
Abstract
Purpose:
Cost is a critical consideration when implementing evidence-based family healthy weight programs (FHWPs). However, real-world implementation cost data are often underreported, and standardized methods for accurate cost collection are lacking. This article synthesizes the implementation costing approaches used across five FHWPs to inform future adopters and implementers by illustrating context-appropriate costing methods and identifying practical considerations for cost data collection and reporting.
Methods:
We descriptively report and compare the implementation strategies and associated cost assessment methods across five projects funded by the Centers for Disease Control and Prevention’s Childhood Obesity Research Demonstration (CORD 3.0) program. CORD 3.0 aimed to package FHWPs for implementation in health care, community, or public health settings. Costing approach information was organized and abstracted using a published checklist.
Findings:
Despite variation in program models and settings, several common costing approaches emerged. All projects used direct measurement methods (e.g., activity-based or micro-costing) and categorized costs consistently (e.g., labor, supplies, space, information technology) to support decision-making and improve comparability. Several projects applied structured frameworks to guide costing efforts and distinguished between fixed, one-time costs (e.g., training development) and variable, recurring costs (e.g., session delivery, supervision). These patterns highlight a balance of methodological consistency and adaptability across diverse contexts.
Conclusions:
This study provides an overview of approaches to assessing FHWP implementation costs within the CDC’s CORD 3.0 initiative. Applying structured frameworks and practical tools, these projects demonstrate how cost assessments can guide strategic planning, reimbursement, and sustainability—laying groundwork for improved cost reporting and integration in future FHWP dissemination and implementation.
Keywords
Introduction
Childhood obesity continues to be a pressing public health concern, affecting approximately one in five U.S. children and adolescents aged 2–19. 1 Obesity contributes to increased risk of chronic diseases such as type 2 diabetes and cardiovascular disease in childhood and later in life. 2 Prevalence of obesity is disproportionately distributed across the U.S. population, with higher prevalence among children in lower-income families 3 and minoritized communities. 4 In response, the 2023 American Academy of Pediatrics (AAP) Clinical Practice Guideline (CPG) for the Evaluation and Treatment of Children and Adolescents with Obesity recommended that children and adolescents living with overweight or obesity should be offered evidence-based treatments. 5 The foundational treatment, referred to as intensive health behavior lifestyle treatments (IHBLTs) by the AAP and as Family Healthy Weight Programs (FHWPs) by the CDC, 6 includes 26 contact hours of a nonstigmatizing, family-based, multicomponent, and structured multidisciplinary intervention that focuses on physical activity, healthful eating, and lifestyle behavior change strategies delivered over 3–12 months.
FHWPs have demonstrated efficacy and effectiveness. A recent review from the US Preventive Services Task Force (USPSTF) included 42 trials testing FHWP (n = 6956 children and adolescents) and concluded that lifestyle-based weight loss interventions with ≥26 hours of intervention contact were likely to reduce excess weight (with absolute BMI z-score reduction of ≥0.2) in children and adolescents. 7 Consequently, the USPSTF assigned a Grade B recommendation for screening children aged six and older for obesity and referring them to intensive behavioral treatments.8,9 Several evidence-based FHWPs that meet the criteria and align with the USPSTF recommendations have been recognized by the CDC and the AAP. 10
Despite the available evidence on FHWP effectiveness and the USPSTF recommendation, the adoption of FHWPs has not been widespread. Only 52% of children’s hospitals in the U.S. reported offering comprehensive multidisciplinary pediatric weight management programs. 11 Challenges to broad dissemination, implementation, and sustainment include limited primary care provider (PCP) time and lack of clarity regarding their roles; inconsistent or insufficient geographic coverage and provider networks 12 resulting in limited access;13,14 inconsistent reimbursement models for evidence-based childhood obesity treatment services (only certain health professionals can bill for the services); and limited community capacity for implementation. 14 These barriers result in racial and ethnic minoritized populations and communities with lower socioeconomic status having less access and/or having lower engagement with clinic-based programs.15,16 This also highlights the disconnect between strong evidence of effectiveness and the realities of implementation—raising the question not only of clinical value, but also of whether existing cost structures and financial models support widespread delivery of FHWPs.
Several studies support the economic value of FHWPs.17–21 For example, the CHOICES study found that upstream interventions such as beverage taxes or active physical activity policies may offer greater population reach and cost savings than clinical treatments.17,18 However, the study, like many others, did not report detailed cost information on implementation.19–21 Implementation costs, defined as the resources required to deliver an FHWP, are not typically captured in the conventional economic evaluation, 22 which often accounts only for intervention costs, especially when applying decision analytic modeling to assess long-term health and economic consequences beyond the period of a research study. As such, a critical gap remains—few studies have examined the actual costs required to implement these programs in diverse real-world settings. As a result, decision-makers lack the cost data needed to plan, fund, and sustain effective delivery at scale. 23 Furthermore, cost is one of the least-reported implementation outcomes.24–27 Without a realistic understanding of implementation costs, the adoption, implementation, and maintenance of FHWPs and other evidence-based interventions by clinical or community delivery agencies is significantly hindered. 28
Possible reasons for the underreporting of implementation costs include the lack of standardized terminology, generalized methodology, and guidance. Implementation costs may include costs related to (1) recruitment and enrollment of eligible participants; (2) recruitment, training, and startup costs for staff; (3) participant- and delivery agent-facing intervention materials; (4) program delivery costs; and (5) potential downstream costs 29 (e.g., changes in health care utilization or productivity as a result of implementation). In addition, implementation costs often include resources required to integrate and sustain evidence-based programs in real-world settings.29,30 These may include modifying electronic health record systems or covering ongoing staff expenses over time. Understanding both implementation and program (or treatment) costs is critical for providing decision-relevant information for stakeholders considering resource allocation and reimbursement and payment models for broad scale-up. The field of implementation science calls for an increasing application of cost analyses or economic evaluation of implementation strategies. 31 Numerous efforts have aimed to increase the application of economic evaluation of dissemination and implementation strategies, 32 highlighting approaches and examples to advance the field, yet none are specific to the deployment of FHWPs.
