
Abstract
Purpose:
Anti-Mullerian hormone (AMH) is a surrogate measure to assess ovarian reserve in childhood cancer survivors, but consensus is lacking on when to obtain and how to use AMH data.
Methods:
Pediatric and adolescent committee (PAC) members of the Oncofertility Consortium were invited by email to complete a survey regarding ovarian reserve surveillance and their use of AMH. Responses were collected through REDCap, and results were stratified by specialty: pediatric oncology and endocrinology (PED) or adult/pediatric gynecology and reproductive endocrinology (GYN). Descriptive statistics and Fisher’s exact tests were used for analysis using SAS v9.4.
Results:
Surveys were completed by 48 of 123 eligible PAC members (28 PED, 19 GYN, response rate 39%). The majority (83.3%) reported using AMH as a measure of ovarian reserve, with the earliest timepoint to begin AMH surveillance to be 12–23 months from therapy completion (63%). While most respondents felt the benefits of testing outweighed the limitations (78.7%), commonly reported limitations included variability of results (60.4%) and lack of standardization in use of AMH (52.1%). Differences between PED and GYN respondents included how AMH was used among their clinical practice and the timing of laboratory evaluation.
Conclusions:
Most respondents indicated they used AMH; however, practices in its application varied depending on specialty backgrounds. Evidence-based clinical practice guidelines would improve the standardization of surveillance and counseling and prevent missed opportunities for fertility preservation in survivorship.
Introduction
Five-year survival rates for childhood cancers have increased to over 80%, resulting in an expanding population of adult survivors experiencing long-term effects from cancer and its treatment. 1 In females, these sequelae include effects on the reproductive system and fertility. Compared to sibling controls, female survivors of childhood cancers in the Childhood Cancer Survivor Study had a decreased likelihood of pregnancy, 2 and an increased risk of clinical infertility. 3 This was associated with increasing doses of radiation to the ovaries and alkylating agent chemotherapy. 3 These therapies are thought to deplete the primordial follicle pool, resulting in diminished ovarian reserve (DOR) and an increased risk of premature ovarian insufficiency (POI).4–6 Childhood cancer survivors have commonly cited fertility and reproductive concerns as a health worry, with a lack of adequate information on this topic as an often-unmet need, and many want to know their fertility status, presenting potential utility for ovarian reserve testing.7–9
Previously, estimating reproductive potential relied on menstrual history and measurement of estradiol, follicle-stimulating hormone (FSH), and luteinizing hormone. Alterations in these measurements are late markers of reduced ovarian reserve and ovarian dysfunction, and once identified, individuals may have limited options for biological children. 10 To assist with timely reproductive counseling for female cancer survivors, an earlier measure of ovarian reserve is needed. Anti-Mullerian hormone (AMH), produced by ovarian granulosa cells surrounding growing antral follicles, 11 has been shown to be a measure of ovarian reserve in the general population and in female cancer survivors.12,13 AMH is decreased among survivors who have received gonadotoxic therapies regardless of pubertal status. 14 While AMH is recognized as one measure of ovarian reserve, 15 there is a lack of evidence linking DOR as measured by AMH to future outcomes. Specifically, evidence is lacking to be able to say a single AMH value from adolescence and young adulthood predicts the future ability to conceive a pregnancy or age at menopause.
While AMH screening can be used for assessing ovarian reserve in the female childhood cancer population, current literature is lacking regarding from whom to obtain AMH, when, and whether repeated screening is useful. 16 Current surveillance guidelines by the Children’s Oncology Group recommend evaluating ovarian function through hormone (FSH, estradiol) testing; however, do not currently recommend standardized AMH testing due to a lack of evidence linking AMH directly to infertility. 17 The International Guideline Harmonization Group (IGHG) has not harmonized DOR guidelines; however, for POI, they report AMH testing may be reasonable to be used in conjunction with estradiol and FSH. 18 Treatment-related infertility is a difficult outcome to ascertain in pediatric patients given the typical time delay from the end of therapy to the start of family building and the difficulty in gathering self-reported data from patients who have transitioned out of the pediatric health care system. Waiting until these data are available to inform recommendations may result in a large cohort of survivors unable to access post-treatment fertility preservation and biological parenthood.
Understanding the risk factors for infertility and the natural history of reproductive concerns is necessary for appropriate counseling of childhood cancer survivors, but also for decision-making regarding fertility preservation and pursuit of fertility treatments after the completion of therapy. This highlights a growing need for standardized practice in long-term follow-up programs to address the oncofertility needs of survivors.19,20 Here, we evaluate current use of AMH in pediatric cancer survivors to better inform future guidelines for oncofertility practitioners.
