
Abstract
Despite the strong empirical evidence linking childhood abuse to negative mental health outcomes later in life, a number of questions remain regarding race variations in this association. Moreover, less is known about the salience of protective factors that can offset or ameliorate the negative effects of abuse on adult mental health, and whether these factors work differently by race. Using three waves of panel data from a nationally representative survey of American adults, the present study examined the long-term effects of childhood abuse on adult mental health over a span of 20 years. In addition, we assessed social support as a protective factor, and examined its differential effects on mental health outcomes for Whites and non-Whites. Results indicate that despite frequent childhood abuse, social support is associated with less depression for Whites—its positive effects being most pronounced for those with the most severe abuse experiences. However, social support is associated with worst depression for non-Whites—its negative effects being most pronounced for those with severe abuse experiences. These findings demonstrate that the factors commonly considered as protective and beneficial for adult victims of abuse work differently across racial groups and in fact, may be detrimental for non-Whites.
Keywords
Researchers in the social sciences must often navigate personal considerations as members of a society that is structured and organized in a manner that perpetuates social inequalities, whilst maintaining a level of scientific “objectivity” when empirically evaluating these same social disparities. In fact, as early as 1917, when discussing the role of the teacher in the social science classroom, the renowned economic sociologist Max Weber remarked as follows: politics is out of place in the lecture-room…. One can only demand of the teacher that he have the intellectual integrity to see that it is one thing to state facts….while it is another thing to answer questions of the value of culture…the prophet and the demagogue do not belong on the academic platform…whenever the man of science introduces his personal value judgment, a full understanding of the facts ceases. (Weber, 1946, p. 145)
More recently, critical race theorists like Patricia Hill Collins (2000) have shed light on the ways that knowledge accumulation under the guise of “science” in the American academy, cannot be fully understood without taking into account the racialized and sexist institutional practices that have long marginalized persons of color within the academy (Collins, 1986). Writers like Collins rightly point out the peripheral location of scholarship that addresses issues related to the exploitation, exclusion, and oppression of Black women in American society. As a sociologist, Collins is also able to show how, within higher educational structures, Black women’s intellectual voices are often stifled in the name of “scientific rigor.” Furthermore, intellectual achievements that are synthesized with social activism are devalued to the point of being seen as disconcerting; possibly dangerous. As Collins argues, “a good deal of U.S. black feminist thought must adhere to the disciplinary procedures of the academy. Elevating black feminist thought to the level of theory and devaluing black women’s activism as less theoretical are strategies that aim to contain them both. Moreover, such actions place U.S. black feminist thought in the academy under surveillance” (2000, p. 282). Such an institutional orientation is distressing on many levels but in an earlier work, Collins highlights the overall loss to intellectual inquiry occurring when voices that hold a distinct standpoint are ignored altogether. Sociologists might benefit greatly from serious consideration of the emerging, cross-disciplinary literature that I label black feminist thought, precisely because, for many Afro-American female intellectuals, “marginality” has been an excitement to creativity. As outsiders within, black feminist scholars may be one of many distinct groups of marginal intellectuals whose standpoints promise to enrich contemporary sociological discourse. Bringing this group—as well as others who share an outsider within status vis-a-vis sociology—into the center of analysis may reveal aspects of reality obscured by more orthodox approaches. (Collins, 1986, p. S15)
While explicitly answering these questions is outside the scope of this article, framing this study with these workplace tensions in mind allows the asking of questions about Results-Based Accountability (RBA) and its potential to provide a bridge between research and community engagement. RBA is often used in areas of community engagement, social service provision, and needs assessment research; yet the empirical application of RBA highlights the descriptive, univariate measurement of data-driven outcomes and it does this with less focus on factors more conducive to multivariate statistical techniques such as linear, logistic, and hierarchical regression. The authors hope to contribute to RBA-driven research and outcome reporting by presenting the results of complex statistical models that conceptually align with the RBA framework. Substantively, this research explores the long-term effects of childhood abuse on adult mental health outcomes. The researchers estimate the effects of social support in the relationship between childhood abuse and mental health by examining panel data that trace the life trajectories of a random sample of Americans. The study intentionally uses the RBA method by estimating a series of multivariate models that conceptualize social support as an intervention that “turns the curve.”
With this overall aim in mind, the remaining sections of the article will proceed as follows. The researchers first offer an overview of RBA and its previous application in published scholarly research. The researchers then discuss the growing body of work that explores childhood maltreatment and its effects on later life outcomes, and then provide several hypotheses informed by the RBA framework. The empirical component of the article discusses the data source, and provides descriptive information of the data, with an emphasis on operationalized focal measures of childhood abuse, mental health outcomes, and statistical controls. The authors next turn to the central results of their study, and present estimates from random-effects regression models predicting two dimensions of mental health in adulthood, namely, depression and anxiety. The article closes with a discussion of findings that presents the results within the broader context of RBA as a plausible framework for studies that use a quantitative multivariate approach. First, the researchers begin with an overview of RBA, its inception, and its widespread application in multiple settings.
