
Abstract
This study aimed to determine the effects of the thermal blanket on patients’ vital signs, shivering level, chill status, and thermal comfort perception in preoperative and postoperative periods. The study was designed as a randomized controlled trial and included 44 female patients who had undergone elective gynecological surgery in a hospital in the south of Turkey. The experimental group (n = 22) was warmed using the passive warming method via a thermal blanket, and the control group (n = 22) was administered routine care via a cotton pique. The data collection tools included the “Patient Information Form,” the “Patient Follow-Up Form,” the “Shivering Level Diagnosis Form,” and the “Thermal Comfort Perception Scale.” Patients were warmed passively before (at least 10 minutes) and after surgery (at least 60 minutes) with a thermal blanket or cotton pique according to their groups. Patients’ vital signs and oxygen saturation were recorded during the preoperative and postoperative periods at 15-minute intervals. The patients’ shivering levels were recorded at 15-minute intervals, and chill status and thermal comfort perceptions were recorded at 30-minute intervals during the postoperative period. The data obtained in the research were analyzed using the SPSS 24.0 program. There were no statistically significant differences between the vital signs and oxygen saturation of the intervention and control groups during the first 60 minutes after surgery. The shivering level and coldness of the control group were higher in the postoperative period, but the difference between the groups was not statistically significant. There were no statistical differences between the groups in the time to reach 36.0°C (p > 0.05). Thermal comfort perception scores during the first 90 minutes were significantly higher in the intervention group (p < 0.05). The thermal blanket is not superior to the cotton pique used in standard care in maintaining body temperature, but it is effective in increasing thermal comfort perception.
Introduction
Inadvertent perioperative hypothermia (IPH) is defined as a drop in body temperature below 36°C occurring from 1 hour before anesthesia until the first 24 hours postoperatively (Akboğa, 2021; Russell et al., 2022; Soysal and İlçe, 2018). The incidence of IPH has been reported to range between 50% and 90% (Russell et al., 2022). In a study involving 2015 patients undergoing various surgical procedures under general anesthesia, the incidence of IPH was found to be 78.6% (Sari et al., 2021). IPH commonly arises due to heat redistribution, impaired thermoregulation, and exposure to a cold environment (Aldemir and Yilmaz, 2021; Simegn et al., 2021; Russell et al., 2022). Although hypothermia frequently occurs during anesthesia, its risk is influenced by both patient and procedure-related factors (Mendonça et al., 2019; Yan et al., 2021).
IPH is associated with various complications that increase morbidity and mortality throughout the perioperative period. It may result in cardiac abnormalities, impaired wound healing, a higher risk of surgical site infections, shivering, delayed postoperative recovery, increased intensive care unit (ICU) admissions, prolonged hospital stays, and coagulopathies (Chun et al., 2019; Keskin, 2021; Sari et al., 2021; Smith et al., 2020). Additionally, IPH contributes to elevated levels of postoperative nausea, pain intensity, anxiety, and decreased patient comfort (Ribeiro et al., 2021; Keskin, 2021). It also imposes a significant economic burden on both individuals and health care systems (Keskin, 2021). Therefore, preventing IPH is essential to ensure patient safety, enhance surgical outcomes, and improve overall patient satisfaction (Aldemir and Yilmaz, 2021).
Many professional organizations emphasize the importance of body temperature monitoring for the early detection of IPH and recommend evidence-based practices and temperature management strategies to maintain normothermia. The American Society of Anesthesiologists advises continuous temperature monitoring in all patients receiving anesthesia (ASA, 2020). The National Institute for Health and Care Excellence recommends assessing and recording body temperature before anesthesia induction and every 30 minutes intraoperatively, as well as initiating active warming at least 30 minutes before anesthesia (NICE, 2016). Similarly, the American Society of PeriAnesthesia Nurses recommends preoperative active warming and frequent temperature assessments throughout the perioperative period (Hooper et al., 2010; Link, 2020).
All perioperative team members share the responsibility of preventing IPH (Soysal and İlçe, 2018). Among them, perioperative nurses play a particularly critical role in assessing patients’ risk for hypothermia, developing individualized care plans, implementing appropriate warming strategies, and evaluating outcomes. Evidence-based nursing interventions should be applied at every stage of the perioperative care process to prevent hypothermia (Ribeiro et al., 2021; Yüksel and Uğraş, 2016). Nurses can significantly reduce heat loss through the use of active and/or passive warming methods (Keskin, 2021; Yüksel and Uğraş, 2016). Several studies have shown that active warming is more effective than passive warming and that preoperative warming is an effective strategy to prevent hypothermia (Connelly et al., 2017; Nieh & Su, 2016; Xu et al., 2019). However, high-quality studies are still needed to evaluate the clinical effectiveness of different passive warming materials and to compare the efficacy of various passive warming techniques (Soysal and İlçe, 2018). One such passive warming device is the Orve+wrap® thermal insulation blanket (About Orvewrap+, 2019), for which limited clinical evidence currently exists in the literature (Smith et al., 2020).