To address these challenges, the CDC’s Childhood Obesity Research Demonstration (CORD) 3.0 was developed to test strategies and methods that can improve access to evidence-based FHWPs for low-income populations that are experiencing disparities in childhood obesity and to consider the potential cost implications. 33 This article provides an overview of the implementation cost assessment approaches used across the five CDC-funded CORD 3.0 FHWP projects. Across projects, we consider the costs of FHWP implementation, the strategies used to achieve dissemination and implementation outcomes (e.g., reach, adoption, implementation, and sustainability), and program delivery. Our aim is to inform others seeking to adopt, implement, or sustain FHWPs by illustrating context-appropriate costing methods and identifying practical considerations for cost data collection and reporting.
CDC Childhood Obesity Research Demonstration (CORD) 3.0
To translate FHWPs into routine practice with packaged intervention materials and messages intended for children from low-income families, the CDC’s CORD 3.0 initiative supported awardees that represented multi-institutional teams led by University of Nebraska System, 34 the Massachusetts General Hospital, 35 Miriam Hospital, 36 Stanford University, 37 and Washington University in St. Louis. 38 Table 1 provides an overview of the five FHWPs included in CORD 3.0. Information on geographic region and settings as well as program characteristics in terms of delivery structure and intended participant-level outcomes is provided to demonstrate consistencies and differences across FHWPs. FHWP delivery settings were characterized as clinical, community, and/or virtual. Table 2 provides an overview of the dissemination and implementation strategies used across FHWPs by stages of implementation, using the EPIS framework—exploration, preparation, implementation, and sustainment. 39 Additional details on the five FHWPs can be found in a special issue of Childhood Obesity.34–38
Overview of the Family Healthy Weight Programs Funded Through the CDC Obesity Research Demonstration 3.0
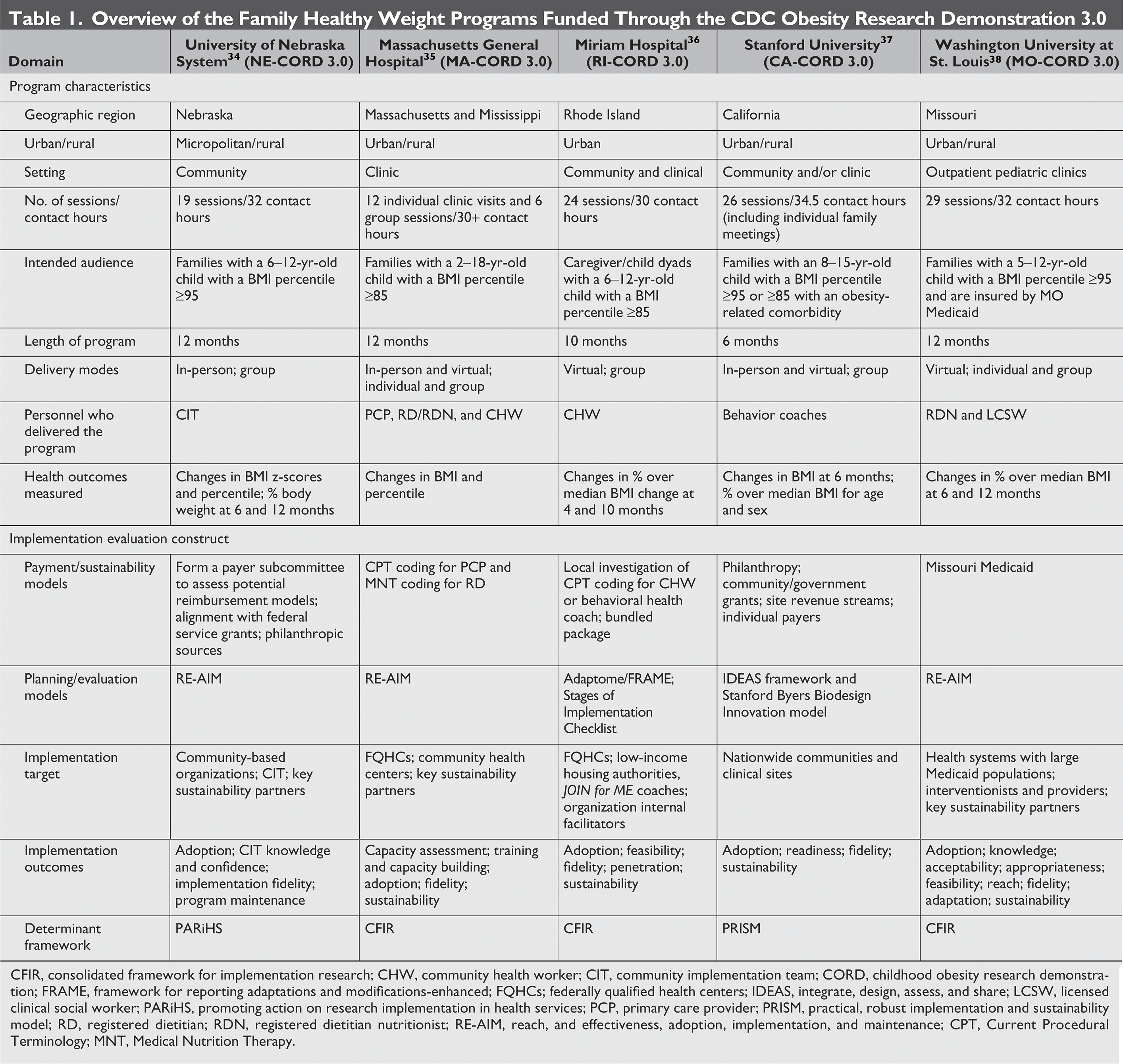
CFIR, consolidated framework for implementation research; CHW, community health worker; CIT, community implementation team; CORD, childhood obesity research demonstration; FRAME, framework for reporting adaptations and modifications-enhanced; FQHCs; federally qualified health centers; IDEAS, integrate, design, assess, and share; LCSW, licensed clinical social worker; PARiHS, promoting action on research implementation in health services; PCP, primary care provider; PRISM, practical, robust implementation and sustainability model; RD, registered dietitian; RDN, registered dietitian nutritionist; RE-AIM, reach, and effectiveness, adoption, implementation, and maintenance; CPT, Current Procedural Terminology; MNT, Medical Nutrition Therapy.