Background
Developed by Mark Friedman, RBA is a framework and method used to achieve measurable outcomes. RBA can be particularly valuable when it is utilized by place-base, collective impact efforts, where multiple partners leverage their combined resources to promote greater advancement and impact (Friedman, 2005; Friedman & Handley, 2008; Keevers, Treleaven, Sykes, & Darcy, 2012). RBA works concurrently on two discrete but interconnected levels: (1) “whole population” level, focused on impacting people in a given locality; and (2) “program population” level, where stakeholders work together in a community partnership with a shared focus on delivering services that positively influence their clients.
RBA first delineates the desired end result and then works backward to identify how to achieve it. For whole populations, the result is a condition of well-being for all people in a locale. For program populations, the result is the outcome for a client—an anticipated change in their knowledge, skills, attitude, behavior, or circumstance. Central to RBA is a data-informed, decision-making process that is continuously recalibrated. Evidence gathered should allow for the evaluation of key interventions, later evaluated for their efficacy.
As part of this strategy, the expectation is that interventions have an impact that is measurable and influential for the communities served. As such, a key conceptual element of the RBA framework is the “turn the curve” concept, conceptualized by Friedman (2015) as a tool for examining or visualizing changes in trends over time. Because trends have a historical trajectory that spans from one point in time to another, it is possible to establish a baseline measure for outcomes. The role of interventions in shaping positive outcomes is captured as deviations from this baseline. The “RBA turn-the curve template” highlights six important steps: Choose the result and indicator. Assess the baseline and projected trajectory of the indicator. Explicate the story behind the indicator. Clarify the contributing factors that support progress and help turn the curve, and those factors that hinder progress. Identify partners that can help turn the curve and be included in solutions. Determine possible solutions that can help turn the curve. These should include a mix of evidence-based programs, no-cost/low-cost ideas, and off-the-wall concepts. What is the action plan? Determine propositions that will help turn the curve, as well as the implementation of these solutions and actions.
For these purposes, panel data allow the researchers to use retrospective reports of childhood abuse as the historical trajectory leading adult outcomes later in time and over the life span. The authors argue that the RBA framework can be used to asses social support as a potential buffer in the relationship between childhood abuse and adult depression and anxiety, and contend that abuse and mental health can be assessed along a “turn the curve” continuum.
Literature Review
The Long-Term Effects of Childhood Abuse
Childhood abuse is a major life trauma that has enduring effects on personal health over the life course. A life course approach to psychological well-being is useful in understanding the noxious effects of childhood abuse on adult health, which are argued to function both independently and cumulatively with other life experiences (Halfon & Hochstein, 2002).
Trajectories of psychological distress among victims of abuse indicate age-related increases, suggesting that psychological health declines into elderly years (Shaw & Krause, 2002). Much of the evidence points to strong links between childhood abuse and psychological and somatic symptoms such as depression, anxiety, posttraumatic stress disorder (Greenfield, 2010; Shaw & Krause, 2002), increased emotional distress (Gilbert et al., 2009; Springer, Sheridan, Kuo, & Carnes, 2003; Taylor, 2010), suicidal ideation, and substance abuse (Lloyd & Taylor, 2006; Lloyd & Turner, 2008; Schaeffer, Swenson, Tuerk, & Henggeler, 2013; Schafer & Ferraro, 2012). Research also notes strong links between childhood abuse and physical health issues in adulthood, noting increased risks for cancer (Morton, Schafer, & Ferraro, 2012), obesity (Greenfield & Marks, 2009), sleep disturbances, frequent headaches, respiratory problems (Barsky & Borus, 1999; Sharpe & Carson, 2001), chronic pain (Heim et al., 2009; Mock & Arai, 2011; Springer et al., 2003), and even physical disability (Currie & Widom, 2010; Springer, Sheridan, Kuo, & Carnes, 2007).
Childhood Abuse and Race/Ethnicity
A growing body of work explores the role of race and ethnic background in childhood experiences related to maltreatment and abuse. A study by Kim and Drake (2018) point to several important findings. First, results show that childhood maltreatment is linked to environmental poverty in all race/ethnic groups. As child poverty rates increase, total and type-specific rates of maltreatment increase for everyone. Interestingly, at similar poverty rates, White rates of maltreatment showed higher trends when compared to Blacks and Hispanics, who showed lower rates. The Black/White disproportionality in maltreatment may be largely driven by Black/White differences in poverty. Kim and Drake (2018) also noted evidence for the “Hispanic paradox,” where Hispanics had lower risks compared with Whites and Blacks with similar socioeconomic situations. Other studies have found that the prevalence of maltreatment was higher for Black boys than for White boys; however, there were no differences in the timing, type, severity, or the chronicity of the maltreatment (Lee et al., 2012). Regarding the racial/ethnic differences in the consequences of childhood maltreatment, research indicates that when controlling for socioeconomic status, childhood maltreatment significantly predicts depression and violence occurring in adolescence but does not predict outcomes in young adulthood (Lee et al., 2012). While race significantly predicted heavy drinking and violence in adolescence and adulthood, no significant maltreatment by race interaction was found (Lee et al., 2012).
Overall, little is known about childhood maltreatment for members of minority racial and ethnic groups. According to scholars, research should address the scant literature in future work with several things in mind (Kenny & McEachern, 2000). First, scholars should seek accuracy in defining groups to ensure that results are valid and replicable. Second, the levels of acculturation of victims and their families should be noted (O’Keefe, 1994). Third, scholars need to account for the geographical location of victims and families to track its relation to incidence and reactions to maltreatment. Fourth, scholars should explore how limited language or language barriers can influence disclosure and the reporting of abuse. In addition, as indicated by the abovementioned work, scholars should consider the socioeconomic status of victims to obtain information about its relationship to incidence, prevalence, and the effects of child maltreatment on victims.
