
Abstract
Out-of-hospital cardiac arrest (OHCA) in children is a rare but catastrophic event, often resulting in significant neurological injury. Targeted temperature management (TTM), including therapeutic hypothermia (TH), has been proposed as a neuroprotective strategy. This systematic review and meta-analysis aims to evaluate the effects of different TTM strategies on survival and neurological outcomes in pediatric patients after OHCA. A comprehensive literature search was conducted across PubMed, Scopus, Web of Science, Embase, and the Cochrane Library. Pooled outcomes were synthesized using odds ratios (OR) with 95% confidence intervals (CI), and the certainty of evidence was appraised using the Grading of Recommendations, Assessment, Development, and Evaluation approach. A total of nine studies encompassing 2107 pediatric patients were included. TH was associated with significantly higher odds of survival (OR: 1.72; 95% CI: 1.36–2.18; p < 0.0001) and favorable neurological outcome (OR: 1.64; 95% CI: 1.16–2.33; p = 0.006) compared to normothermia. Subgroup analysis demonstrated greater survival benefit at 12 months and improved neurological outcomes at 6–12 months. There were no statistically significant differences between groups in blood lactate levels, odds of arrhythmia, culture-proven infections, or length of hospital stay. The certainty of evidence for most outcomes was graded as low due to the predominance of nonrandomized studies and imprecision. TH as a TTM strategy following pediatric OHCA may offer survival and neurological advantage, particularly at longer-term follow-up, without a significant increase in adverse events. However, the low certainty of evidence highlights the need for further high-quality randomized trials to inform clinical practice and optimize neuroprotective care in this vulnerable population.
Introduction
Although relatively rare, out-of-hospital cardiac arrest (OHCA) in children is a devastating event with profound implications for patients, families, healthcare providers, and society at large. The global incidence of OHCA in children is estimated at approximately 8 cases per 100,000 individuals annually (Fink et al., 2016; Le Bastard et al., 2021); in contrast, the incidence among infants (<1 year) is substantially higher (Atkins et al., 2009; Herlitz et al., 2007; Rajan et al., 2015).
OHCA management necessitates high-quality medical care in both prehospital settings and after hospital admission. A common consequence of postcardiac arrest shock is profound neurological injury, which is the major contributor to poor prognosis and heightened mortality risk. These issues make it of particular concern during intensive care unit (ICU) management of pediatric OHCA survivors (Nikolovski et al., 2024). For this reason, developing neuroprotective strategies has become the primary concern for enhancing outcomes in pediatric patients after OHCA.
Targeted temperature management (TTM) is an intervention that includes both therapeutic hypothermia (TH) and the prevention of hyperthermia or targeted normothermia (Karnatovskaia et al., 2014). TH is recommended by international guidelines for OHCA in adults (Peberdy et al., 2010). However, in a trial by Nielsen et al., there was no significant difference in outcomes between TH with a target temperature of 33°C and maintained therapeutic normothermia at 36°C in adult patients (Nielsen et al., 2013). Nevertheless, substantial discrepancies exist in the etiologies, incidence, and outcomes of OHCA between adult and pediatric populations, limiting generalization of findings between age groups (Lee, 2020).
The use of TTM in pediatric populations has been addressed in several randomized controlled trials (RCTs) and observational studies; however, findings have been inconsistent. A study conducted in 2013 by Lin et al. reported that TH was associated with higher survival rates following pediatric resuscitation, highlighting the possible advantages of TTM in this population (Lin et al., 2013). A more recent study utilizing inverse probability of treatment weighting to adjust for confounders reported no statistically significant difference in favorable neurological outcomes between TTM and non-TTM groups (odds ratio [OR]: 1.36; 95% CI: 0.55–3.35) (Matsui et al., 2022).
Given these conflicting findings, it is necessary to conduct a comprehensive synthesis of the available evidence. Moreover, the variability in temperature targets, cooling durations, and outcome measures across existing studies underscores the need for a comprehensive and up-to-date systematic review and meta-analysis to guide evidence-based postresuscitation strategies in children. This systematic review and meta-analysis aims to evaluate the impact of different TTM strategies on survival and neurological outcomes in pediatric OHCA survivors.
Methods
Protocol and registration
This systematic review was conducted in accordance with the recommendations of the Cochrane Collaboration (Cochrane Handbook for Systematic Reviews of Interventions | Cochrane) and adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021). The protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO) [CRD420251108537].
Search strategy
A comprehensive review of articles was conducted from databases including PubMed, Scopus, Web of Science, Embase, and Cochrane Library databases. The search strategy incorporated both Medical Subject Headings (MeSH) terms and keyword variations for terms such as “out-of-hospital,” “cardiac arrest,” “pediatric,” and TTM strategies, including both normothermia and hypothermia. A full description of the search methodology and the search strategy for each database is provided in Supplementary Table S1. The reference lists of the articles included were manually screened to identify any additional eligible publications.
Eligibility criteria
Population
Included studies involved pediatric patients (<18 years old) who achieved return of spontaneous circulation (ROSC) after experiencing OHCA and were comatose following resuscitation efforts.
