
Abstract
Background:
Standardized workflows supporting primary care provider (PCP) detection and management of obesity and its comorbidities are lacking in resource-poor settings. We evaluated the use of technological and visual aids to support PCP documentation, assessment, and management of comorbidities in youth with overweight and obesity.
Methods:
A prospective electronic medical record (EMR) chart review evaluated the impact of technological (EMR SmartPhrases) and visual (graphic and written reminders) aids, as well as provider training, on standardizing provider documentation and management of overweight- and obesity-related comorbidities during health care maintenance visits. Baseline intervention (T0) and postintervention (T1, T2, and T3) assessments were conducted from March 2022 to June 2023. Patient charts of children aged 5–12 years with overweight and obesity were reviewed for PCP identification of comorbidities, relevant laboratory orders, plans, and 3-month follow-up. T1, T2, and T3 measures were compared with T0 measures using Fisher’s exact test and t-test for categorical and continuous variables, respectively.
Results:
Of 100 baseline and 300 postintervention charts reviewed, 3-month follow-up visits increased significantly in patients with overweight and class 1 obesity (3%–27% and 14%–40%, respectively, from T0 to T3; p = 0.02). Planned lifestyle changes increased significantly in patients with class 1 obesity (8% at T0 versus 30% and 40% at T1 and T2; p = 0.02 and p = 0.002), respectively, but not in patients with overweight. Initial increases in the use of aids were not sustained.
Conclusions:
Technological and visual aids, along with PCP training, may support the adoption of standardized provider documentation, assessment, and management of weight-related comorbidities in youth with overweight and obesity in resource-poor settings.
Introduction
Obesity is a chronic, complex, and multifactorial disease frequently managed by pediatric primary care providers (PCPs).1,2 Following the COVID-19 pandemic, obesity rates among American youth rose to 22% from 2021 to 2023, with the highest rates found in African American (36%) and Hispanic (26%) youth, exceeding the Healthy People 2030 goal of 15.5%.3,4 Similar to postpandemic national rates, there was an overall 11% increase in pediatric obesity among New York State public school students, excluding New York City, from 2022 to 2024. 5 As the rates and severity of pediatric obesity have increased, rates of comorbid chronic conditions have also increased over time, especially for ethnic minority youth.2,6–10 Prevalence rates of obesity-related comorbidities for children with overweight and/or obesity vary widely, including, metabolic syndrome (37%–54%), prediabetes or type 2 diabetes (15%–47%), dyslipidemia (22%–43%), metabolic dysfunction-associated steatotic liver disease (MASLD) (44%–85%), hypertension (4%–30%), obstructive sleep apnea (46%–60%), orthopedic problems (16%–32%), and psychological conditions (2%–27%).1,6,7,11–18
As primary entry points to the pediatric health care system, PCPs play a key role in assessing weight status and identifying comorbidities during health care maintenance (HCM) visits. These visits are annual, routine, proactive, and comprehensive checkups designed to monitor a child’s physical growth, development, and overall health. The American Academy of Pediatrics (AAP) Bright Futures handbook, both the new (2023) and old (2007) AAP clinical guideline recommendations, the 2015 Institute for Healthy Childhood Weight algorithm for the assessment and management of childhood obesity, and subspecialty guidelines from the Pediatric Endocrine Society, North American Society for Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN) Society, and AAP pediatric hypertension guidelines provide obesity and comorbid condition assessment and management support.1,15,19–23 The new AAP clinical guidelines also offer guidance on weight management medications and bariatric surgery. 1
Although increased documentation of a diagnosis of obesity leads to increased comorbidity screening, which may facilitate sooner follow-up and referral to appropriate specialists, particularly for minority youth, the implementation of existing guidelines during annual HCM visits is often limited by time constraints, lack of provider interest, and inadequate staffing or resources.24–26 Standardized electronic medical record (EMR) technological aids, including SmartPhrases, order sets, and clinical decision trees, improve clinical efficiency and chronic condition-associated patient care.24,27–29 While provider education and EMR changes improve provider documentation and management of childhood obesity, evidence-based EMR tools that guide both the identification and management of comorbid conditions are less available, especially in ethnic minority clinical settings.24,25,30–33 There is a need for brief, standardized EMR tools that support the early detection and management of both obesity and its comorbidities while limiting documentation burden in time-limited pediatric HCM visits, especially in medically and socially complex patient populations.34,35
The current study aimed to assess changes in PCP use of technical and visual aids to assist documentation and recognition of obesity-related comorbidities, and engagement of families in making lifestyle changes over time. The study also sought to explore associations between BMI and provider use of these tools, which may help inform individualized treatment planning.