Dissemination and Implementation Strategies Applied Across Family Healthy Weight Programs, by the EPIS Framework 39
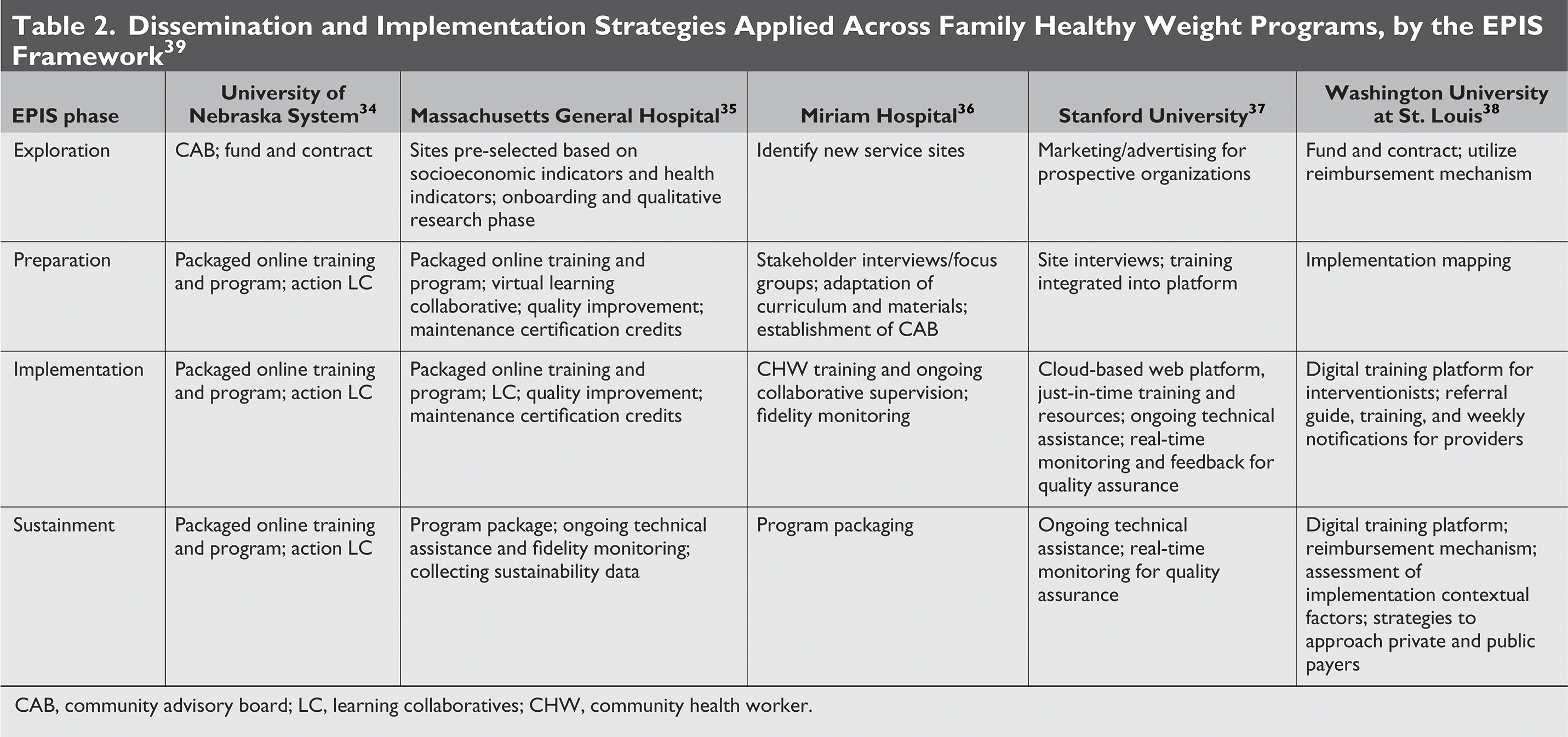
CAB, community advisory board; LC, learning collaboratives; CHW, community health worker.
In a recent review of costs of implementation strategies, Michaud and colleagues 27 developed a checklist to guide the conduct and reporting of cost assessment of implementation strategies. This checklist can inform the application of cost assessment of implementation among the CORD 3.0 projects and other FHWPs that focus on the adoption, implementation, and maintenance. Applying the checklist (see Supplementary Table S1), in Table 3, we provide an overview of cost assessment of FHWP implementation, including framework, measurement, tools, and instruments applied to determine the cost, the cost-benefit relationship, and how data are intended to be used for support payment or reimbursement models across each of the five FHWPs.
