
Abstract

Adolescents and young adults (AYAs) with cancer, defined as individuals 15–39 years of age at diagnosis, are recognized as a distinct group with unique needs related to the intersection of developmental milestones and cancer treatment. Evidence suggests that survivors of AYA cancers experience a significant burden of late effects after cancer treatment, including increased risks of late mortality, chronic health conditions, and secondary malignancies. 1 Care tailored to the unique needs of this group is needed to best optimize health outcomes. 2
Models of survivorship care range from specialized cancer center-based clinics to shared-care models between oncologists and primary care to community-based primary care-led clinics.2,3 Strengths and weaknesses may vary, and access often depends on resources and geographic location. Regardless of the setting, ideally services should be comprehensive, include screening for late effects and subsequent cancers, and provide psychosocial support, educational and vocational services, sexual and reproductive health services, and general health promotion.
This article aims to summarize the relevant guidelines for AYA survivorship care, describe barriers to implementation, and provide potential practical solutions for professionals seeking to establish and/or maintain an AYA-focused survivorship program.
Relevant Guidelines for the Provision of AYA Survivorship Care
There are numerous guidelines relevant to the provision of survivorship care for the AYA population. The National Comprehensive Cancer Network 4 in the United States and Alberta Health Services 5 in Canada are two examples of clinical practice guidelines developed specifically for AYA oncology. The goals of these supportive care guidelines are to increase awareness of the unique issues in AYA oncology, identify available resources, and make recommendations for patient management. They are based on high-quality evidence from the literature and expert consensus. The Children’s Oncology Group (COG) consortium has also developed an extensive evidence- and consensus-based guideline, the Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent, and Young Adult Cancers (COG LTFU Guidelines) 6 These have historically focused on long-term survivors of childhood cancers but have been extended to included adolescents and young adults with cancer. Given the number of available guidelines and variations between them, the International Late Effects of Childhood Cancer Guideline Harmonization Group 7 has established international working groups to create integrated guidelines for the surveillance of health and psychosocial late effects among childhood, adolescent, and young adult cancer survivors.
There is clear consensus across guidelines that optimal survivorship care includes screening, surveillance, and disease prevention based on the individual characteristics and treatment exposures of the survivor, as well as attention to the complex psychosocial needs of AYA survivors based on life stage. At a minimum, survivorship care should include provision of a survivorship care plan detailing treatment exposures (chemotherapy doses, radiation therapy doses and sites, surgical procedures, etc.), possible late effects, and recommendations for risk-based surveillance. Important for all populations, but particularly needed for AYA survivors, is screening for psychosocial outcomes (e.g., school, employment, insurance, finances, and interpersonal relationships), lifestyle behaviors (e.g., physical activity, nutrition, sleep, and substance use), reproductive and sexual health, and coordination of care between primary care providers and subspecialists. AYA survivors incur substantial economic burdens, loss of work, and reductions in health-related quality of life.2,8,9 Intervention studies are needed to address these adverse outcomes for a population with decades of life ahead of them. 8
Under ideal circumstances, AYA survivors would have access to a multidisciplinary team, including primary and subspecialty care as needed, social work, psychology, onco-fertility, vocational counseling, financial navigation services, legal counseling, genetic counseling, nutrition, integrative care services (e.g., acupuncture, massage, and tai chi), and a care coordination navigator. When newly establishing an AYA program, it has been recommended to start small and phase in more services over time. 10 For example, smaller programs or individual providers may offer a consultative model delivering a comprehensive survivorship care plan and referrals for psychosocial and onco-fertility services. More established, multidisciplinary programs embed medical and psychosocial services to tailor referrals based on individual needs and provide ongoing follow-up.
In the United States, the National Standards for Cancer Survivorship Care were recently developed for health care systems to use to guide the development of new survivorship care services or assess the quality of existing services for survivors of any cancer at any age. 11 These new standards detail essential policies and processes for survivorship care delivery and encourage health care systems to target services to meet the unique needs of relevant populations, including AYA survivors. 11
Barriers to Implementing AYA Survivorship Care
Individual, health care system, and policy-level barriers to high-quality, comprehensive AYA survivorship care have been well documented and include the geographic mobility of these survivors, costs of care (including missed work), challenges in establishing and maintaining adequate health insurance coverage, lack of awareness of specific health risks associated with cancer treatment, lack of providers with expertise in survivorship care, the burden of the fragmented health care system, and lack of care coordination.2,12 Common institution-level issues in establishing and maintaining AYA programs include inadequate resources, lack of trained and available staff, lack of dedicated space, insufficient clinical time to address complex needs during patient appointments, and unclear care coordination.10,13–15 Table 1 presents potential strategies for overcoming such challenges.
