
Abstract
Although evidence-based recommendations for preventing perioperative unintentional hypothermia have long been available, observational studies evaluating their implementation in hospital practice and the effectiveness of preventive interventions in at-risk patients are limited. This study aimed to determine the scope of nursing interventions for preventing perioperative unintentional hypothermia and examine the relationship between patient characteristics and these practices. This study employed a descriptive observational design. Patients undergoing elective surgery in the surgical units (orthopedics, gynecology, urology, neurosurgery, general surgery, and cardiovascular surgery) of a tertiary hospital in Turkey were observed preoperatively, intraoperatively, and on the first postoperative day. The mean age of the participants was 51.30 ± 19.32 years; 77% were overweight or obese, 55.2% had chronic diseases, and 39.6% underwent surgeries lasting more than 2 hours. The findings indicated that the duration of surgery was a significant determinant of nurses’ perioperative hypothermia prevention practices. In longer procedures, nurses’ awareness of hypothermia risk increased, which was reflected in patient education, environmental temperature management, and the use of active and passive warming methods (p < 0.05). This study highlights the importance of educational programs, strengthening standard care protocols, and policy development to enhance nurses’ awareness and practice in preventing perioperative unintentional hypothermia. In conclusion, effective strategies are needed to improve nursing practice and promote evidence-based interventions in this area.
Introduction
Perioperative unintended hypothermia (UH), defined as a core body temperature below 36°C from 1 hour before surgery to 24 hours postoperatively, affects approximately 70% of surgical patients (Giuliano and Hendricks, 2017; Hegarty et al., 2009). UH is a common and preventable complication that can lead to adverse outcomes, such as bleeding, coagulation disorders, surgical site infections, altered drug metabolism, and prolonged postanesthesia care unit stay (Rauch et al., 2021).
Risk factors for perioperative UH include male sex, advanced age, high American Society of Anesthesiologists (ASA) scores, smoking, prolonged surgical duration (Sagiroglu et al., 2020), large surgical incisions, low preoperative body temperature, low body mass index (or altered fat distribution), type of anesthesia, and cold ambient temperature (Sessler, 2016). Maintaining normothermia requires accurate and continuous monitoring of the temperature. Clinical guidelines recommend reliable temperature monitoring, particularly via esophageal, bladder, or tympanic probes, for patients undergoing general anesthesia lasting longer than 30 minutes (Association of Perioperative Registered Nurses (AORN), 2019; Hooper et al., 2010; National Institute of Health and Care Excellence (NICE), 2021).
A prewarming period of approximately 30 minutes and the use of forced-air warming devices are essential for maintaining intraoperative normothermia. Passive warming methods alone are often insufficient, particularly during prolonged surgical procedures. In this context, the use of warmed intravenous (IV) fluids for large-volume infusions significantly reduces the risk of UH. Additionally, the operating room temperature should be appropriately adjusted according to the type of surgery and patient population, especially for neonatal, geriatric, or long-duration procedures. Monitoring perioperative body temperature and implementing warming strategies are strongly recommended for UH management (AORN, 2019; Coello et al., 2010; Hooper et al., 2010; NICE, 2021; Turkish Anesthesia and Reanimation Association (TARD), 2013). To maintain normothermia during anesthesia and surgery, it is essential to reduce cutaneous heat loss and prevent temperature loss associated with cold IV or irrigation fluids administered intraoperatively (Bilgin, 2017). Passive warming, a simple and commonly used method to reduce cutaneous heat loss, is applied using cotton or wool blankets, socks, and caps in recovery units and surgical wards, as well as surgical or plastic drapes in operating rooms. However, passive warming alone has been reported to be insufficient for maintaining adequate normothermia (TARD, 2013).
Compared with passive methods, active warming strategies (including forced-air warming, radiant warmers, water-circulating garments, heated IV fluids, blood and blood product warmers, resistive electric blankets, heat-moisture exchanger filters, and negative pressure warming) are more effective in sustaining normothermia (Hooper et al., 2010; TARD, 2013). Among the active warming methods, forced-air warming systems are strongly recommended because of their high level of evidence and clinical efficacy (Hooper et al., 2010).