Interventions and comparators
The review evaluated studies that implemented TTM strategies post-ROSC, specifically normothermia (>35.1°C), and induced hypothermia (32–35°C) for durations of 24, 48, or 72 hours.
Outcomes
Outcomes being assessed included 30-day and 12-month survival rates, favorable neurological outcome at 1 month and 6–12 months, as defined by validated neurological scoring systems (Pediatric Cerebral Performance Category [PCPC] score), length of hospital stay, and incidence of adverse events such as arrhythmia and culture-proven infections.
Study design
Eligible study designs included RCTs, prospective and retrospective cohort studies, and other observational studies. We excluded case reports, narrative reviews, editorials, and expert opinions.
Screening
Two reviewers independently and blindly screened the studies using the predefined eligibility criteria. Discrepancies were addressed through discussion or by consulting a third independent reviewer. Title and abstract screening were conducted following duplicate removal. Potentially relevant studies underwent full-text screening to assess for final inclusion in the systematic review.
Data extraction and outcomes
Two independent reviewers extracted data from each eligible study using a standardized data extraction form. Any discrepancies were resolved through discussion or consultation with a third reviewer when necessary. Extracted data included study-level characteristics (first author, year of publication, country, study arms, study design), population characteristics (sample size, age, sex distribution), intervention details (TTM protocols, including target temperature, method of cooling, and duration), control conditions (normothermia or noninduced hypothermia), and clinical variables (underlying comorbidities, OHCA etiology, and cardiopulmonary resuscitation [CPR] duration). Primary outcome measures included survival rates at 30 days and at 6–12 months, and favorable neurological outcomes at one month and at 6–12 months. Outcome data were extracted separately for the TTM and control groups. These were collated in structured data tables under two domains: (1) survival rate and (2) good neurological outcome. Other outcomes assessed included blood lactate levels, odds of arrhythmia, culture-proven infections, and length of hospital stay.
Quality assessment
Quality assessment for all included studies was performed independently by two reviewers using the ROBINS-I tool (Risk Of Bias In Non-randomized Studies–of Interventions) for evaluating observational studies (Sterne et al., 2016). ROBINS-I assesses bias across seven domains, including confounding, participant selection, classification of interventions, deviations from intended interventions, missing data, outcome measurement, and selection of the reported result. For randomized trials, the Revised Cochrane Risk of Bias Tool for Randomized Trials (RoB 2) (Sterne et al., 2019) was used, evaluating bias across five domains: randomization process, deviations from intended interventions, missing outcome data, measurement of outcomes, and selection of reported results. Each study’s overall risk of bias was categorized as low, some concerns, or high risk. A consultation with a third reviewer was undertaken to resolve any conflicts (M.A.). This approach has been used in a previous study (Rath et al., 2025).
Certainty of evidence
The Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) tool was employed by two independent authors (M.A. and S.R.) using the GRADEpro Guideline Development Tool (Antesso et al., 2016) to evaluate the level of certainty of the evidence in this meta-analysis, with categorizations ranging from high to very low (Shao et al., 2023). Any disagreements were discussed and resolved through consensus. This approach has been used in a previous study (Rath and Alam, 2025).
Statistical analysis
Statistical analysis was performed using RevMan 5.4 software. For dichotomous outcomes, OR with 95% confidence intervals (CI) were calculated. For continuous outcomes, mean differences (MD) with 95% CI were computed. A random-effects model was utilized to account for variability among studies wherever heterogeneity was significant (I2 > 50%; p < 0.10), while a fixed-effects model was used when pooled analysis was homogenous (I2 < 50%; p > 0.10). Heterogeneity was assessed using the I2 statistic, with values of 25%, 50%, and 75% representing low, moderate, and high heterogeneity, respectively. Subgroup analyses were conducted based on the time of measurement of the outcome. Sensitivity analyses were performed by leave-one-out analysis. Statistical significance was defined at p < 0.05.
Results
Screening and study selection
An initial search yielded 2233 records, following which 1583 records were screened after duplicate removal. Following exclusion of 1561 records after an initial title and abstract screening, 22 records were assessed using a full-text screening. Finally, nine records were included for qualitative and quantitative synthesis (Kadden et al., 2024; Lin et al., 2013; 2019; Matsui et al., 2022; Moler et al., 2016; Prajongkit et al., 2019; Moler et al., 2015; Chang et al., 2016; Silverstein et al., 2016) (Fig. 1).