In this context, this study aimed to investigate the effects of the thermal blanket on patients’ vital signs, shivering levels, chill status, and thermal comfort perception during the preoperative and postoperative periods.
Methods
Study design
This was a randomized controlled trial.
Participants
The study was conducted in the operating room and gynecology clinic of a hospital in the south of Turkey between February and June 2021. The study population consisted of patients who underwent planned gynecological surgery. The study sample consisted of patients who met the inclusion criteria (Table 1).
Study Inclusion and Exclusion Criteria
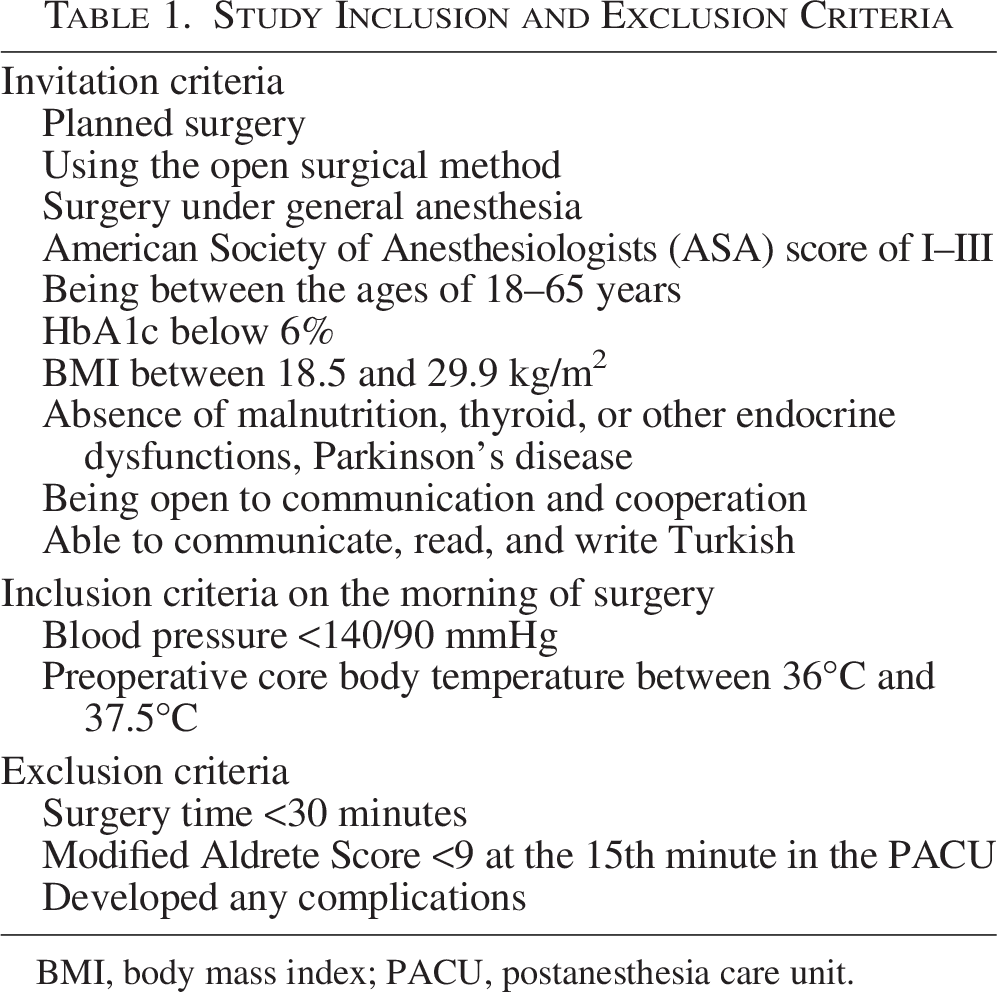
BMI, body mass index; PACU, postanesthesia care unit.
Of the 141 patients assessed for eligibility, 50 met the criteria and were included in the study. Six patients were excluded from follow-up due to canceled surgery (n = 2), withdrawal from the study (n = 1), development of complications (n = 1), ICU transfer (n = 1), and problem with the warming device (n = 1). The study was completed with a total of 44 patients (n1 = 22; n2 = 22). Patients were assigned to either the intervention or control group using block randomization. Computer-generated random numbers were used to create randomly permuted blocks. The study was conducted and reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) 2010 (Updated Guidelines for Reporting Parallel Group Randomized Trials) (Fig. 1).