Institution-Level Barriers to Establishing or Maintaining AYA-Specific Survivorship Care
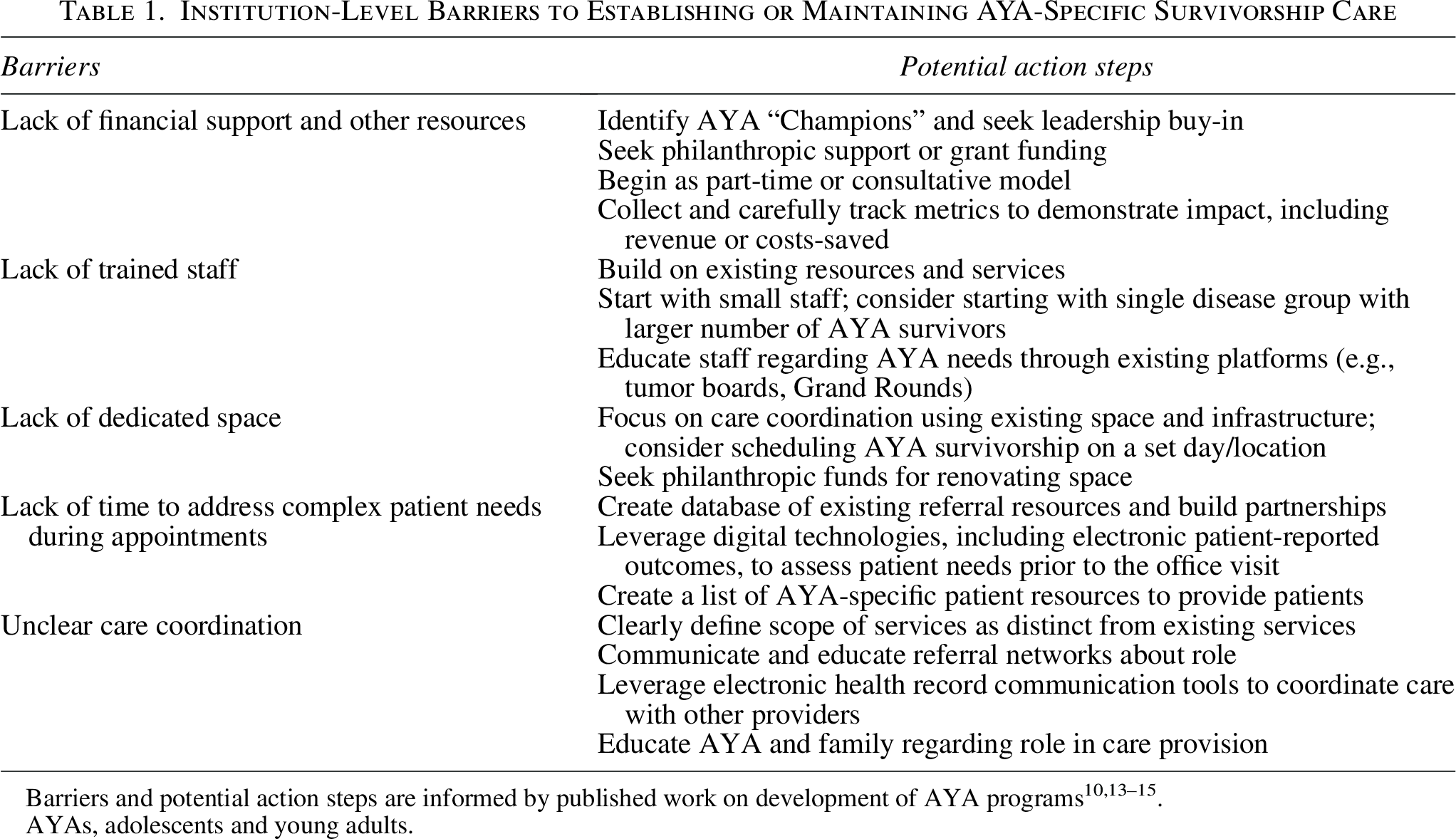
Barriers and potential action steps are informed by published work on development of AYA programs10,13–15.
AYAs, adolescents and young adults.
Conclusions and Future Directions
There is no standard coordinated approach to transition AYA survivors from the end of cancer therapy into long-term survivorship care. While models may differ depending on the resources available at the treating facility and patient preferences and needs, more work is needed to identify effective processes for successfully transitioning care. One critical gap identified in the literature is inconsistent coordination between oncology and primary care providers throughout the cancer trajectory.16,17 Prior to a cancer diagnosis, AYA survivors may not have established routine primary care. Leveraging electronic health record programs and interoperability across systems may help promote more seamless communication among providers during important transition points in care and better serve this mobile population. 18
Future directions include developing a national referral base of qualified health care providers for AYA cancer survivors. Regional networks with telehealth services may also help address access issues for AYA survivors in areas with limited services. Telehealth services are acceptable to AYA survivors and can overcome barriers to attendance and access, though some survivors may prefer in-person services.19,20 Finally, continued work in creating developmentally appropriate patient education materials and digital technologies to promote health care self-management and healthy lifestyles for AYA survivors is needed. Multi-level approaches that address individual, provider, health care system, and policy-level factors are needed to promote optimal survivorship care and enhance outcomes for AYA survivors.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This project was supported by Faculty Affairs and the Department of Psychosocial Services at St. Jude Children’s Research Hospital (SJCRH). Support to SJCRH is provided by the American Lebanese Syrian Associated Charities (ALSAC).