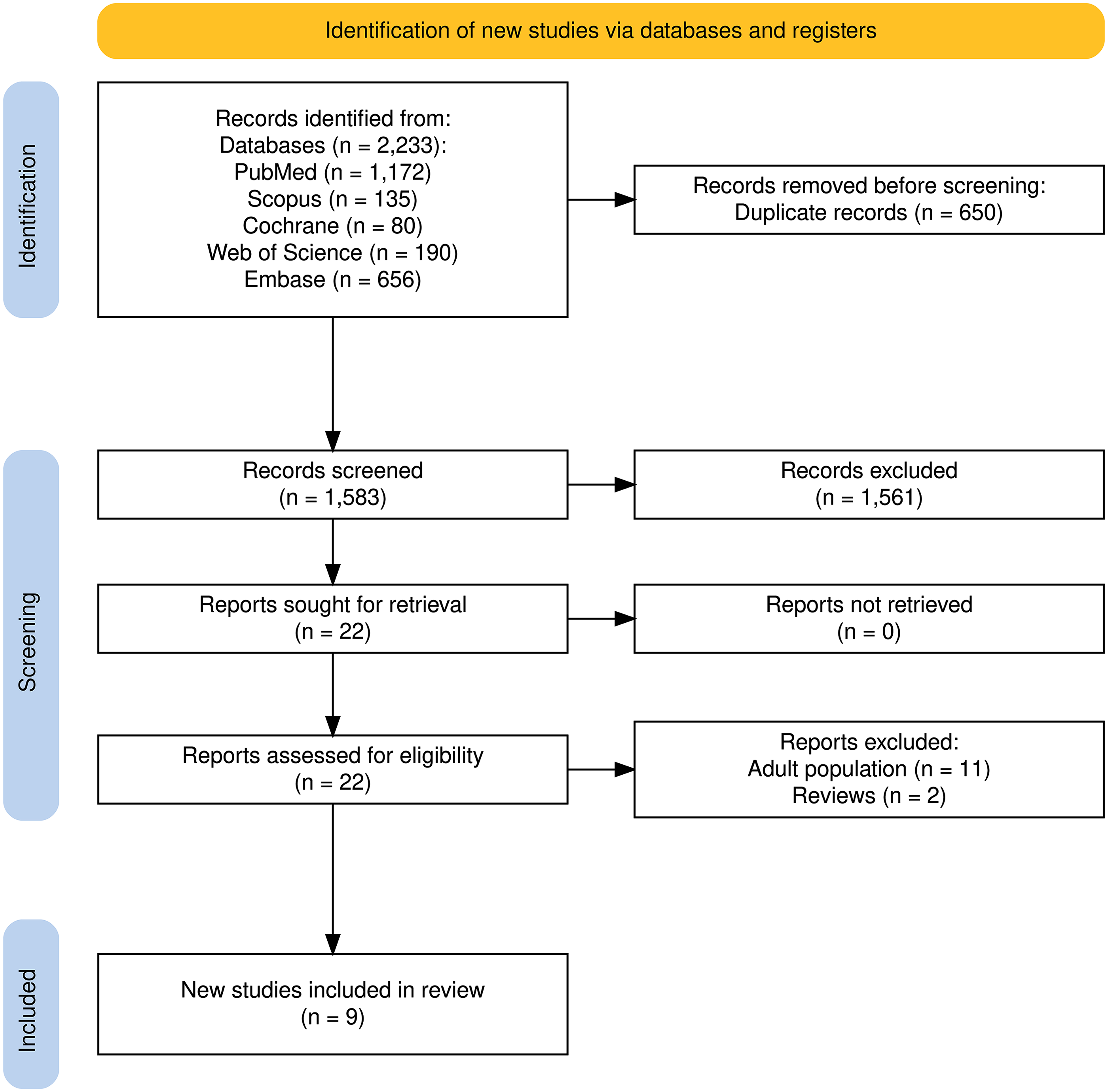
PRISMA flowchart of screening and study inclusion. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Baseline characteristics of included studies
A total of nine studies with 2107 patients were included for further analysis. The included studies primarily consisted of retrospective cohort designs, with two randomized trials conducted by Moler et al. (2015) and Silverstein et al. (2016). Sample sizes varied considerably, ranging from as few as six participants in the intervention group to nearly 600 controls in some cohorts. TH temperatures targeted were generally between 32°C and 37°C, with most studies aiming for around 33°C. The study populations were predominantly pediatric, with mean ages ranging from approximately 1–14 years, and females constituted between 29% and 69% of participants were reported. Health status reporting was variable; several studies noted a significant proportion of patients with lung or airway disease, although many studies did not report this characteristic. Regarding event circumstances, the proportion of witnessed cardiac arrest events ranged widely, with some studies reporting up to 90% witnessed status. Rates of bystander CPR also varied, from as low as 1.4% in some control groups to as high as 67.5% in others. Shockable rhythms were relatively uncommon across cohorts, generally observed in fewer than 25% of cases. It is important to note that several studies had missing data for key baseline characteristics such as witnessed status, bystander CPR, and initial rhythm, limiting comprehensive comparison across all cohorts. Detailed assessment is presented in Supplementary Table S2.
Quality assessment
Seven included studies were assessed by ROBINS-I. All studies were graded as having “Moderate” risk of bias, due to biases in confounding and measurement of outcomes. Two included studies were assessed using RoB2 and were graded as having “Some concerns” due to biases in confounding. Detailed assessment is presented in Supplementary Figures S1–S4.
Certainty assessment
The certainty of evidence for the outcomes comparing TTM with normothermia in pediatric OHCA was variable across endpoints. For survival and good neurological outcomes, both assessed from nonrandomized studies, the evidence was rated as low certainty, though findings suggested a potential benefit with TTM (OR: 1.72 and 1.64, respectively). Similarly, outcomes such as blood lactate levels and length of hospital stay, also derived from nonrandomized studies, were graded as low certainty due to imprecision, with wide CI and uncertain clinical impact. In contrast, high-certainty evidence from RCTs indicated no significant differences between TTM and normothermia in the risk of arrhythmia (OR: 1.02) or culture-proven infections (OR: 1.67), though estimates were imprecise and compatible with both benefit and harm. Overall, while some outcomes suggest potential advantages with TTM, the quality of evidence remains low for most clinically important endpoints, warranting cautious interpretation (Table 1).