Anesthesia induction should not commence until the patient’s core temperature exceeds 36°C (low recommendation) (Coello et al., 2010; NICE, 2021), and exposure to cold ambient conditions should be minimized (Hooper et al., 2010). The operating room temperature should be maintained at approximately 21°C, although it may be lowered once active warming systems are effectively established to maintain optimal working conditions (NICE, 2021). Narrative reviews, randomized controlled trials, and recent network meta-analyses consistently support the comprehensive use of active warming throughout the pre-, intra-, and postoperative periods as the most reliable approach for preventing perioperative hypothermia (Rauch et al., 2021).
Perioperative nurses are central to the implementation of temperature management practices, including risk assessment, initiation of prewarming, application and monitoring of forced-air warming devices, maintenance of appropriate ambient temperature, patient and family education, and temperature protection during postoperative care (Koyuncu et al., 2023). Studies in the literature on nurses’ knowledge and practices have reported gaps in knowledge and inconsistencies in implementation (Akboğa, 2024). Variability in nursing interventions to prevent UH has been observed, which is influenced not only by knowledge level but also by organizational conditions, shift differences, duration of surgery, and type of surgical procedure (Munday et al., 2019; Sessler, 2016).
Direct observation is the most appropriate method for understanding how nurses perform these interventions in real clinical settings. Self-report and survey-based data collection methods often reflect idealized practices rather than actual clinical behaviors. Social desirability bias and recall limitations can lead to significant discrepancies between reported and actual practice (Polit and Beck, 2021). Observational methods eliminate this gap by allowing the assessment of nursing care in its natural and direct flow (Harrison, 2011). This enables an objective evaluation of whether interventions for preventing perioperative UH are implemented. Observational studies are among the strongest designs for identifying evidence–practice gaps (Coker et al., 2013). Randomized or experimental studies, owing to the need for control groups and interventions, can alter the natural course of perioperative care. In contrast, UH prevention is a routine and continuous aspect of nursing care (Simegn et al., 2021). In this context, a descriptive observational design allows for the recording of nursing practices as they occur, without disrupting the clinical process.
Aim
In light of this, the present study aimed to determine the scope of nursing interventions for preventing perioperative UH and examine the relationship between patient characteristics and these interventions. By making the clinical reality of perioperative UH management visible and identifying variations in practice, this study provides a guiding framework for institutional policies and educational programs.
Methods
This study employed a descriptive design utilizing direct bedside observation data. The observational approach allows for the assessment of nursing interventions as they occur within the routine flow of care, providing an opportunity to identify gaps between the guideline recommendations and clinical practice (NICE, 2021; Polit and Beck, 2021; Sessler, 2016). This study aimed to determine the extent to which surgical and operating room nurses in Turkey implement evidence-based practices for managing perioperative UH in clinical settings.
A tertiary hospital in Turkey will be selected for the study between November 2024 and September 2025. Reporting was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines (von Elm et al., 2014). A structured observation checklist was developed to evaluate the perioperative UH prevention practices of surgical and operating room nurses in line with evidence-based recommendations.
Participants
The study sample included patients who underwent elective surgery at the selected center. Patients whose tympanic temperature fell below 36°C at any point during the perioperative period were considered to have perioperative UH. A total of 96 patients met the inclusion criteria: (1) undergoing elective surgery, (2) aged between 18 and 75 years, and (3) experiencing perioperative UH. Surgeries that did not meet the inclusion criteria, including emergency operations (n = 45), were excluded from the study. Patients who did not experience hypothermia at any stage of the surgical process (n = 93) were excluded from the study. The number of patients was determined with an 80% margin of error and a 5% confidence interval in the known sample calculation formula for the universe.
The researchers observed the surgical and operating room nurses responsible for the care of these patients during both day and night shifts. Planning for each preoperative observation was conducted 1 day prior. Patients were primarily monitored during the preoperative period and then followed during transfer to the operating room, with researchers accompanying patients and nurses during transport. Finally, postoperative care was observed in the surgical unit, including day and night shifts, to complete the 24-hour observation period. During the study, both the nurses and the patients were informed that the observations would focus solely on monitoring the patient’s temperature.
