
Abstract
Background:
Neighborhood food access is considered a structural determinant of childhood obesity, yet prior studies report inconsistent findings, and longitudinal weight trajectories are understudied. This study sought to examine the association between neighborhood food access and obesity risk across the COVID-19 pandemic, which exacerbated pediatric obesity disparities.
Methods:
We conducted a retrospective longitudinal cohort study of 13,832 children aged 2–11 years receiving primary care in eastern Massachusetts between 2019 and 2024. Baseline residential addresses were geocoded to classify a child’s residence in low-income, low-food access neighborhoods with low vehicle availability (LILV). Mixed-effects models examined associations between LILV residence and repeated BMI z-scores and obesity risk over follow-up, adjusting for insurance type. Secondary analyses among publicly insured children (n = 3548) explored the association between LILV residence and obesity risk, adjusting for household food insecurity.
Results:
At baseline, 26.1% of children resided in LILV neighborhoods. No significant differences in BMI z-scores or obesity risk were observed at age 5 years. By age 10, LILV residence was associated with higher BMI z-scores [β = 0.08; 95% confidence interval (CI): 0.01–0.16] and increased obesity risk [risk ratio (RR) = 1.55; 95% CI: 1.01–2.39]. By age 15, associations strengthened [BMI z-score β = 0.14; 95% CI: 0.05–0.22; obesity RR = 1.94; 95% CI: 1.17–3.23]. Among the subset of children with public insurance, these associations were not observed.
Conclusions:
Residence in low-income, low-food access neighborhoods is associated with higher BMI and obesity risk across childhood and adolescence, independent of insurance type. These findings highlight neighborhood food access as a potentially modifiable structural determinant of pediatric obesity disparities.
Introduction
Childhood obesity prevalence in the United States has continued to rise above pre-pandemic levels and is estimated to affect over one in five children ages 2–19 years. 1 Despite some evidence that the rapid acceleration in child weight gain seen early in the COVID-19 pandemic has slowed in more recent years,2,3 the pandemic exacerbated longstanding childhood obesity disparities in the United States, with obesity prevalence rising sharply among children from low-income, Black, and Hispanic backgrounds.4,5 The pandemic also exposed structural inequities in the social and built environments that shape child health, while adding new health, economic, and psychological stressors through job losses, school closures, and social isolation.6,7
Neighborhood food access, which represents neighborhood infrastructure, and household food insecurity, an indicator of household economic resources, are both social factors related to the food environment that have been associated with childhood obesity.8–12 Specifically, neighborhood food access refers to the availability and proximity of food retailers within the area where individuals reside, typically at the census tract level. 13 Household food insecurity is defined as “an economic and social condition of perceived limited or uncertain access to sufficient amounts of nutritious food needed for an active and healthy life.”14,15 Previous research on household food insecurity and childhood obesity has yielded inconsistent findings, with reviews reporting positive, null, and even negative associations depending on age group, level of food security, and type of study design.9,16,17 Similarly, in a systematic review of neighborhood supermarket access and childhood obesity, low supermarket access was associated with obesity in half of predominantly cross-sectional studies, while others found null or opposite associations. 18 Several research gaps remain, as few studies examining the food environment have tracked weight trajectories longitudinally in a large electronic health record (EHR), across developmental periods, or throughout the COVID-19 pandemic period.9,18,19 In addition, prior studies have examined exposures of household food insecurity and neighborhood food access in isolation, focusing either on individual/household-level food security or neighborhood proximity to food retailers in distinct cohorts.20,21 Limited research examining both neighborhood food access and household food insecurity in the same cohort suggests they operate at different ecological levels 22 ; in one study, residence in a food desert was associated with higher BMI percentile only among children with household food insecurity, suggesting that neighborhood-level disadvantage may be particularly detrimental when combined with household food insecurity. 23 Examining both factors may provide different scientific and policy-level implications by distinguishing between structural environmental contexts and household-level economic constraints, which require different interventions.
Thus, this analysis examined the multilevel and longitudinal associations between neighborhood food access and childhood obesity across a 5-year period (2019–2024) straddling the COVID-19 pandemic. Our primary analysis examined whether residence in low-income, low-food access (LILV) neighborhoods among children aged 2–11 years at baseline (2019) was associated with BMI z-score and obesity risk trajectories through follow-up (2020–2024). We hypothesized that children residing in LILV neighborhoods would demonstrate higher BMI z-scores and obesity risk over time, independent of insurance type, given that insurance type is considered a proxy for socioeconomic status and an indicator of family economic resources in pediatric obesity research.22,24 Our secondary analysis focused on a subset of children with public insurance for whom household food security data were available following Massachusetts’ 2018 implementation of food insecurity screening in state accountable care organizations. 25 In this subset, we explored whether baseline neighborhood food access, as a contextual exposure, influences longitudinal weight trajectories independent of household food insecurity.