Materials and Methods
In this study, we surveyed members of the Pediatric and Adolescent Committee (PAC) (formerly the Pediatric Initiative Network [PIN]) of the Oncofertility Consortium, an international, interdisciplinary network of clinicians and researchers, to inquire about current practices of AMH screening in the female childhood cancer survivor population. The goals of this study were to (1) examine current practices and perspectives regarding the use of AMH as a surveillance tool in pediatric and adolescent cancer survivors, and (2) identify potential differences in practice patterns/perspectives between clinicians working in survivorship clinics (pediatrics trained) versus reproductive health specialists (trained in obstetrics/gynecology [GYN]).
Survey development
Survey questions were developed by a multidisciplinary group of experts from the Oncofertility Consortium. The survey consisted of 32 questions and used mixed formatting including multiple choice, rank order, and Likert-scale of agreement (Supplementary Data). We asked participants to answer questions in relation to their practice for pediatric, adolescent, and young adult survivors. The questions were modified from existing literature or created by a multidisciplinary panel of providers who routinely provide care for this population of patients. Broad survey themes included personal and institutional demographics, specific use of AMH (including timing and frequency of obtaining AMH levels), and general approach to testing ovarian reserve (including AMH and other laboratory or imaging tests and patient or treatment factors that may affect the likelihood of assessing ovarian reserve for individual patients). The survey was created with the use of REDcap. Prior to distribution, the survey was assessed by two pediatric oncologists and one pediatric endocrinologist and met criteria for face validity. The survey was also ß tested outside the research group for usability and to ensure the length and language were appropriate. The survey took between 5 and 10 minutes to complete. This study was approved by the IRB at St. Jude Children’s Research Hospital.
Survey distribution
All PAC members of the Oncofertility Consortium were invited to complete the survey. The PAC is an international group of health care providers and researchers from various specialties, including reproductive endocrinology and infertility, oncology, endocrinology, and urology. On March 22, 2021, members of the PAC were invited by email to complete the internet-based survey. Reminders to complete the survey were sent four times (4/6/21, 4/19/21, 5/3/21, and 6/28/21) prior to inactivation of the survey on July 13, 2021.
Statistical analysis
Descriptive statistics and Fisher’s exact tests were obtained using SAS v9.4. We summarized provider characteristics using summary statistics. Respondent count and proportion were calculated based on total respondents per question, and the number skipping a question was not included in the denominator. As answers to the questions in the survey were predominantly categorical, no imputation was used. To better understand the difference in practice patterns among clinicians who perform surveillance for ovarian dysfunction compared with those who receive consults for DOR, participants were stratified by their training/discipline. Those who are initially obtaining surveillance AMH are typically working in survivor clinics and are in subspecialties requiring pediatric-specific training (e.g., oncology or endocrinology) and formed the PED group of survey respondents. The group likely to receive a consult for evaluation for DOR have GYN-specific training (e.g., reproductive endocrinology and infertility [REI] or pediatric and adolescent GYN) and formed the GYN group of survey respondents.
Results
Participant and institutional demographics
At the time of survey distribution, there were 128 members with distinct email addresses as part of the PAC listserv. Of those, five members were not eligible due to involvement in the survey creation, leaving 123 eligible members (Consort diagram, Supplementary Fig. S1). We received 51 responses, of which 3 members had answered twice, and only their first submission was retained for data analysis, leaving a total of 48 individual responses for a response rate of 39%.
Respondents were divided based on their specialty training. Over half of respondents (58.3%) identified with a pediatric (PED) specialty (24 oncology and 4 endocrinology; n = 28), while 19 respondents (41.7%) were GYN trained (1 obstetrics and GYN, 9 pediatric and adolescent GYN, and 9 reproductive endocrinology and infertility [REI]) (Table 1). One individual described their specialty as “other,” did not fit in either the PED or GYN group, and was not included in analysis. Overall, 60.4% of the respondents were physicians, 22.9% were advanced practice providers, and 10.4% were nurses. The distribution of provider type was significantly different between the PED and GYN groups (p = 0.02). The distribution of years working in fertility assessments was not significantly different between PED and GYN groups. However, over half of all respondents (56.3%) had worked in fertility assessment for ≤5 years (56.3%) (Table 1). The PED groups responded that they mostly took care of pediatric or adolescent and young adult patients (78.5%) compared with the GYN group (52.7%). The GYN group described their fertility practice as being mostly adult or a 50/50 split (47.4%), with the difference in age of the population seen being significantly different (p = 0.03). While preservation consults pre- and post-cancer therapy and fertility status assessments were the most reported roles, PED respondents were less likely than GYN to report participation in all three areas (Table 1).
