstract were independently screened by two reviewers. Discrepancies between the two reviewers were discussed and resolved. Articles that fulfilled the inclusion criteria were moved to full-text review. The reviewers communicated on an approximately weekly basis to discuss the title and abstract screening process and address any questions.
Full-text review
To ensure quality and consistency during the full-text review process, a random sample of 10 articles had a full-text review completed by all reviewers (M.S., C.T.W., C.F.A., C.C.C., and S.V.L.) for inclusion or exclusion. 30 Discrepancies between reviewers were resolved through discussion, full-text review expectations were adjusted accordingly, and IRR was assessed. 30 This process was repeated in which a total of 30 randomly selected articles had a full-text review completed by all reviewers and an IRR of ≥0.80 was established. 30 Once an agreement on the full-text review process was met (IRR ≥0.80), two reviewers independently completed full-text reviews of the articles, and any discrepancies were discussed and resolved. Articles that fulfilled the inclusion criteria were moved to data charting. The reviewers communicated weekly to address any questions that arose during the full-text review process.
Data charting process
For the articles that were included in this review, data were collected using Qualtrics™ software version 2020 (Provo, UT), an online survey/data collection tool. The data form was created and tested by the research team before data collection. To ensure consistency during the data charting process, the first 16 articles had data charting completed independently by two reviewers (C.F.A. and E.I.T.). The reviewers discussed differences, and data charting expectations were adjusted accordingly. Once consensus was met after the 16 articles, the reviewers began data charting independently, and each article had one reviewer complete the data charting process. The reviewers communicated weekly to address questions about articles and/or the data charting process. Upon data charting completion, a third reviewer (J.C. and C.T.W.) confirmed the accuracy of the data tables.
Data items
Our data charting process was organized into four domains as follows: (a) article information, (b) study information, (c) questionnaire information, and (d) additional notes (Supplementary Table S3).
Synthesis of results
Descriptive analysis was used to summarize the findings, and all quantitative analyses were conducted using Microsoft Office 365, Microsoft Excel (Microsoft Corporation, Redmond, WA) spreadsheet software.