Methods
Study Design and Population
We conducted a retrospective study of children seeking primary care at 11 Mass General Brigham pediatric primary care clinics between 2019 and 2024. We included children who met the following criteria: (1) were aged 2–11 years during the baseline study period (January 1, 2019–March 1, 2020); (2) had a residential address in 2019 that could be geocoded to a census tract; and (3) had at least one measure of BMI at baseline and during the follow-up period (June 1, 2020–May 31, 2024). We selected these study periods to capture the pre-pandemic and pandemic phases of COVID-19. We restricted the analysis to this age group to minimize loss to follow-up among adolescents aging out of pediatric care during the study period. The Mass General Brigham Institutional Review Board determined that this project met the criteria for exemption.
Exposure
Our primary exposure was residence in a low-income, low-food access neighborhood at baseline. The Harvard Center for Geographic Analysis geocoded and linked each child’s baseline residential address using ArcGIS software version 10.6 (Esri) to census tract-level food access data from the USDA 2019 Food Access Research Atlas (FARA). 26 In urban settings, FARA defines low food access as a low-income census tract (i.e., federal poverty rate ≥20% or median family income ≤80% of the statewide median family income) where >100 housing units do not have a vehicle (LILV) and are >0.5 mile from the nearest supermarket. 26 The exposure was categorized as a binary variable: residence in an LILV or non-LILV neighborhood.
Outcomes
The primary outcomes were BMI z-score and obesity prevalence during follow-up. We extracted weight and height measures from EHRs, which were used to calculate BMI as weight in kilograms divided by height in meters squared. We used the growthcleanr R package to exclude implausible BMI values. 27 We used the CDC growth reference to derive age- and sex-specific z-scores and defined obesity as age- and sex-specific BMI ≥95th percentile. 28
Covariates
We selected covariates a priori based on their established associations with neighborhood food access and childhood obesity risk. We obtained variables from the EHR including child date of birth, sex, race and ethnicity (as reported in the EHR), insurance type (public or private), residential address, household food security (caregiver-reported), visit dates, clinic site, height and weight measurements. Race and ethnicity were categorized as Hispanic, non-Hispanic White, non-Hispanic Black, or non-Hispanic other. Household food insecurity at baseline was abstracted from the Hunger Vital SignTM, a validated 2-item screener administered during routine pediatric visits and recorded in the EHR. 29 Caregivers who screened positive to either question were categorized as having household food insecurity.
Statistical Analyses
Primary analysis
We used mixed-effects models to examine the associations between residence in LILV neighborhoods at baseline and repeated BMI z-scores and risk of obesity across follow-up. Our mixed-effects model included child age as a linear term, an interaction between LILV exposure and child age, and insurance type as a covariate. We included child-level random intercepts and slopes for age (to account for repeated BMI measures within the same child), as well as clinic- and census tract-level random intercepts (to account for clustering of children at clinic sites and children residing in the same neighborhood). Use of the baseline residential address in 2019 ensured that the exposure temporally preceded the outcome. These models estimated the mean predicted BMI z-scores and obesity risk over time. Furthermore, we estimated the adjusted mean differences in predicted BMI z-scores and risk ratios (RRs) for obesity at ages 5, 10, and 15 years for the average child seeking primary care in the average clinic site and the average census tract in a LILV versus a non-LILV neighborhood. These ages spanned the range of our longitudinal data (children aged 2–11 years at baseline in 2019 were followed through 2024, with the oldest reaching age 16 years), thereby capturing effects across early childhood, middle childhood, and adolescence.
In alignment with prior studies examining low-income, low-food access neighborhoods,22,30 we did not adjust for race and ethnicity in the primary analysis because we consider them social constructs and proxies for unmeasured social determinants, such as systemic racism, discrimination, and differential access to resources. 31
Secondary analysis
Our secondary exploratory analysis focused on a subset of children with public (i.e., Medicaid) insurance and available caregiver-reported household food security data (n = 3548 with complete data). Household food insecurity data were obtained from standardized screening implemented in 2018 as part of Massachusetts Medicaid accountable care organization program requirements. 25 Because this screening was not systematically implemented for privately insured patients, the secondary analysis was restricted to children with public insurance who had complete food insecurity data.
We conducted a descriptive analysis of baseline characteristics for this complete-case sample. We examined the distribution of demographic characteristics, anthropometric measures, and food insecurity status overall and stratified by both food security status (food secure vs. food insecure). We assessed differences in baseline characteristics between food security groups using chi-square tests for categorical variables, Welch’s t-tests for continuous variables with normal distributions, and Wilcoxon rank-sum tests for skewed continuous variables. Statistical significance was set at α = 0.05.