Methods
Design
We conducted a prospective EMR chart review using a quasi-experimental multiple time-series design to evaluate the longitudinal impact of an intervention designed to improve PCP standardized EMR documentation of their assessment and management of overweight and obesity, and their attendant comorbidities during HCM visits from March 2021 to May 2023. The interventions consisted of brief, provider-focused technological aids, visual aids, and provider training, and were delivered as an initial intervention, followed by two booster interventions administered at 3 and 6 months later, respectively. Study participants were 14 pediatric PCPs at the Family Care Center (FCC), a comprehensive health care clinic located adjacent to a busy urban academic children’s hospital serving an ethnically diverse and underserved population in Bronx, NY, USA. Patient charts of youth aged 5–12 years with a documented BMI ≥ 85th percentile were reviewed. Provider names and patient charts were de-identified. HCM visits were identified as those visits denoted as “Well-Child visit” in the EMR. PCP documentation of obesity-related comorbidities, recommended laboratory assessment, referrals, timely follow-ups, and selected lifestyle goal-setting was assessed at four time points: (1) retrospective preintervention baseline data (T0) (from March 2021 to December 2021), (2) postinitial intervention (December 2021) (T1) (from March 2022 to June 2022); (3) first booster (August 2022) (T2) (from September 2022 to December 2022); and (4) second booster (March 2023) (T3) (from March 2023 to May 2023). The study protocol was reviewed and deemed exempt by the Montefiore-Einstein Institutional Review Board (IRB #2021-13416), in accordance with 45 CFR 46.102(d).
The Intervention
The initial and booster interventions (Table 1) were informed by the 2015 AAP Institute for Healthy Childhood Weight Algorithm and current guidelines (2007 AAP obesity, NASPGHAN, and Endocrine Society guidelines) available at the time of implementation.19,20,22,23 Notably, the 2023 AAP clinical guideline regarding childhood obesity management was released during the implementation of this project. 1
Intervention to Support Standardized Documentation of Assessment and Management of Obesity and Comorbidities During Health Care Maintenance Visits
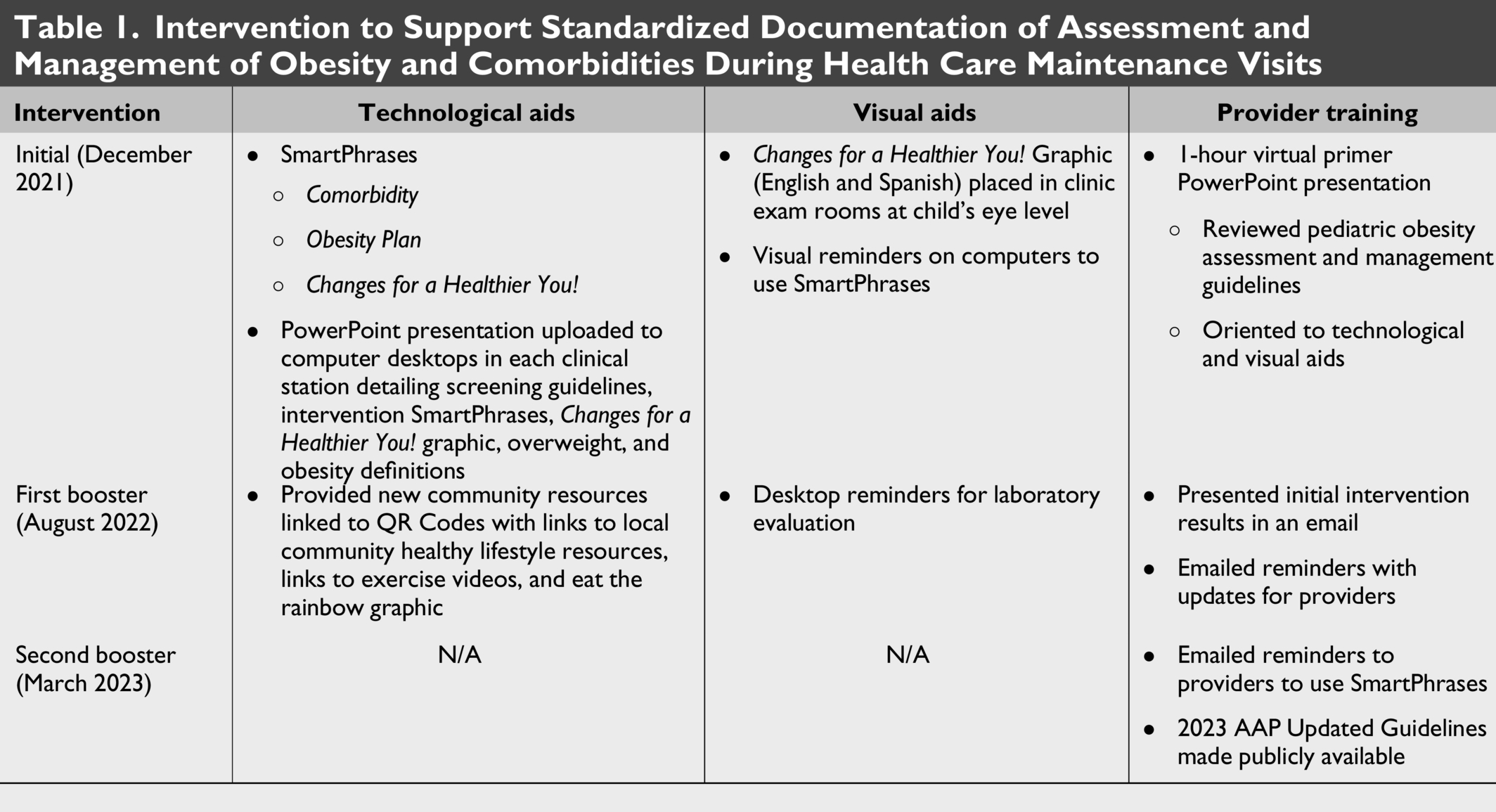
Initial intervention (T1)
Study interventions were categorized as technological aids, visual aids, and PCP training (Table 1). Technological aids, consisting of SmartPhrases and computer desktop resources, were developed to facilitate standardized PCP completion and documentation of comorbidities assessment, behavior change support, and timely follow-up. The following three Smart Phrases were recommended: (1) the Comorbidity SmartPhrase supports efficient documentation of anthropometrics, blood pressure (BP), recent laboratory results, and PCP documentation of review-of-systems-based comorbidity assessment, with a distinct version for postpubertal females (Supplementary Figs. S1A and S1B); (2) the Obesity Plan SmartPhrase prompts providers to counsel on and document SMART Goal selection and timely follow-up visit (Supplementary Fig. S2); and (3) the Changes for a Healthier You SmartPhrase facilitates the addition of the visual aid, described below, in the after visit summary (Supplementary Fig. S3). Additionally, a PowerPoint presentation summarizing the intervention was uploaded to computer desktops at clinical workstations (Table 1).