Participant Demographics of Oncofertility PAC Members Respondents
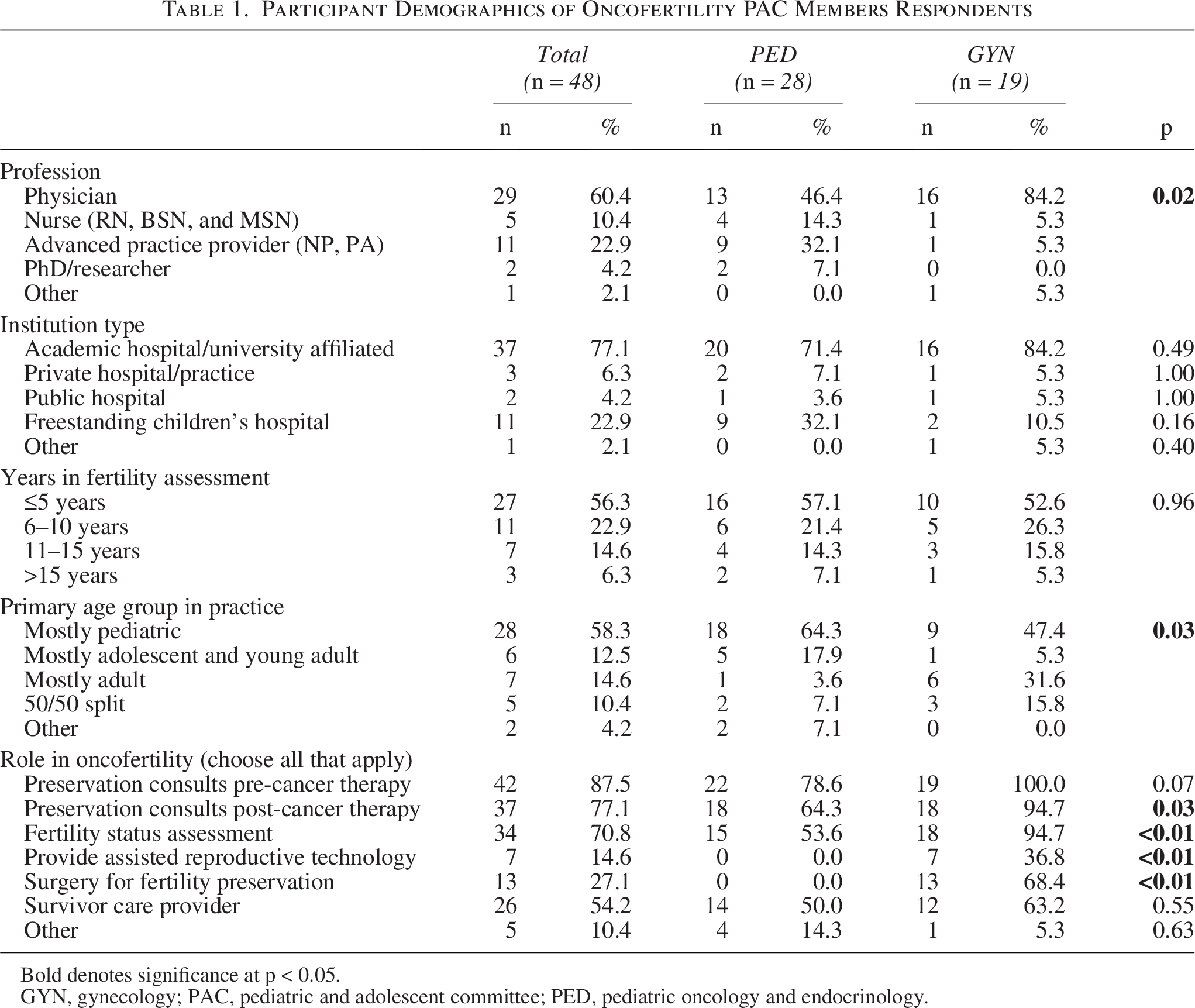
Bold denotes significance at p < 0.05.
GYN, gynecology; PAC, pediatric and adolescent committee; PED, pediatric oncology and endocrinology.
