
Abstract
Target temperature management (TTM) is a neuroprotective strategy widely used in acute brain injury. However, its real-world implementation remains highly heterogenous and the clinical implications of different temperature targets and treatment durations are not well defined. This study aimed to describe real-world TTM practices and to explore associations between TTM characteristics, coagulopathy, and in-hospital mortality in patients with acute brain injury. We retrospectively analyzed 180 patients who underwent TTM between January 2011 and December 2024 at a single tertiary medical center. Patients diagnosed with acute brain injury, including aneurysmal subarachnoid hemorrhage, traumatic brain injury (TBI), intracerebral hemorrhage, or acute infarction, were included. Clinical variables, TTM parameters, complications, comorbidities, and in-hospital outcomes were analyzed. Univariable and multivariable analyses were conducted to identify factors associated with in-hospital mortality and TTM-related coagulopathy. In-hospital mortality occurred in 78 patients (43.3%). In multivariable analysis, post-cardiac arrest state (odds ratio [OR] = 3.99, p = 0.003) and coagulopathy during TTM (OR = 5.31, p = 0.005) were significantly associated with increased in-hospital mortality. Coagulopathy occurred in 21 (11.7%) patients and was significantly associated with type of injury, which showed it was most prevalent in TBI. Prolonged duration of TTM was not associated with an increased risk of coagulopathy and was associated with lower in-hospital mortality (OR = 0.30, p < 0.001). Injury subtype demonstrated significant heterogeneity in mortality risk and was retained as a covariate in the final multivariable model. In this real-world cohort, TTM practices varied substantially across acute brain injury subtypes. Coagulopathy was associated with increased in-hospital mortality and occurred more frequently in patients with TBI. Prolonged TTM was associated with lower in-hospital mortality. However, this finding should be interpreted cautiously given the potential for survivorship bias. Mortality risk differed across injury subtypes. These findings suggest that the clinical context and underlying injury type should be considered when applying TTM in patients with acute brain injury.
Keywords
Introduction
Target temperature management (TTM) has been applied as a neuroprotective strategy aiming to mitigate secondary brain injury following acute cerebral insults (Ito et al., 2024). While its efficacy has been well established in specific conditions such as cardiac arrest and neonatal hypoxic brain injury, its indications and therapeutic benefits in patients with acute brain injury remain a subject of ongoing debate (Montaldo et al., 2024; Gluckman et al., 2005; Choi et al., 2021). In clinical practice, TTM is applied in two distinct contexts in acute brain injury: As a rescue therapy for refractory intracranial hypertension and as a broader neuroprotective strategy aimed at reducing secondary brain injury. To date, large-scale randomized controlled trials (RCTs) have produced heterogeneous results depending on the subtype of brain injury, with some reporting modest differences in outcomes (Olah et al., 2021; Lyden et al., 2005; Andrews et al., 2015). Although these studies generally support the feasibility and safety of TTM in neurocritical care, consistent evidence for survival benefit remains limited. Moreover, there is no unified international guideline that clearly defines the indications or protocols in this population. In this context, we conducted a retrospective analysis of patients treated with TTM at a single tertiary medical center to identify clinical factors associated with in-hospital mortality and complications. Through this investigation, we aim to provide real-world data that may help inform future refinement of TTM protocols in patients with acute brain injury.
Patients and Methods
Patient selection and data collection
Between January 2011 and December 2024, a total of 198 patients who underwent TTM during their admission to the neurosurgery department at our institution were retrospectively identified. Inclusion criteria were (1) patients who received TTM and (2) admission for acute brain injury. Exclusion criteria were (1) patients under the age of 18, (2) patients with diagnoses not consistent with acute brain injury (e.g., brain tumor), and (3) cases in which body temperature was not managed using core temperature-controlled cooling systems.
Clinical data were retrospectively collected from medical records and imaging archives. Variables included demographic characteristics, a target temperature, duration of TTM, application of rewarming protocol, surgical interventions, reoperation due to postoperative deterioration, Glasgow Outcome Scale (GOS) score at discharge, and complications during TTM such as pneumonia and coagulopathy.
TTM protocol
All patients underwent TTM using either an endovascular cooling catheter system (CoolGard™, Zoll Medical, USA) or a surface cooling device (Arctic Sun®, Medivance, USA). The target temperature was set between 31°C and 36.5°C, depending on the patient’s clinical condition. In patients who underwent rewarming, the rate was maintained between 0.05°C/hour and 0.1°C/hour. Rewarming was not performed in patients who died during TTM, experienced device malfunction, had persistent hemodynamic instability, or in whom the target temperature was close to normothermia (e.g., target temperature of ≥36°C), making a formal rewarming protocol unnecessary. All patients received continuous intravenous sedation with either midazolam or pentobarbital during TTM. Endotracheal intubation and mechanical ventilation were applied throughout the treatment period.