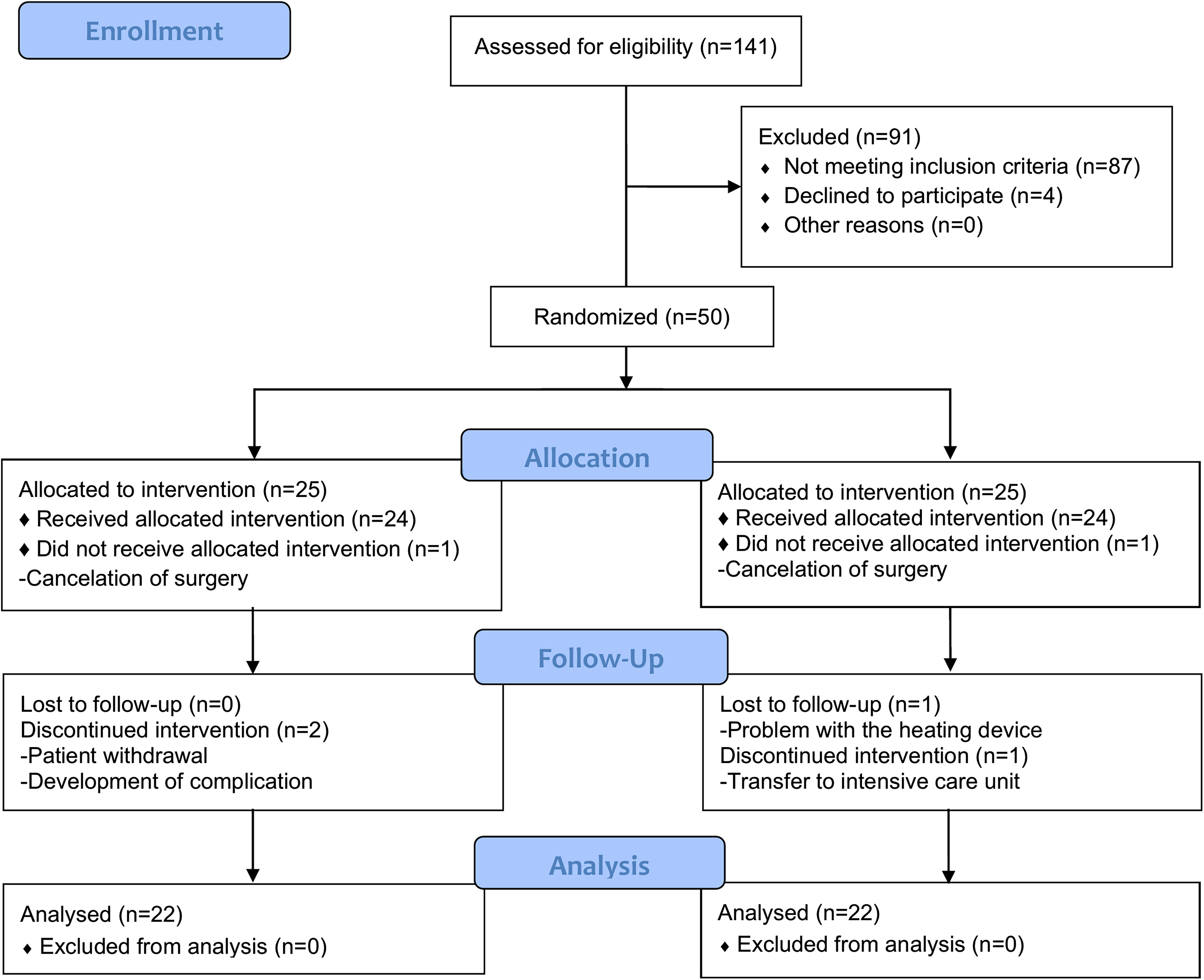
CONSORT diagram of patient recruitment.
Sample size
A preliminary study with 20 patients (10 per group) was conducted to calculate the sample size, as no similar data were available. Power analysis was used to determine the required sample size. Power analysis was performed using the variable “time to reach 36°C” to determine the sample size. Power analysis with G*Power 3.0.10 indicated that a total of 44 participants (n1 = 22; n2 = 22) would be sufficient with 80% power and a 5% margin of error (Faul et al., 2007). To account for potential dropouts, 50 patients were included (25 per group). Data from the preliminary patients were excluded.
Data collection
Data were collected through interviews, measurements, and medical records using the “Patient Information Form,” “Patient Follow-Up Form,” “Shivering Level Diagnosis Form,” and “Thermal Comfort Perception Scale.” Body temperature was measured with a tympanic thermometer; pulse and SpO2 with a pulse oximeter; blood pressure with a sphygmomanometer; and ambient temperature and humidity with a thermohygrometer. An Orve+wrap thermal insulation blanket (Orvecare) was used for passive warming.