We then performed a complete-case analysis to explore the association between LILV neighborhoods and BMI z-score and obesity risk trajectories in this Medicaid cohort. Our mixed-effects model included child age as a linear term, an interaction between LILV exposure and child age, and household food security as a covariate, with the same random-effects structure used in the primary analysis.
Supplemental analysis
Sensitivity analyses were performed for both the primary and secondary analyses, with race and ethnicity included as an additional covariate.
Across all analyses, we used multiple imputation with chained equations 32 to impute missing covariate values. Insurance type and race and ethnicity had 1.8% and 14.3% missing data, respectively. We generated 15 imputed datasets for all participants in the analytic sample. Our imputation model included the exposure (LILV status), outcome (BMI measurements), and all covariates. The imputation-specific results were pooled into an aggregate model using the pool function in R.
Results
Primary Analysis: Neighborhood Food Access
We included 13,832 children between ages 2 and 11 years with neighborhood food access data, of whom 26.1% (n = 3616) resided in LILV neighborhoods (Table 1). Children residing in LILV neighborhoods were more likely to identify as Hispanic or non-Hispanic Black (p < 0.001), have public insurance (70.3% vs. 50.0%, p < 0.001), and have obesity (23.1% vs. 17.8%, p < 0.001) compared with children living in non-LILV neighborhoods. Age, sex, and the median number of visits did not differ significantly between groups.
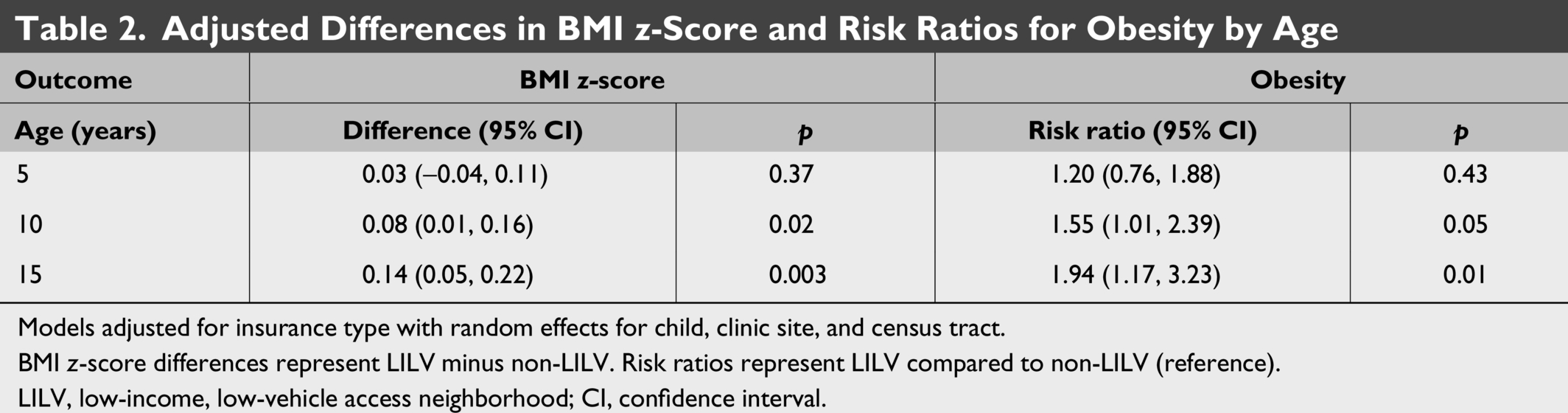
Models adjusted for insurance type with random effects for child, clinic site, and census tract.
BMI z-score differences represent LILV minus non-LILV. Risk ratios represent LILV compared to non-LILV (reference).
LILV, low-income, low-vehicle access neighborhood; CI, confidence interval.