The use of AMH in clinical practice
Respondents reported several ways they utilize AMH in their practice. Overall, the most common uses reported were as a measure of ovarian reserve (83.3%), to track ovarian reserve over time to identify declines (72.9%), to support the likelihood of developing POI (60.4%), and to assist with decisions to refer to reproductive specialists, such as reproductive endocrinology (60.4%) (Table 2). Importantly, there were no respondents who reported that we should not use AMH. There were no significant differences between the GYN and PED groups except in the use to predict response to ovarian stimulation (overall 35.4%; GYN 68.4% vs. PED 14.3%; p < 0.05) (Table 2). The most common time to begin AMH surveillance was 12–23 months post-therapy, suggested by 63% of respondents (GYN 63.2% vs. PED 61.5%) (Table 2). Those from the GYN specialties were significantly more likely to obtain AMH levels annually than PED specialties (68.4% vs. 35.7%; p = 0.04), and monitoring until two or three values are stable (26.3% vs. 3.6%; p = 0.03) (Table 2).
Attitudes toward AMH Measurements in Female Childhood Cancer Survivors and Patterns of Use
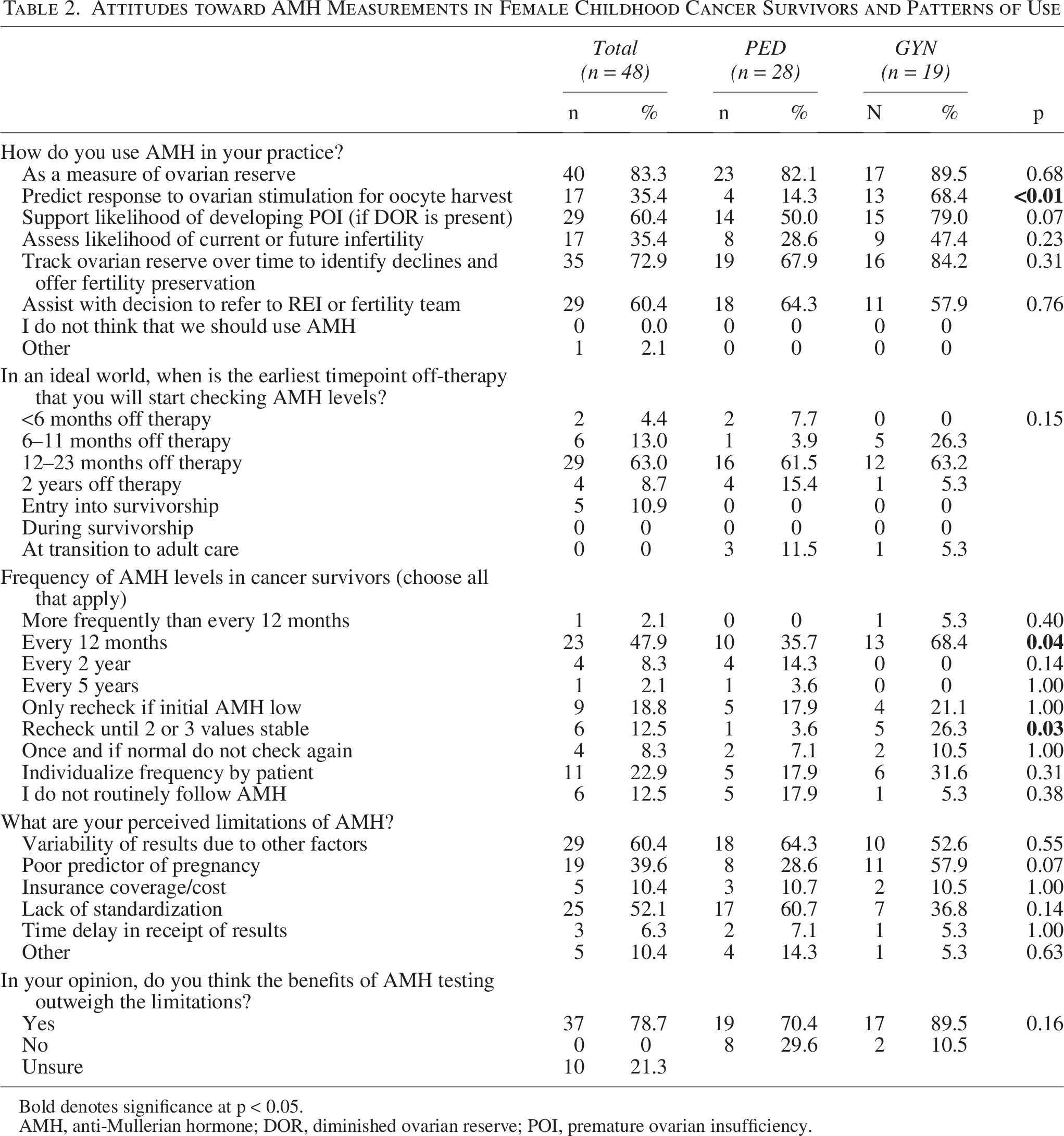
Bold denotes significance at p < 0.05.