Patient Information Form
This form consists of three sections addressing patients’ sociodemographic and disease characteristics, as well as the features of the surgical procedure.
Patient Follow-Up Form
This form is used to record patients’ vital signs, SpO2 levels, chill status, covering duration, and environmental humidity and temperature. Chill status was assessed by asking, “Are you cold?” Responses such as “very little,” “a bit,” “a little,” and “a lot” were recorded as “yes”; “not at all” and “no” were recorded as “no” based on self-report.
Shivering Level Diagnosis Form
It provides the evaluation of the shivering level of the patients through observation. The patients’ shivering level is 0: no shivering, 1: mild, localized shivering in the neck/chest region, 2: intermittent, moderate upper extremity shivering, 3: severe shivering in the trunk, lower, and upper extremities (Kim et al., 2014; Zaman et al., 2018).
Thermal Comfort Perception Scale
It is a visual analog scale used to assess thermal comfort perception. Patients rate their thermal comfort on a scale from 0 (extreme cold) to 10 (extreme heat), with a score of 5 indicating optimal thermal comfort (Duff et al., 2012; Akhtar et al., 2016).
Orve+wrap thermal insulation blanket (Orvecare)
It comprised a foil blanket in combination with a fleece lining. Under laboratory conditions, it has demonstrated the ability to absorb and retain heat, providing effective insulation. It is X-ray compatible, light, easy to store, latex-free, disposable, recyclable, suitable for use with diathermy and cautery treatments, can be cut when necessary, and has a six-layer laminated fabric blanket. It can be used on its own or preheated in a blanket warmer (Smith et al., 2020; About Orvewrap+, 2019).
Intervention and procedure
Stage 1 (clinic)
Patients’ sociodemographic and disease-related characteristics were recorded in the clinic on the morning of the surgery day. After putting on surgical gowns, vital signs and SpO2 levels were measured before transfer. All patients were covered (the intervention group with the thermal blanket and the control group with cotton pique) after being placed on the stretcher and taken to the preoperative waiting unit.
Stage 2 (preoperative waiting unit)
Patients remained covered in the preoperative waiting unit for at least 10 minutes. Their vital signs and SpO2 levels were recorded before transfer. After anesthesia induction in the operating room, the coverings were removed and placed in an 80°C heater. The covering duration was documented.
Stage 3 (end of surgery)
A single operating room was used throughout the study. At the end of the surgery, vital signs, SpO2 levels, and surgery-related data were recorded. Once consciousness was regained, control group patients were covered with a warmed pique, while intervention group patients were covered with a preheated thermal blanket and then transferred to the recovery unit.
Stage 4 (postanesthesia care unit)
The moment of arrival at the postanesthesia care unit (PACU) was recorded as postoperative 0th minute. Patients were monitored for 15 minutes, and their vital signs, SpO2 levels, and shivering levels were recorded at minutes 0 and 15. Those with a Modified Aldrete Score ≥9 were transferred to the clinic with their bodies covered.
Stage 5 (clinic)
All patients were followed in the clinic with their bodies covered for the first 60 minutes postoperatively. During this period, vital signs, SpO2 levels, and shivering levels were assessed every 15 minutes, while chill status and thermal comfort perception were evaluated every 30 minutes. After the 60th minute, follow-up continued for patients whose body temperature had not yet reached 36°C.
Ethical considerations
The study was carried out by Helsinki Declaration principles. Ethics committee approval was obtained from the Çukurova University Non-Interventional Clinical Research Ethics Committee (Date: March 6, 2020; Meeting No. 97). Institutional permission was obtained from the hospital where the study was conducted. After explaining the purpose, scope, and duration of the study to the patients and informing them that participation was voluntary and their personal information would be kept confidential, written informed consent was obtained.
Data analysis
The IBM Statistical Package for Social Science 24 was used for the statistical analysis of the data. Frequency tables and descriptive statistics were used to interpret the findings. Independent samples t-test and Mann–Whitney U test were used to compare measurement values between two independent groups. To examine the relationships between two categorical variables, cross-tabulation analyses were performed using Fisher’s exact test, continuity correction, and Pearson’s chi-square (χ2) test. The significance level was set at 0.05.
Results
The study was completed with a total of 44 patients (n1 = 22; n2 = 22). There were no statistically significant differences between the groups in terms of sociodemographic and disease characteristics or surgical procedure features (p > 0.05) (Table 2). The mean ambient temperature (°C) and humidity (%) in the clinic, operating room, and PACU were similar between the groups (p > 0.05). The time for body temperature to reach 36°C postoperatively was defined as “time to reach 36.0°C.” The mean duration was 71.59 ± 40.60 minutes in the intervention group and 79.77 ± 29.78 minutes in the control group, with no statistically significant difference between the groups (p > 0.05) (Table 3).