Despite strong evidence indicating the deleterious effects of childhood abuse on several outcomes, these studies reflect several limitations. First, many early studies were based on clinical samples (Thompson, Kaslow, Lane, & Kingree, 2000), the results of which cannot be generalized to the population. A number of epidemiological studies document the link between childhood abuse and health outcomes using cross-sectional data, which cannot ascertain temporal ordering (Hyman, 2000; McCloskey, Figueredo, & Koss, 1995). Several longitudinal studies have examined long-term outcomes but have focused on adolescents and young adults from childhood abuse reports that likely comprise severe cases of abuse. This approach overestimates the effects of maltreatment and produces results that are not generalizable to the population. Finally, few studies have explored how victims can achieve resiliency (Bonanno, 2004; Cromer & Sachs-Ericsson, 2006; Pepin & Banyard, 2006), but most of this work considers personality or health behaviors as paths toward resiliency. Few studies offer insight into the role of social institutions and family involvement as protective factors that, in spite of risks, can help promote positive outcomes (Carver & Connor-Smith, 2010; Taylor, 2010).
Method
Data and Sample
Data come from the Midlife in the United States (MiDUS), a national longitudinal study of health and well-being. The MiDUS is a survey of a nationally representative sample of noninstitutionalized adults aged 25–74 living in the United States. The first data collection period (Wave I) took place in 1995, collecting data from 7,108 respondents. Wave II took place in 2004, collecting data from 4,963 of the original respondents. Finally, in 2015, data for Wave III were collected from 3,294 of the original participants. The analytical sample includes participants who responded to questionnaire items for key analytical measures at all three waves, yielding an effective sample size of n = 2,164.
Study Measures
Dependent variables
The authors use two dependent variables to capture distinct but related dimensions of adult mental health: depression and anxiety. Depression is a continuous measure ranging from 0 to 7 that tallies the total number of affirmative responses to yes/no questions. Respondents were asked: “During 2 weeks in the past 12 months, when you felt sad, blue, or depressed, did you…” (1) lose interest in most things, (2) feel more tired or low on energy, (3) lose your appetite, (4) have trouble falling asleep, (5) have more trouble concentrating than usual, (6) feel down on yourself, no good, or worthless, or (7) think a lot about death?
Anxiety is included as a continuous measure ranging from 0 to 10. Respondents were asked: “How often over the past 12 months were you…” (1) restless because of your worry, (2) keyed up, on edge, or had a lot of nervous energy, (3) irritable because of your worry, (4) had trouble falling asleep, (5) had trouble staying asleep because of your worry, (6) had trouble keeping your mind on what you were doing, (7) had trouble remembering things because of your worry, (8) low on energy, (9) tired easily because of your worry, or (10) had sore or aching muscles because of tension. Response categories range from 0 to 3, where 0 = never, 1 = less than half of days, 2 = half of days, and 3 = most days. The final measure used in analytical models tallied the total number of “most days” responses.
Independent variables
The authors include a mean index ranging from 0 to 3 that gauges retrospective childhood abuse using questions from the Conflicts Tactics Scale, which ask about the frequency of emotional abuse and physical abuse. The following question prompted respondents to first regard their mother, then their father: “During your childhood, how often did your [parent type] do any of these things to you”: (1) emotional abuse: (a) insulted you or swore at you, (b) sulked or refused to talk to you, (c) stomped out of the room, (d) did or said something to spite you, (e) threatened to hit you, and (f) smashed or kicked something in anger; (2) physical abuse and severe physical abuse: (g) pushed, grabbed, or shoved you, (h) slapped you, or (i) threw something at you, (j) kicked, bit, or hit you with a fist, (k) hit or tried to hit you with something, (l) beat you up, (m) choked you, or (n) burned or scalded you. Response categories range from 0 to 3, where 0 = never, 1 = rarely, 2 = sometimes, and 3 = often.
Social relationships are multidimensional and can be conceptualized in numerous ways. Some studies have assessed social relationships by considering number of social ties while others have used frequency of contact with individuals or groups. These approaches to social relationships emphasize the structural aspects of social networks (Berkman & Syme, 1979; Ertel, Glymour, & Berkman, 2008). However, network density and social contact are not synonymous with overall relationship quality. In fact, individuals may feel isolated and alone despite having many social ties, or on the contrary, perceive having very close connections and reliable support systems despite having one or two close relationships (George, Blazer, Hughes, & Fowler, 1989; Kiecolt-Glaser, Gouin, & Hantsoo, 2010; Lett et al., 2005; Lyyra & Heikkinen, 2006). Therefore, when it comes to assessing social relationships, individual perceptions of relationship quality may be a better marker than network density or frequency of social contact with others.
In line with this conceptualization, the authors use a measure of “affectual solidarity” to gauge levels of social support. Affectual solidarity is a measure defined by the principal investigators as part of original MiDUS data collection and refers to the amount of positive sentiments held about close social members and their overall support and reciprocity. The battery of items comprising affectual solidarity capture individual appraisals of support and strain from (1) family members, (2) friends, and (3) significant others. Together, these items strongly characterize many of the qualitative attributes of social relationships and social support. For this reason, and throughout the remaining analysis, the article will simplify the original terminology and refer to these combined measures as a form of “social support.”