Comparison of Approaches to Assess Implementation Costs Associated with Family Healthy Weight Program Across Five Projects Funded Through CDC CORD 3.0
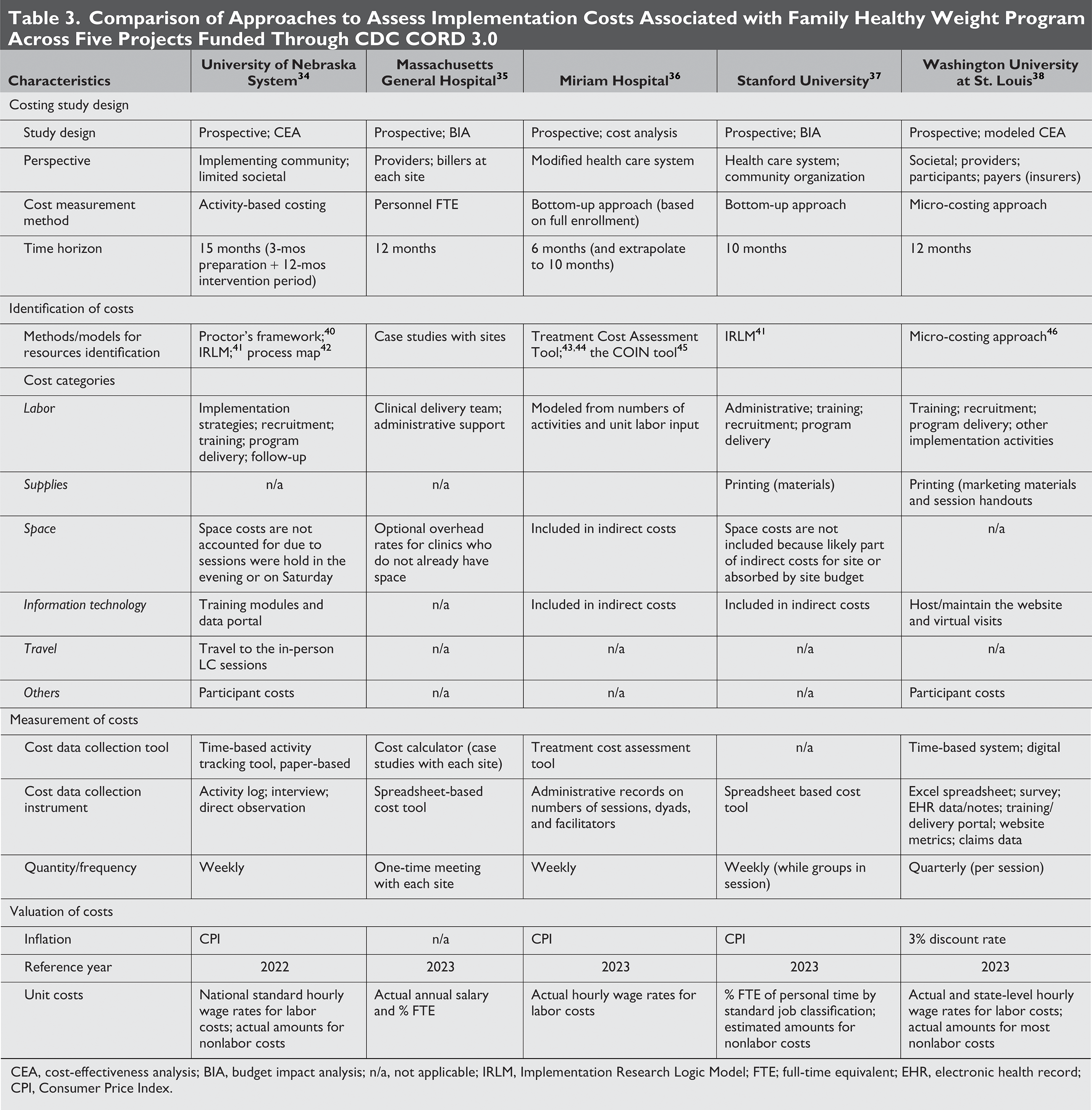
CEA, cost-effectiveness analysis; BIA, budget impact analysis; n/a, not applicable; IRLM, Implementation Research Logic Model; FTE; full-time equivalent; EHR, electronic health record; CPI, Consumer Price Index.
University of Nebraska System, NE-CORD 3.0
Family healthy weight program
The Building Healthy Families (BHF) is a 12-month parent–child dyad program, adapted from Epstein’s traffic light diet pediatric weight management interventions, and is designed for rural communities. 47 BHF focuses on nutrition education, behavioral modification, and physical activities to support families in the rural and micropolitan areas. The program includes 12 weeks of consecutive education lessons (2 hours each session), four relapse prevention refresher sessions (1 hour every 3 weeks), and one additional refresher session (2 hours) between 6 and 12 months. It also features two follow-up check-ins (1 hour each) at 6 and 12 months. To qualify, families must have a child aged 6–12 years with a BMI at or above the 95th percentile. BHF provides structured support to help families develop sustainable healthy habits, making the program an effective approach to combatting pediatric obesity in underserved areas.
Dissemination and implementation strategy
The NE-CORD 3.0 project included three dissemination and implementation strategies: (1) product packaging, (2) community readiness identification through a fund and contract approach, and (3) an action learning collaborative. The research team developed the online resources and training program, a user-centered resource, to help rural communities implement and sustain BHF. This online program includes training modules covering program delivery, participant recruitment, nutrition education, lifestyle management, and physical activity coordination, along with session-specific lesson plans and materials for families. Knowledge checks for community implementation facilitators ensure understanding of core concepts, while a Health Insurance Portability and Accountability Act (HIPAA)-compliant data portal tracks family metrics (e.g., BMI, physical activity, healthy eating goals) and implementation fidelity. The portal generates aggregated deidentified reports for stakeholders and supports quality improvement (QI) activities. The fund and contract process identified communities with readiness to deliver BHF. This strategy, guided by a community advisory board, issued a statewide call for proposals. Communities submitted a letter of intent and then a project narrative detailing the priority of childhood obesity in their community, resources to dedicate to addressing it, and partnerships for implementation. Finally, quarterly learning collaborative meetings facilitated peer sharing, goal-setting, and sustainability planning among community teams. Action periods between meetings focus on implementation goals with midpoint feedback to address barriers and track progress.