Comparison of Sociodemographic and Disease Characteristics of Patients and Features of Surgical Process

More than one answer was given to the question.
Others: Asthma, heart disease, arrhythmia, epilepsy, essential thrombocytosis, and cerebrovascular accident.
ASA, American Society of Anesthesiologists; BSO, bilateral salpingo-oophorectomy; IQR, interquartile range; IV, intravenous; TAH, total abdominal hysterectomy; USO, unilateral salpingo-oophorectomy.
Comparison of the Time to Reach 36.0°C
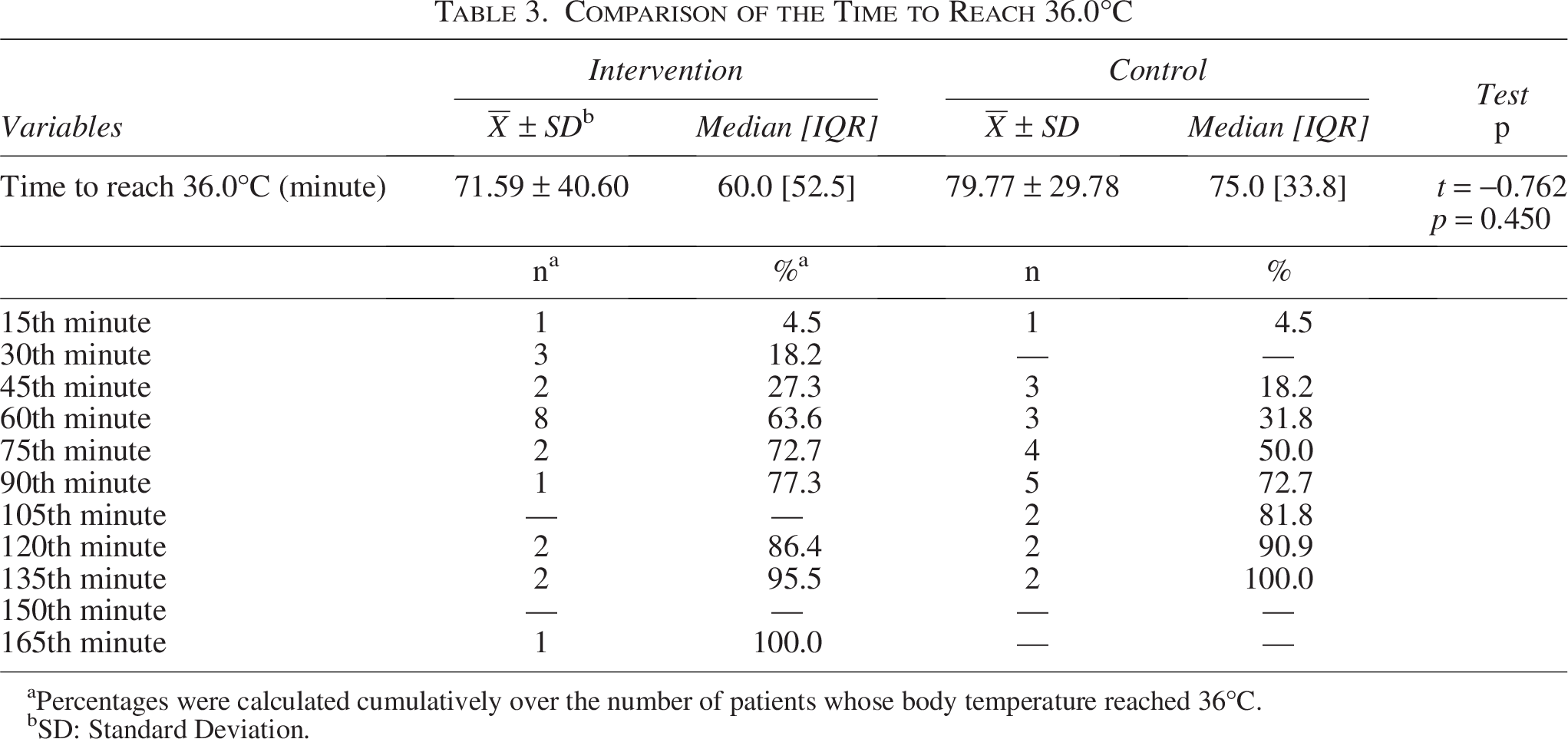
Percentages were calculated cumulatively over the number of patients whose body temperature reached 36°C.
SD: Standard Deviation.