Data collection ınstruments
Data were collected using a survey form developed based on a literature review (de Oliveira Souza et al., 2019). The form consisted of two sections: the first section included seven items on personal information, while the second section comprised a checklist with 19 items for observing evidence-based interventions to prevent perioperative UH (Coello et al., 2010; Hooper et al., 2010; NICE, 2021; TARD, 2013). The survey form was reviewed by five experts with at least a doctoral degree in surgical nursing and academic experience in perioperative UH. The experts confirmed that the content of the form was adequate and appropriate, and no recommendations for modifications were provided.
Personal ınformation form
This section collected basic demographic and clinical data, including patients’ age, body mass index, smoking status, presence of chronic disease, history of previous surgeries, ASA classification, type of surgery, anesthesia method, and duration of surgery. Data were obtained directly from patients during the initial interview upon their consent to participate and were cross-verified and completed through a review of hospital records.
Checklist for evidence-based perioperative UH prevention practices
The checklist covered three stages: preoperative, intraoperative, and postoperative periods, including both day (08:00–16:00) and night (16:00–08:00) shifts. Six items were specified for preoperative observation, including risk assessment for hypothermia, application of active or passive warming methods, patient education, and regular body temperature monitoring. For the intraoperative and postoperative periods, 13 items were included to cover interventions such as monitoring patient temperature and room temperature, as well as the application of active (e.g., radiant warmers, forced-air warming) or passive (e.g., blankets, socks) warming methods. Postoperative observations were continued during the night shift on the day of surgery.
The internal consistency of the checklist was evaluated using Cronbach’s alpha, yielding a coefficient of 0.703, which indicated acceptable reliability. This result demonstrates that the items were sufficiently related to the concept being measured and that the data collection instrument possessed a statistically supported internal consistency (Cronbach, 1951).
Data collection
Data were collected in three stages: preoperative, intraoperative, and postoperative. During preoperative admission and hospitalization, surgical nurses were observed regarding the identification of hypothermia risk factors, monitoring of body temperature, initiation of prewarming, patient or family education, and patient transfer procedures across various surgical units (orthopedics, gynecological surgery, urology, neurosurgery, general surgery, and cardiovascular surgery).
During the intraoperative period, the nurses’ implementation of interventions to prevent perioperative UH was systematically observed. This included monitoring whether nurses regularly checked the patient’s body temperature and applied appropriate warming methods if hypothermia was detected. Depending on the duration of surgery, it was observed whether high-risk patient groups were actively warmed in procedures lasting more or less than 30 minutes. The control of the operating room temperature by nurses and interventions to ensure adequate thermal conditions were also evaluated. For procedures involving fluid replacement of more than 1.000 mL (e.g., IV fluids or blood products), we observed whether the fluids were prewarmed and whether this intervention was effective in maintaining patient normothermia. In major surgical procedures, it was additionally assessed whether multiple warming methods were applied simultaneously; however, surgeries lasting less than 30 minutes were not included in this evaluation.
Postoperatively, surgical nurses regularly monitored and documented patients’ body temperature, as well as assessed and recorded patient conditions according to clinical needs. Room temperature monitoring and adjustments to ensure an appropriate environment, particularly in patients with postoperative hypothermia, were also assessed. The nurses’ use of passive warming methods (e.g., blankets and socks) and active warming methods (e.g., radiant warmers and forced-air warming devices) was systematically observed. These observations continued through the night shifts. Patients for whom no hypothermia measurement was recorded at any stage were excluded from the study due to noncompliance with the evaluation criteria.
Data analysis
Descriptive statistical methods were used to evaluate the demographic and clinical characteristics of the patients included in the study. Continuous variables are presented as mean ± standard deviation (SD) or median (minimum–maximum), whereas categorical variables are expressed as number (n) and percentage (%). The relationship between patients’ personal characteristics and nurses’ perioperative hypothermia prevention practices was also examined. Appropriate statistical tests were applied, and a significance level of p < 0.05 was considered statistically significant.
Ethical considerations
Ethical approval was obtained from the Ethics Committee of the university where the study was conducted (Decision No: 16/24, dated July 17, 2024) and institutional permission was obtained from the relevant center (E-16142545-302.14-269934). Prior to initiating the study, the researchers secured all necessary legal and official ethical approvals and formally announced the study in accordance with the permissions.