Grading of Recommendations, Assessment, Development, and Evaluation Assessment Table
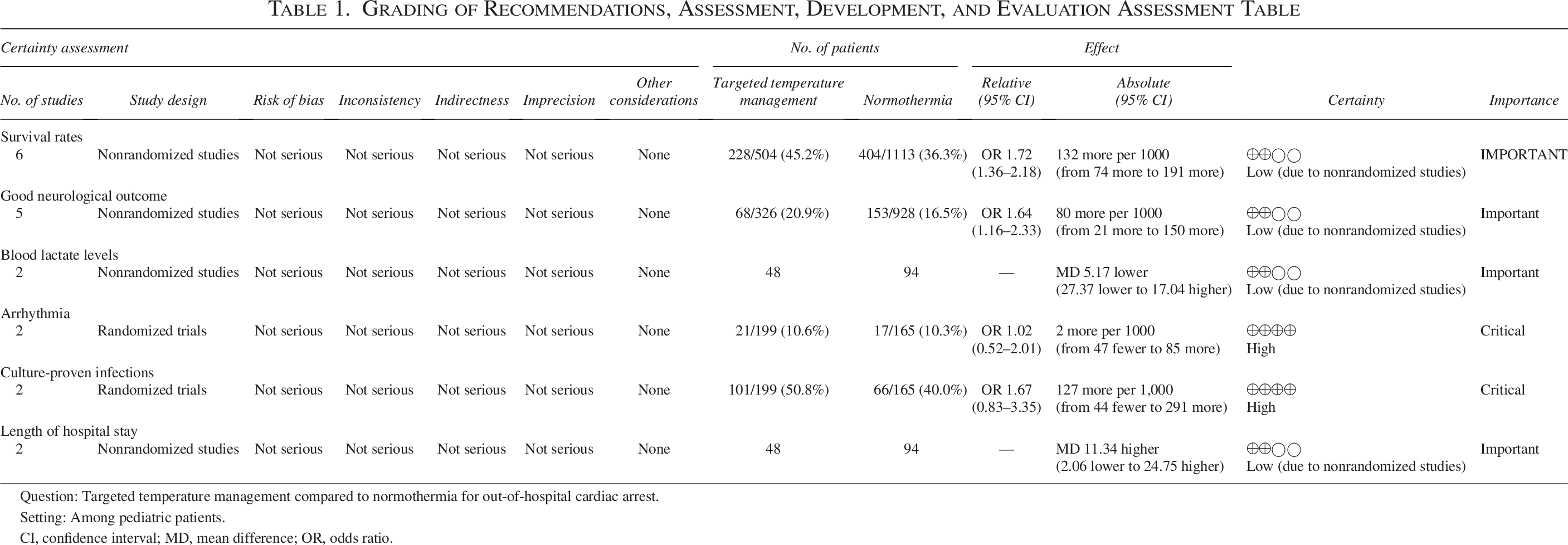
Question: Targeted temperature management compared to normothermia for out-of-hospital cardiac arrest.
Setting: Among pediatric patients.
CI, confidence interval; MD, mean difference; OR, odds ratio.
Outcomes
Survival rates
Pooled analysis of six studies revealed significantly higher survival odds in the TH arm (OR: 1.72; 95% CI: 1.36, 2.18; p < 0.0001). Pooled estimate demonstrated mild heterogeneity (I2 = 28%, p = 0.22). Subgroup analysis based on survival at 30th day or 12 months revealed significantly higher odds of survival at 12 months (OR: 1.86; 95% CI: 1.21, 2.85; p = 0.004), and at 30 days (OR: 1.66; 95% CI: 1.26, 2.20; p = 0.0004) (Fig. 2A).