Preoperative diastolic blood pressure and SpO2 levels measured in the clinic were significantly lower in the intervention group (t = −2.071, p = 0.046; Z = −2.778, p = 0.005, respectively). The mean respiratory rate at the 105th postoperative minute was significantly higher in the intervention group (t = −2.008, p = 0.036). At the 90th minute, the mean body temperature of the intervention group was lower than that of the control group (t = −2.315; p = 0.036). No significant differences were found between the groups in other periods regarding pulse, respiratory rate, blood pressure, or SpO2 levels (p > 0.05). At the end of the surgery, patients in both groups exhibited mild hypothermia (35–35.9°C), with no statistically significant difference in body temperature levels between the groups. Figure 2 illustrates the changes in body temperature over time in both the intervention and control groups.
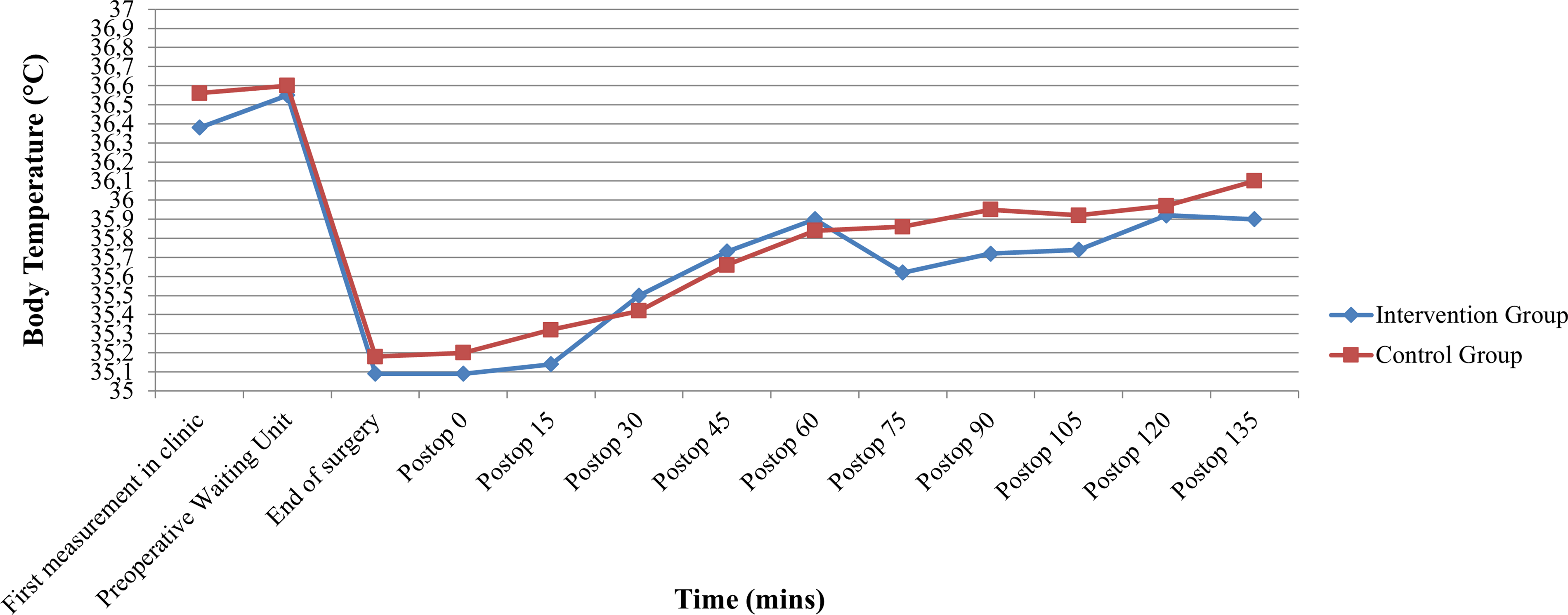
Changes in body temperature over time in intervention and control groups.
Upon arrival at the recovery unit, 82% of the intervention group and 63.6% of the control group had no shivering. At the 60th minute, all patients in the intervention group had no shivering, while 13.7% of the control group had mild shivering. Although shivering was more common in the control group at all postoperative time points, the difference was not statistically significant (p > 0.05) (Table 4).
Comparison of Patients’ Shivering Levels

Although chilling was more frequent in the control group throughout, the difference was not statistically significant (p > 0.05). At the 120th postoperative minute, no patients in either group exhibited shivering (Table 5).
