
Abstract
Purpose:
In hormone therapy for premenopausal breast cancer (BC), gonadotropin-releasing hormone (GnRH) agonist (GnRHa) formulations, especially long-acting formulations, are often used in combination with tamoxifen (TAM). On the other hand, in recent years, endocrine therapy is increasingly interrupted to achieve pregnancy. Here, we examined ovarian function and the timing of resumption of menstruation after the interruption of GnRHa therapy.
Methods:
Fertility preservation patients with BC who visited our hospital between January 2010 and August 2023 and who interrupted endocrine therapy with a GnRHa formulation were included. Information on 22 cases (24 cycles), including two interruptions due to the desire for a second child, was collected from medical records and examined retrospectively.
Results:
Three cases started assisted reproductive technology treatments before menstruation resumed and were excluded from the analysis. Menstruation resumed at approximately 7, 9, and 12 months from the last dose of the 1-, 3-, and 6-month GnRHa formulations, respectively. The long delay of menstruation resumption was presumably caused by the use of (1) the 3-month formulation in the 6 months before the last GnRHa dose, (2) the 6-month formulation in the 12 months before the last dose, and (3) TAM when menstruation resumed.
Conclusions:
In BC patients who may seek pregnancy after interrupting endocrine therapy, it may be easier to estimate the timing of resumption of menstruation if the use of long-term GnRHa depot formulations is avoided for >6 months before the interruption. BC endocrine therapy should be optimized to achieve pregnancy and childbirth as soon as possible during its interruption.
Keywords
Introduction
Breast cancer (BC) is the leading cause of malignant tumor incidence among women in Japan, and focusing on the Adolescent and Young Adult generation, it has been reported that the BC incidence rate by age group begins to increase in the late 20s but is about 10 times higher in the late 30s. 1 In Japan, where women are marrying later and having their first child at an older age, the incidence of BC in the reproductive age has become a problem.
In the treatment of BC, the expression of hormone receptors, namely estrogen receptor (ER) and progesterone receptor (PgR), and human epidermal receptor-2 (HER2), an oncogene and membrane protein involved in cell proliferation, in tumor tissue is important. ER-positive BC accounts for 70% of all BCs, 2 and the premenopausal incidence of estrogen-dependent BC is increasing with the increasing incidence of BC in Japan.3,4 On the other hand, it has also been reported that BC in younger age is often ER-negative, such as only HER2-positive as well as so-called triple-negative BC in which ER, PgR, and HER2 are all negative. 5
The Japanese Breast Cancer Society guidelines recommend the use of tamoxifen (TAM) as endocrine therapy for premenopausal ER-positive BC for at least 5 years. 6 It has been reported that the addition of a gonadotropin-releasing hormone (GnRH) agonist (GnRHa) to TAM significantly improves both disease-free survival (DFS) and overall survival (OS) in the overall population. 7 In patients at high risk of recurrence as defined by clinicopathologic characteristics (age, presence of lymph node metastases, expression of ER or PgR, etc.), the efficacy of combining TAM with a GnRHa formulation has been reported to be promising.8,9
In addition to the 1-month formulation, there are long-term depot formulations of GnRHa, such as 3- and 6-month formulations. There are reports suggesting the safety and efficacy of long-term depot formulations of GnRHa in BC patients, which may improve treatment compliance and quality of life by reducing the number of hospital visits. 10
Recently, oncofertility, which aims to balance cancer treatment with pregnancy and childbirth, has been attracting attention, and the number of young patients with BC who interrupt endocrine therapy to become pregnant has been increasing. Based on this, the POSITIVE study 11 reported that the risk of short-term recurrence was not affected by the interruption of endocrine therapy for up to 2 years for women with ER-positive BC who were trying to conceive and give birth.
To shorten the interruption period of endocrine therapy due to pregnancy and childbirth, the resumption of menstruation after the interruption should be earlier. However, there are few reports on the effect of endocrine therapy on the resumption of menstruation. Therefore, we collected information from medical records and conducted a retrospective study on the recovery of ovarian function after the interruption of GnRHa therapy and its effect on the resumption of menstruation.
Materials and Methods
BC patients who underwent fertility preservation therapy at our clinic between January 2010 and August 2023 were extracted from our medical records.
We examined the recovery of ovarian function and the timing of resumption of menstruation after the interruption of GnRHa endocrine therapy.
Twenty-two cases were included in this study, of which two cases were identified in which endocrine therapy was interrupted twice due to the desire for a second child. The 24 cycles were retrospectively examined from the medical records, including age, chemotherapy use, type of GnRHa formulation administered, blood hormone levels after interruption, and time of resumption of menstruation.
JMP Pro ver. 16 was used for statistical analysis, and information on patients with a history of BC treatment at other hospitals was also obtained by requesting each facility to provide medical information.
We obtained approval from the Research Ethics Committee of Saitama Medical Center for this study (Approval No. 2024-023) and published an opt-out document on our website regarding obtaining clinical data from medical records.