The Changes for a Healthier YOU! Graphic, a visual aid, adapted from the 7 Target Behavior Tool designed to support evidence-based healthy lifestyle changes, was displayed in exam rooms. Small written reminders to use the SmartPhrases were affixed to all computers. 36 PCP training consisted of a 1-hour virtual primer to reviewing existing pediatric assessment and treatment guideline recommendations, as well as the technological and visual aids designed to support documentation and management of youth with obesity and its comorbidities.
First booster (T2)
Technological aids introduced for booster intervention included a compilation of QR codes containing local community healthy lifestyle resources, and links to internet-based, child-friendly exercise videos (Supplementary Digital Content, Supplementary Fig. S4A–C) (Table 1). Print copies were also made accessible to PCPs for distribution to patients. Small visual reminders affixed to desktop computers prompted PCPs to order recommended laboratory tests. PCP training consisted of an email providing initial intervention updates and a reminder to use resources.
Second booster (T3)
The second booster consisted of an email reminder to encourage PCPs to utilize resources and notification of the newly published 2023 AAP Clinical Practice Guidelines.
Methods of Evaluation
Measures
Primary outcomes related to PCP documentation were: (1) use of assessment and management tools, namely the three EMR SmartPhrases; (2) recommendation of a 3-month (or sooner) time to follow-up; (3) documentation of planned lifestyle change by including a SMART goal in the plan; and (4) inclusion of laboratory assessment in the plan when appropriate (if not done within the past 2 years or had previous abnormal value) during annual HCM visits. Identification of new comorbidities was established through chart review of provider documentation in current and prior encounters, active problem lists, and/or subsequent telephone encounters noting vitals, laboratory results, and referrals supporting the relevant diagnoses. Comorbidities were defined as follows: (1) elevated BP if >90th percentile systolic Blood Pressure (BP) and/or diastolic BP; (2) MASLD, defined as liver enzymes Aspartate Aminotransferase (AST) and/or Alanine Aminotransferase (ALT) > 37 U/L and 24 U/L, respectively; (3) snoring/Obstructive Sleep Apnea (OSA), defined as documented snoring; (4) orthopedic issues, defined as lower extremity complaints such as hip, knee, or leg pain; (5) dyslipidemia, defined as any lipid abnormalities (high-density lipoprotein cholesterol <40 mg/dL, total cholesterol <170 mg/dL, triglycerides >130 mg/dL, or low-density lipoprotein cholesterol >130 mg/dL); (6) prediabetes, defined as HgBA1C between 5.7% and 6.4%; and (7) mental health issue, defined as documentation of bullying, anxiety, depression, or attention-deficit/hyperactivity disorder.
Additional patient outcomes included age (calculated from visit date and date of birth), height, weight, BMI, and BMI percentile. Initial chart reviews were cross-checked among team members to ensure consistency.
Statistical Analysis
Sample size was determined based on a power calculation. A minimum of 52 encounters per time point (208 total encounters) achieves 80% power at a 0.05 significance level using a chi-square test with three degrees of freedom, assuming outcome proportions of 25%, 35%, 45%, and 55% at T0, T1, T2, and T3, respectively. To achieve 80% power at each time point versus T0 in the subgroup of BMI >95%, assuming 70% of patients had BMI >95%, a minimum of 75 encounters at each time point was needed. Therefore, 100 encounters were reviewed at each time point (T0–T3) to ensure adequate power. Additionally, this sample size provides over 90% power to detect a difference between T0 and T3 using a two-sided proportion test at a 0.05 significance level.