Definitions
Patients with a target temperature ≤35°C were classified as the lower target temperature group, while those with a target temperature >35°C were classified as the higher target temperature group. A long-term hypothermia group was defined as patients whose TTM duration was 6 days or longer. The cutoff of 6 days was selected based on the distribution of TTM duration in the study cohort, representing a prolonged treatment course in real-world practice. Pneumonia was diagnosed based on radiographical findings (e.g., chest X-ray) in conjunction with the identification of pathological organisms on culture studies. Coagulopathy was defined as an international normalized ratio (INR) of ≥1.5 at any point during the TTM period.
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics, version 29.0.2.0 (IBM Corp., Armonk, NY, USA). Categorical variables were expressed as frequencies and percentages (%). Patients were categorized into survivor and nonsurvival groups, with nonsurvival defined as in-hospital death (GOS score of 1 at discharge). An independent t-test and chi-square analyses were conducted to compare demographic and clinical variables between the survivor group and the nonsurvivor group. Univariable and multivariable logistic regression analyses were conducted to identify variables associated with in-hospital mortality. To assess factors associated with TTM-related coagulopathy, patients were dichotomized according to the development of coagulopathy, and similar statistical analyses were performed. As the number of events was limited (n = 21), a parsimonious modeling strategy was applied to reduce the risk of model overfitting. Candidate variables were selected based on univariate screening (p < 0.20) and clinical relevance, and the final multivariate logistic regression model was constructed accordingly. A p-value of <0.05 was considered statistically significant.
This study was approved by the Institutional Review Board at Ajou University School of Medicine.