The T2 (Wave II) measure of social support uses a 28-item mean index intended to gauge overall perceptions of one’s relations and interactions with family, friends, and spouse. The variables comprising this index ask about (1) support and (2) strain from these relationships. Questions for family support included: (a) Not including your spouse or partner, how much do members of your family really care about you? (b) How much do they understand the way you feel about things? (c) How much can you rely on them for help if you have a serious problem? and (d) How much can you open up to them if you need to talk about your worries? Questions for friend support included: (e) Not including spouse or partner, how much do your friends really care about you? (f) How much do they understand the way you feel about things? (g) How much can you rely on them for help if you have a serious problem? and (h) How much can you open up to them if you need to talk about your worries? Finally, questions for spouse support included: (i) How much does your spouse or partner really care about you? (j) How much does he/she understand the way you feel about things? (k) How much does he/she appreciate you? (l) How much do you rely on him/her for help if you have a serious problem? (m) How much can you open up to him/her to talk about worries? (n) How much can you relax and be yourself around him/her? All support items were scored on a 4-point Likert-type scale, where 0 = not at all, 1 = a little, 2 = some, and 3 = a lot, and were coded so that a higher number indicates more solidarity and support.
Additional questions examined strain from family, friends, and spouses. Questions for family strain included: (a) Not including spouse or partner, how often do members of family make too many demands on you? (b) How often do they criticize you? (c) How often do they let you down when you are counting on them? or (d) How often do they get on your nerves? Questions for friend strain included: (e) Not including spouse or partner, how often do your friends make too many demands on you? (f) How often do they criticize you? (g) How often do they let you down when you are counting on them? or (h) How often do they get on your nerves? Questions about spousal strain asked: (g) How often does your spouse or partner make too many demands on you? (h) How often does he/she argue with you? (i) How often does he/she make you feel tense? (j) How often does he/she criticize you? (k) How often does he/she let you down when you are counting on him/her? (l) How often does he/she get on your nerves? Strain items were scored on a 4-point Likert-type scale, where 0 = never, 1 = rarely, 2 = sometimes, and 3 = often, with higher scores indicating more solidarity and support.
Control variables
A series of controls are included in all analytical models. The first is a dummy comparing males (=1) to females (=0). Race dummies are included to compare Whites to African Americans, Hispanics, and racial Others. Marital status dummies compare married to never married, and to separated, divorced, or widowed individuals. Age, income, and education are included as continuous measures, gauging actual years or dollars. Employment is included as a dummy, comparing employed (=1) to unemployed (=0).
Analytical Strategy
The current study estimated a series of random-effects (RE) models 1 to address its central question regarding the impact of childhood abuse on adult mental health, and the role of social support in this relationship. These models allow the authors to assess how abuse exerts additional influence on outcomes of depression and anxiety. Multiplicative terms interacting childhood abuse with race and social support were included to assess combined effects.
After presenting descriptive statistics, the authors overview results from RE models assessing depression and anxiety outcomes. Tables 2 and 3 are organized as follows: Model 1, the full model, includes childhood abuse, social support, and covariates. Model 2 interacts childhood abuse and social support. Model 3 interacts childhood abuse with race, while Model 4 interacts race with social support. Finally, Model 5 adds a three-way interaction between childhood abuse, social support, and race to the full model.
Results
The researchers noted important characteristics from the descriptive data shown in Table 1. Mean levels of childhood abuse were relatively low, with the average respondent experiencing abuse between none of the time and rarely. Average levels of depression and anxiety were low and showed a modest decline over time, with the average respondent reporting a mean of 0.50 out of 7.00, and 0.10 out of 10.00 for anxiety. When it comes to social support, respondents report high levels, with a mean of 2.25 of 3.00.
Descriptives of Analytical Variables—MiDUS I, II, III.