Patient characteristics at T0 and postintervention timepoints, T1, T2, and T3, were summarized as counts (%) for categorical variables and mean [standard deviation (SD)] for continuous variables, and were compared using Fisher’s exact test and a t-test, respectively. Primary outcomes in each postintervention period were compared with the preintervention period using Fisher’s exact test for categorical variables and a t-test for continuous variables. Data at each time point were reported in aggregate rather than linked to individual provider behaviors. Further, we repeated analyses, stratified by four BMI groups: (1) overweight (85th to <95th percentile); (2) class 1 obesity (≥95th percentile to <120% of the 95th percentile); (3) class 2 obesity (120% to <140% of the 95th percentile); and (4) class 3 obesity (≥140% of the 95th percentile or BMI ≥ 40). Due to low numbers, patients with class 2 and 3 obesity were combined in the analysis (herein referred to as class 2 + 3 obesity). 1
Results
Comparison of 100 unique well-child visits for the preintervention baseline assessment (T0) and 300 charts postintervention (T1, T2, and T3) revealed no significant differences in age, sex, weight, height, BMI, or the proportion of patients with overweight or obesity (Table 2).
Baseline and Postintervention Cohort Characteristics
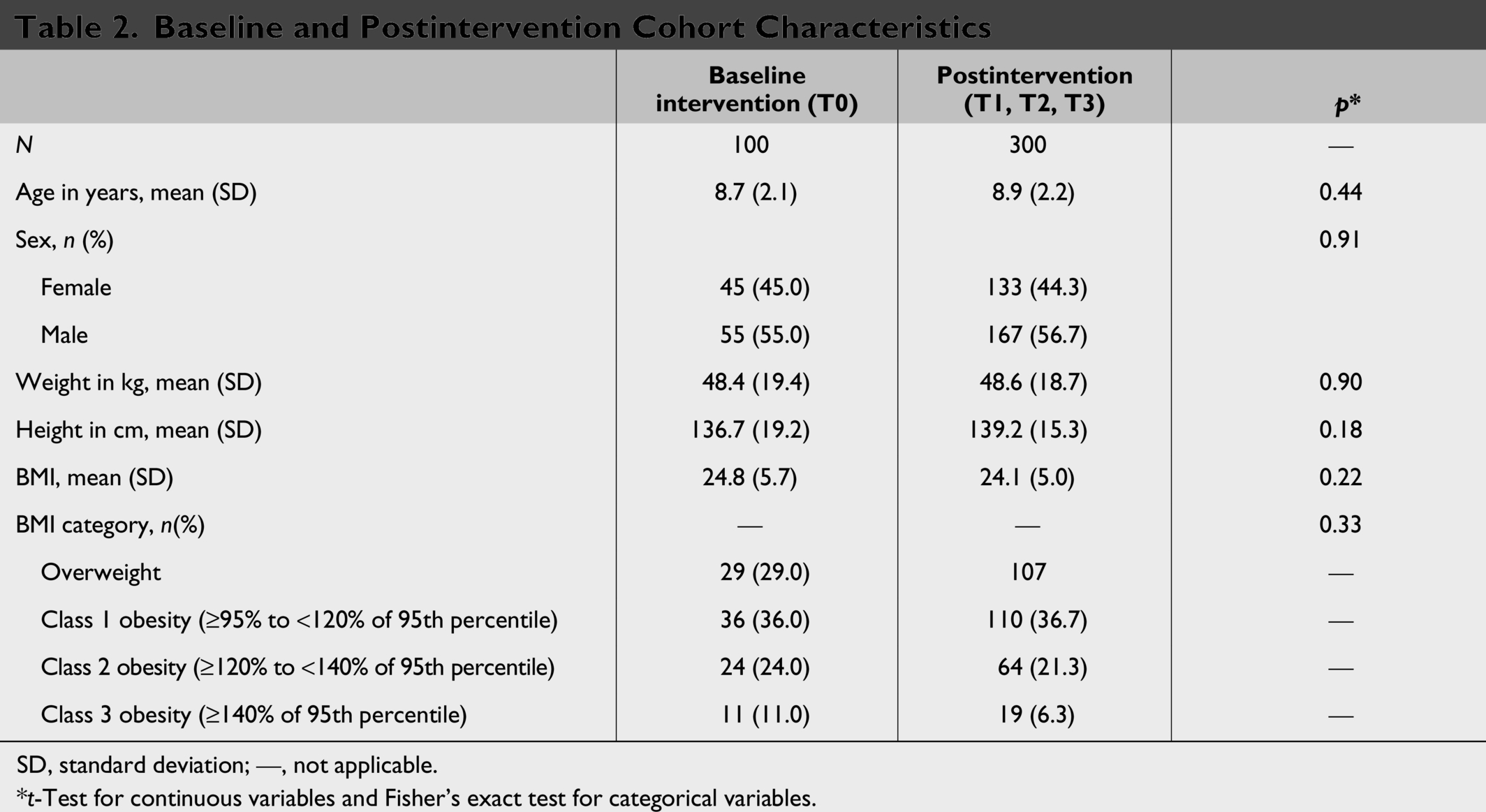
SD, standard deviation; —, not applicable.
*t-Test for continuous variables and Fisher’s exact test for categorical variables.