Results
A total of 198 patients met the inclusion criteria. Among them, 9 patients who underwent noncore temperature-controlled surface cooling rather than a standardized core temperature management system (CoolGard or Arctic Sun) and 5 patients under the age of 18 were excluded. Additionally, 4 patients diagnosed with brain tumors were excluded. As a result, 180 patients diagnosed with acute brain injuries—specifically aneurysmal subarachnoid hemorrhage (aSAH), traumatic brain injury (TBI), intracerebral hemorrhage (ICH), or acute infarction—were included in the final analysis (Fig. 1).
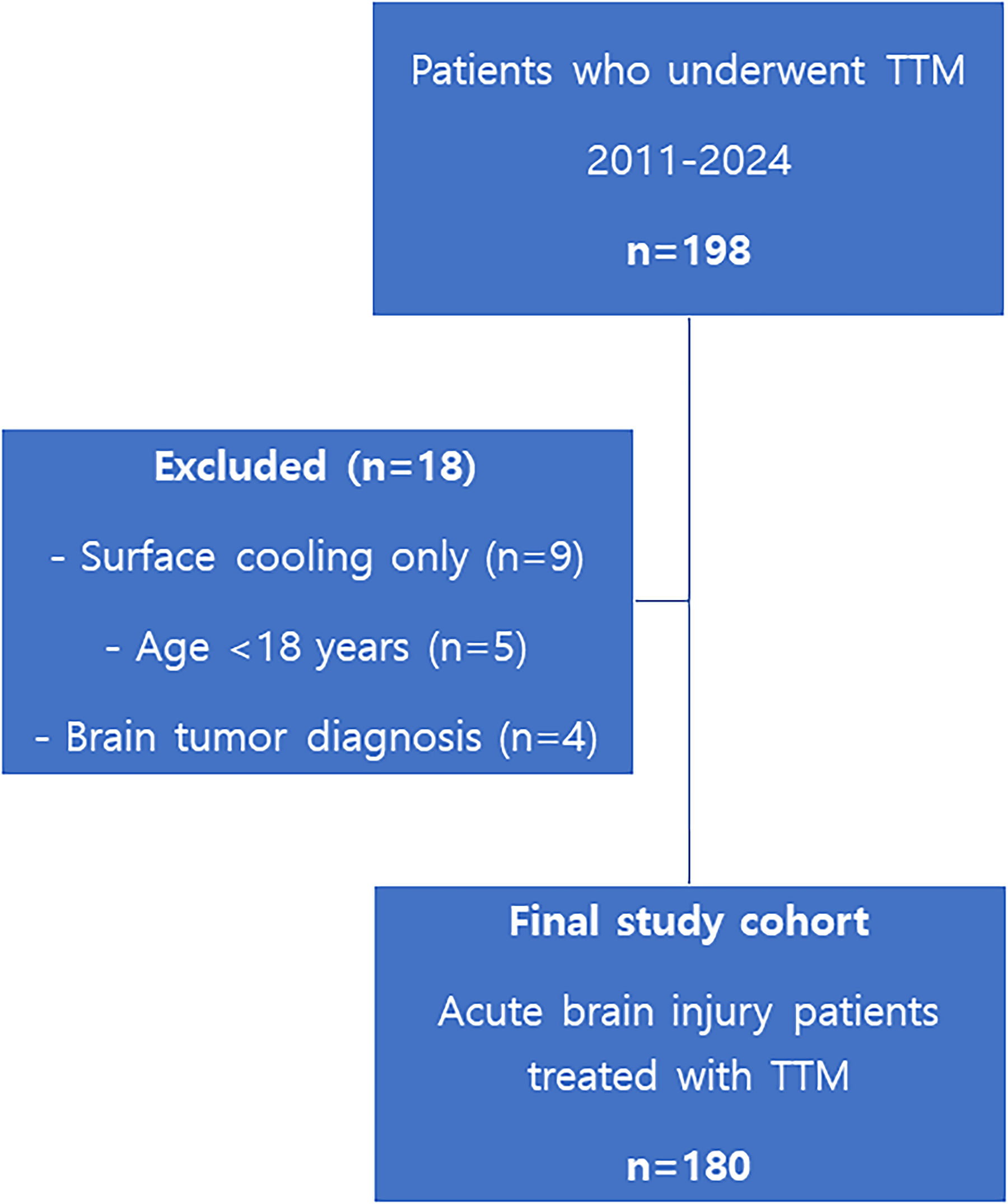
Study cohort assembly. Flow diagram showing the selection of patients included in the final analysis.
Table 1 summarizes the demographic and clinical characteristics, laboratory findings, injury type, and comorbidities of the 180 patients included in the study. The mean age was 51.66 ± 12.22 years, and 100 patients (55.6%) were male. Regarding injury type, aSAH was the most common, accounting for 83 patients (46.1%), followed by TBI in 47 (26.1%), acute infarction in 28 (15.6%), and ICH in 22 patients (12.2%).
Baseline Characteristics, Comorbidities, and Clinical Outcomes of the Total 180 Patients Included in the Study
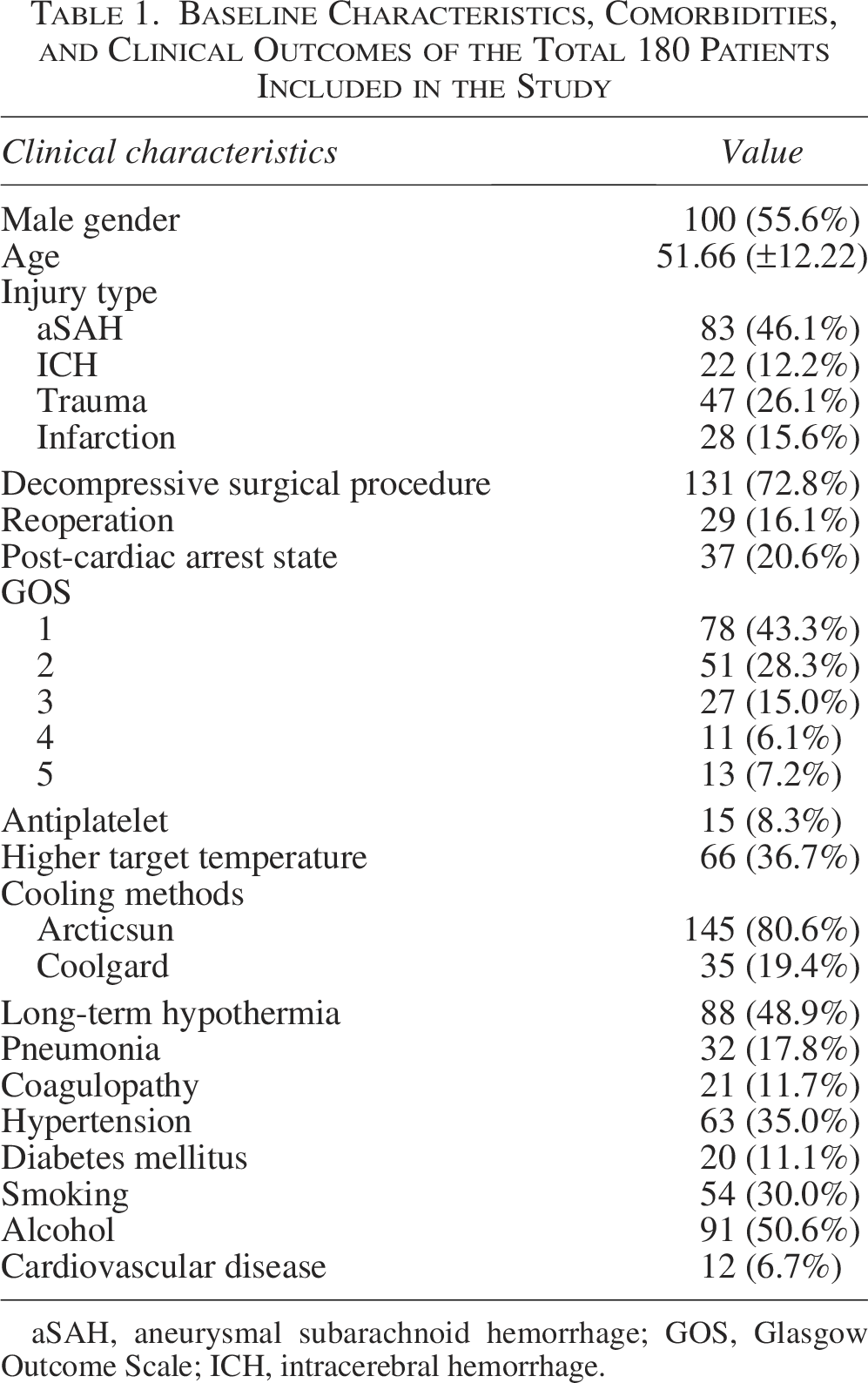
aSAH, aneurysmal subarachnoid hemorrhage; GOS, Glasgow Outcome Scale; ICH, intracerebral hemorrhage.
Decompressive surgical procedures were performed in 131 patients (72.8%), and 29 patients (16.1%) underwent reoperation due to postoperative deterioration, including increased cerebral edema, rebleeding, or intracranial hypertension. A total of 37 patients (20.6%) were in a post-cardiac arrest state at the time of admission.