Baseline Characteristics of Children Ages 2–11 Years by Neighborhood Food Access Status in 2019
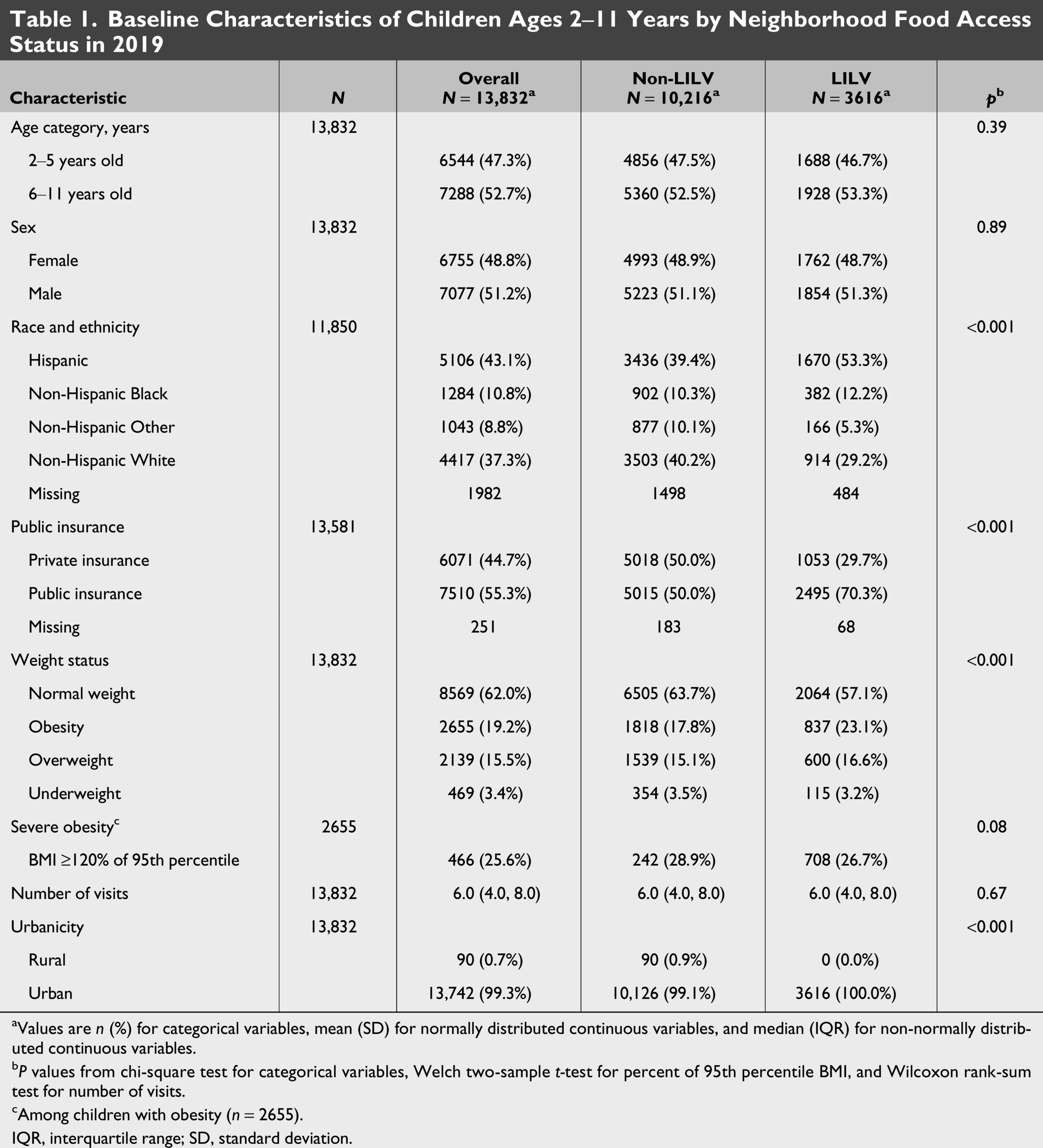
aValues are n (%) for categorical variables, mean (SD) for normally distributed continuous variables, and median (IQR) for non-normally distributed continuous variables.
bP values from chi-square test for categorical variables, Welch two-sample t-test for percent of 95th percentile BMI, and Wilcoxon rank-sum test for number of visits.
cAmong children with obesity (n = 2655).
IQR, interquartile range; SD, standard deviation.