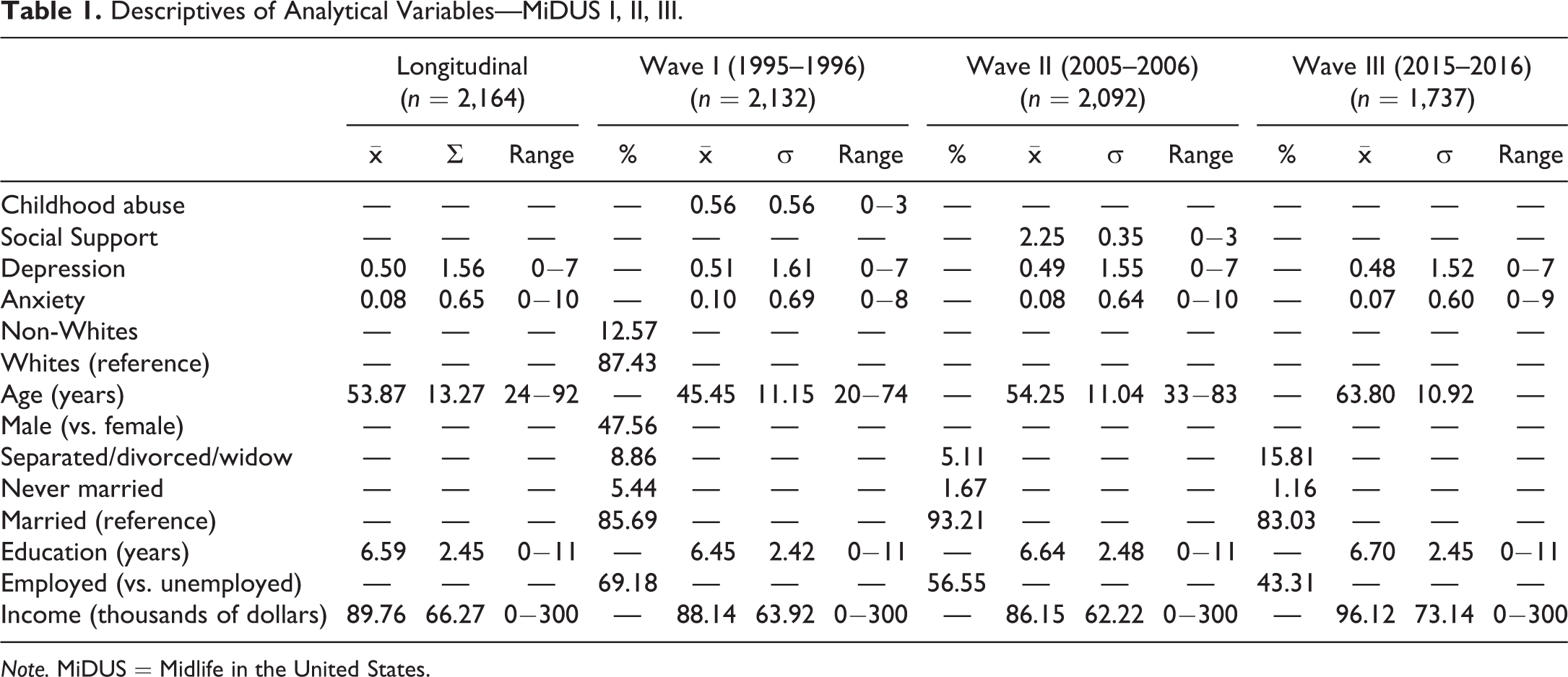
Note. MiDUS = Midlife in the United States.
Roughly 48% of respondents are men. In terms of race/ethnicity, Whites comprise the majority at 87%. The non-White group comprises 13% of the total sample, with 2.7% of these individuals being African Americans, 1.3% being Latinos, and 9% being all Others. The average level of education for respondents is equal to 3 years of college without a degree. Average income for respondents is moderate, averaging approximately US$89,760 per year.
Table 2 presents results of RE models predicting changes in adult depression over time, net of relevant controls. Results from Model 1, the full model, indicate that increases in abuse frequency are associated with increased depression (b = .23, p ≤ .001), while increases in support are associated with declines in depression (b = −.45, p ≤ .001).
Random-Effects Models Predicting Changes in Depression Over Time.

Note. n = 2,164.
*p ≤ .05. **p ≤ .01. ***p ≤ .001.
Model 2 adds the interaction term between childhood abuse and social support, with results indicating that the effects of social support on depression are greater for individuals who experienced more frequent childhood abuse. As seen in Figure 1, depression