Regarding outcomes, 78 patients (43.3%) had a GOS score of 1, indicating in-hospital mortality. GOS scores of 2, 3, 4, and 5 were observed in 51 (28.3%), 27 (15.0%), 11 (6.1%), and 13 (7.2%) patients, respectively. Fifteen patients (8.3%) were on antiplatelet therapy at the time of admission. As for TTM settings, 66 patients (36.7%) underwent higher target temperature hypothermia with a target temperature of >35°C. Arctic Sun was used in 145 patients (80.6%) and CoolGard in 35 (19.4%). Long-term hypothermia, defined as TTM duration ≥6 days, was applied in 88 patients (48.9%), while the remaining 92 patients (51.1%) received TTM for less than 6 days.
Complications observed during TTM included pneumonia in 32 patients (17.8%) and coagulopathy in 21 (11.7%). Comorbidities included hypertension in 63 patients (35.0%), diabetes mellitus in 20 (11.1%), and cardiovascular disease in 12 (6.7%). Smoking and alcohol use were reported in 54 (30.0%) and 91 (50.6%) patients, respectively.
Table 2 summarizes the results of univariable and multivariable analyses performed to identify risk factors associated with in-hospital mortality. Patients were classified into survivor and nonsurvivor groups for comparison. In univariable analysis, several factors were significantly associated with in-hospital mortality: injury type (p = 0.007), decompressive surgical procedure (odds ratio [OR] = 0.288, p < 0.001), post-cardiac arrest state (OR = 5.787, p < 0.001), long-term hypothermia (OR = 0.292, p < 0.001), applying a rewarming protocol (OR = 0.504, p = 0.024), and development of coagulopathy during treatment (OR = 5.006, p = 0.001). In contrast, reoperation, higher temperature target hypothermia, cooling method, occurrence of pneumonia, and various comorbidities did not show statistically significant differences between the two groups. Among the significant variables, post-cardiac arrest state (OR = 3.990, p = 0.003), long-term hypothermia (OR = 0.298, p < 0.001), and coagulopathy (OR = 5.308, p = 0.005) remained independently associated with in-hospital mortality in the multivariable analysis. Injury type was also included as a covariate in the final predictive model, despite not reaching statistical significance in the multivariable analysis.