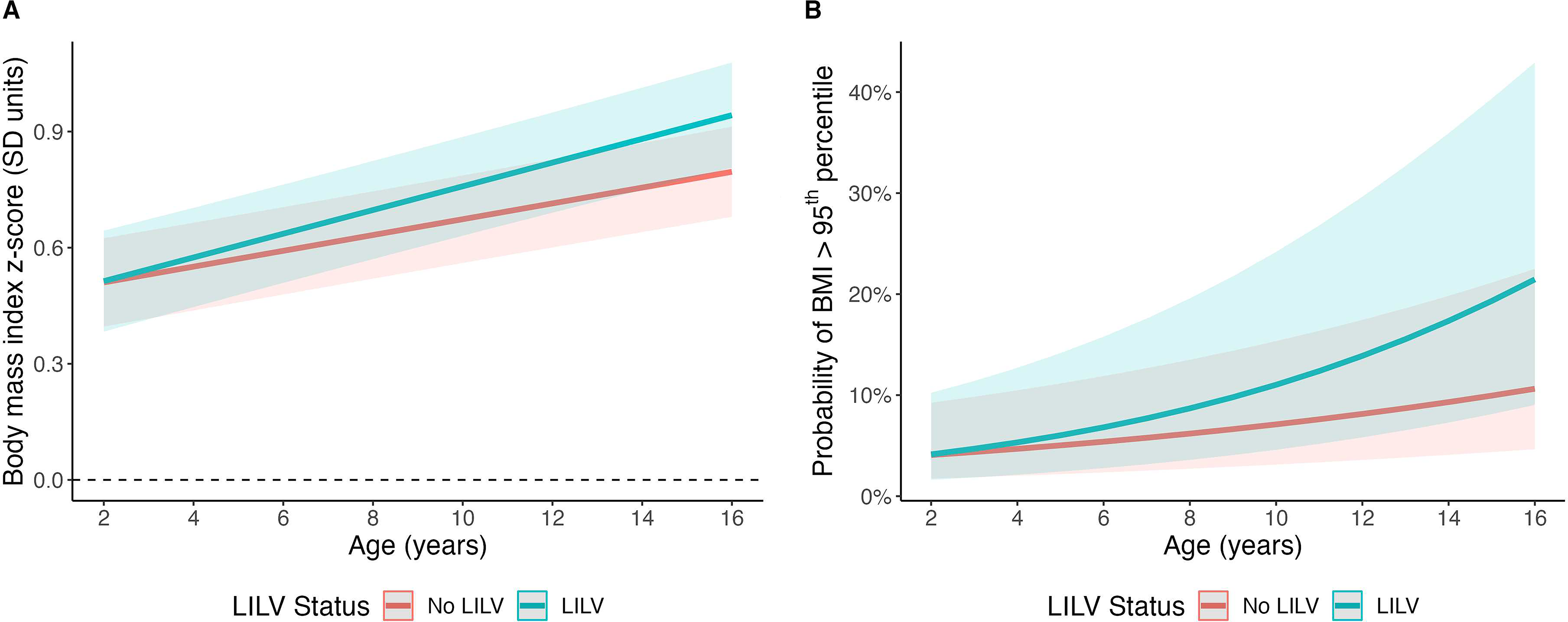
After adjusting for insurance type, residence in LILV neighborhoods at baseline was associated with higher mean BMI z-score and obesity probability trajectories over the 5-year follow-up period (Fig. 1). These differences widened progressively as children aged (Table 2). At age 5 years, there were no significant differences observed in BMI z-score [β = 0.03; 95% confidence interval (CI): −0.04, 0.11] or obesity risk [RR = 1.20; 95% CI: 0.76, 1.88]. By age 10 years, however, children who resided in LILV (vs. non-LILV) neighborhoods had higher mean BMI z-score [β = 0.08; 95% CI: 0.01, 0.16] and higher risk of obesity [RR = 1.55; 95% CI: 1.01, 2.39]. These estimates were stronger with higher mean BMI z-score [β = 0.14; 95% CI: 0.05, 0.22] and nearly double the risk of obesity [RR = 1.94; 95% CI: 1.17, 3.23] at age 15 years.
Secondary Analysis: Public Insurance Cohort
Among a subset of 3548 children with public insurance, LILV status, and household food insecurity data, 34.3% (n = 1044) resided in LILV neighborhoods, and 21.4% (n = 650) reported food insecurity. Our descriptive analysis showed that those experiencing household food insecurity had a higher baseline obesity prevalence (30.3% vs. 24.4%, p = 0.012) and were more likely to identify as Hispanic or non-Hispanic Black (Table 3). Notably, residence in LILV neighborhoods did not differ significantly between children who were food secure and those who were food insecure (p = 0.60). We did not observe significant associations between LILV neighborhood residence and weight trajectories in the public insurance cohort (Table 4). At age 5 years, the effect estimates were close to null [BMI z-score difference: −0.03, 95% CI: −0.15, 0.09; obesity RR: 1.03, 95% CI: 0.55, 1.94]. At ages 10 and 15 years, effect estimates suggested progressively higher BMI z-scores and obesity risk among children in LILV neighborhoods; however, CIs were wide and included the null value. Adjusting for household food insecurity did not meaningfully change these null estimates.