declines as support increases, with the most pronounced declines happening for the most frequent reports of childhood abuse among respondents (b = −.51, p ≤ .001). Models 3 and 4 each add separate interaction terms that interact childhood abuse and social support with race. Results indicate no statistically significant interaction effects in these models.
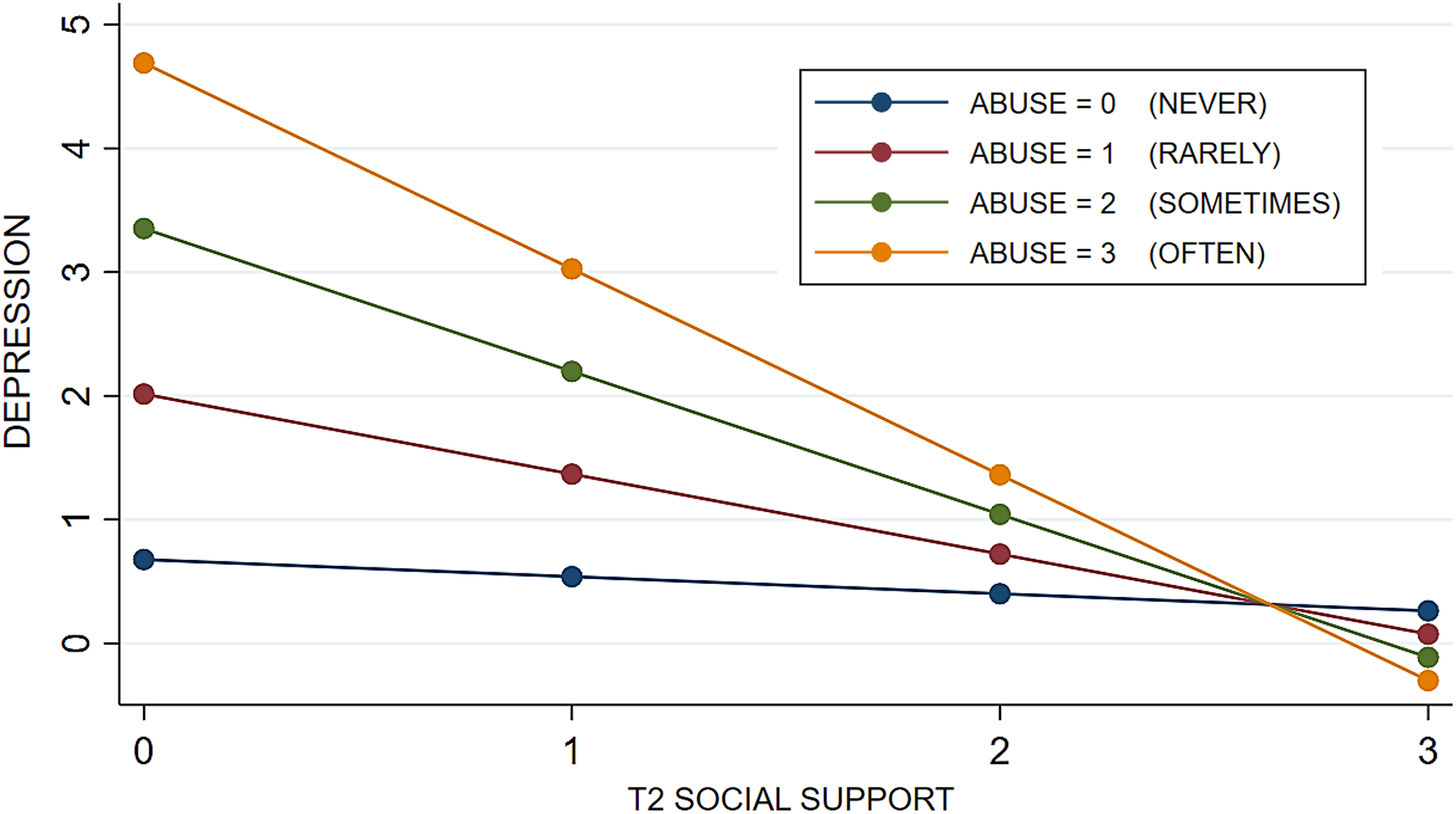
Childhood Abuse × T2 Social Support on change in depression over time.
Finally, Model 5 includes a three-way term, which interacts abuse, support, and race. Results, as reflected in Figure 2, indicate that support has very weak protective effects for non-Whites reporting more frequent abuse. In fact, increases in social support seem to have adverse effects for non-White victims who reported abuse occurring “sometimes” or “often,” with their depression levels slightly increasing over time. However, the same is not true for Whites who reported the same abuse experiences. Increased social support for Whites is associated with lower depression over time, and especially among those who reported more frequent abuse.
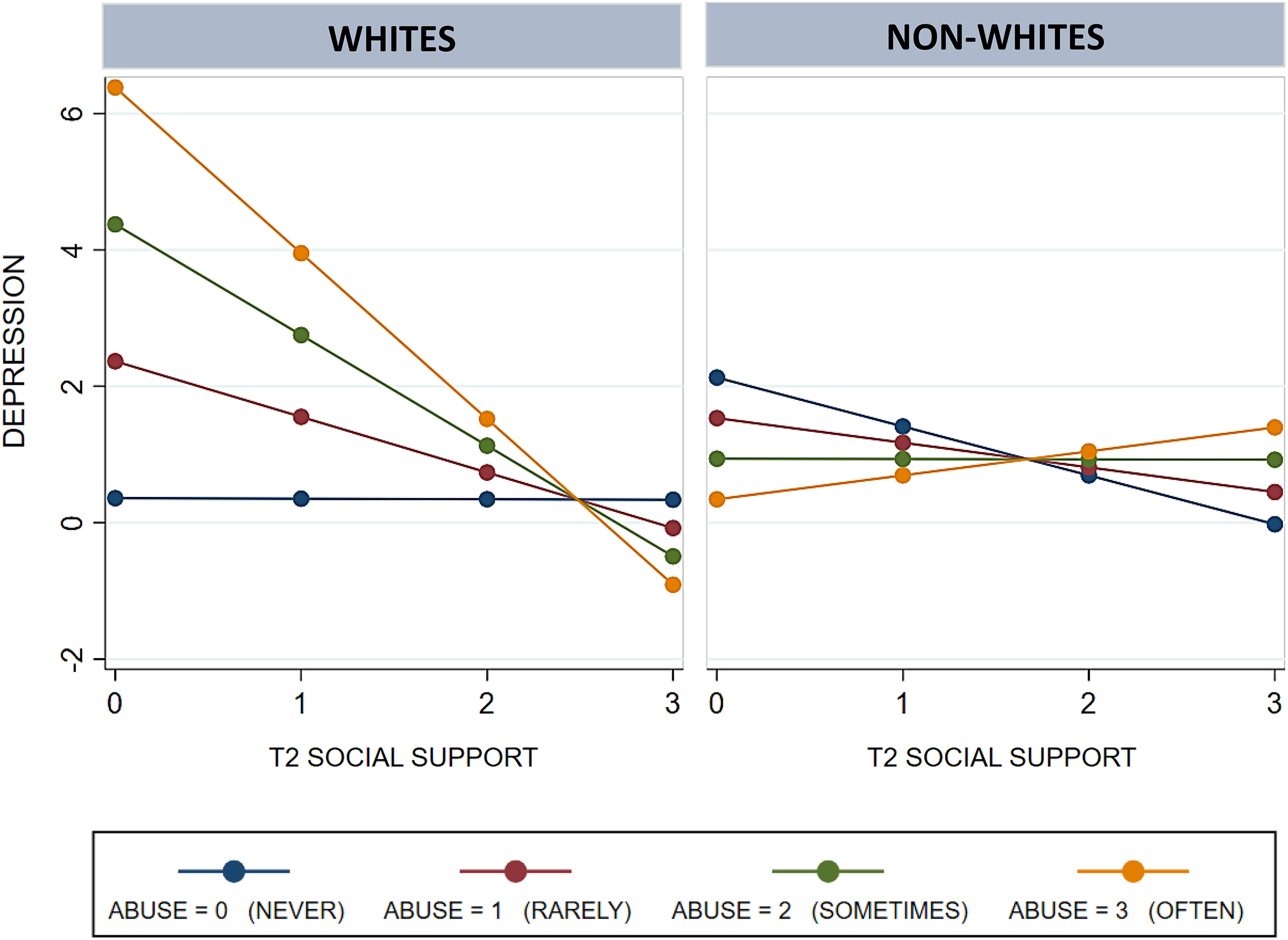
Childhood Abuse × T2 Social Support × Race on change in depression over time.