AMH, anti-Mullerian hormone; DOR, diminished ovarian reserve; POI, premature ovarian insufficiency.
Both groups identified several limitations of AMH, including AMH being a poor predictor of pregnancy (39.6%), lack of standardization (52.1%), and variability in values due to other factors (60.4%). However, most practitioners stated that the benefits of AMH testing outweigh those limitations (78.7%) (Table 2).
Measuring ovarian reserve in female pediatric cancer survivors
No respondents evaluated ovarian reserve while patients were receiving cancer-directed therapy, and the majority (54.4%) report 12–23 months after therapy as the earliest timepoint to begin checking ovarian reserve (Table 3). When asked which test(s) are used to evaluate ovarian reserve (choose all that apply), in pre-pubertal patients the most common test used was AMH in 56.3% of respondents, and in post-pubertal patients the most common test was AMH (95.8%), followed by FSH (81%). AMH was reported as the “best test” for evaluating ovarian reserve in 47.8% of pre-pubertal patients and in 60.9% of post-pubertal patients.
Measuring Ovarian Reserve in Female Childhood Cancer Survivors
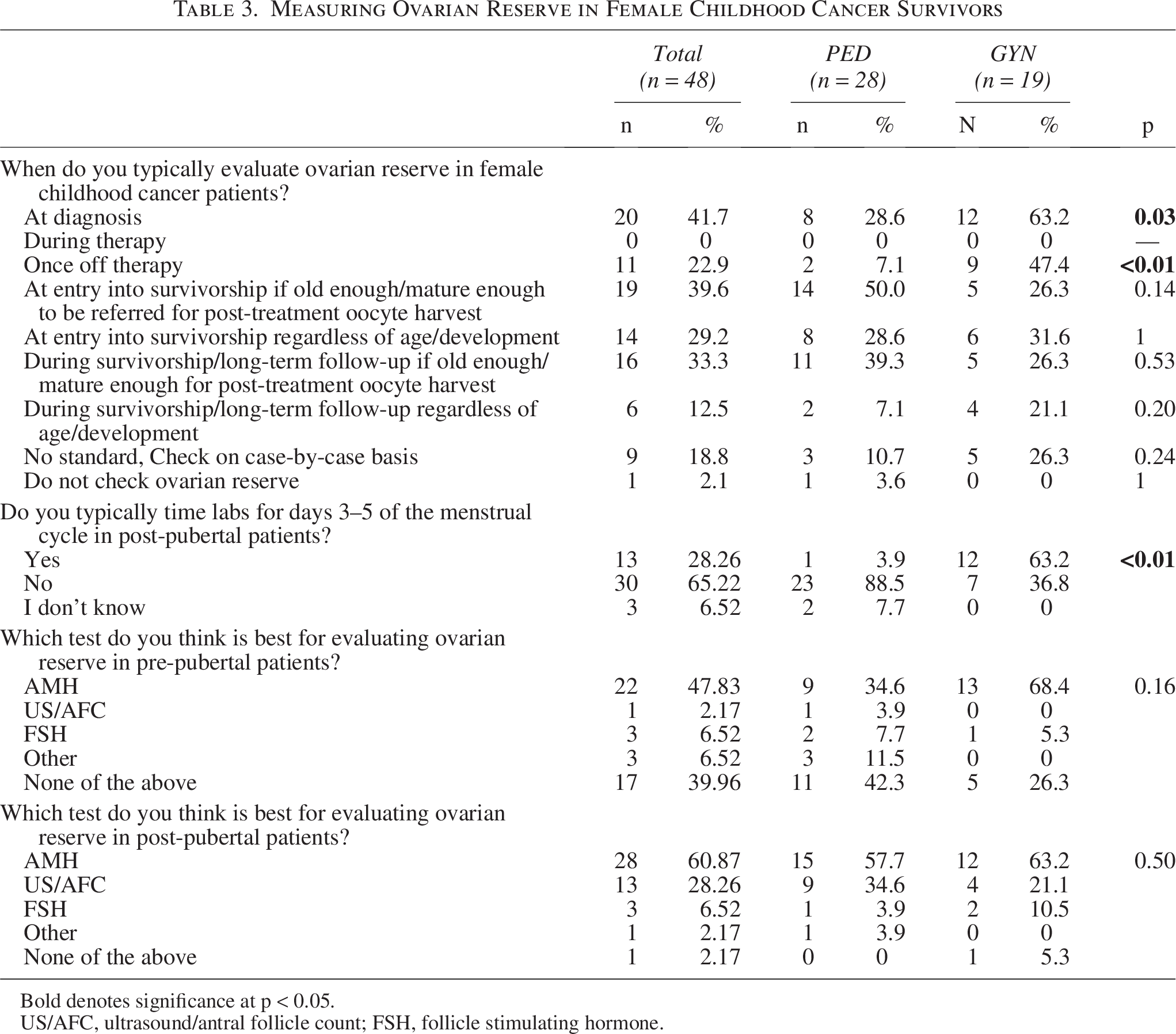
Bold denotes significance at p < 0.05.