Results
Selection of Sources of Evidence
Figure 1 presents the PRISMA flow diagram for the selection of sources. The search yielded 26,642 articles, of which 15,293 were identified as duplicates, 10,467 were excluded during title and abstract screening, and 659 were excluded during full-text review, resulting in 223 articles. A total of 106 unique questionnaires were identified from the articles. We excluded six questionnaires that were described as valid by authors, but for which we were unable to locate reported psychometric results (Supplementary Table S4), resulting in 100 questionnaires that were included in this review (Table 1).
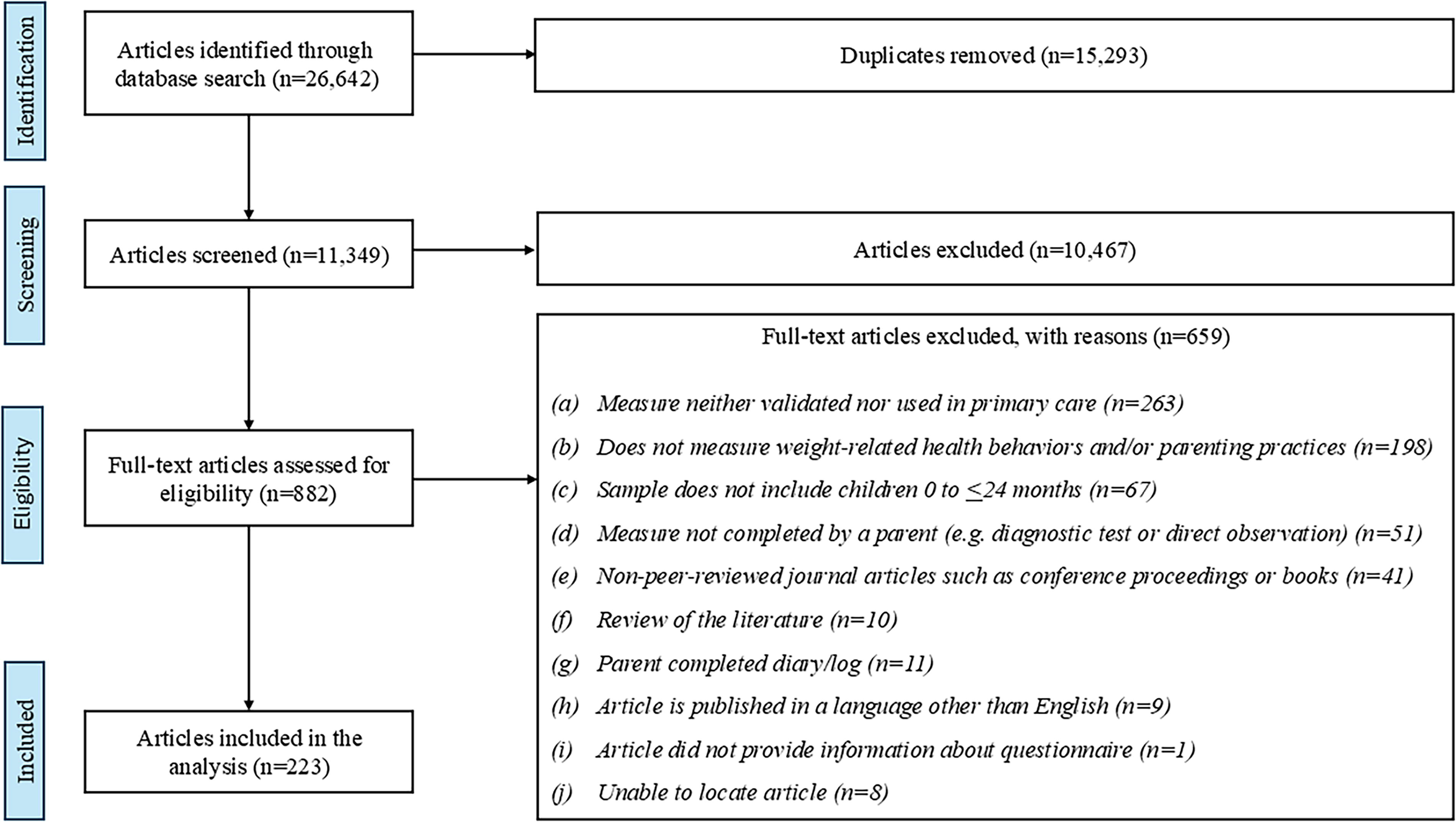
PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
Characteristics of Questionnaire Identified (n = 100) from 216 Articles That Met the Inclusion Criteria

The authors state the questionnaire was validated by the Swedish Pediatric Association and unable to identify type of validation because citation is not available in English.
The authors state the questionnaire is valid but unable to verify the citation, which is a master’s degree thesis. The questionnaire has been used in the Chinese Nutrition and Health Surveillance of children aged 0–2 years in 2013.
The authors state the questionnaire is valid but did not provide a citation or psychometric results.
The authors state the questionnaire is valid and that the citation provided is a short report presenting preliminary testing and test–retest results and indicate that a validation study is needed to establish construct and content validity.
The authors state the questionnaire was validated through the use of pretested questionnaires and experts’ opinions.
The authors indicated that the fourth component of the questionnaire used a validated questionnaire (Bengali Version of Household Food Security scale-short form) and that the questionnaire had fixed-choice answer options.
Count does not include questions about “parenting practices” and “parenting style.”
The authors state that the questionnaire was previously validated but did not provide a citation or psychometric results.
Participants were recruited from inpatient and outpatient wards at the KK Women’s and Children’s Hospital, Singapore. In email communication, the authors confirmed that the outpatient services included pediatric primary care.
A, acute care setting/specialty clinic; C, community setting; H, home/residential setting; P, primary care setting; R, research setting; W, women, infants, children program.