Some noteworthy effects of control variables from Table 2, Model 1 are as follows. When compared to women, men experience decreased levels of depression over their lifetime, net of childhood abuse, solidarity, and controls (b = −.33, p ≤ .001). Increases in age are associated with lower levels of depression over time (b = −.01, p ≤ .001). Finally, employed respondents have lower levels of depression over the life span when compared to those who are unemployed (b = −.17, p ≤ .001).
Table 3 presents results from RE models estimating change in anxiety over time. Results from Model 1, the full model, indicate that increases in childhood abuse are associated with increased anxiety over time (b = .08, p ≤ .001), while increases in social support at T2 are associated with declines in anxiety (b = −0.17, p ≤ .001). Model 2 adds an interaction between abuse and support, with results indicating that the buffering effects of support are strongest for individuals who reported more frequent abuse (b = −.25, p ≤ .001).
Random-Effects Models Predicting Changes in Anxiety Over Time.
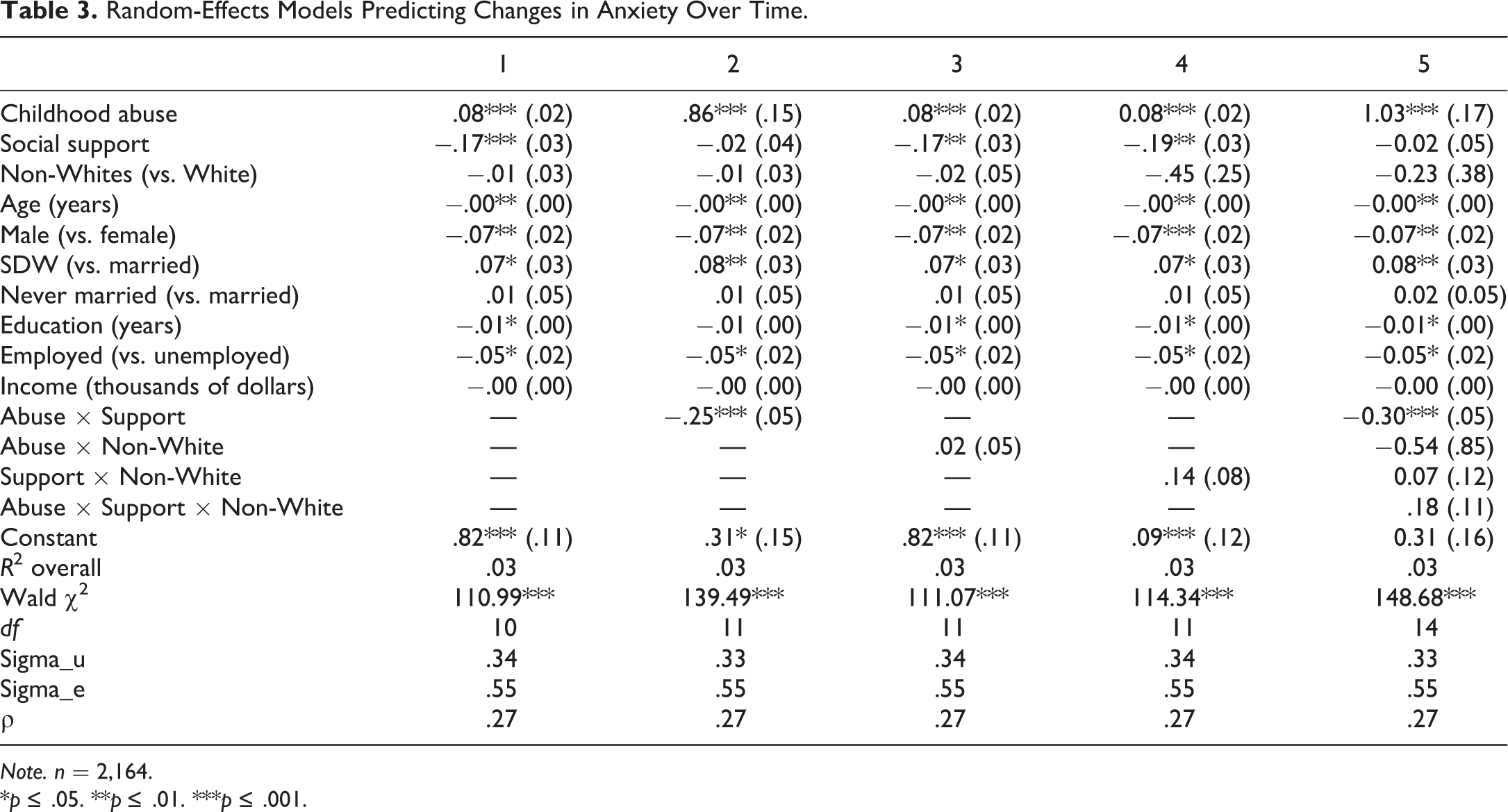
Note. n = 2,164.