Results
At the time of GnRHa interruption, the last formulation administered was a 1-month leuprorelin formulation in 2 patients (L1 group), a 3-month leuprorelin formulation in 5 patients (L3 group), a 6-month leuprorelin formulation in 7 patients (L6 group), a 1-month goserelin formulation in 3 patients (G1 group), and a 3-month goserelin formulation in 7 patients (G3 group). The three groups were compared according to the last GnRHa formulation administered: 1-month formulation group (L1, G1), 3-month formulation group (L3, G3), and 6-month formulation group (L6).
Of the total 24 cycles, the 1-month formulation group had 5 cycles (20%), the 3-month formulation group had 12 cycles (50%), and the 6-month formulation group had 7 cycles (29%). The age at the last dose of GnRHa was significantly higher in the 1-month formulation group (38.7 ± 2.1 years) than in the 6-month formulation group (34.2 ± 3.2 years) (p = 0.037), indicating that older patients tended to use shorter duration formulations.
Chemotherapy was administered to three patients (60%) in the 1-month formulation group, seven patients (58%) in the 3-month formulation group, and three patients (42.9%) in the 6-month formulation group. Chemotherapy administration, serum anti-Müllerian hormone (AMH) concentration before chemotherapy, and duration of GnRHa administration (days from the first to last administration dates) were not significantly different among the three groups.
In three cycles in three cases, assisted reproductive treatment was started without waiting for menstruation to resume, and in two of these cases, frozen embryo transfer under hormone replacement was performed. In the remaining case, ovarian stimulation for oocyte retrieval was initiated after confirming that ovarian function had recovered to the early follicular phase level, although menstruation had not resumed.
The number of days from the last day of GnRHa administration to the resumption of menstruation was 207 ± 77 days in the 1-month formulation group (L1 and G1 groups), 270 ± 94 days in the 3-month formulation group (L3 and G3 groups), and 355 ± 85 days in the 6-month formulation group (L6 group), showing significant differences between the 6- and 1-month formulation groups (p = 0.039), but there was no significant difference between the 1- and 3-month formulation groups (Table 1 and Fig. 1).
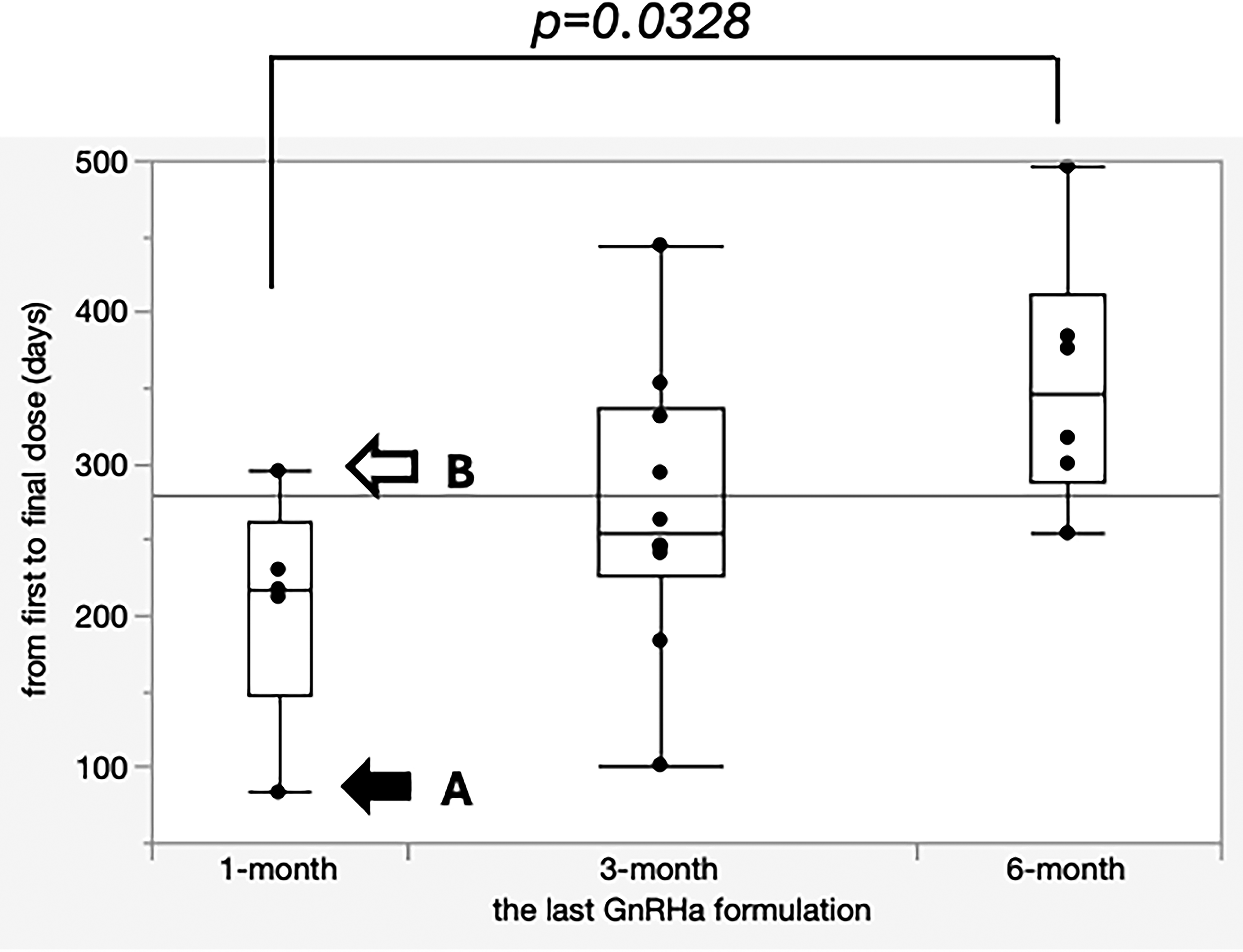
The days from the last GnRHa injection to the resumption of menstruation. The number of days between the last dose of GnRHa and the resumption of menstruation was compared (excluding the three cycles in which assisted reproductive therapy was resumed without waiting for the resumption of menstruation) among the 1-, 3-, and 6-month formulation groups. The ends of the box represent the first quartile (Q1) and the third quartile (Q3), and the width of the box indicates the interquartile range (IQR: Q3–Q1). A thick line inside the box represents the median. Whiskers extend to the smallest and largest values within 1.5 × IQR of the box. In Case A (black arrow) and Case B (white arrow), the time to the resumption of menstruation was particularly short and long in the 1-month formulation group, respectively.
