
Abstract

Introduction
Optimizing outcomes for adolescents and young adults (AYAs) with cancer requires significant daily self-management behaviors (i.e., medication adherence, physical activity, and dietary behavior). During active treatment, medication adherence, or medication-taking behavior that aligns with the treatment protocol, 1 is associated with a decreased risk of relapse 2 and death.3,4 Following active treatment, participation in regular physical activity and following dietary guidelines5,6 may decrease an AYA’s risks of second cancers, chronic medical conditions, and mortality. 7 Unfortunately, 21%–60% of AYAs with cancer are non-adherent to treatment protocol medications 8 and less than half of survivors meet physical activity and/or dietary behavior guidelines.9–16 This means that thousands of AYAs receiving active treatment and AYAs who have completed treatment (hereafter collectively referred to as “AYAs with cancer”) are currently at risk for devastating consequences that could be prevented with adequate self-management behaviors.
Guidelines
As a result of the prevalence and implications of adherence and self-management difficulties, adherence and self-management promotion has been recognized as a critical component of clinical care for AYAs with cancer. Specifically, the National Comprehensive Cancer Network (NCCN) AYA Guidelines (developed for patients 15–39 years of age) and the Standards for Psychosocial Care for Children with Cancer and Their Families (developed for patients 0–18 years of age) recommend a multi-step approach to medication adherence promotion including: (1) education; (2) routine and repeated evaluation of adherence and barriers; (3) delivery of interventions matched to the patient’s barriers (e.g., smartphone reminders for patients experiencing forgetting).17,18 To promote optimal self-management, the NCCN AYA Guidelines also recommend that behavioral factors (i.e., tobacco, vaping, alcohol, cannabis, and other substance use, sexual behavior/risks/concerns, nutritional requirements, exercise needs, hobbies and recreational activities, and sleep patterns) be evaluated throughout treatment with education and referrals to appropriate services (e.g., smoking cessation program, registered dietitian-certified specialist in oncology) provided as necessary. 17 Similarly, the Children’s Oncology Group long-term follow-up guidelines for survivors of childhood, adolescent, and young adult cancers (developed for patients diagnosed before 21 years of age) state that “the survivorship care plan should address the contribution of comorbid health conditions, familial and genetic factors, and health behaviors that affect the risk of chronic disease and provide interventions and resources to remediate and prevent late effects of cancer and promote healthy lifestyle behaviors. 19 ”