*p ≤ .05. **p ≤ .01. ***p ≤ .001.
Figure 3 plots this interaction, indicating that more frequent abuse is associated with the highest levels of anxiety. However, as social support increases, anxiety drops substantially for high-frequency childhood abuse experiences. Models 3 and 4 interact abuse and support with race and indicate no statistically significant effects. Finally, Model 5 adds a three-way interaction between childhood abuse, social support, and race. Unlike results from the previous table, this interaction is not significant. However, the interaction between abuse and social support remains significant in this model, indicating its robust effects (b = −.30, p ≤ .001).

Childhood Abuse × T2 Social Support on change in anxiety over time.
Some noteworthy effects from Table 3, Model 1 controls are as follows. Compared to females, males show declines in anxiety over time, net of abuse, support, and controls (b = −.07, p ≤ .001). Higher levels of education are associated with lower levels of anxiety (b = −.01, p ≤ .05). In addition, when compared to unemployed individuals, those with employment have lower levels of anxiety (b = −.05, p ≤ .05).
Discussion and Conclusion
This article has attempted to apply RBA to the examination of panel data to produce estimates of multivariate statistical models. The researchers find that adult depression and anxiety are negatively impacted by early childhood abuse experiences, but that these negative effects are offset or ameliorated in the presence of social support systems. In other words, while the current research confirms previous studies indicating noxious effects of childhood trauma on later mental health outcomes in adulthood, the results here suggest that these outcomes are not fixed. The presence of social support was found to protect against the harmful effects of childhood abuse and improve adult anxiety and depression over time. However, not everyone benefits from social support.
Study results indicate that social support functions differently. While social support protects against the impact of childhood abuse on depression, this is true only for Whites. White respondents who reported frequent abuse showed declines in depression over time as social support increased. However, a nearly opposite pattern is found for non-Whites who experienced childhood abuse, whereby depression worsened as social support increased.
These findings are consistent with both empirical research and interpretive writings that underscore the multiple dimensions of race-based marginalization experienced by Americans on daily and long-term bases. Even with models accounting for the role of social economic background, the researchers find that resources ameliorate the negative effects of childhood abuse. However, for African Americans, the protective effects of social support are weaker than they are for Whites. Even in the presence of support systems, the experiences and microaggressions faced by African Americans serve to diminish and undermine the positive impact of support systems that, for Whites, protect against the effects of abuse on later mental health.
While the relationship between childhood abuse and poor mental health is positive, the net effects of social support for victims moderate the toxic impact of their childhood abuse experiences. The researchers suggest that the RBA framework is amenable to consideration of such individual-level effects when several features of the data are present. First, the data should contain a time element that allows for the examination of trends over time, or what Friedman calls, “the historical part of baselines” (Friedman, 2015, p. 58). Second, the analysis should include an intervention, often referred to as a “treatment” by social and experimental psychologists. This allows for the introduction of a turn the curve element, where trends can be examined as functions of interventions. Third, the topic addressed through the data should be of public concern and with specific policy implications. This allows empirical results based on RBA to be applied to policy initiatives and programming efforts specifically aimed at the populations coping with the condition or inequity under consideration. This discussion will place results within the context of the RBA method and propose avenues for the community-oriented emphasis of RBA to bridge with the more empiricist orientation of academic research.
The researchers take the position that RBA is capable of bringing strong value to the traditional ideas and approaches of “scientific” research. The principles of RBA emphasize the grounding of research directly on communities and explore change mechanisms that truly work in their communities. RBA argues that systems grounded on the “means” or real-life conditions can provide results with the potential for real-world/life implications. This shift in thinking moves scholarly research into community application and can place them on the path toward policy implementation and change. The researchers offer evidence for empirical methods using specific techniques for data analysis that account for spurious effects that can occur within different measures. In addition, when identifying underlying effects of measures, data collection and management established through the scientific method, systematic ethnography, and processes of interviewing can offer a level of empirical rigor.
The results present the effects of social support in situations where childhood abuse experiences are linked to poor mental health outcomes later in life. Applying the RBA framework allows for the consideration of community-based family support systems as buffers against the detrimental effects of childhood abuse. The authors encourage continual work in this area and welcome continued dialogue regarding ways to bridge scientific inquiry with community engagement and service provision.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.