Provider Documentation of Use of Assessment Tools
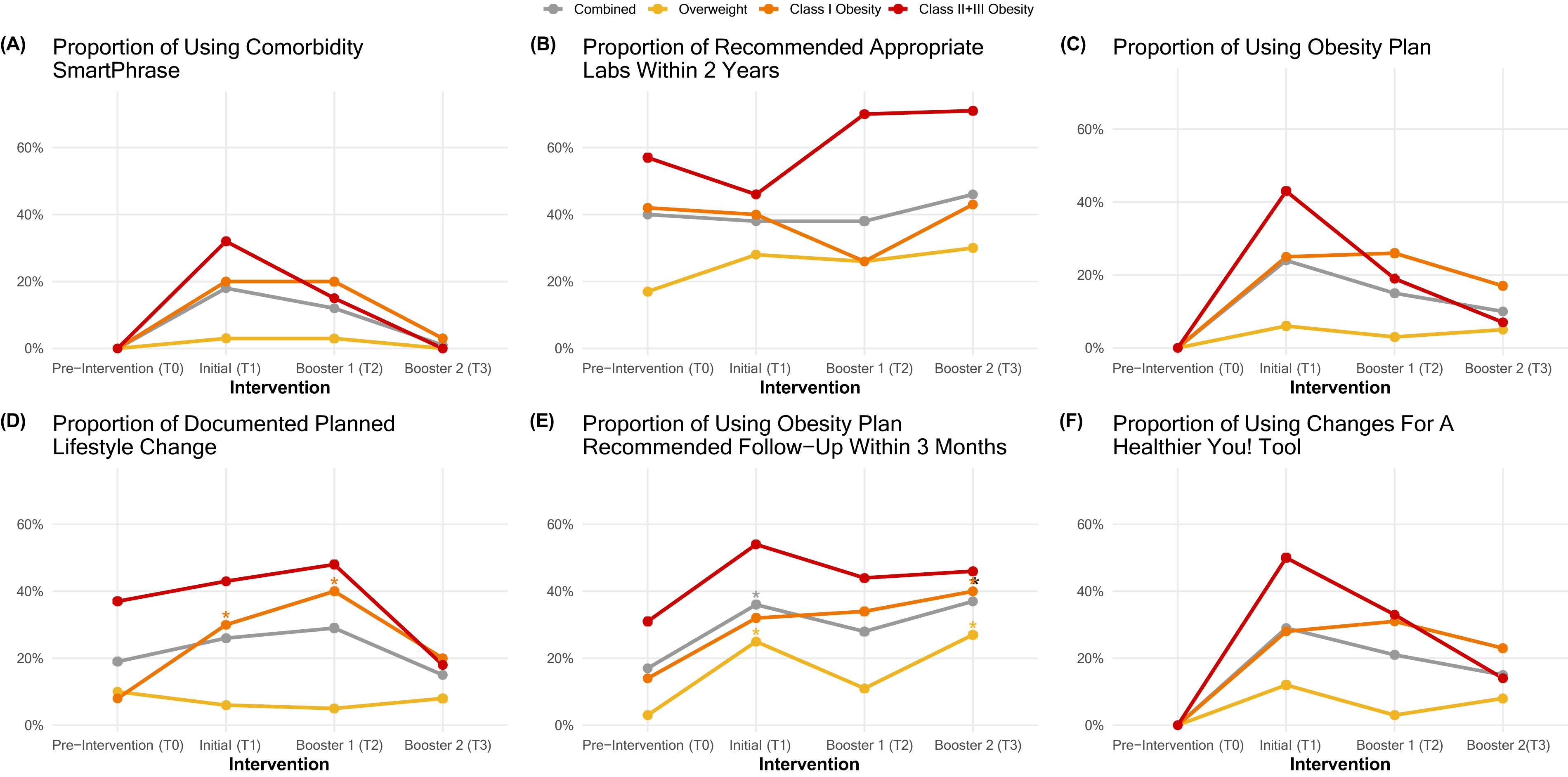
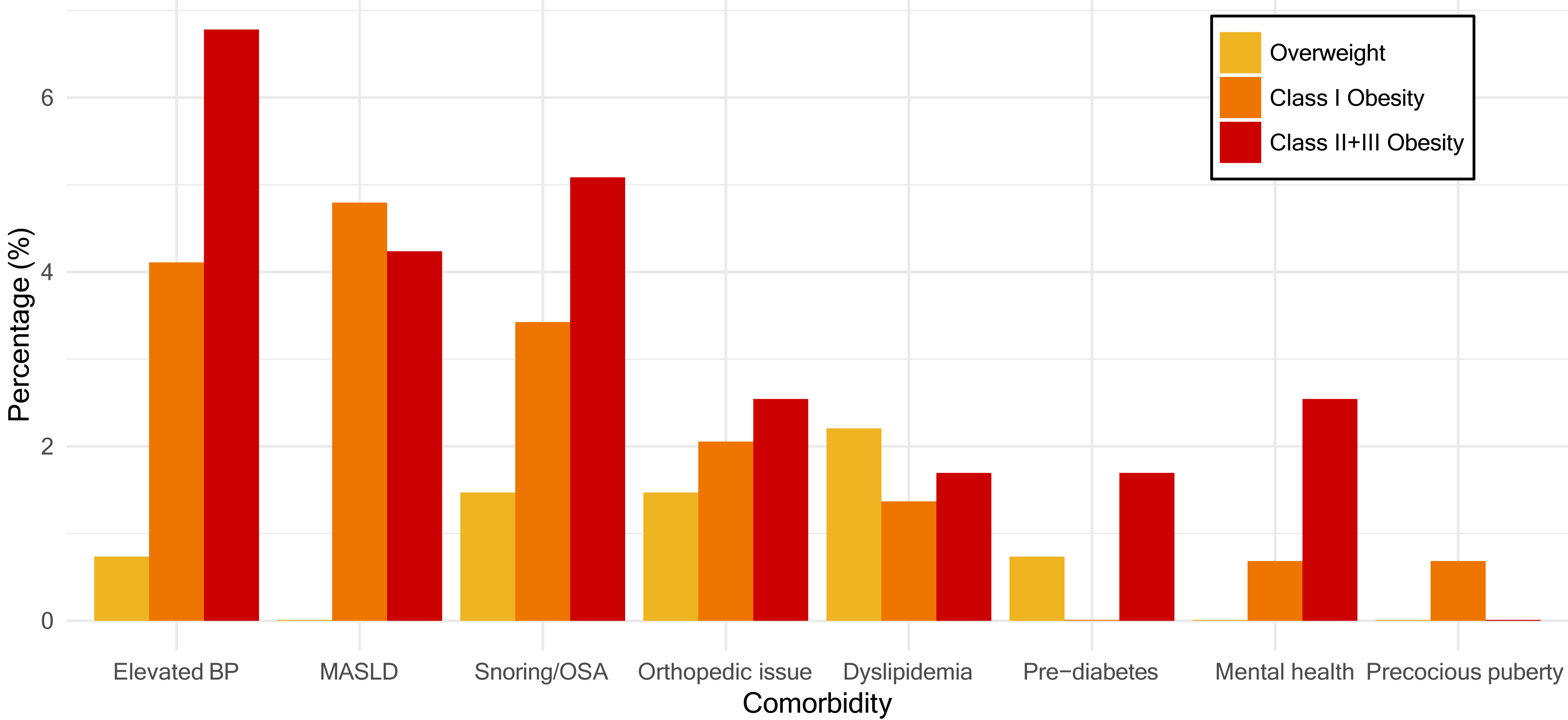
Utilization of the comorbidity screening SmartPhrase reached 3%, 20%, and 32% for patients with overweight, class 1 obesity, and class 2 + 3 obesity, respectively, at T1, but demonstrated a nonsignificant downward trend over time (Table 3 and Fig. 1A). While identification rates of new comorbidities increased with BMI [overweight (3%), class 1 obesity (17%), and class 2 + 3 obesity (37%), respectively] at T0, proportions decreased over time, with a significant decrease in documentation of comorbidities in patients with class 2 + 3 obesity at T3 (11%) relative to T0 (Table 3). Elevated BP (23%), snoring/OSA (20%), and MASLD (20%) were the most common new comorbidities identified, whereas mental health concerns, including bullying (6%), and prediabetes (elevated HbA1c) (5%) were the least common (Supplementary Fig. S5). Overall, rates of newly identified comorbidities increased with increasing BMI (Fig. 2).
Proportion of Encounters with Documentation of Assessment and Management Tools Baseline and Postintervention in Patients with Obesity and Overweight
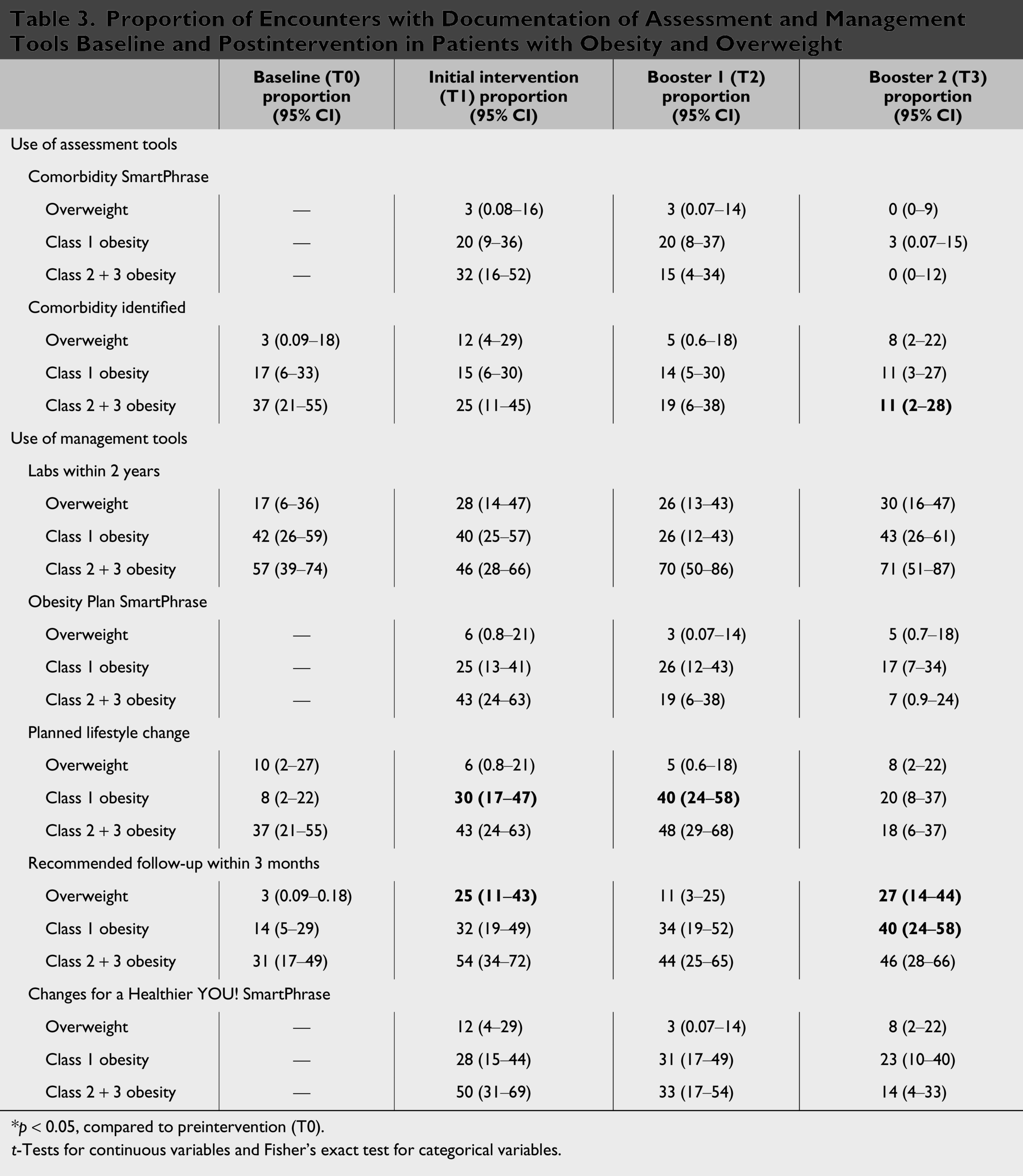
*p < 0.05, compared to preintervention (T0).
t-Tests for continuous variables and Fisher’s exact test for categorical variables.
Provider Documentation of Use of Management Tools
Documentation rates of laboratory assessment increased with BMI [overweight (17%), class 1 obesity (42%), and class 2 + 3 obesity (57%), respectively] at T0 and demonstrated a nonsignificant upward trend over time (Table 3 and Fig. 1B).