US/AFC, ultrasound/antral follicle count; FSH, follicle stimulating hormone.
GYN respondents were more likely than PED respondents to report evaluating ovarian reserve both at diagnosis (63.2% vs. 28.6%; p = 0.03) and once off therapy (47.4% vs. 7.1%; p = 0.003), as well as using AMH in pre-pubertal patients (79.0% vs. 39.3%; p = 0.009) and ultrasound/antral follicle count (US/AFC) in both pre- (21.1% vs. 0%; p = 0.02) and post-pubertal patients (47.4% vs. 14.3%; p = 0.02). Another difference between GYN and PED responses included the timing of lab evaluation. GYN respondents were significantly more likely to time labs for days 3–5 of the menstrual cycle in post-pubertal patients (63.2% vs. 3.9%; p < 0.05) compared with PED (Table 3).
Ovarian reserve assessment by treatment modality and risk stratification
Respondents were asked their likelihood of completing ovarian reserve assessments based on different cancer treatment modalities and doses, corresponding to levels of increased risk by the Oncofertility PAC risk stratification (Table 4). 21 Overall, most respondents reported that treatment factors aligning with a significant or high risk for gonadotoxicity would make them more likely to complete an ovarian reserve assessment, including a history of bone marrow transplant (BMT), high doses of alkylating agent therapy, and a history of pelvic radiation.
Treatment Related Factors More Likely to Affect the Likelihood of Completing an Assessment of Ovarian Reserve
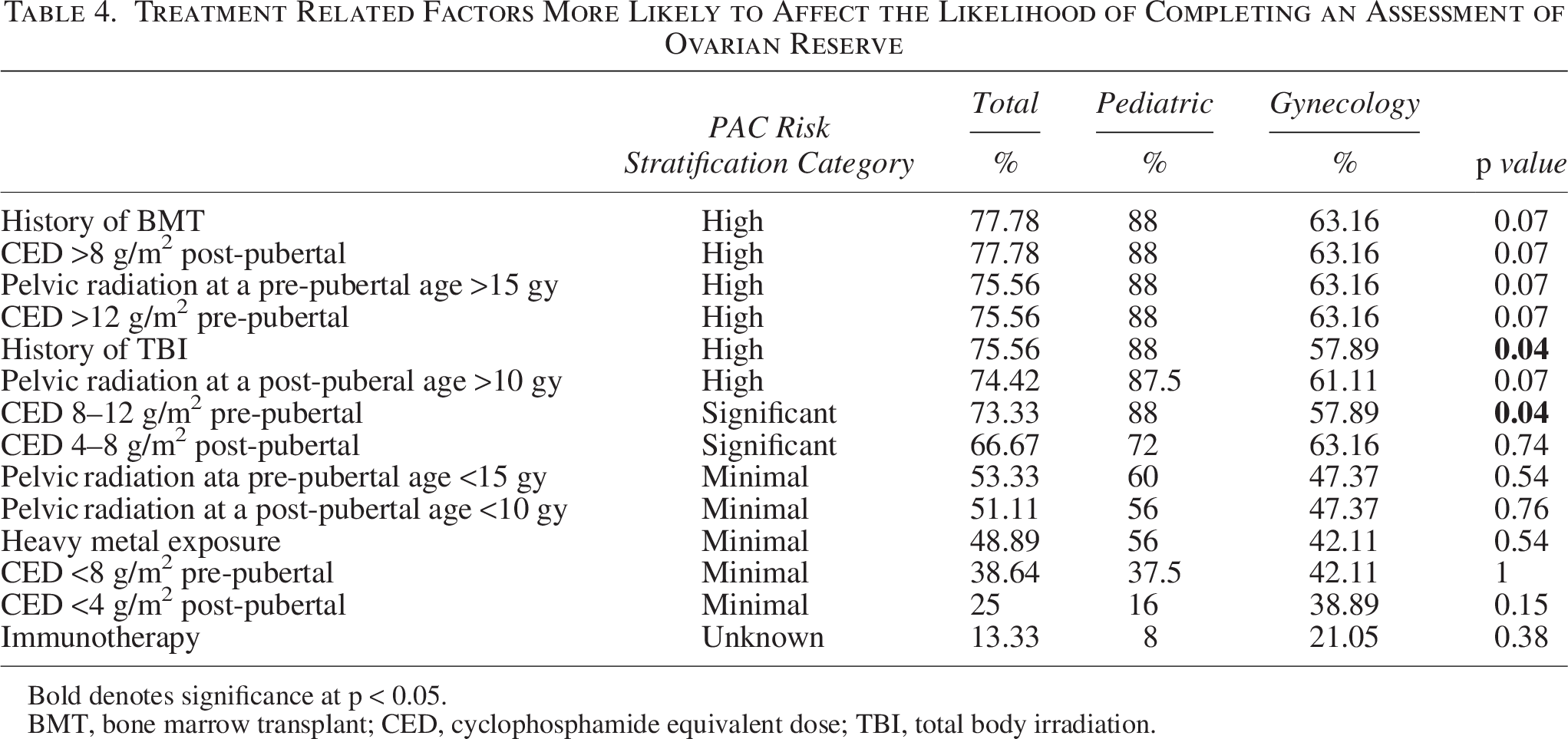
Bold denotes significance at p < 0.05.
BMT, bone marrow transplant; CED, cyclophosphamide equivalent dose; TBI, total body irradiation.
Discussion
In this study, members of the Oncofertility Consortium PAC were surveyed regarding attitudes and uses of AMH in evaluating gonadotoxicity among female childhood cancer survivors. Overall, oncofertility professionals reported AMH was the best test to evaluate ovarian reserve in post-pubertal cancer survivors. Both groups of specialists reported limitations in the use of AMH, specifically variability of results and the lack of