Cost assessment of implementation
The activity-based costing approach was applied to capture the labor costs associated with implementation activities. Proctor’s framework was used to specify the activities of implementation strategies. 40 The research team populated the prespecified implementation activities on an online time-tracking tool (i.e., Clockify), complemented by the meeting minutes or activity logs. They calculated the costs associated with each activity by multiplying the total time (in hours) spent on that activity by the unit cost (e.g., national average hourly wage) of the personnel conducting the activity. Nonlabor costs were tracked by administrative database, invoices, and receipts. The overall implementation costs were estimated by summing up the labor and nonlabor costs. All cost analyses were conducted using a Microsoft Excel spreadsheet.
The cost-effectiveness analysis was assessed by associated implementation costs and implementation outcomes using an incremental implementation cost-effectiveness ratio, interpreted as the additional cost incurred for the intervention to achieve one-unit increase in implementation outcomes (e.g., reach, adoption, implementation, and maintenance) measured. The cost data and results are intended to support policy makers (e.g., insurers) for informed decision-making regarding the reimbursement of FHWPs in the community context, such as the cost range (intervention plus implementation) per enrolled family. 48
Massachusetts General Hospital, MA-CORD 3.0
Family healthy weight program
The Healthy Weight Clinic (HWC) is a family-based program for children aged 2–18 years with overweight or obesity. It meets the criteria for an IHBLT program and was developed by the Massachusetts General Hospital in partnership with the AAP Institute for Healthy Childhood Weight. HWC integrates components from the Connect for Health initiative 49 and a primary care-based intervention informed by the CDC-funded Mass in Motion Kids 50 and Clinic and Community Approaches to Healthy Weight trials. 51 The program is grounded in the Knowledge to Action Framework, which translates research into practice through an iterative process of adapting interventions to local context, identifying barriers, implementing strategies, and ensuring sustainability. Stakeholder input is central throughout.
HWC includes 12 individual visits over 12 months with a multidisciplinary team [pediatric medical provider, community health worker (CHW), and registered dietitian/nutritionist] and six group visits within the first 6 months. Families receive tailored educational tools and materials, while group sessions foster peer support and shared learning. Through the MA-CORD 3.0 project, the packaged HWC was piloted across multiple health centers in Mississippi and Massachusetts, including federally qualified health centers (FQHCs) and an academic medical institution. 35
Dissemination and implementation strategy
The HWC implementation support package includes a suite of resources, online asynchronous training modules, technical assistance, and structured virtual learning community with QI improvement to drive implementation and maintenance. Some key aspects of the training that are unique to the HWC include 11.5 hours of asynchronous provider training modules and integration of QI and virtual learning collaboratives with AAP and the Massachusetts General Hospital staff for technical assistance. HWC teams were offered to participate in QI and earn specialized Maintenance of Certification (MOC) credits to maintain licensure. The onboarding and training package integrates multiple MOC credit opportunities along with continuing medical education credits. In addition to QI science, the onboarding, training, and technical assistance provided to sites are driven by implementation science with the ultimate goal of integrating these programs into workflows and structures that support ongoing sustainability.
Cost assessment of implementation
The HWC cost calculator is a spreadsheet-based tool incorporating parametric models to support scenario analyses by varying key assumptions such as staff salaries and clinic capacity. It allows clinical sites to estimate site-specific delivery costs—including staffing needs—and adjust for contextual factors like urban or rural settings. The research team applied this tool in case studies at three clinics to assess site-level break-even points and project potential revenue from medical reimbursement.
Building on prior evidence from an RCT demonstrating HWC’s cost-effectiveness, 20 this analysis focused on budget impact analysis (BIA) to support real-world implementation and long-term sustainability planning. The BIA quantified program costs by itemizing components and estimating the minimum number of patients needed to achieve break-even. Cost inputs included staffing time for PCPs, registered dietitians, CHWs, and medical assistants. Using the cost calculator, the team produced practical estimates to guide financial and operational planning for broader dissemination of the HWC model. The resulting data provide actionable insights to inform the development of sustainable payment models for pediatric obesity care, based on real-world costs and revenue data from clinical implementation sites. 52
Miriam Hospital, RI-CORD 3.0
Family healthy weight program
JOIN for ME is an evidence-based FHWP initially developed as a collaboration between United HealthGroup and Y-USA. JOIN for ME is a 10-month program where groups of 6–8 dyads (caregivers and children ages 6–12) complete 16 weekly one-hour sessions, followed by 6 months of advanced sessions (four biweekly and four monthly sessions). Dyads also have a brief individual check-in surrounding weekly weight and goals in advance of the group session.
Although originally designed to be delivered in -person by YMCA coaches, in RI-CORD 3.0, JOIN for ME was adapted for virtual delivery by CHWs to increase the likelihood of dissemination. Consistent with the initially developed in-person model of JOIN for ME, the remote program was delivered to families over 10 months. Groups were delivered via HIPAA-compliant Zoom platform, with interactive activities embedded into sessions to enhance engagement.
Dissemination and implementation strategy
RI CORD 3.0 used implementation strategies that spanned multiple domains, including (1) adapting JOIN for ME to their implementation settings (FQHCs and low-income housing authorities) and the clients served in these settings; (2) training, educating, and providing clinical supervision to CHWs who led JOIN for ME; and (3) engaging stakeholders through blended program facilitation and establishment of a community advisory board. Intervention adaptations were informed by in-depth interviews with stakeholders within implementation organizations, previous coaches of JOIN for ME, and key community members with experience working with the targeted population. Focus groups were also conducted with caregivers and children who would be eligible to participate in JOIN for ME. 53 Blended facilitation 54 was utilized to harness complementary knowledge and skills of the research team, the community setting staff, and the CHWs. Specifically, within each community setting, internal facilitators were identified to serve as champions of the program, collaborating with the research team on recruitment and delivery. Internal facilitators were paired with a CHW and members of the research team to promote, increase awareness, and share information about JOIN for ME with families.