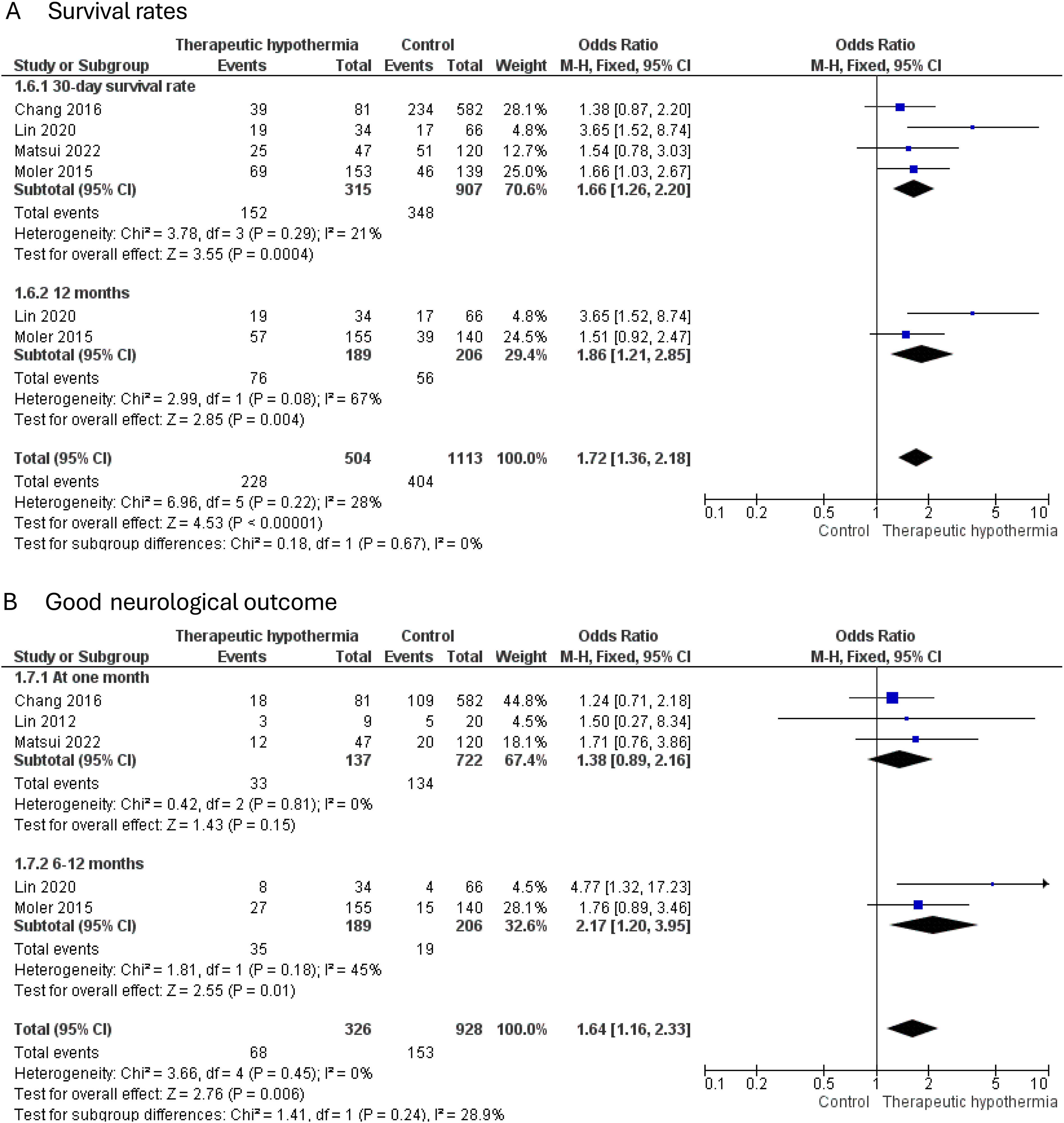
Forest plot of primary outcomes:
Good neurological outcome (defined as PCPC scale <2)
Pooled analysis of five studies with 326 patients revealed significantly higher odds of good neurological outcome in the TH arm (OR: 1.64; 95% CI: 1.16, 2.33; p = 0.006), with homogenous estimate (I2 = 0%). Following subgroup analysis, better neurological outcomes were noted at 6–12 months (OR: 2.17; 95% CI: 1.20, 3.95; p = 0.01) than at 1 month (OR: 1.38; 95% CI: 0.89, 2.16; p = 0.15) (Fig. 2B).
Blood lactate levels
Pooled analysis of two studies with 48 patients revealed similar lactate levels across both intervention and control arms (MD: −5.17; 95% CI: −27.37, 17.04; p = 0.65), with homogenous estimate (I2 = 0%) (Fig. 3A).
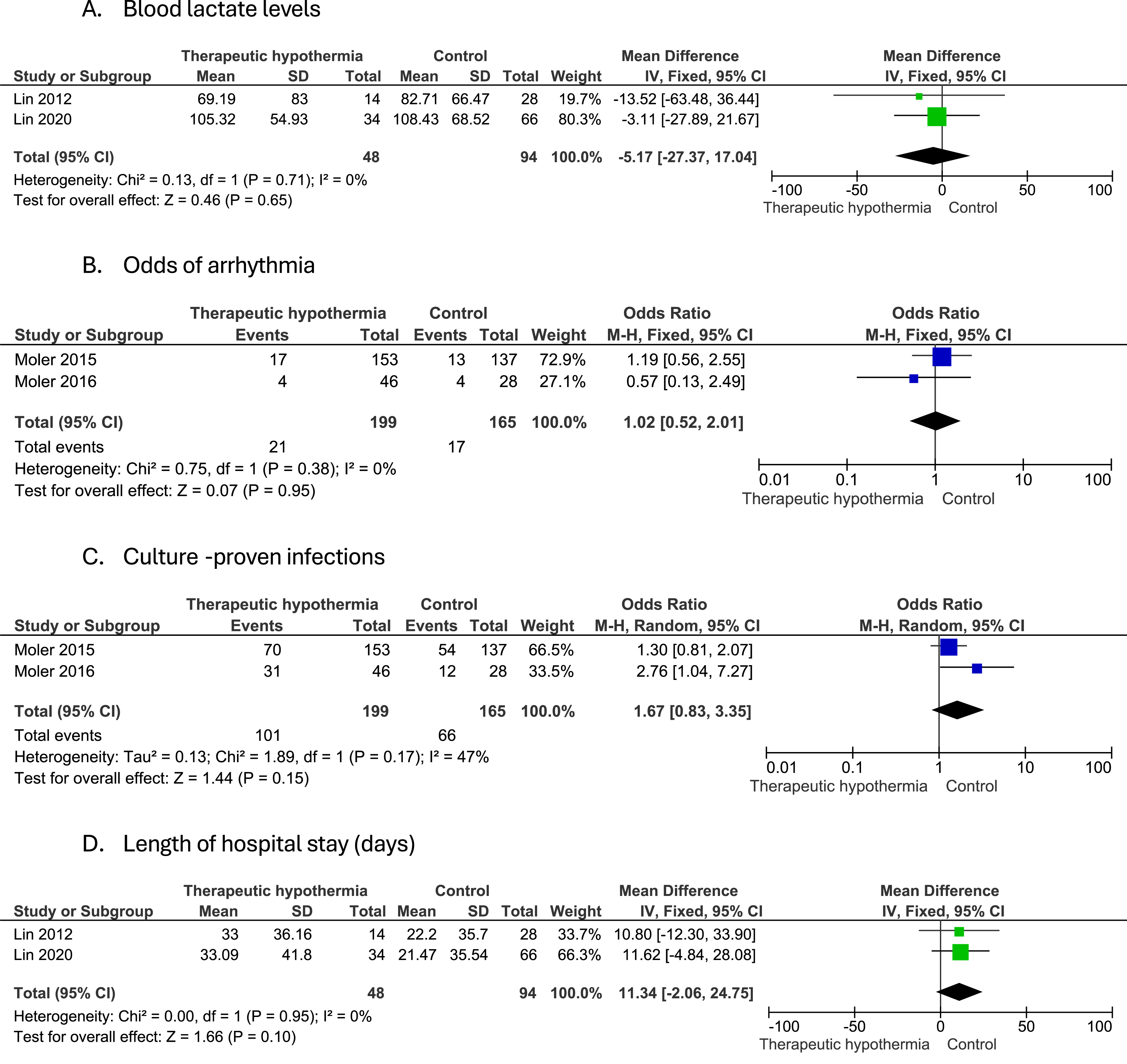
Forest plot of secondary outcomes:
Odds of arrhythmia
Pooled analysis of two studies revealed slightly higher but insignificant odds of arrhythmia in the TH arm (OR: 1.02; 95% CI: 0.52, 2.01; p = 0.95), with homogenous estimate (I2 = 0%) (Fig. 3B).
Culture-proven infections
Pooled analysis of two studies revealed slightly higher but insignificant odds of infections in the TH arm (OR: 1.67; 95% CI: 0.83, 3.35; p = 0.15), with mild heterogeneity (I2 = 47%, p = 0.17) (Fig. 3C).
Length of hospital stay
Pooled analysis of two studies revealed slightly higher but insignificant length of hospital stay in the TH arm (OR: 11.34; 95% CI: −2.06, 24.75; p = 0.1), with homogenous estimate (I2 = 0%) (Fig. 3D).
Other outcomes
Status epilepticus (SE) was reported in two studies, Prajongkit et al., 2019 and Lin et al., 2013. In Prajongkit et al., 2019, status epilepticus occurred in 2 of 6 patients (33.33%), while in Lin et al., 2013, 9 of 14 patients noted status epilepticus (64.28%), recording a high incidence of SEs. Additionally, Vineland Adaptive Behavior Scales (VABS-II) score was reported in Moler et al., 2015, which noted >30 points in 13% of patients in the TH arm versus 11% in the control arm, 16–30 points in 7% in the intervention arm and 3% in the control arm, and ≤15 points in 14% of the intervention arm and 13% of the control arm.
Discussion