standardization/guidelines around AMH use. Despite these, oncofertility providers report that AMH testing is generally valuable in their practice and is helpful in identifying pre-POI states of ovarian dysfunction. In general, there was consensus that AMH should not be obtained earlier than 12 months off therapy. This is likely secondary to evidence showing that AMH levels are suppressed during cancer therapy, and recovery may take up to 1–2 years off therapy.22,23 Several studies have reported AMH values in childhood cancer survivors,14,15,24–29 many of which show reduced AMH values compared with controls or pre-treatment values. In addition, AMH values are not static but can fluctuate after cancer treatment and show progressive decline overtime.23,29
There were, however, differences between the PED and GYN groups. Differences in timing of obtaining AMH among GYN respondents, including both pre-therapy and once immediately off therapy, may be reflective of their use of AMH in determining feasibility of fertility preservation techniques. This contrasts with PED providers who may be more aware of the lag in AMH recovery post-therapy and are typically providing surveillance to identify patients to refer to GYN specialists. One trend noted between PED and GYN providers was their difference in adherence to current published risk stratification levels and how it guides the likelihood of completing ovarian reserve assessments. 21 GYN practitioners were significantly less likely to obtain ovarian reserve assessments for patients who had a history of total body irradiation (TBI), a high-risk feature. There was also a trend toward significance in differences in surveillance after all other high-risk treatment factors, including high levels of both alkylating agents and pelvic radiation (Table 4). It is not clear whether GYN practitioners are not systematically recognizing these treatment factors as high risk, or if the difference lies in the fact that GYN practitioners may be more likely to obtain ovarian reserve assessments on any referred patients, regardless of the patient’s prior therapy.