Cost assessment of implementation
The JOIN for Me costing approach followed a health system perspective, which includes direct medical costs but excludes opportunity cost of time spent by families making lifestyle changes. Thus, the costs that were modeled reflect costs likely to be incurred by organizations implementing JOIN for ME with their patient or client population and are meant to inform decision-making around reimbursement and delivery models. The needed time and economic data were taken as a snapshot of labor involved in delivery of the program during a two-year period. Necessary parties (e.g., CHWs, CHW supervisor, support staff, internal facilitator) were asked to track their time dedicated to program implementation. This information was compiled using the Treatment Cost Assessment Tool.43,44 Actual costs per dyad were then modeled for both the core sessions (first 4 months of weekly sessions) and the entirety of the 10-month treatment delivery. The research team extended the cost analysis to also manipulate certain logistical details, including modeling cohorts that each started with 8 dyads, as some cohorts in the research project were smaller due to the delayed treatment assignment.
Acknowledging that financial investment is not just undertaken in the delivery of a program but also in its start-up, costs of pre-implementation activities were tracked using the Cost of Implementing New Strategies (COINS) tool. 45
Stanford University, CA-CORD 3.0
Family healthy weight program
Stanford HEALTHY is a secure, online platform based on the Stanford Pediatric Weight Control Program, a proven family-based, group, behavioral weight control program. 37 Designed with technology and user-centered biodesign principles, it enables any health care professionals, hospitals, clinics, insurers, employers, or community organizations to deliver an effective program with minimal training. The platform supports in-person or remote delivery, ensuring accessibility and scalability.
The six-month program includes 26 weekly sessions: 23 90-minute group sessions and three 30-minute individual family meetings, totaling 36 contact hours. Sessions provide tailored feedback from a behavior coach (group leader) and teach skills for healthy eating, physical activity, reducing screen time, and problem-solving. The program is grounded in Bandura’s social cognitive theory 55 to promote self-monitoring, goal-setting, reciprocal contracting, and strategic rewards. Activities include enactive rehearsal, role-playing, behavior modeling, social support, 56 and supervised physical activities. Individual family meetings with a behavior coach occur at key intervals (the 7th, 14th, and 21st sessions). The platform highlights personalized reviews of progress and problem solving and skills reinforcement.
Dissemination and implementation strategy
The CA-CORD 3.0 project repackaged the Stanford Pediatric Weight Control Program to create a scalable, cost-effective behavioral weight control solution. After more than two decades of clinical and public health program dissemination, the research team integrated scaling insights from the technology industry. 57 This approach utilized the IDEAS framework (Integrate, Design, Assess, Share) for digital health innovation 58 and the Stanford Byers Center Biodesign innovation process. 59 The IDEAS framework incorporates behavior change principles, 58 design thinking, software development, and rigorous evaluation. Its four key tasks are: integrating behavioral theory and user insights, designing iteratively with user feedback, assessing efficacy via rigorous testing, and sharing results. The Biodesign process 59 commonly used for medical device innovation, complements IDEAS by emphasizing dissemination, commercialization, and strategy development. It uses a needs-driven, design-thinking approach to address challenges and identify solutions tailored to end-users and stakeholders. Leveraging decades of experience in behavioral research and clinical care for childhood obesity, the research team combined these frameworks to refine interventions, prototype solutions, and plan for implementation and commercialization.
Cost assessment of implementation
The CA-CORD 3.0 project has primarily focused on packaging and dissemination strategies; however, a prospective pilot trial has not yet been conducted. To estimate costs, the Massachusetts General Hospital HWC calculator was used to model various scenarios based on historical data and current expenses for the Stanford Pediatric Weight Control Program. These models incorporated different assumptions and projections to account for implementation in other settings. Given that Stanford HEALTHY is designed for broad adaptability across different types of organizations and environments, payment models and associated costs are expected to be locally driven and vary significantly.
Washington University at St. Louis, MO-CORD 3.0
Family healthy weight program
The Washington University at St. Louis-led MO-CORD 3.0 project, partnered with Children’s Mercy Kansas City, Freeman Health Systems, and Pennington Biomedical Research Center, provided Missouri Medicaid-insured children aged 5–12 and their caregivers with family-based behavioral treatment (FBT) for obesity, 60 referred through PCPs. FBT emphasizes parenting support, social network facilitation, and skill-building for both children and parents across environments. Licensed clinical social workers and registered dietitians received training via an electronic curriculum and ongoing supervision from expert psychologists to deliver group and individual coaching sessions. Parent–child dyads participated in weekly virtual sessions over 4 months, followed by monthly and then bimonthly visits for a total of 6 months (29 contact hours). Dyads also received 1 hour and 45 minutes of virtual medical nutrition therapy delivered by a registered dietitian nutritionist. Participants were also offered an additional 3 hours of virtual FBT and 30 minutes of medical nutrition therapy in the following 6 months. Sessions aligned Missouri Medicaid’s family-based behavioral treatment benefits, enabling billing and coordinated care between coaches and PCPs with no out-of-pocket costs for the family.
Dissemination and implementation strategy
The implementation strategies for FBT included (1) contracting with two pediatric health systems to fund interventionists to deliver the FBT, (2) launching a digital platform for interventionists and patient families, (3) using implementation mapping to create tools for PCPs to refer eligible patients, and (4) leveraging a new reimbursement mechanism to sustain and expand the program.