Baseline Characteristics of Children with Public Insurance by Household Food Security Status
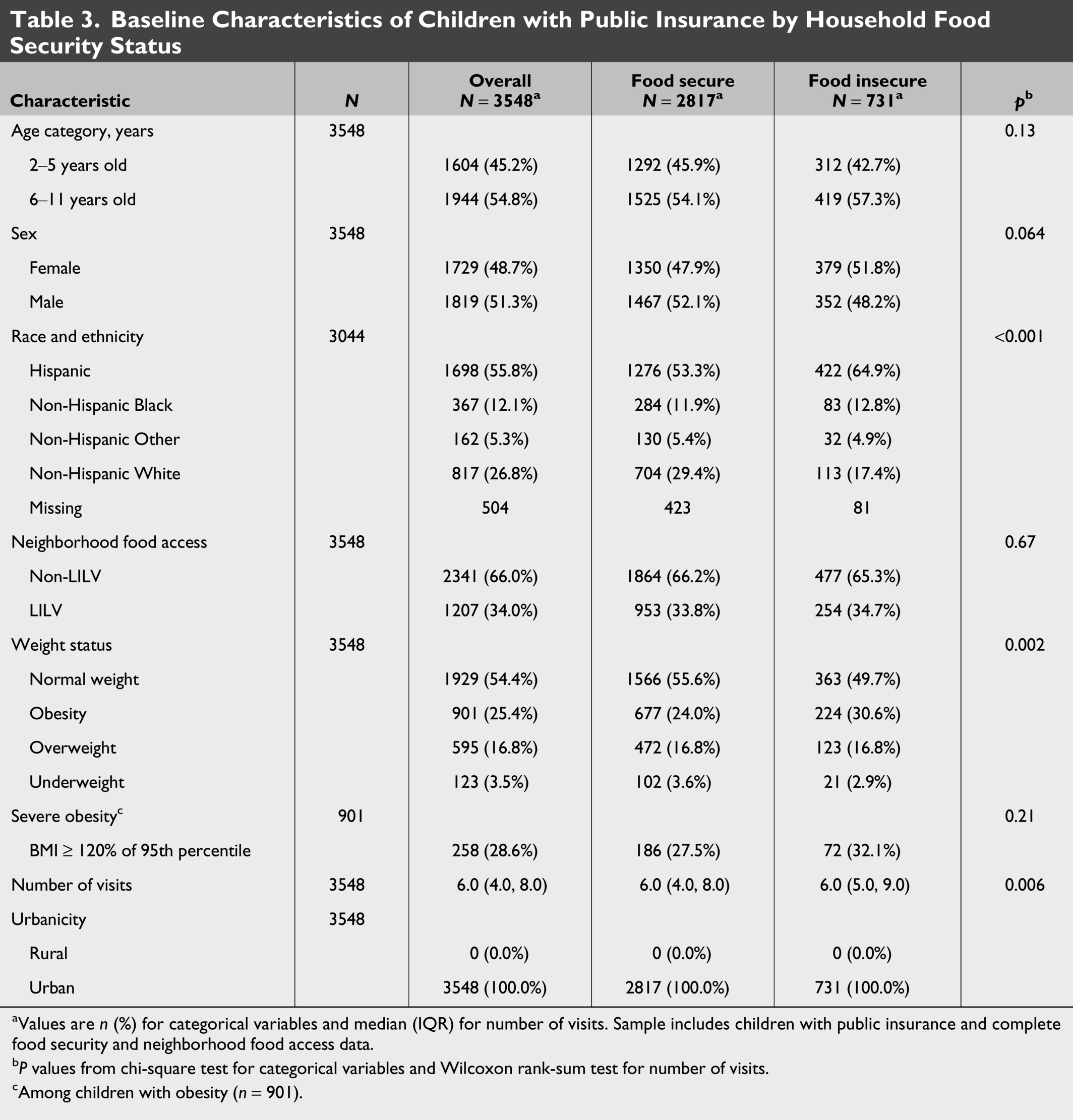
aValues are n (%) for categorical variables and median (IQR) for number of visits. Sample includes children with public insurance and complete food security and neighborhood food access data.
bP values from chi-square test for categorical variables and Wilcoxon rank-sum test for number of visits.
cAmong children with obesity (n = 901).