Comparison of Patients’ Chill Status
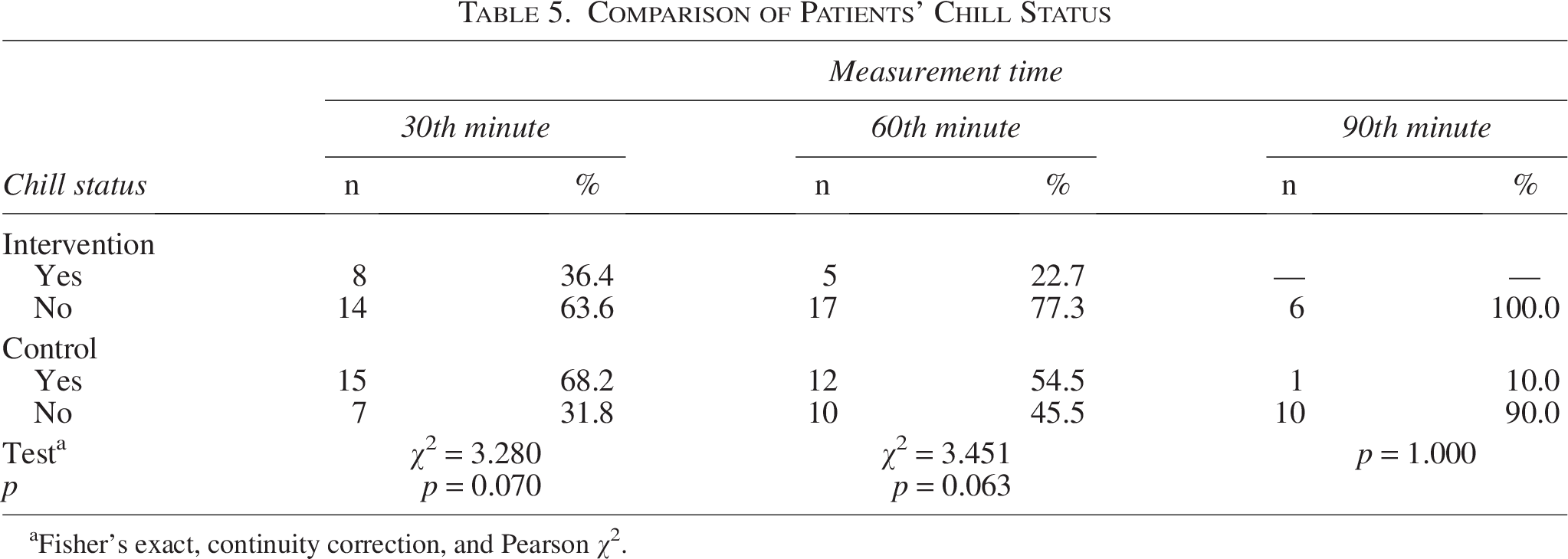
Fisher’s exact, continuity correction, and Pearson χ2.
A statistically significant difference was observed between the groups in mean thermal comfort perception scores at the 30th, 60th, and 90th minutes, with the intervention group reporting higher scores than the control group (p < 0.05) (Table 6).
Comparison of Patients’ Thermal Comfort Perception Score Averages

Bold values indicate statistically significant results (p < 0.05).
Since there are not enough data for the temperature comfort perception at the 150th minute, the analysis was not performed.
Patients whose body temperature was below 36°C.
SD: Standard Deviation.
Discussion
This study aimed to examine the effects of thermal blanket use on patients’ vital signs, shivering level, chill status, and thermal comfort perception in the preoperative and postoperative periods. No statistically significant differences were found between the intervention and control groups in terms of vital signs, SpO2 levels, shivering, chill status, or rewarming time during the first 60 minutes postoperatively. Thermal comfort perception scores during the first 90 minutes were significantly higher in the intervention group.
Studies report a high incidence of hypothermia, especially after major abdominal surgeries (Aksu et al., 2019). Similarly, this study found that nearly all patients experienced mild postoperative hypothermia. This may be attributed to the inclusion of patients undergoing major abdominal surgery under general anesthesia without intraoperative warming. The finding highlights that, despite advances in perioperative warming strategies, postoperative hypothermia remains common, underscoring the importance of effective temperature management.