Characteristics of Questionnaires
The questionnaires were utilized in 36 different countries/territories, of which the United States (n = 29, 29%) and Australia (n = 9, 9%) were the most common. In some questionnaires (n = 28, 28%), the authors reported specific characteristics of the study population such as socioeconomic status (n = 10, 10%),66,71,72,91,97,125,158,219,224,232 attendance at a Women, Infant, Children program (n = 9, 9%),43,66,71,100,125,135,140,153,243 and/or a specific race and/or ethnicity for the study population (n = 15, 15%).44,71,100,112,121,135,137,138,153,162,166,168,224,228,237
For the 100 unique questionnaires identified, 66 (66%) questionnaires had psychometric results reported, of which 18 (27%) were used in the primary care setting (Fig. 2). Table 2 presents the reported psychometric results for the 66 questionnaires. The most frequently reported psychometric results included (a) Cronbach’s alpha (n = 31, 47%), (b) Pearson correlation (n = 20, 30%), and (c) Spearman’s correlation (n = 18, 27%). For the questionnaires that reported Cronbach’s alpha, 27 (87%) questionnaires had an alpha value fall within the recommended threshold of 0.70–0.90. For the questionnaires that reported Pearson correlations, eight (40%) had an “r” value within the “strong correlation” threshold of 0.70–1.0. 249 For the questionnaires that reported Spearman correlation, eight (44%) had a “p” or “r” value within the recommended threshold of 0.70–1.0. 249

Venn diagram of scoping review objectives.
Psychometric Analyses Reported for the Questionnaire Identified (n = 100) from 223 Articles that Met the Inclusion Criteria

See the Supplement Table for detailed information about the reported psychometric results.
Most questionnaires assessed parent feeding practices and/or child dietary/nutrition intake (n = 90, 90%), while few assessed children’s sleep duration/routine (n = 13, 13%), screen time (n = 13, 13%), and/or physical activity/sedentary behavior (n = 12, 12%). Almost half of the questionnaires (n = 43, 43%) had fixed-choice answer options, some questionnaires (n = 15, 15%) had both fixed-choice and open-ended responses, and five (5%) questionnaires had open-ended responses, while 37 (37%) questionnaires did not specify the response option.
The method and mode of administration included the following: 41 self-administered questionnaires, completed by parents on paper (n = 8, 20%), computers (n = 16, 39%), or unspecified (n = 21, 51%), and 46 questionnaires administered via interview, completed via the phone (n = 10, 22%), in-person (n = 26, 57%), or unspecified (n = 16, 35%). The personnel who conducted the interview-administered questionnaires included trained research staff (n = 23, 50%), health professionals (e.g., clinicians or allied health professionals) (n = 12, 26%), and 11 (24%) did not report who administered the questionnaire. Three (3%) questionnaires reported both self-administration and interview options based on participant preference, while 16 (16%) questionnaires did not provide the mode of administration.
Synthesis of Results
Questionnaires utilized in primary care
We identified 52 (52%) questionnaires that were used in primary care. Of the questionnaires utilized in primary care, 18 (35%) reported psychometric results. Most questionnaires used in primary care (n = 49, 94%) assessed parent feeding practices and/or dietary/nutrition intake, while few assessed screen time (n = 8, 15%), physical activity/sedentary behavior (n = 7, 14%), or sleep duration/routine (n = 7, 14%). For the questionnaires that reported the number of items (n = 25, 48%), the range of items was 2–150 (median: 27, interquartile range: 25). Parents completed the questionnaires via interview (n = 26, 50%), self-administration (n = 17, 33%), were given the option to complete the questionnaire via interview or self-administration (n = 1, 2%), and eight (15%) questionnaires did not specify the method of administration. The most frequently cited questionnaire utilized in primary care was the Infant Feeding Questionnaire, 66 which reported an exploratory factor analysis with a seven-factor solution and Cronbach’s alpha results ranging from 0.24 to 0.74 for the factors. This self-administered 20-item questionnaire assessed parent feeding practices and was completed by mothers with children aged 11–24 months. The Feeding, Lifestyle, Activity Goals (FLAGs) 247 questionnaire (19 items) assessed all five health behaviors and reported psychometric results (Cronbach’s alpha: 0.71; intraclass correlation: 0.861; p-value: <0.001; and principal component analysis with a two-component solution: (a) structure and variety at mealtime and (b) enjoyment and self-regulation of eating that accounted for 55.9% of the total variance). The questionnaire had fixed-choice and open-ended answer options and was completed by parents with a child between the ages of 0 and <24 months in both the inpatient and outpatient settings of the KK Women’s and Children’s Hospital, Singapore.