Obesity Plan SmartPhrase use increased with BMI [overweight (6%), class 1 obesity (25%), and class 2 + 3 obesity (43%), respectively] after the initial intervention (T1), but demonstrated a nonsignificant downward trend over time (Table 3 and Fig. 1C).
Notably, rates of documenting a planned lifestyle change increased only in patients with class 1 obesity (30%) and class 2 + 3 obesity (43%), respectively, after the initial intervention (T1). While minimal change was observed in planned lifestyle change documentation rates in patients with overweight, this proportion increased significantly in patients with class 1 obesity from 8% at T0 to 30% at T1 and 40% at T2, but then decreased to 20% at T3. A similar nonsignificant trend was observed in patients with class 2 + 3 obesity (Table 3 and Fig. 1D).
Overall, within each BMI category, 3-month follow-up recommendation rates increased over time, with significant increases observed in patients with overweight and class 1 obesity (3% at T0 to 27% at T3, p = 0.03, and 14% at T0 to 40% at T3, p = 0.17, respectively) (Table 3 and Fig. 1E).
Provider utilization of the patient-selected goal/plan and Changes for a Healthier YOU! graphic SmartPhrases reached 12%, 28%, and 50% for the patients with overweight, class 1 obesity, and class 2 + 3 obesity at T1, respectively; however, this increase was not maintained over time (Table 3 and Fig. 1F).
Discussion
We successfully implemented technical and visual aids during HCM visits for children with overweight and class 1 obesity in a resource-poor, inner-city setting. We observed significant increases in provider documentation of more frequent follow-up visits and, although not sustained, significant increases in planned lifestyle change documentation among patients with class 1 obesity. We also observed an upward trend in