This systematic review and meta-analysis evaluated the impact of TTM, including TH, on survival and neurological outcomes among pediatric patients who achieved ROSC following OHCA. Our findings indicate that TTM, particularly TH, may confer a survival and neuroprotective advantage in this critically ill population, though the certainty of evidence for these benefits remains low for most outcomes, primarily due to reliance on nonrandomized data.
Our analysis showed that TH significantly improved survival at both 30 days and 12 months post-OHCA. This finding aligns with several prior observational reports suggesting a survival benefit with induced hypothermia in pediatric cardiac arrest patients (Lin et al., 2013; Prajongkit et al., 2019). Additionally, a substantial neurological benefit was noted with hypothermia, particularly at longer-term follow-up (6–12 months: OR: 2.17; 95% CI: 1.20–3.95), reinforcing the hypothesis that hypothermia may mitigate delayed hypoxic-ischemic neuronal injury mechanisms (Arnautovic et al., 2024; Topjian et al., 2019). The delayed improvement in neurological outcomes observed at 6–12 months in our analysis may reflect the underlying mechanisms of neuroprotection conferred by hypothermia, which target evolving secondary brain injury rather than immediate structural damage. TH is thought to attenuate glutamate-mediated excitotoxicity, reduce free radical formation, stabilize mitochondrial function, and modulate pro-inflammatory cascades, thereby limiting neuronal apoptosis and cerebral edema in the postischemic period (Arnautovic et al., 2024). These effects unfold over days to weeks and may explain why short-term neurological assessments, such as at one month, did not show a significant benefit, while longer-term outcomes did. Moreover, the pediatric brain differs structurally and metabolically from the adult brain; it has a higher water content, greater plasticity, and lower metabolic reserve, which may modify its vulnerability to hypoxia and its responsiveness to hypothermic intervention. These developmental factors may influence both the trajectory and magnitude of neurological recovery, further supporting the importance of long-term follow-up in pediatric TTM studies.