Univariable and Multivariable Analyses of Factors Associated with in-Hospital Mortality in Target Temperature Management
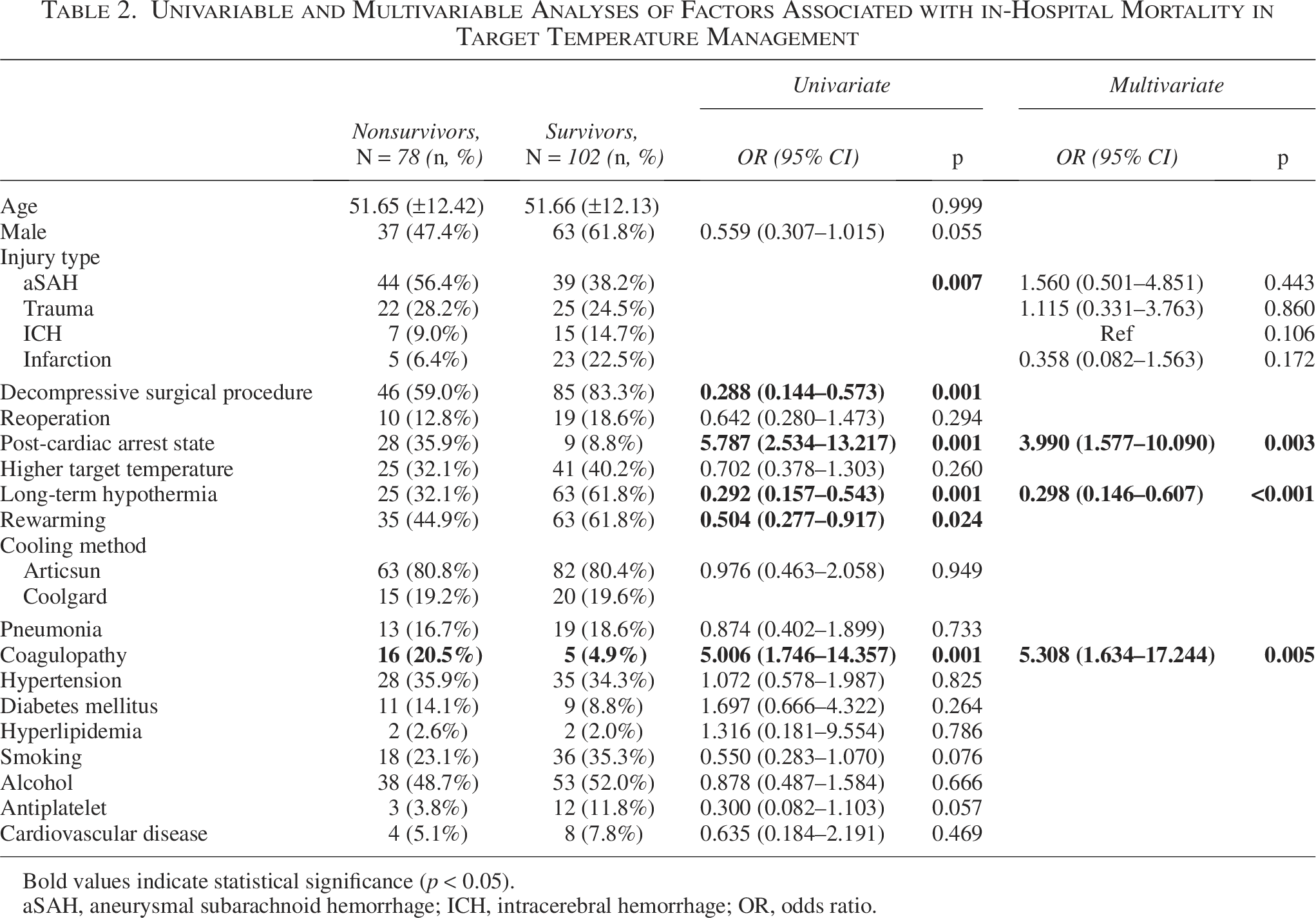
Bold values indicate statistical significance (p < 0.05).
aSAH, aneurysmal subarachnoid hemorrhage; ICH, intracerebral hemorrhage; OR, odds ratio.
A sensitivity analysis excluding patients with post-cardiac arrest states was performed to address potential cohort heterogeneity and confounding (Supplementary Table S1). In this analysis, long-term hypothermia and the coagulopathy during TTM remained significantly associated with in-hospital mortality. In contrast, variables that were significant in the univariate analysis of the primary cohort, including injury subtype and decompressive surgical procedure, were no longer statistically significant. Overall, the persistence of the associations for long-term hypothermia and coagulopathy suggests that these findings were relatively robust, whereas other variables appeared to be more susceptible to confounding effects related to patient selection and clinical heterogeneity.
As TTM-related coagulopathy was identified as a significant complication associated with in-hospital mortality, we conducted additional analyses to identify its risk factors. Table 3 summarizes the results of univariable and multivariable analyses performed to identify risk factors associated with TTM-related coagulopathy. Injury subtype emerged as the only statistically significant variable in the univariable analysis. In the final multivariable model, both the injury subtype and decompressive surgical procedure, which were not statistically significant in the univariate analysis, were included as covariates. These variables were retained as covariates in the final model due to their potential confounding effects and clinical relevance, despite not reaching statistical significance in univariable analysis.