recommended laboratory orders for patients with overweight and class 2 + 3 obesity over time. As in other studies, we observed that provider education and EMR changes improved weight management follow-up recommendations in an ethnically diverse and underserved population.³³ Observed increases in documentation of recommended follow-up and planned lifestyle changes align with previous work suggesting that increased opportunities to set short-term goals may lead to long-term behavior modification.37,38 Furthermore, our findings align with other studies demonstrating that simple, targeted, evidence-based tools may enable busy clinicians to implement guideline recommendations with minimal provider time or effort, to ensure more frequent follow-up visits, ordering laboratory testing, and lifestyle change support.1,28,39 The 2023 AAP clinical practice guideline coincided with the second booster period and may have reinforced provider behavior change. 1
Interestingly, we did not observe significant increases in the Comorbidity SmartPhrase, comorbidity identified, Obesity Plan SmartPhrase, or Changes for a Healthier You! SmartPhrase use. Implementation of these tools may require greater provider skill, comfort, effort, and time, thereby decreasing the likelihood of their routine implementation. Importantly, these findings suggest that it may be difficult for providers to add more complex tasks to the already overburdened HCM visit. Nevertheless, having readily accessible tools and a standardized approach in place may be the first step in assisting providers to complete a thorough assessment of children with overweight and obesity aligned with the current AAP guidelines, although they may be better suited for follow-up visits.