Questionnaires with reported psychometrics in nonprimary care settings or unspecified settings
Among the 48 (48%) questionnaires with reported psychometrics in nonprimary care or unspecified settings, most assessed parent feeding practices and/or dietary/nutrition intake (n = 41, 85%). Few questionnaires assessed sleep duration routine (n = 6, 13%), screen time (n = 5, 10%), or physical activity/sedentary behavior (n = 5, 10%). For the questionnaires (n = 44, 92%) that reported a number of items, the range of items was 7–211 (median: 34, interquartile range: 35). The most frequently cited questionnaire with psychometric results was the Brief Infant Sleep Questionnaire, 167 which reported the Pearson correlation of all sleep measures 0.82–0.95, p-value <0.001. This self-administered, 15-item questionnaire assessed sleep duration/routine and was completed by parents of children aged 0–36 months.
Discussion
In this scoping review, we identified 223 publications describing 100 unique questionnaires assessing weight-related health behaviors or parenting practices. Most questionnaires assessed parent feeding practices and/or children’s dietary/nutritional intake, while few assessed children’s sleep duration/routine, physical activity/sedentary behavior, or screen time. Our findings demonstrate substantial heterogeneity in the statistical methods utilized to assess the psychometric properties of the questionnaires. Most questionnaires utilized in primary care lacked reporting of psychometric results to assess reliability and/or validity.
Our findings build upon prior reviews demonstrating a need for the development of a pragmatic questionnaire that assesses multiple weight-related health behaviors, which can be utilized in pediatric primary care.250–252 Each of the prior reviews identified less than 10 questionnaires that included children ≤24 months, and none of which included all health behaviors of interest (parent feeding practice, dietary/nutrition intake, sleep duration/routine, physical activity/sedentary behavior, and screen time). The knowledge gap regarding questionnaires that assess health behaviors and parenting practices related to obesity risk in early childhood is essential to address because health behaviors that develop in early childhood may have a lifetime impact on a child’s health and well-being.
PCCs have limited time during well-child visits to screen and counsel, and the inclusion of multiple health behaviors in a screening tool could allow PCCs to efficiently tailor counseling topics to address families in a meaningful way. Among the questionnaires that reported psychometric results, we identified one questionnaire—the FLAGs 247 questionnaire—designed for the clinical setting, used in pediatric primary care, and assessed all five health behaviors of interest.
Few questionnaires provided detailed information regarding the feasibility, appropriateness of administration, and implementation of the questionnaires. Information about the frequency of administering the questionnaire, the location or method of administration, the integration of the questionnaire into the electronic health record (if applicable), and suggested resources to support the administration and implementation is needed to understand barriers and opportunities to adopt screening broadly.250,253 Few provided details about the populations/communities in which the questionnaire was administered beyond the geographic location. Information about participants’ language, sociodemographic characteristics, and health status can provide more context and support the reliability and validity of the questionnaire for specific populations/communities. 252 Information on the feasibility, appropriateness, and acceptability across diverse populations can guide efforts to build local capacity to implement screening successfully and equitably. 254
To successfully screen for weight-related health behaviors in early childhood, a comprehensive parent-reported measure should balance validity and reliability with acceptability (e.g., the questionnaire is agreeable, palatable, or satisfactory) 255 among those using the questionnaire.
Suggested future research includes the following: (a) Development of a reliable and valid screening questionnaire for early childhood that assesses multiple weight-related health behaviors that is practical to use in primary care; (b) the impact of the questionnaire on the delivery of care and the health outcomes of a child 250 ; and (c) psychometric results for diverse populations/communities to ensure that the questionnaire is measuring the health behaviors of interest. For example, the 19-item FLAGs 247 questionnaire could be further evaluated in additional geographic locations to further support the validity and reliability of the instrument, or psychometric analyses could be completed on the two questionnaires (15-item Child’s Health-Related Behavior245 and the questionnaire by Alshahrani et al. 246 ) previously used successfully in primary care that included all the health behaviors of interest but lacked reporting of psychometric results. Alternatively, distinct questionnaires with psychometric evidence of reliability and validity could be combined to include all the health behaviors of interest. For example, the Healthy Kids Assessment Tool 243 could be combined with the Toddler Feeding Style Questionnaire 101 to create a questionnaire with 31 items. Such novel combinations of individual questionnaires would benefit from psychometric evaluation to confirm the reliability and validity of the combined battery of questionnaires among parents of children aged ≤24 months, as well as the feasibility and acceptability of their use in primary care settings.