Univariate and Multivariate Analyses of Factors Associated with Coagulopathy During Target Temperature Management
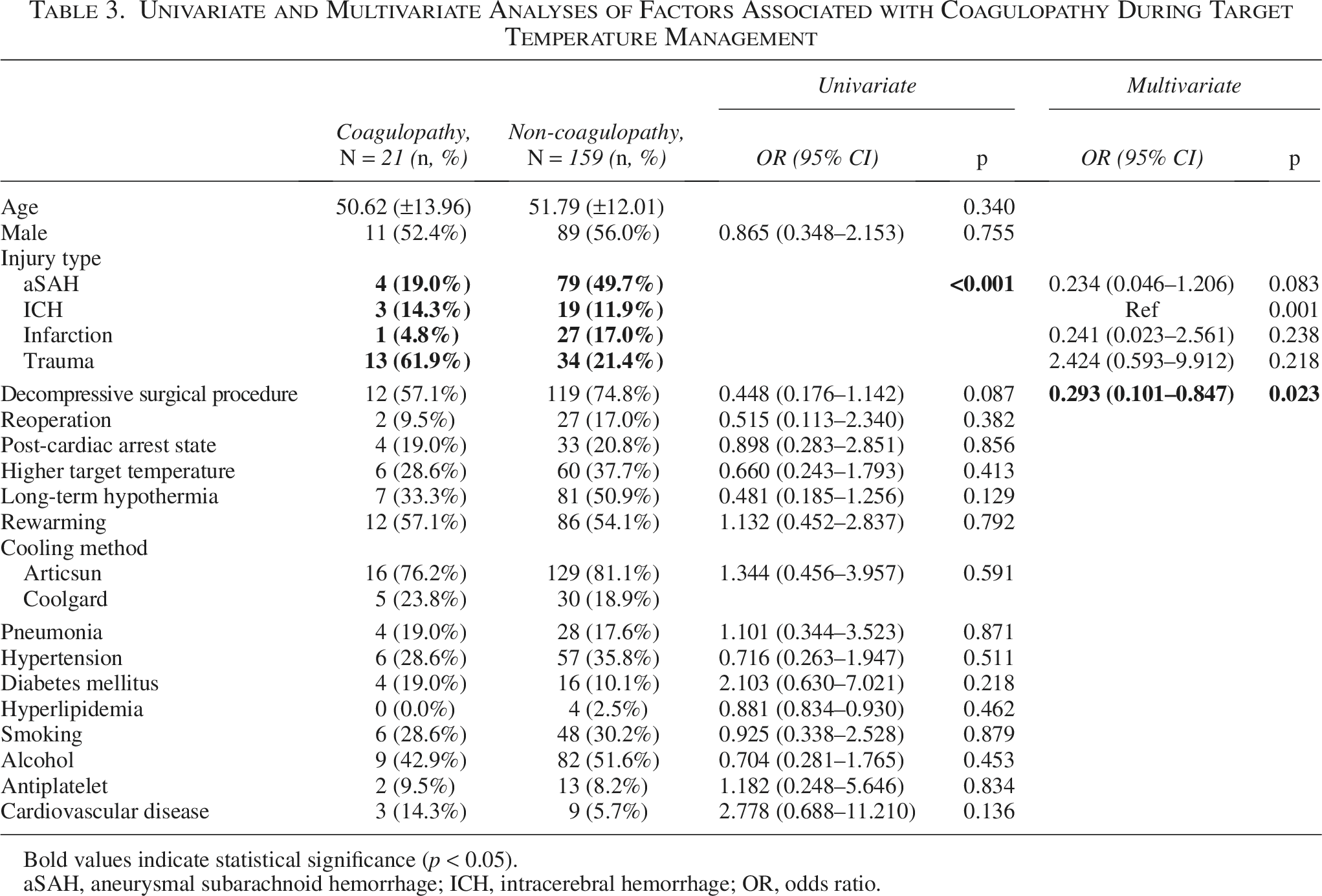
Bold values indicate statistical significance (p < 0.05).
aSAH, aneurysmal subarachnoid hemorrhage; ICH, intracerebral hemorrhage; OR, odds ratio.