Additionally, one-on-one meetings were held with nurses responsible for surgical units (orthopedics, gynecological surgery, urology, neurosurgery, general surgery, and cardiovascular surgery) to provide detailed information about the study’s content, scope, and objectives, ensuring active participation and cooperation. Participants were explicitly informed that participation was entirely voluntary and that they could withdraw at any time without providing a reason. It was also explained that observations would be limited to the surgical process, no medical or nursing interventions would be performed, and participation would neither provide direct benefits nor pose any risks. Following this information, both verbal and written informed consent were obtained from the nurses and patients, and data collection commenced in accordance with ethical principles. All procedures performed in this study were conducted in accordance with the ethical standards of the institutional and/or national research committee and with the principles of the Declaration of Helsinki.
Results
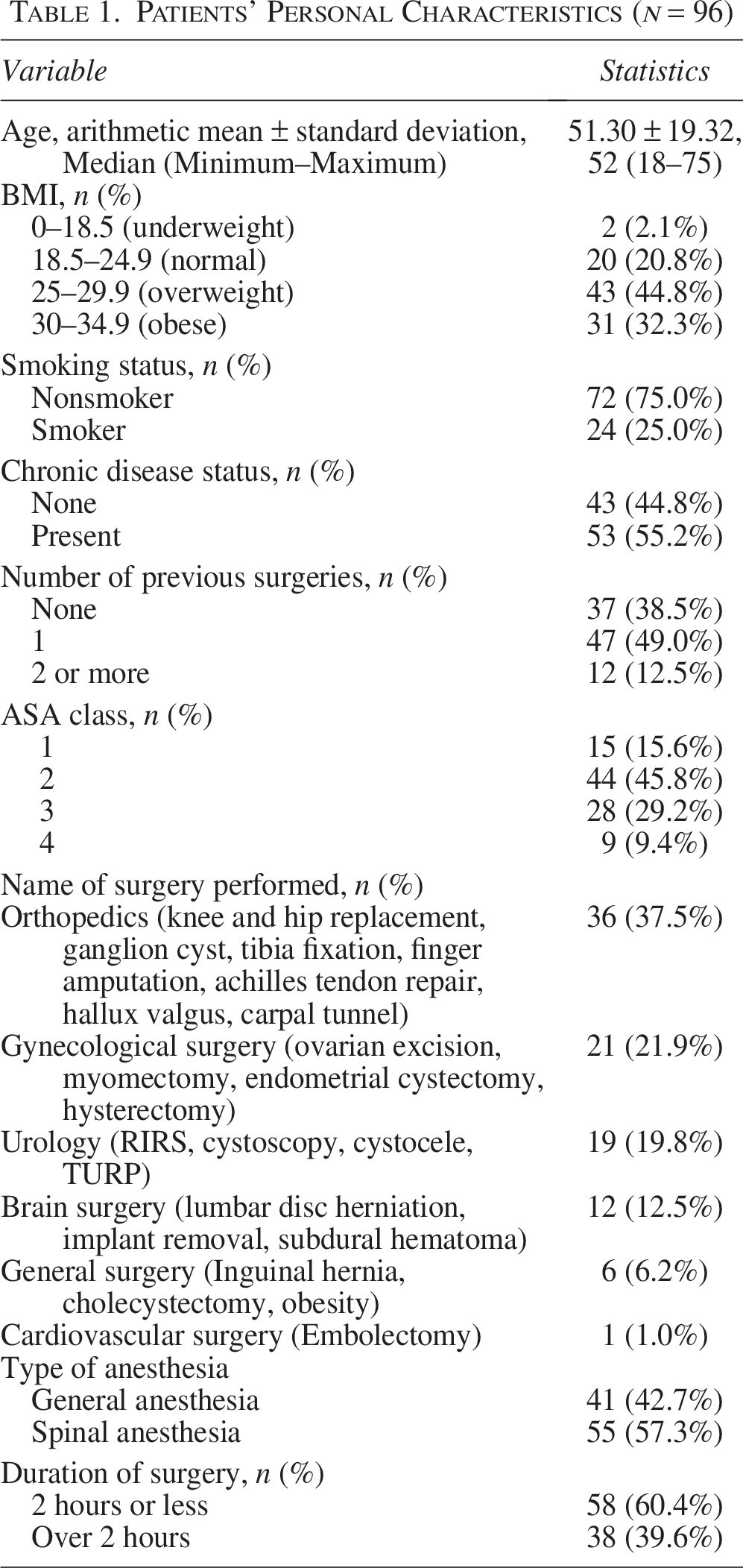
In the study setting, the estimated incidence of perioperative UH ranged from 41.02% to 60.25%. The mean age of the participants was 51.30 ± 19.32 years, with ages ranging from 18 to 75 years. Approximately 77% of the participants were overweight or obese, 25% were smokers, and 55.2% had at least one chronic disease. Approximately 60% had undergone at least one prior surgery, and approximately 85% were classified as ASA II–IV. The most frequently performed surgeries were orthopedic (37.5%), gynecologic (21.9%), and urologic (19.8%), followed by neurosurgery (12.5%) and general surgery (6.2%) surgeries. Surgery duration was ≤2 hours in 60.4% of cases, general anesthesia was applied in 42.7%, and 39.6% of operations lasted longer than 2 hours (Table 1).