In this study, there were no differences in mean vital signs and SpO2 values of the intervention and control groups in the preoperative and postoperative periods (first 60 minutes). The two passive warming methods seem to be similar in terms of maintaining and increasing patients’ body temperature, and the thermal blanket was not superior to cotton pique. In a study conducted to evaluate the effect of the additional use of a thermal reflective blanket on preventing hypothermia, the patients in the control group were brought to the operating room covered with two cotton blankets and actively heated during the surgery. On the contrary, the patients in the experimental group were additionally warmed with a thermal reflective blanket while being transported to the operating room and until they were taken to their beds in the clinic after surgery. It was determined that there was no significant difference between the groups in terms of the incidence of postoperative hypothermia (Koëter et al., 2013). In a study conducted to compare the thermal efficiency of heat-loss prevention of three methods (prewarmed cotton, reflective blanket, and forced-warm-air inflatable blankets), no significant differences were detected in temperature change among the groups (Cohen et al., 2002). In a study conducted with patients who had knee surgery, the reflective blanket was found to be less effective than using two cotton blankets (Ng et al., 2003). It was determined that thermal blankets were not more effective than warmed cotton blankets in preventing intraoperative hypothermia in patients undergoing intra-abdominal gynecological surgery (Whitney, 1990). Tjoakarfa et al. (2017) reported that, with adequate prewarming, reflective blankets were as effective as forced-air systems in maintaining intraoperative normothermia during hip and knee arthroplasty. Smith et al. (2020) compared thermal blankets with forced-air warming and found no significant difference in 60-minute postoperative body temperature. They suggested thermal blankets as a potential alternative.
This study found that patients in the intervention group reached 36.0°C more quickly; however, the difference between the groups was not statistically significant. A study involving patients who underwent hip and knee arthroplasty found that a reflective blanket was not more effective than a double cotton blanket in achieving a body temperature of 36.5°C in the recovery unit (Ng et al., 2003). Williams (2018) found no significant difference in recovery unit stay between the standard care group (cotton hospital gown, cotton fall prevention socks, and cotton bedsheet) and the passive warming group (thermal reflective cap and chemical hot pack on top of the arm in addition to standard practices). This finding aligns with the results of the present study.
This study found that although shivering and chill were less frequent in the intervention group across all assessment periods, the differences were not statistically significant. Another study using the same thermal blanket found no significant difference in postoperative shivering between the thermal blanket and forced-air warming groups (Smith et al., 2020). A study comparing passive (reflective blanket) and active (radiant) warming in patients who underwent major surgery reported no significant difference in shivering between the groups (Bredahl et al., 1995).
This study found that patients in the intervention group felt warmer and reported significantly higher thermal comfort perception scores during the 90-minute postoperative period compared with the control group. Patients who used reflective blankets during the preoperative and postoperative periods reported high thermal comfort and satisfaction, consistent with our findings (Palmer et al., 2019). Space blanket use reduced patients’ perception of cold during general anesthesia (Buggy and Hughes, 1994). A study on patients who underwent total hip and knee arthroplasty found that, unlike our study, thermal reflective blankets were not superior to standard care in thermal comfort (Koëter et al., 2013). These findings suggest that thermal reflective blankets have the potential to improve thermal comfort; however, their effectiveness may vary depending on the type of surgery and clinical setting.
Strengths and limitations
The randomized controlled trial design is a strength of the study. The limitations of the study include the inclusion of only women who underwent gynecological surgery, the inability to work with a fixed surgical team, and the limited number of studies using similar materials.
Conclusion
There were no statistically significant differences between the groups in achieving a postoperative body temperature of 36°C, preoperative and early postoperative (first 60 minutes) vital signs, SpO2 levels, shivering, or chill status. However, thermal comfort perception scores at the 30th, 60th, and 90th minutes were significantly higher in the intervention group. These findings indicate that hypothermia remains a common postoperative issue and that the thermal blanket is not superior to standard cotton pique in maintaining or increasing body temperature. However, it appears to be more effective in enhancing patients’ thermal comfort perception. Based on the study findings, it is recommended to use evidence-based practices throughout the perioperative period to prevent hypothermia. Additional covers may help improve thermal blanket contact with the patient’s body. Further research with larger and more diverse samples is needed to generalize the results and assess the role of gender. Moreover, as not all patients with hypothermia exhibit shivering or chill, health care providers should avoid relying solely on these signs to detect hypothermia.
Authors’ Contributions
İ.K.T.: Conceptualization, data curation, investigation, methodology, resources, visualization, and writing—original draft. E.N. and G.İ.Ç.: Conceptualization, project administration, methodology, resources, writing—review and editing, and supervision.
Footnotes
Author Disclosure Statement
The authors declare that they have no competing financial interests.
Funding Information
No funding was received for this article.
Acknowledgments
The Orve+wrap blankets were provided free of charge by the manufacturer, Orvec International Ltd. The company had no role in the design, conduct, analysis, or reporting of this study. Other instruments and materials used in the study were provided by the researchers.
Disclaimer
All authors have contributed significantly to the article and declare that the study is original and has not been submitted or published elsewhere.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki. Ethics committee approval was obtained from the Çukurova University Non-Interventional Clinical Research Ethics Committee (Date: March 6, 2020; Meeting No. 97). Institutional permission was obtained from the hospital where the study was conducted. Written informed consent was obtained from all participants.
Data Availability
The data sets used and/or analyzed during this study are available from the corresponding author upon reasonable request.