Each health system funded 0.8 full-time equivalent (FTE) interventionist time, employing a licensed clinical social worker in the rural system and hiring a new registered dietitian nutritionist in the urban health system. The digital platform, developed with user-centered design, 60 provided an online video-based training for interventionists and materials, including weekly reflection forms for families. Provider referrals were critical for sustaining the program by maintaining a steady stream of participants. Tools for referrals included workshops, daily notifications in electronic pre-visit checklist, a referral guide, patient materials, and recruiter follow-up calls. Missouri Medicaid’s approval of the biopsychosocial obesity treatment package allowed for reimbursement for FBT, 61 supporting its sustainability and providing a framework for team-based care beyond the project.
Cost assessment of implementation
Missouri Medicaid launched the Biopsychosocial Obesity Treatment benefit to reimburse obesity treatment services for Medicaid enrollees, 61 laying the foundation for the FBT program. As part of MO-CORD 3.0, a cost analysis was conducted to examine the human, economic, and societal values of the program. This analysis considered disease prevalence; anticipated participation and attrition rates; outcomes from prior trials; and modeling cost savings for adults and children at 1 and 3 years.
Using a micro-costing approach, the research team estimated both labor and nonlabor costs from a societal perspective, capturing expenses for providers, participants, and payers. Training and program costs were evaluated separately. Training costs comprised time spent completing FBT modules, measured through website analytics and self-reported surveys. Program costs were estimated using electronic health record data, including visit frequency, session duration, and provider time. The research team also tracked provider engagement with training resources during program delivery and used survey to record time spent on nonresearch implementation activities by FBT providers, medical providers, and clinic administrators. Participant-incurred costs and website maintenance fees were also included. This comprehensive costing approach informed the program’s value and sustainability within Medicaid settings.
Discussion
This article examines the application of cost analysis and economic evaluation in implementing FHWPs using case studies from five CDC’s CORD 3.0 funded projects. It highlights various costing approaches, including identification, measurement, and valuation of costs, and contextualizes these methods within the unique settings and characteristics of each program. Despite variability in program models, delivery settings, resource needs, and partner priorities, several generalizations emerge. First, all five projects employed direct measurement approaches—such as time-driven activity-based costing or micro-costing methods 42 —to estimate the costs associated with implementation strategies. Although the specifics differed, each site systematically identified implementation resources, assigned costs, and tracked expenditures prospectively. Labor consistently represented the largest category across sites, especially those associated with training, recruitment, and program delivery. Projects also captured costs related to supplies and IT infrastructure. Second, several sites applied structured frameworks to guide their costing efforts. For example, University of Nebraska System used Proctor’s specification framework 40 and the Implementation Research Logic Model 41 to identify discrete implementation strategies and match them to time-based activity tracking. Miriam Hospital employed the COINS tool 45 to capture phase-specific implementation costs. Massachusetts General Hospital developed a site-customized cost calculator that allowed for modeling break-even points based on projected costs and revenues. Third, many sites distinguished between fixed, one-time costs (e.g., training development, adaptation) and variable or recurring costs (e.g., session delivery, supervision). This allowed for sensitivity analyses on scalability and provided useful information for sites and payers interested in forecasting future costs under different enrollment scenarios. Together, these general patterns reflect both methodological convergence and adaptations to fit diverse delivery environments.
Cost Categories: Labor, Supplies, Space, and Information Technology
Applying Michaud et al.’s checklist for guiding the conduct and reporting of cost analysis of implementation strategies, costs across five FHWPs were organized into standard categories (e.g., labor, supplies, space, information technology, travel, and others), 30 to produce decision-relevant data and improve the comparability of implementation cost findings across settings. Unlike traditional economic evaluations, which often incorporate formal and informal health care costs and downstream (e.g., opportunity costs), 62 the implementation cost analysis focuses solely on resources required to execute strategies that enable evidence-based programs to function effectively within specific systems or contexts. 29 That said, participant costs are not always included when estimating implementation costs. These costs—such as time, transportation, or access to care—can be highly relevant to program engagement. For instance, University of Nebraska System and Washington University at St. Louis incorporated participant costs into their cost assessment. In addition, most projects did not account for space costs since sessions were often conducted during off-hours (University of Nebraska System) or included in the indirect cost of the project funding (Miriam Hospital and Stanford University).
Distinguishing Implementation Strategy versus Program Costs
It is recognized that evidence-based programs intended to improve health outcomes generally include two cost domains—costs of the intervention/treatment and costs of its implementation (i.e., implementation strategies). 30 All projects measured FHWP delivery costs, but projects of University of Nebraska System, Miriam Hospital, and Washington University at St. Louis have also explicitly estimated cost associated with implementation strategies, such as fund and contract, learning collaboratives, facilitation, or implementation mapping. Disentangling implementation costs from program costs can be challenging, particularly when strategies span multiple implementation stages. For example, all FHWP projects used program packaging implementation strategies across preparation, implementation, and sustainment phases as outlined in Table 2. Finally, even within the term ‘implementation strategy,’ there are strategies that are intended to improve reach (e.g., recruitment and retention strategies), strategies intended to improve adoption (e.g., recruitment and retention of delivery staff or organizations), strategies intended to improve implementation (e.g., fidelity to core program components), and strategies intended to improve maintenance of delivery (e.g., delivering the program to multiple cohorts over time). 48 Clearly, distinguishing costs across strategy types and intended outcomes is a ripe area for future research.