Barriers, Strategies, and Resources and Recommendations
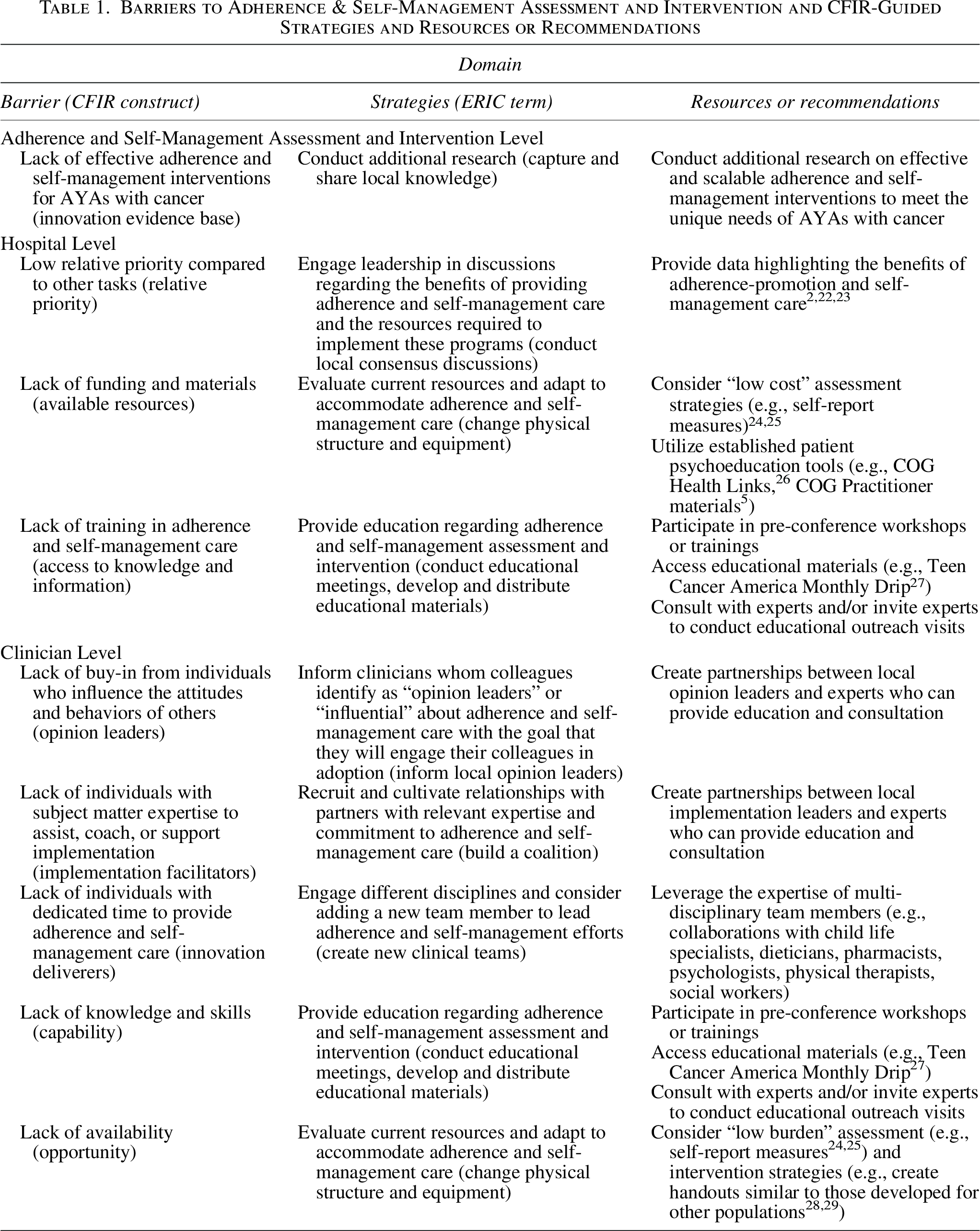
Although the importance of supporting adherence and self-management is increasingly recognized as critical to AYA cancer care, it is likely that many programs have opportunities to improve the quality of adherence and self-management care provided to their patients. 20 While data on barriers to adherence and self-management promotion efforts in AYA oncology are not available, data from psychologists providing adherence-promotion care to children, adolescents, and young adults with multiple medical conditions, 21 our experience, and feedback from our peers highlight several barriers that teams should consider when developing and implementing these services. To contextualize these barriers within the larger implementation science literature, we have categorized them according to Consolidated Framework for Implementation Research (CFIR) constructs as detailed in Column 1 of Table 1. 30 As data on effective strategies to address potential barriers (particularly those faced by older AYAs) are also limited, we used the CFIR-ERIC (Expert Recommendations for Implementing Change) matching tool 31 to identify strategies 32 teams may wish to consider (Column 2) and provide our personal recommendations and available resources to aid teams in executing these strategies (Column 3). Differences across health care systems are likely to result in systems-level barriers and facilitators (e.g., supports, resources [e.g., clinician time, availability of psychosocial providers]) to providing adherence and self-management care that are unique to each practice. As a result, we encourage teams to use this table as a starting point for discussion and generate specific actions that align with their institution’s/team’s characteristics, goals, and resources.
Barriers to Adherence & Self-Management Assessment and Intervention and CFIR-Guided Strategies and Resources or Recommendations
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This project was supported by Faculty Affairs and the Department of Psychosocial Services at St. Jude Children’s Research Hospital (SJCRH). Support to SJCRH is provided by the American Lebanese Syrian Associated Charities (ALSAC). This work was also supported by the philanthropic support of the Vestavia Hills High School RISE Program via the O’Neal Comprehensive Cancer Center.