Discussions
TTM has been extensively investigated in various types of acute brain injury with heterogeneous results. In the context of TBI, the effect of TTM remains controversial due to inconsistent results across major randomized trials. Large-scale RCTs in the TBI context, such as the POLAR and Eurotherm3235 trials, have failed to demonstrate significant improvements in survivor functional outcomes (Cooper et al., 2018; Andrews et al., 2015). However, recent re-analyses and meta-analytic reviews have challenged this interpretation, suggesting that TTM may reduce mortality in TBI patients with specific conditions regarding the cooling index (Olah et al., 2021). Similarly, previous studies in aSAH have not established a clear benefit of therapeutic hypothermia, despite theoretical neuroprotective mechanisms. Although TTM in aSAH has failed to demonstrate significant improvement in mortality of functional outcomes in several studies, it has been shown to be beneficial in reducing the incidence of vasospasm and delayed cerebral ischemia (Lee et al., 2024; Won et al., 2022). In contrast, acute ischemic stroke represents a more favorable setting for TTM. Several trials, including the ICTuS-L and EuroHYP-1, have demonstrated that therapeutic hypothermia is feasible and may reduce infarct size, cerebral edema, and reperfusion injury (Lyden et al., 2005; Van Der Worp et al., 2019). In a meta-analysis by Huang et al., therapeutic hypothermia administered in conjugation with mechanical thrombectomy for ischemic stroke was associated with improved 3-month functional outcomes (Huang et al., 2023). However, the study found no significant association with mortality reduction or complication rates. Similarly, other meta-analyses have largely failed to demonstrate consistent improvements in either mortality or neurological outcomes (Wan et al., 2014; Kuczynski et al., 2020).
In the present study, which retrospectively analyzed 180 acute brain injury cases of the neurosurgery department treated with TTM, several significant findings were observed. The overall in-hospital mortality was 43.3%. Injury type was significantly associated with in-hospital mortality in the univariable analysis, indicating that the risk of mortality varies depending on the underlying etiology of brain injury. This result highlights the need to tailor TTM based on the underlying pathophysiological mechanisms of secondary brain injury in different patient populations. Decompressive surgical procedure and rewarming appeared to be protective factors against in-hospital mortality in univariate analysis. However, they did not remain as independent predictors in the final multivariable model. This finding likely reflects treatment selection and survival bias, as decompressive surgery and rewarming protocol are typically performed in patients who survive long enough to undergo surgical intervention and rewarming protocol (Karibe et al., 2014; Mraček et al., 2021). Multivariable analysis revealed that post-cardiac arrest state, long-term hypothermia, and coagulopathy were independently associated with mortality. Among 37 patients who presented in a post-cardiac arrest state, 31 (83.8%) were aSAH patients, while 4 (10.8%) had TBI and 2 (5.4%) had ICH. The association between post-cardiac arrest state and increased in-hospital mortality has been well established in previous studies (Khan et al., 2023; Ridwan and Kristof, 2019). Interestingly, long-term hypothermia (≥6 days) was associated with a significantly lower risk of mortality, suggesting a potential benefit from extended TTM duration.
The sensitivity analysis excluding patients with post-cardiac arrest state, provided additional insight into the robustness of the observed associations. In the sensitivity analysis, long-term hypothermia and the development of coagulopathy remained significantly associated with in-hospital mortality, suggesting that these findings were not solely driven by the inclusion of patients with cardiac arrest. Importantly, although long-term hypothermia remained significantly associated with lower mortality in the sensitivity analysis and was not associated with a higher incidence of coagulopathy in the primary cohort, these findings should be interpreted with caution given the potential for survivorship bias inherent to the observational design. The prolonged duration of TTM in this cohort was not protocol-driven but rather reflected ongoing clinical necessity, such as refractory intracranial hypertension or persistent cerebral edema. Therefore, long-term hypothermia in this study should not be interpreted as a causal protective intervention but rather as a surrogate marker of patients who survived the early critical phase and were deemed clinically stable enough to continue temperature modulation. This inherent survivorship and indication bias limits causal inference, and prospective studies are required to better clarify the safety of extended temperature management. As most previous RCTs limited TTM to 24–72 hours, the present findings may provide a rationale for further investigation of extended TTM protocols in carefully selected patient populations (Montaldo et al., 2024; Lyden et al., 2005; Cooper et al., 2018). As coagulopathy during TTM emerged as a critical complication, univariable, and multivariable analyses of factors associated with coagulopathy during TTM were conducted, which revealed a significant difference in incidence according to injury subtype. Notably, its incidence was significantly higher in patients with TBI, accounting for 13 out of 21 cases (61.9%). The predominance of coagulopathy in TBI patients suggests trauma-related systemic pathophysiology may play an important role in the development of coagulation abnormalities observed during TTM. Trauma-induced coagulopathy, characterized by early dysregulation of the coagulation pathway due to tissue injury, shock, and inflammatory responses, is a well-established determinant of poor outcomes in trauma patients. In this context, hypothermia may potentially contribute to coagulation abnormalities rather than acting as the primary cause. This may help explain why TBI patients in prior studies tended to have poorer outcomes with TTM (Cooper et al., 2018; Andrews et al., 2015; Olah