The comparatively lesser benefit at the 1-month mark might reflect the delayed recovery trajectory often observed in pediatric brain injury postarrest, wherein neurocognitive recovery becomes more apparent only over time (Kirschen et al., 2014). Early neurological assessments often underestimate functional potential, given the complex interplay of sedation effects, postarrest encephalopathy, and delayed cortical maturation. Short-term scores may also fail to capture neurocognitive and behavioral adaptation that emerges gradually over time (Kirschen et al., 2014). Our findings of improved survival (OR: 1.72) and favorable neurological outcome (OR: 1.64) with TH contrast with the neutral results of the THAPCA-OHCA trial (Chang et al., 2016), which found no significant difference in 1-year survival with good neurological outcome between hypothermia (33.0°C for 48 hours) and normothermia (36.8°C) in comatose pediatric OHCA survivors. Despite methodological rigor, THAPCA-OHCA was underpowered for detecting modest differences and excluded certain high-risk groups (e.g., traumatic arrest), which may limit generalizability. However, the discrepancy between our pooled positive signal and THAPCA’s neutral findings likely reflects the influence of residual confounding and selection bias inherent in the observational studies that dominate our analysis. Nonrandomized designs may inadvertently capture more intensive care environments or centers with greater neurocritical care expertise, thus conflating center-level practices with treatment effect. This reinforces the need for caution in interpreting pooled observational data as causal. Furthermore, the 2020 AHA Pediatric Post-Cardiac Arrest Care statement (Topjian et al., 2019) highlights the lack of sufficient evidence to recommend for or against TTM in children, instead placing emphasis on fever avoidance rather than active hypothermia. Our findings, while suggestive of benefit, should therefore be viewed as hypothesis-generating and supportive of further individualized, protocolized care approaches.
Our meta-analysis revealed no statistically significant increase in adverse events associated with the use of TH, suggesting an overall favorable safety profile when appropriately monitored. Specifically, pooled analyses demonstrated similar odds of arrhythmia between TTM and normothermia groups, with no detected heterogeneity. This finding aligns with recent evidence indicating that while bradyarrhythmias may be a physiological response to cooling, they are typically benign and rarely necessitate intervention when core temperature remains above 32°C (Wung, 2016). Despite well-documented concerns in adult populations where TTM has been associated with increased risks of infection and cardiac arrhythmias (Kim et al., 2015), our meta-analysis found no significant increase in arrhythmias or infections, with both outcomes supported by high-certainty evidence. These results suggest that when hypothermia is carefully monitored and protocolized, it does not confer unacceptable safety risks in children. This is a clinically meaningful finding, particularly in light of historical reluctance to adopt hypothermia in pediatric settings due to safety concerns. Our data support the view that TTM can be implemented without a substantial increase in adverse events, reinforcing the feasibility of incorporating TTM into postresuscitation care when delivered in experienced settings.
Similarly, the risk of culture-proven infections, a concern due to potential immunosuppressive effects of hypothermia, was slightly higher but statistically nonsignificant in the TTM group. These findings were consistent with those of the THAPCA trial, which also reported no significant differences in infection rates or antibiotic use between groups (Chang et al., 2016). Additionally, the length of hospital stay did not differ significantly, further supporting that TTM does not appear to prolong acute recovery or ICU burden when carefully implemented. However, these adverse event outcomes were based on a limited number of trials and relatively small patient populations, highlighting the need for future studies to more comprehensively assess the safety profile of hypothermia, particularly in diverse pediatric subgroups with differing comorbidities, immune status, and arrest etiologies.
While the pooled estimates show promising trends, our GRADE assessment revealed low certainty for the primary outcomes, primarily due to the observational nature of most included studies, risk of confounding, and imprecision. Moreover, while the trials provided high-certainty evidence for adverse outcomes (arrhythmia, infections), they also revealed no significant increase in harm with TTM, thus supporting its safety profile. The absence of increased adverse events like arrhythmia (OR: 1.02) or infection (OR: 1.67) suggests that with rigorous ICU monitoring and standard care protocols, hypothermia can be administered safely even in vulnerable pediatric populations (Thabet and Tabarki, 2019).
The neurological benefits, although modest and delayed, are particularly encouraging. Favorable outcomes on the PCPC and Vineland Adaptive Behavior Scales (VABS-II) highlight the potential for meaningful recovery when hypothermia is appropriately applied. Notably, our analysis of VABS-II in Moler et al. (Moler et al., 2016) indicated slightly better adaptive functioning scores in the hypothermia group, which, although not statistically significant, may hold clinical relevance when considering long-term quality of life and developmental trajectory (Holubkov et al., 2015).