Fixed versus Variable Costs and Break-Even Thinking
Depending on the purpose of the cost information, implementation costs can be categorized into fixed costs (unaffected by participant numbers) and variable costs (dependent on participant volume), 29 escalating with scaling. Implementation costs could also be categorized as the fixed one-time cost (e.g., start-up investment) contrasted with recurring costs like ongoing training or QI and control.63,64 Combining the concept of fixed versus variable and one-time versus recurring costs, studies planning to conduct the cost estimate of implementation could further report fixed one-time costs alongside variable costs. This allows for the calculation of the break-even point—where the number of participants enrolled and completing evidence-based programs offsets total program costs through generated revenue, as demonstrated in the BIA conducted by Massachusetts General Hospital. 52
Cost Measurement Methods and Frequency
All projects used direct measurement methods 30 (e.g., micro-costing, activity-based costing, bottom-up, or ingredient approach) to estimate implementation costs, tracking inputs (labor, space, supplies) and multiplying quantities of the inputs with their corresponding unit costs. While these costing methods differ in name—time-based activity-driven, activity-based, bottom-up, ingredient—they share core principles and can be broadly classified under the umbrella of micro-costing. While precise, the micro-costing approach is resource-intense and expensive, resulting in tradeoffs when planning implementation cost assessments. Massachusetts General Hospital adopted a less resource-intensive top-down approach—using percentage FTE coverage supplemented with cost surveys to estimate the time and costs for training, supervision, and QI—slightly different from all the micro-costing or similar methods used in other four projects. This approach, along with invoices from the delivery sites, may be more feasible and pragmatic for FHWPs delivered in clinical settings, given the competing demands of clinical services and its alignment with how other treatment programs are typically delivered. This observation emphasizes the importance of selecting and applying an appropriate costing method that fits specific settings and personnel characteristics.
The frequency, associated with precision, of cost data collected is also varied. For example, University of Nebraska System, Miriam Hospital, and Stanford University conducted weekly activity tracking, while Massachusetts General Hospital conducted cost data collection monthly per personnel, and Washington University at St. Louis gathered data quarterly. Moreover, established tools, such as the Treatment Cost Assessment Tool and COINS tool (Miriam Hospital), the Cost Calculator (Massachusetts General Hospital), 52 and a prespecified time-based activity-tracking (University of Nebraska System), facilitated these processes. 48
Cost Estimate by Implementation Phases
To provide practical and actionable cost information for decision-makers, some projects also organized and categorized cost data in innovative ways. For instance, Miriam Hospital combined a bottom-up costing approach with the COINS framework to estimate implementation costs by phases. The COINS tool, an extension of the Stages of Implementation Completion, tracks all activities across three phases: pre-implementation, implementation, and sustainment. Similarly, a family-based weight management intervention under the CDC’s CORD 2.0 project divided its cost analysis into preparation and implementation phases.65,66 In another example, University of Nebraska System tracked specific implementation strategies used at each phase, such as “fund and contract” strategies during the exploration phase and “packaged programs” and “action learning collaboratives” during preparation, implementation, and sustainment phases. Assigning costs to specific implementation phases is complex, particularly when strategies (e.g., training or packaged programs) span multiple phases or overlap with general operations. 27 However, this information is critical for stakeholders seeking a comprehensive understanding of implementation activities and assessing the feasibility of adoption.29,67
Costs associated with the early stages of implementation—particularly pre-implementation—can be difficult to capture once a project progresses beyond that stage. 68 Nonetheless, at least one project, University of Nebraska System, collected cost data across the pre-implementation stage, including exploration and preparation. Another concern is that some pre-implementation activities are one-time costs that are not required in future adoption or sustainability efforts and are therefore excluded from overall implementation cost estimates. 69 For example, Miriam Hospital identified its pre-implementation activities—such as qualitative data collection and stakeholder analyses to adapt JOIN for ME—as a one-time investment. These activities contributed to the development of a final packaged product, thereby eliminating the need for future organizations to undertake similar efforts. As such, these development costs were excluded from the overall implementation expense across the spectrum.
Lessons Learned
Balancing accuracy with feasibility is critical in cost assessments. Although the micro-costing approach offers precision, it can be burdensome, especially with prospective designs. Technologies like smartphone apps and online tracking tools could reduce respondent burden, but stakeholders may prioritize program delivery over detailed cost tracking. While we acknowledge that the cost assessment protocol may be of limited direct relevance for program providers, it is important to note that without a clear and consistent process to understand costs, there is a real possibility that the true costs of implementation may be overlooked. This article attempted to apply a published checklist 27 for reporting cost assessment methods in implementation studies. Beyond supporting standard reporting, the checklist could also aid in planning, resource identification, and enhancing methodological rigor—thereby advancing the field. Moreover, mixed-method approaches can complement quantitative findings. 70 Techniques such as systems mapping, 71 stakeholder engagement, and process mapping,42,72 can further support the documentation of resources and implementation activities. Finally, with a Grade B rating from the USPSTF, childhood obesity treatment is required to be covered by private insurers without cost-sharing. 8 The cost data can guide policymakers in determining reimbursement structures for FHWPs in various settings, including community, primary care, and digital environments.
Conclusions
The cost of implementation remains an underreported but essential consideration for the adoption, implementation, and sustainability of evidence-based programs. This study offers an overview of five diverse approaches used to assess implementation costs for FHWPs within CDC’s CORD 3.0 initiative. By applying structured frameworks and practical costing tools, these projects demonstrate how implementation cost assessment can inform strategic planning, reimbursement negotiations, and long-term sustainability. These findings lay a foundation for improving cost conceptualization, transparent reporting, and more effective integration of economic evaluation in future FHWP dissemination and implementation efforts.
Impact Statement
This study reviews and summarizes implementation cost assessment methods across five family healthy weight programs in CDC’s CORD 3.0 initiative. It highlights consistent, structured costing approaches that support planning and sustainability, offering practical guidance for future adopters to enhance cost transparency, comparability, and integration in diverse implementation settings.
Authors’ Contributions
Conceptualization: T.L.M. and P.A.E.; Methodology: T.L.M., P.A.E., C.F.R., D.D.F., J.D.S., and A.E.S.; Project administration: J.L.H., K.A.H., L.F., E.J., T.R., and D.W.; Writing—original draft: All authors; Writing—review and editing: All authors.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.