By analyzing the use of different intervention tools by BMI, we observed how these tools may promote early recognition, assessment, and intervention in children with overweight, when lifestyle changes may be easier to implement and have a longer-lasting impact on future health. Some of the new reported comorbidities, including prediabetes and dyslipidemia, were disproportionately lower compared to published prevalence rates.6,12,13,38,39 An explanation for this finding may be that these comorbidities were diagnosed previously. Alternatively, providers may not have consistently assessed for these comorbidities at all HCM visits, even in patients with higher BMIs who are at risk of developing comorbidities. A lack of provider confidence or time to assess comorbidities, even in patients with higher BMIs, resulting in lower identification of these comorbidities, has been previously reported.24,30 These findings may highlight the challenges associated with addressing the complex health care needs of patients with elevated BMI during time-limited HCM visits. In fact, patients with complex health care needs in resource-poor settings may have other social concerns, including inadequate housing and food needs, or acute medical concerns that take priority over addressing comorbidities.40,41
Interestingly, while there was a significant increase in 3-month follow-up recommendations for patients with overweight, there was no significant increase in provider usage of the Obesity Plan SmartPhrase, recommending planned lifestyle change, or the use of the Changes for a Healthier You! SmartPhrase for these patients. In contrast, planned lifestyle change recommendations increased over time in patients with class 1 obesity. Despite evidence that earlier follow-up visits may potentially delay or prevent the onset of obesity-related comorbidities, we observed a missed opportunity for providers to support the implementation of lifestyle changes in children with overweight. 42 Recognizing low lifestyle change counseling rates in youth with overweight and fewer comorbidities (29% of this cohort) identifies a future area of intervention, where earlier preventive counseling may be more impactful.
Next Steps
By focusing on preventing progression to obesity in children with overweight, additional provider training to support the implementation of these EMR tools may provide increased PCP confidence and self-efficacy in the early management of overweight. 43 Furthermore, incorporation of infrastructures that routinely inform PCPs (i.e., quarterly faculty meetings) of the positive impact of their efforts to assess, provide counseling and healthy lifestyle change guidance, and necessary referrals to patients starting with overweight status may reinforce positive PCP behaviors. Expanded support and training on the use of these EMR tools and resources in other clinics in the hospital system, the creation of dedicated follow-up visits for all children with overweight or obesity to screen for obesity-related comorbidities, and the piloting of both individual and shared medical appointment group virtual follow-ups with health educators or nutritionists to discuss lifestyle interventions may serve as future interventions to support the sustained management of pediatric overweight and obesity in a resource-poor, time-limited HCM visits.
Limitations
There are several limitations to this study. During the study, providers experienced a COVID-19 surge, shortened visit times between the initial and booster interventions, and frequent staff turnover. Less allowable time spent with patients, combined with a higher acuity sick visits, may have adversely affected providers’ ability to implement the recommended SmartPhrases. In addition, this initiative differed from the newest AAP guidelines regarding laboratory evaluation recommendations (AAP recommends obtaining laboratory studies ≥10 years of age, whereas we suggested >5 years). However, the remainder of the intervention, including comorbidity assessment and 3-month follow-up visits, is congruent with the latest AAP obesity guidelines, affirming the importance of comprehensive evaluation and frequent follow-up. 1
Conclusions
Standardizing PCP documentation, assessment, and management of children with overweight, obesity, and associated comorbid conditions using technological and visual aids, along with PCP training, can improve adherence to current pediatric guidelines. Reinforcing the use of these tools in children with overweight may support earlier identification of comorbid conditions and help prevent progression to obesity and its associated comorbidities.
Impact Statement
This study demonstrates that EMR tools can support the delivery and adoption of standardized provider documentation, assessment, and management of weight-related comorbidities in youth with overweight and obesity in resource-poor settings. Simple EMR tools changed provider behavior related to recommending more frequent follow-ups and lifestyle counseling.
Author’s Contributions
S.N.S.: Conceptualization, methodology, writing—original draft preparation, data curation, and project administration. D.M.R.: Conceptualization, methodology, software, resources, data curation, and writing—review and editing. H.J.L.: Data curation, formal analysis, writing—original draft, and visualization. J.-Y.M.: Data curation, formal analysis, and writing—review and editing. J.R.: Writing—original draft, supervision, and funding acquisition.
Footnotes
Acknowledgment
The authors acknowledge the leadership and providers of the Montefiore FCC who participated in this project.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was funded by the Health Resources and Services Administration (HRSA), Grant No. H1733892.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.