Notably, while the effectiveness outcomes were graded as low certainty, our analysis included high-certainty evidence from RCTs regarding key safety outcomes. Specifically, there were no significant differences in the incidence of arrhythmia (OR: 1.02; 95% CI: 0.52–2.01; p = 0.95) or culture-proven infections (OR: 1.67; 95% CI: 0.83–3.35; p = 0.15) between TTM and normothermia groups. These findings, supported by well-conducted randomized trials such as the THAPCA trial provide high-certainty reassurance regarding the short-term safety of TH when delivered under appropriate critical care protocols. This is particularly relevant in pediatric ICU settings, where concern over potential adverse effects may limit adoption of TTM. Therefore, while the efficacy of TTM remains uncertain, the evidence does support its safety, which is an essential consideration in shared decision-making with families and care teams.
Notably, the observed heterogeneity in outcomes across included studies may be partly explained by key baseline differences and variations in TTM protocols. Differences in patient populations, such as age distribution, underlying health status, and event characteristics (witnessed arrest and bystander CPR rates), likely influenced neurological and safety outcomes. Furthermore, variations in TH parameters, including target temperature depth, duration of cooling, and rewarming rates, may have affected treatment efficacy and adverse event profiles. For example, deeper cooling or longer durations could offer neuroprotective benefits but may increase the risk of complications, while rapid rewarming may negate some protective effects. These factors underscore the importance of individualized TTM protocols and highlight the need for future studies to systematically evaluate how such protocol nuances impact clinical outcomes to optimize therapeutic strategies.
This review has several limitations. First, the optimal duration, depth, and method of TTM in pediatrics, while extracted, were unable to be implemented in the analysis due to heterogeneity across studies. The majority of included studies were observational, thus subject to confounding and bias. Additionally, certain secondary outcomes, such as seizure incidence and adaptive functioning, were reported in only a few studies, precluding meta-analytic pooling. Furthermore, residual confounding remains a significant concern, as the majority of included studies (7 out of 9) were nonrandomized. These designs are susceptible to unmeasured differences in case mix, resuscitation quality, and postarrest care. Importantly, observed benefits may partly reflect center-level expertise or selection biases, rather than a true treatment effect of TTM. Although some studies adjusted for known confounders using statistical methods such as multivariable regression, these cannot fully substitute for randomization. More high-quality RCTs are needed, and future meta-analyses should explore hierarchical models or metaregression incorporating hospital or system-level variables to better account for these contextual effects. Additionally, the interplay between TTM and other neuroprotective strategies such as early seizure detection and management, sedation protocols, and extracorporeal membrane oxygenation (ECMO) support requires further exploration. Emerging technologies such as near-infrared spectroscopy (NIRS) and continuous EEG may aid in real-time assessment of cerebral perfusion and injury, thus helping personalize TTM protocols (Francoeur et al., 2022).
Given the heterogeneity in cardiac arrest etiology and patient physiology, we advocate for stratified randomized trials that distinguish between asphyxial and arrhythmic causes, as well as age-based subgroups (<1 year vs. >1 year), in line with the pediatric-specific pathophysiology (Bockemuehl et al., 2025). Additionally, integrating advanced neuromonitoring tools such as NIRS and continuous EEG into trial protocols may help personalize TTM by identifying early patterns of cerebral hypoperfusion and seizure activity, thereby optimizing intervention windows (Grunau et al., 2015). Finally, future trials should explore multimodal therapeutic strategies, including the use of hypothermia in combination with early antiepileptic prophylaxis or ECMO support, particularly in patients with prolonged or refractory cardiac arrest. These approaches could address complex secondary injury cascades more comprehensively and enhance the neuroprotective effect of TTM.
Conclusion
In conclusion, TTM, particularly TH, may offer survival and neurological benefits in pediatric patients resuscitated from OHCA. While the current evidence supports a favorable risk-benefit profile, especially at longer-term follow-up, the low certainty of most findings necessitates cautious interpretation. Importantly, high-certainty evidence shows no significant increase in adverse events, such as arrhythmias or infections, reinforcing the safety of TTM when applied under appropriate clinical conditions. Given the critical need for effective neuroprotective strategies in this population, these results underscore the importance of further high-quality randomized studies and standardized outcome assessments. Clinicians should individualize TTM strategies based on patient context, with vigilant avoidance of postresuscitation hyperthermia.
Authors’ Contributions
M.A.: Conceived the project and developed the protocol. Led article writing, contributed to data analysis, coordinated all stages of the project, maintained communication with coauthors, and served as first and corresponding author. S.R.: Conducted the statistical analysis, drafted the discussion, and critically reviewed and approved the final article. I.K.: Assisted in research strategy, screening, data refinement, and analysis. Reviewed and approved the final article. S.T.A.: Performed screening and data extraction; contributed to writing the introduction and methods; reviewed and approved the final article. M.M.A.: Performed screening and data extraction; reviewed and approved the final article. E.L.: Provided critical revisions and editorial feedback on the final draft; reviewed and approved the final article. Z.S.: Reviewed and edited the final draft and approved the final article.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.