Strengths and Limitations
The strengths of this scoping review include an extensive search for all articles that measured weight-related health behaviors in early childhood. A total of 11,349 titles and abstracts were screened, and 882 full-text articles were assessed for inclusion. We followed the PRISMA-ScR and the guidance suggested by the Joanna Briggs Institute and the Arksey and O’Malley framework for conducting scoping reviews.29–31
There were also limitations to this scoping review. First, it is possible that not all relevant questionnaires were identified in the search process. Questionnaires published in the gray literature, publications in languages other than English, reviews of the literature, and conference abstracts were not included in this review. In addition, the scope of our review focused on identifying pragmatic, valid instruments for use in primary care settings, so we lack information about potentially feasible questionnaires used outside of primary care settings that did not report psychometric results. Second, some authors of the included articles described the topics assessed in the questionnaire but did not provide details about the items included in the questionnaire, which could have resulted in misclassification. The scoping review did not involve an appraisal of the quality of studies as this is not a mandatory step in scoping reviews29–31 ; instead, we provided a summary of the questionnaires and psychometric analyses so that PCCs and researchers can use the information to determine if a questionnaire is suitable to use in the context of their study and/or the patient population being served.
Conclusion
Most questionnaires measured parent feeding practices and/or dietary/nutrition intake, while a few assessed sleep duration/routine, physical activity/sedentary behavior, or screen time. Most questionnaires utilized in the primary care setting reported limited information about the questionnaire, and few reported psychometric results. The development and validation of a brief, pragmatic questionnaire to assess weight-related health behaviors and parenting practices may facilitate screening and delivery of tailored pediatric primary care to mitigate obesity risk in early childhood.
Impact Statement
This scoping review summarizes the literature on questionnaires assessing weight-related behaviors/parenting practices in early childhood to inform the selection of measures for use in primary care. Most questionnaires measured feeding/diet. Few utilized in primary care reported psychometrics. Our findings highlight the need for validation of comprehensive, feasible questionnaires for primary care.
Authors’ Contributions
C.F.A. designed the study approach and data collection instruments, collected data, completed the analysis, drafted the initial article, and critically reviewed and revised the article. M.C.F. was the lead librarian in executing the review, assisted with the study approach, and critically reviewed and revised the article. E.I.T., S.V.L., K.A.B., and C.C.C. critically reviewed and revised the data collection instrument, collected data, and critically reviewed and revised the article. J.L., C.T.W., A.E.S., G.B., and R.S.G. critically reviewed and revised the study design, the data collection instrument, and the article. M.S. conceptualized, designed, and supervised the study, critically reviewed and revised the data collection instrument, and critically reviewed and revised the article.
Footnotes
Acknowledgments
The authors thank Mala Thapar, MPH, for assisting with conceptualizing the study. They thank Victoria Helwig and Vermetha Polite of the Cushing/Whitney Medical Library for technical support. The authors also thank John I. Cho, MPH, and Shreya Pathak for assistance with reviewing the data tables and Christina Tong, MPH, for assisting with the title/abstract screening, full-text review, and reviewing the data tables for the updated literature search.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
This project was developed in partnership with the AAP Institute for Healthy Childhood Weight and was made possible through a grant from the CDC, Grant # 6 NU38OT000282-05-04. C.C.C. was supported by the Fogarty Global Health Equity Scholars Fellowship (FIC D43 TW010540) and by the Yale Center for Clinical Investigation (NCATS TL1 TR001864), and is currently supported by the NIH Pathway to Independence Award (K99 HL166781-01A1). A.E.S. is supported, in part, by the Office of the Director, the NIH under Award Number UG1OD024959. G.B. is supported, in part, by the NICHD Pathway to Independence Award (R00HD097301) and the NICHD Transformative Health Equity Research (U01HD115256). The content is solely the responsibility of the authors and does not necessarily represent the official views of the CDC or the NIH.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.