Differences between PED and GYN responses highlight the importance of which lens oncofertility practitioners are looking through when evaluating patients. Different subspecialties often fill different roles in an oncofertility program. 19 Pediatric oncologists and endocrinologists are more likely to be involved in primary surveillance for ovarian dysfunction as part of a survivor clinic. Survivor clinics provide surveillance for myriad late effects affecting many organ systems with an ever-mindful eye on evidence-based practice and cost-effectiveness. Reproductive endocrinologists/gynecologists are more typically recipients of referrals from survivor clinics, seeing patients who present for post-treatment fertility evaluations and preservation, sometimes, too late for intervention. In this model, survivor clinics and practitioners generally act as the gatekeepers to specialized fertility care. It is important to develop standards to ensure equitable care and timely referral while intervention is possible, as these patients may have reduced success compared with other patients requiring assisted reproductive technology. 30
In the Children’s Oncology Group (COG) long-term follow-up guidelines, there is currently no standard recommendation for AMH testing. 17 AMH is listed under potential considerations for further testing of DOR or infertility; however, there is no specific guidance on when, or how often, to obtain testing. 17 This lack of clear guidance reflects gaps in current knowledge, as well as challenges in studying reduced ovarian reserve and its impact on fertility potential among female childhood cancer survivors. A more comprehensive understanding of fertility outcomes, including rates of infertility, requires the collection of long-term data. Due to difficulties in obtaining long-term self-reported and laboratory evidence, we are left with surrogate measures, such as AMH, to best predict patients who have developed or are at risk of DOR. In our survey, both clinician groups reported checking AMH 12–23 months off therapy and would not recommend initiating AMH testing until at least 12 months post-therapy. Once a baseline had been established, the most reported interval was annual AMH testing across both PED and GYN groups. Surveillance strategies may be best targeted to those patients who received therapy conferring significantly increased, or a high level of increased risk based on our current understanding of gonadotoxic therapy. 21
While there was some consensus in this survey regarding timing and frequency of AMH testing for female pediatric survivors at risk for adverse fertility outcomes, fertility evaluations may be appropriate for any patients with concerns or questions regarding their fertility, as fertility-related distress is common among cancer survivors across oncology treatment time points. 31 Alternatively, there may be patients who may not be interested in fertility evaluations at the proposed timepoints above or who may find fertility evaluations to be distressing. Shared decision-making, a tenant of high-quality fertility care, should be employed to determine the timing and schedule of any fertility evaluations, allowing for informed decision-making regarding options for post-treatment fertility preservation and family building. 32
While the PAC represents the largest group of global pediatric oncofertility experts, participation was a limitation in our study with only a 39% response rate. Given our small sample size, we were limited in controlling for certain variables, including specific training, type of institution, or years involved in oncofertility practice. Our data emphasize differences in the approach to AMH testing in the survivor setting, where detection of ovarian damage and the need for ongoing surveillance are weighed against the costs of overtesting, compared with a GYN/fertility setting, where patients are referred from survivor clinics based on prior testing or specific concerns. However, the lack of a standardized approach may result in missed opportunities for fertility preservation or biological parenthood. It is important to note that this survey was completed among practitioners knowledgeable and familiar with gonadotoxic therapy and fertility testing. It is likely that responses regarding the utilization of AMH as a screening tool would be more varied among a group of general survivorship practitioners. While more research should be done in this area to develop practice guidelines to increase standardization, patient or family request should be the most important factor for completing testing or referring for fertility evaluation. Given the current lack of clear guidance regarding AMH surveillance, we plan to harness Delphi methodology to develop a consensus opinion surrounding AMH use in female childhood cancer survivors among experts in the field. Other groups, such as the IGHG, are addressing the use of AMH in other aspects of care, including in updating guidelines for premature ovarian reserve. 18 We hope research regarding how AMH values in survivorship correlate with long-term fertility and reproductive outcomes is ongoing to better inform future clinical practice.
Conclusions
Among members in the Oncofertility Consortium PAC, AMH is the most used test to evaluate DOR. Respondents recommend obtaining levels no earlier than 12 months after the end of cancer therapy and support annual testing. This may be particularly warranted for patients with abnormal AMH levels or for those at the highest levels of risk. Future evidence-based guidelines would improve the standardization of surveillance and counseling and prevent missed opportunities for reproductive health counseling as well as fertility preservation in survivorship.
Authors’ Contributions
K.B.: Conceptualization, methodology, formal analysis, writing—original draft preparation. A.C. and J.R.: Conceptualization, methodology, conceptualization, writing—review and editing. A.A., J.L., C.Y., and L.N.: Conceptualization and writing—review and editing. L.M.: Conceptualization, writing—review and editing, and supervision. All authors read and approved the final article.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.