Association low-income, low-food access neighborhoods with low vehicle availability with BMI and Obesity in Children with Public Insurance
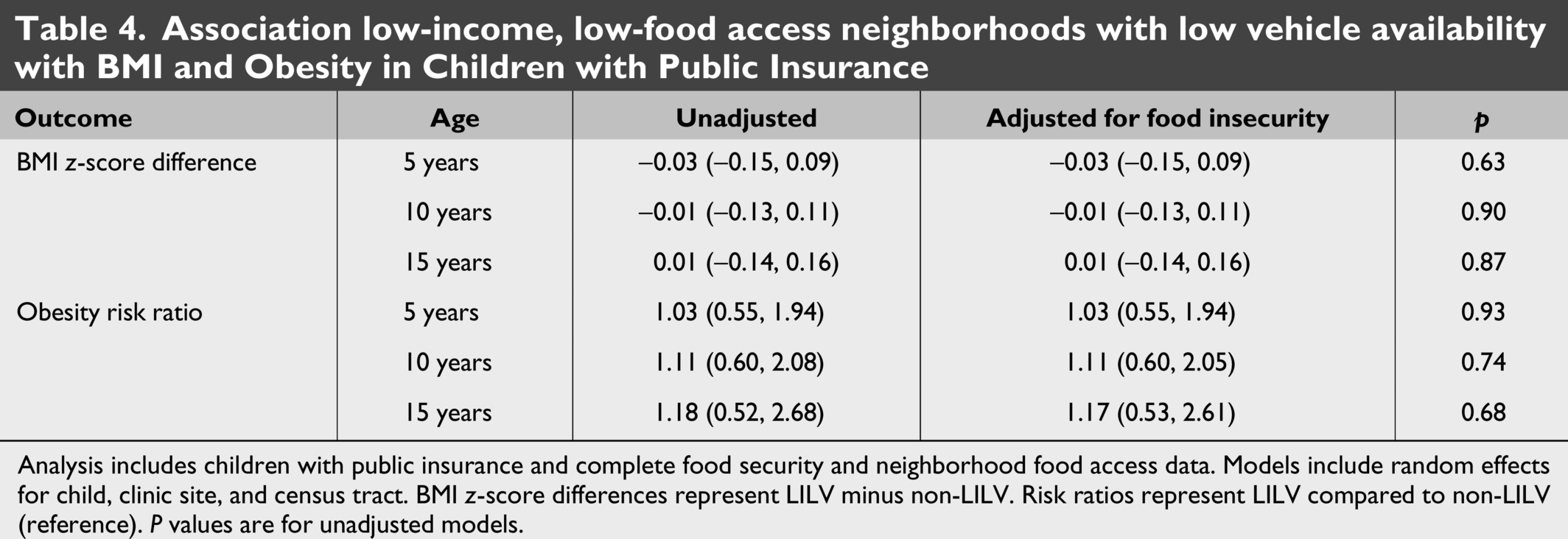
Analysis includes children with public insurance and complete food security and neighborhood food access data. Models include random effects for child, clinic site, and census tract. BMI z-score differences represent LILV minus non-LILV. Risk ratios represent LILV compared to non-LILV (reference). P values are for unadjusted models.
Supplemental analysis: Adjustment for Race and Ethnicity
In supplemental analyses (Supplementary Table S1), we examined whether adjustment for race and ethnicity altered the association between LILV neighborhood residence and weight trajectories in the full cohort (N = 13,832). After adjustment for both insurance type and race/ethnicity (Model 2), the associations remained largely consistent with the primary findings.
In our secondary analysis among children with public insurance (N = 3548), adjustment for race and ethnicity (Supplementary Table S2) similarly showed minimal impact on the effect estimates. At ages 5, 10, and 15 years, BMI z-score differences and obesity RRs remained nearly identical across the unadjusted (Model 1), race/ethnicity-adjusted (Model 2), and fully adjusted models including both race/ethnicity and food insecurity (Model 3).
Discussion
In this longitudinal cohort study of 13,832 children aged 2–11 years, residence in LILV neighborhoods at baseline was associated with elevated BMI z-scores and higher obesity risk at follow-up across childhood and adolescence compared to peers residing in non-LILV neighborhoods. Although no significant differences were observed at age 5, children residing in LILV neighborhoods demonstrated nearly double the obesity risk by age 15 years compared with their peers in non-LILV neighborhoods, independent of their insurance type.
Our findings are consistent with those of a nationwide study that observed associations between residence in low-income, low-food-access neighborhoods during early life and higher BMI z-scores and risk of obesity through adolescence. 22 However, our study focused on a fixed baseline period for children ages 2–11 years in 2019, whereas the prior study examined early life exposures during pregnancy and childhood. The widening of differences, from null effects at age 5 to nearly double the obesity risk at age 15 years, suggest there may be cumulative effects such as resource deprivation that compound over time.22,33 A longitudinal UK study observed that low-income children at age 5 already had higher obesity risk, and income inequalities widened by age 11 alongside higher risk of obesity and overweight, and a follow-up analysis showed the income inequalities associated with BMI and body fat disparities widened further by age 17.34,35
Our longitudinal study extends a predominantly cross-sectional literature on food access and childhood obesity. A systematic review of 24 studies [20 cross-sectional, primarily from North America and the United Kingdom] found that half showed an association between low neighborhood supermarket access and childhood obesity, whereas the rest found null or opposite associations. 18 These inconsistencies may reflect methodological differences and heterogeneity of the exposures measured. Our study addresses these limitations by using LILV status as characterized by the USDA, which captures multiple barriers of income constraints with transportation barriers and geographic distance and has policy-relevant implications. 26 In addition, we tracked weight trajectories over time within a socioeconomically diverse cohort within eastern Massachusetts between 2019 and 2024, which straddled the COVID-19 pandemic. We built upon prior work examining pandemic-associated rises in obesity prevalence,4,19,36 to describe the associations specifically between neighborhood food access and BMI trajectories during this period.