Patients’ Personal Characteristics (n = 96)
Preoperatively, more than half of the surgical nurses assessed patients for hypothermia risk (61.5%), nearly all checked patients’ body temperature (96.9%), most did not apply active warming methods (97.9%), over half preferred passive warming interventions (64.6%), approximately half provided preoperative patient education (54.2%), and over half covered the patients during transfer (63.5%). During surgery, most operating room nurses did not monitor patient temperature (71.9%), and more than half did not apply warming methods when hypothermia was detected (58.3%). Most controlled the ambient temperature (69.8%), and nearly all did not use fluid warming or multiple warming methods (99.0% and 95.8%, respectively).
Postoperatively, during day shifts, nearly all surgical nurses monitored and documented patient body temperature (97.9%), whereas more than half did not increase room temperature when patients were hypothermic (61.5%). Passive warming methods were the most commonly used (70.8%), active warming methods were rarely applied (89.6%), and 80.2% of nurses monitored room temperature. During night shifts, the rates of UH prevention practices were similar, although there was a decrease in increasing room temperature and applying passive warming methods.
A comparison of UH prevention practices with patient characteristics revealed that only surgery duration was significantly associated with multiple preventive interventions (p < 0.05). As surgery duration increased, nurses’ awareness of hypothermia risk, provision of preoperative education, and use of protective measures increased; intraoperatively, patient temperature monitoring, ambient temperature regulation, and active warming interventions increased; postoperatively during day shifts, rates of adjusting room temperature and applying passive/active warming methods increased; and during night shifts, only the rate of increasing and monitoring room temperature increased (Table 2).
Evidence-Based Interventions by Nurses to Prevent Perioperative Unintentional Hypothermia

Bold characters indicate statistically significant values (p < 0.05).
Fisher’s exact test.
Discussion
Direct observation of nursing practices during the perioperative period is crucial for objectively demonstrating the relationship between clinical interventions and patient safety (Gurunathan et al., 2017). In this study, the incidence of perioperative UH ranged from 41.02% to 60.25%, and the majority of participants were overweight/obese and classified as ASA II–IV. Considering the UH risk for this sample, it can be inferred that high-risk patients were included and that the institution exhibited a relatively high incidence of perioperative UH. This finding underscores the need to review existing nursing practices for hypothermia prevention through observational studies and integrate active warming strategies into routine care.
Sessler (2016) also emphasized that UH occurs more frequently in prolonged surgeries, obese patients, and those with higher ASA classifications. It has been reported that a substantial proportion of patients undergoing elective surgery (69.8%) develop intraoperative hypothermia (de Assunção Peixoto et al., 2021). While most nurses are aware of UH and its risk factors (Durmaz et al., 2024), the implementation of preventive measures remains suboptimal (Jallow and Bayraktar, 2024). The high incidence observed in the current study is consistent with previous research and may be associated with patient characteristics and deficiencies in perioperative care practices.
In the preoperative period, approximately half of the nurses assessed patients for hypothermia and measured their body temperature; however, the use of active warming methods was limited. Most nurses preferred passive warming interventions and environmental temperature control to prevent hypothermia in patients. Mutluay (2023) similarly reported that nurses more frequently rely on passive methods—such as patient coverings or increasing room temperature—rather than active warming techniques. Most health care personnel reportedly demonstrate positive attitudes and acceptable practices regarding perioperative UH prevention (Guo et al., 2025). This aligns with the current study, indicating that active warming interventions are minimally integrated into routine clinical practices.