et al., 2021). This distinction is clinically important, as it indicates that coagulopathy was observed during TTM should be interpreted within the broader framework of injury-specific physiology, particularly in TBI patients (Kornblith et al., 2019). In multivariable analysis, the significantly lower rate of coagulopathy observed in patients who received decompressive surgical procedures. However, this finding should be interpreted cautiously and should not be considered evidence of a protective effect of surgery. A more plausible explanation is the presence of reverse causation and selection bias. In clinical practice, patients presenting with significant coagulation abnormalities may be less likely to undergo decompressive surgical procedures due to concerns about perioperative bleeding risk. Therefore, the observed association likely reflects underlying clinical decision-making rather than a mechanistic protective effect of decompressive surgery. Another important consideration is the definition of coagulopathy used in this study. In the present analysis, coagulopathy was defined as an INR ≥1.5 at any point during the TTM period, which was selected as a pragmatic indicator of clinically relevant coagulation abnormality in a retrospective cohort. However, this simplified definition does not capture the full spectrum of coagulation disturbances that may occur in critically ill patients. In particular, detailed hemostatic parameters such as baseline coagulation status, platelet count, fibrinogen levels, activated partial thromboplastin time, transfusion exposure, or perioperative bleeding were not systematically available across the entire study period. Therefore, the observed association between coagulopathy and mortality should be interpreted cautiously. Future prospective studies incorporating more comprehensive hemostatic variables and baseline coagulation profiles will be necessary to better clarify the relationship between TTM and coagulation abnormalities in acute brain injury. Injury subtype remained in the final multivariable model as a covariate based on the variable selection process of the regression analysis. Although it did not reach statistical significance after adjustment, its inclusion reflects the underlying heterogeneity of the study population and its potential confounding effect on in-hospital mortality. Given the well-known differences in baseline severity, systemic responses, and mortality risk across acute brain injury etiologies, the persistence of injury subtype in the model suggests that outcome interpretation should account for etiological diversity, even when statistical significance is attenuated after multivariable adjustment. Although these results are preliminary and observational, they offer important insight for real-world application of TTM and its relationship with in-hospital mortalities and complications. The findings of this study offer valuable insights to help decision-making in the absence of standardized TTM protocols for acute brain injury patients. However, rather than applying uniform indications, it is crucial to tailor TTM strategies to the individual clinical context of each patient. In addition, given the heterogeneity of acute brain injury etiologies included in this cohort, the findings of this study should be interpreted as exploratory observations reflecting real-world clinical practice rather than definitive causal effects.
Limitations
This study has several limitations. First, as a retrospective observational analysis, the statistical associations identified do not imply causal relationships between the variables and in-hospital mortality. Furthermore, as with most retrospective studies, the potential for selection bias and unmeasured confounding cannot be entirely excluded. Second, although injury type was included in the analysis, we were unable to control or directly compare the initial severity of brain injury across different etiologies (e.g., aSAH, TBI, ICH, and infarction), which may have influenced both treatment decisions and outcomes. Third, this study focused on in-hospital mortality and did not assess long-term functional outcomes. Therefore, the prognostic impact of TTM on functional status remains unclear in this cohort. Prospective, controlled studies will be necessary to validate these findings and clarify the optimal indication of TTM in acute brain injury patients.
Conclusion
This retrospective real-world analysis demonstrated that coagulopathy during TTM and a post-cardiac arrest state were significantly associated with increased in-hospital mortality in patients with acute brain injury. The occurrence of coagulopathy during TTM was most prevalent among patients with TBI, suggesting that injury-specific pathophysiology may contribute to this complication. Prolonged TTM duration (≥6 days) was associated with lower in-hospital mortality in this cohort; however, this observation should be interpreted cautiously given the potential for survivorship bias inherent to the study design. Overall, these findings highlight the heterogeneity of TTM application across different acute brain injury subtypes and suggest that clinical context and underlying injury characteristics should be considered when applying TTM in neurocritical care practice.
Authors’ Contributions
Y.J.L.: Conceptualization, data curation, formal analysis, investigation, methodology, visualization, and original draft. J.S.: Formal analysis, validation, and review and editing. Y.C.L.: Conceptualization, methodology, supervision, and review and editing.
Footnotes
Acknowledgments
This article complies with all instructions to authors, and the final article was approved by all authors. This article has not been published elsewhere and is not under consideration by another journal.
Ethics Declarations
This retrospective study was approved by the Institutional Review Board of the Ajou University School of Medicine, and the requirement of informed consent was waived due to the retrospective design of the study and the use of anonymized clinical data.
Author Disclosure Statement
All authors have no conflicts of interests to declare.
Funding Information
No funding was received for this article.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.