Our secondary, exploratory analysis among children with public insurance warrants cautious interpretation. Generalizability is limited by the smaller sample size (N = 3548) and by the residence of all Medicaid-insured children resided in urban neighborhoods in eastern Massachusetts. Although one in five children in this cohort had caregiver-reported household food insecurity, which is higher than national estimates, it is aligned with estimates of food insecurity in other pediatric Medicaid cohort populations of 19% in New York City, 37 and 27% across five major US cities. 38 The distribution of children residing in LILV neighborhoods did not differ significantly by household food security status (p = 0.60), suggesting that these measures represent different dimensions of food-related hardship. While both constructs of residence in LILV neighborhood and caregiver-reported household food insecurity are related to the food environment, they represent distinct ecological levels: One captures the structural food environment within the broader community context, whereas the other reflects the circumstances of the household or immediate family unit. 10 Structural barriers, including distance to retailers, transportation limitations, and neighborhood food offerings (e.g., perceived food swamps), may influence eating patterns through mechanisms distinct from a household’s ability to purchase healthy foods.39–41
Several mechanisms may underlie the strengthening associations observed across childhood. Limited proximity to healthy food retailers may constrain dietary quality by reducing access to fresh produce while increasing reliance on convenience stores and fast-food outlets. Healthier food environments associating with higher fruit and vegetable intake, whereas a greater density of fast-food and convenience outlets linking to unhealthy purchases, poorer diet quality, and higher BMI in youth.11,42,43 Widening disparities may reflect accumulating dietary exposures during critical developmental periods, as eating behaviors established in early childhood track over time and adolescence represents a key stage when eating habits become more established and teens gain more autonomy over food choices.42,44 Additionally, LILV neighborhoods often differ in other contextual features—more obesogenic food environments, fewer recreational facilities, higher neighborhood stressors, and more prevalent targeted promotion of unhealthy foods—all contributing to poorer diet quality, less physical activity, and higher odds of overweight and obesity in youth.43,45,46
Strengths of our study include a large and diverse cohort, longitudinal BMI measurements spanning 5 years, objective LILV assessment using USDA criteria, and examination of household food insecurity in a subset. Limitations include LILV measurement as a baseline contextual measure in 2019 rather than a time-varying exposure, selection bias as only children presenting to primary care were included, constraints of EHR analysis, and missingness of social factors data. We were unable to assess household food security in the overall cohort due to missing data. This study also did not explore how time-varying household food insecurity may relate to subsequent BMI; however, systematic and repeated measures of household food insecurity were not collected for the majority of the cohort, even among the publicly-insured population. We expect minimal residual confounding as we followed the exact cohort from 2019 to 2024. While beyond this study’s scope, future studies merit investigation of the complexity and temporal dynamics of the food environment (e.g., shifts in local food environments during the COVID-19 period) by considering repeated measures of household food insecurity and residential mobility in and out of LILV neighborhoods. Our study did not examine other aspects related to neighborhood food access, such as fast food availability, or access to safe outdoor physical activity or neighborhood green space, though future studies could be considered to explore these other potential mechanisms.
In conclusion, our study observed that childhood residence in LILV neighborhoods was associated with higher BMI trajectories and obesity risk over time. While clinical obesity prevention guidelines are forthcoming, the American Academy Clinical Practice Guidelines for Obesity Evaluation and Treatment include screening for food security and acknowledges increased access to food assistance resources are needed to mitigate the obesity risk factors faced by children living in under-resourced communities.47,48 Our findings highlight neighborhood food access as a potentially modifiable structural determinant of pediatric obesity inequities and support comprehensive strategies to improve the multilevel food environment, targeting both individual economic resources and neighborhood infrastructure, to promote childhood obesity prevention.
Authors’ Contributions
A.J.W. conceptualized and designed the study, carried out data analyses, drafted the initial article, and critically reviewed and revised the article. I.A. conceptualized and designed the study, coordinated and supervised data analysis, and critically reviewed and revised the article. M.L. carried out the data abstraction, data analyses, and critically reviewed and revised the article. T.-Y.L. drafted the initial article and critically reviewed and revised the article. M.E.P., L.F., and E.M.T. coordinated and supervised data abstraction and critically reviewed and revised the article. All authors approved the final article as submitted and agree to be accountable for all aspects of the work.
Ethical Considerations
The Mass General Brigham Institutional Review Board determined that this study met the criteria for exemption under 45 CFR 46.104(d). All procedures performed were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments.
Consent to Participate
The IRB determined that informed consent was not required for this exempt research.
Data Availability Statement
Deidentified individual participant data will not be made available.
Footnotes
Acknowledgments
The authors thank the Harvard Center for Geographic Analysis.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
Research reported in this publication was supported by the
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.