Consistent with the findings of this observational study, surgical nurses rarely applied active warming methods and acknowledged the necessity of interventions such as fluid warming or simultaneous application of multiple warming techniques. Although nurses have expressed that hypothermia prevention practices should be more extensively implemented (Şahin Akboğa and Dikmen Aydın, 2024), this observational study revealed that these practices were applied at a low rate in clinical settings. This discrepancy highlights the evidence–practice gap and demonstrates that findings obtained through direct observation differ from those reported in self-reported surveys (Harrison, 2011; Polit and Beck, 2021). Similar studies in the literature also indicate that while nurses possess knowledge of active warming methods, various barriers impede their practical implementation (Kırtıl and Akboğa, 2025).
Sessler (2016) noted that prolonged surgical duration accelerates heat loss, thereby facilitating the development of perioperative hypothermia (UH). This finding parallels the results of the current study, which demonstrated that nurses’ awareness of UH and implementation of preventive measures increased significantly as the surgery duration increased. The literature also reports various factors that influence nurses’ perioperative UH prevention practices. Woretaw et al. (2023) highlighted that intensive care experience, prior training on UH, and sufficient knowledge levels are important individual factors affecting nurses’ implementation of hypothermia prevention interventions. However, while that study extensively examined the relationship between nurses’ individual characteristics and hypothermia prevention practices, it paid limited attention to the impact of patient-related factors (e.g., age, body mass index, ASA classification, and comorbidities). This underscores the need for a holistic approach to evaluate the multidimensional factors influencing perioperative UH.
Additionally, Honkavuo and Loe (2020) reported that nurses monitor body temperature during prolonged surgeries (e.g., aneurysm, gastrointestinal, or renal operations) but frequently omit this monitoring in shorter procedures (e.g., cholecystectomy), further supporting a direct relationship between surgery duration and nursing practice. Nurses encounter various institutional and individual barriers when attempting to prevent hypothermia, including inadequate resources, negative attitudes from physicians, and some nurses’ reluctance or lack of motivation (Şahin Akboğa and Dikmen Aydın, 2024). The level of nurses’ knowledge and awareness of perioperative UH prevention is closely linked to clinical experience, work environment, surgery duration, and institutional support. Similarly, in the current study, as the surgery duration increased, nurses’ risk awareness and application of preventive measures also increased; however, active warming methods remained underutilized. Furthermore, a decrease in hypothermia prevention practices was observed during night shifts, which may be associated with a reduction in patient hypothermia incidence or patient feedback over time.
Conclusion
This study revealed a high incidence of perioperative UH within the institution, with the majority of participants belonging to high-risk groups for UH. Nurses’ awareness and preventive practices for UH varied according to the duration of surgery. Surgical duration significantly influenced nurses’ adherence to UH prevention measures. In longer surgeries (over 2 hours), nurses demonstrated greater attentiveness during preoperative preparation, intraoperative monitoring, and postoperative care. As the surgery duration increased, nurses’ risk awareness and use of protective measures significantly increased; however, the overall application of active warming methods remained insufficient. Passive warming interventions, patient covering, ambient temperature control, and patient education showed the greatest variability. Active warming methods are generally applied at low rates. A decrease in hypothermia prevention practices was observed during the night shifts.
Recommendations
To reduce the incidence of perioperative UH, standardized protocols and clinical guidelines based on evidence-based approaches should be developed within institutions. It is important to comprehensively identify barriers arising from individual nurse characteristics, patient factors, and institutional limitations. Targeted strategies should be designed to address the identified problem areas, and continuous monitoring and evaluation mechanisms should be implemented to ensure effective compliance and quality improvement in hypothermia prevention practices.
Authors’ Contributions
ÖŞ.A. and B.A: Study conception and design, ÖŞ.A. and B.A: Analysis and interpretation of data. B.A. and ÖŞ.A.: Acquisition of data, analysis and interpretation of data, and drafting of article. All authors read and approved the final article.
Footnotes
Acknowledgments
The authors would like to thank F.E. (Dr.) for his support in statistical consultancy.
Author Disclosure Statement
The authors certify that there is no conflicts of interest with any financial organization regarding the material discussed in the article.
Funding Information
The study was not supported.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.