Comparison of the Last Dose of GnRHa
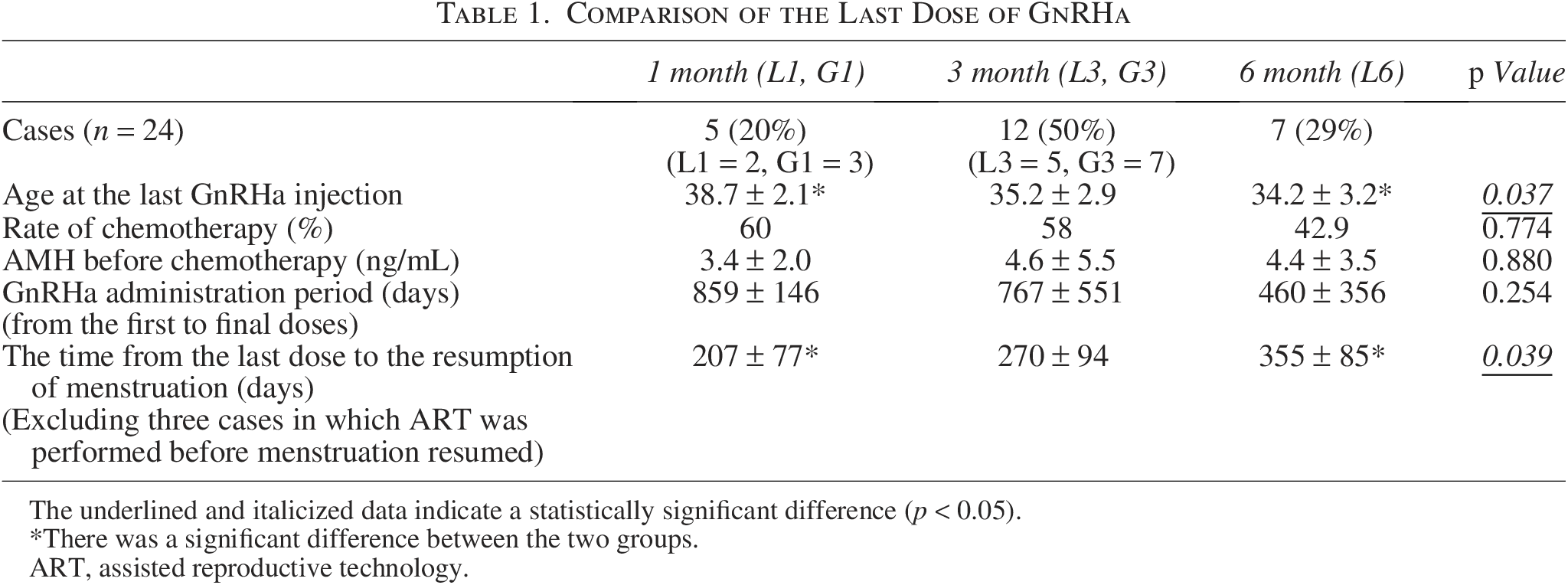
The underlined and italicized data indicate a statistically significant difference (p < 0.05).
There was a significant difference between the two groups.
ART, assisted reproductive technology.
In particular, when serum hormone levels were measured in some patients with delayed resumption of menstruation (one cycle in the 1-month formulation group, nine cycles in the 3-month formulation group, and five cycles in the 6-month formulation group), serum follicle-stimulating hormone levels increased approximately 3 months after the last dose in the 1-month formulation group and approximately 6 months in the 3-month formulation group, showing that serum gonadotropins were suppressed beyond the duration of the drug effect shown in their prescribing information (Fig. 2). Similarly, serum estradiol levels were found to increase more slowly than expected from their prescribing information (Fig. 3).
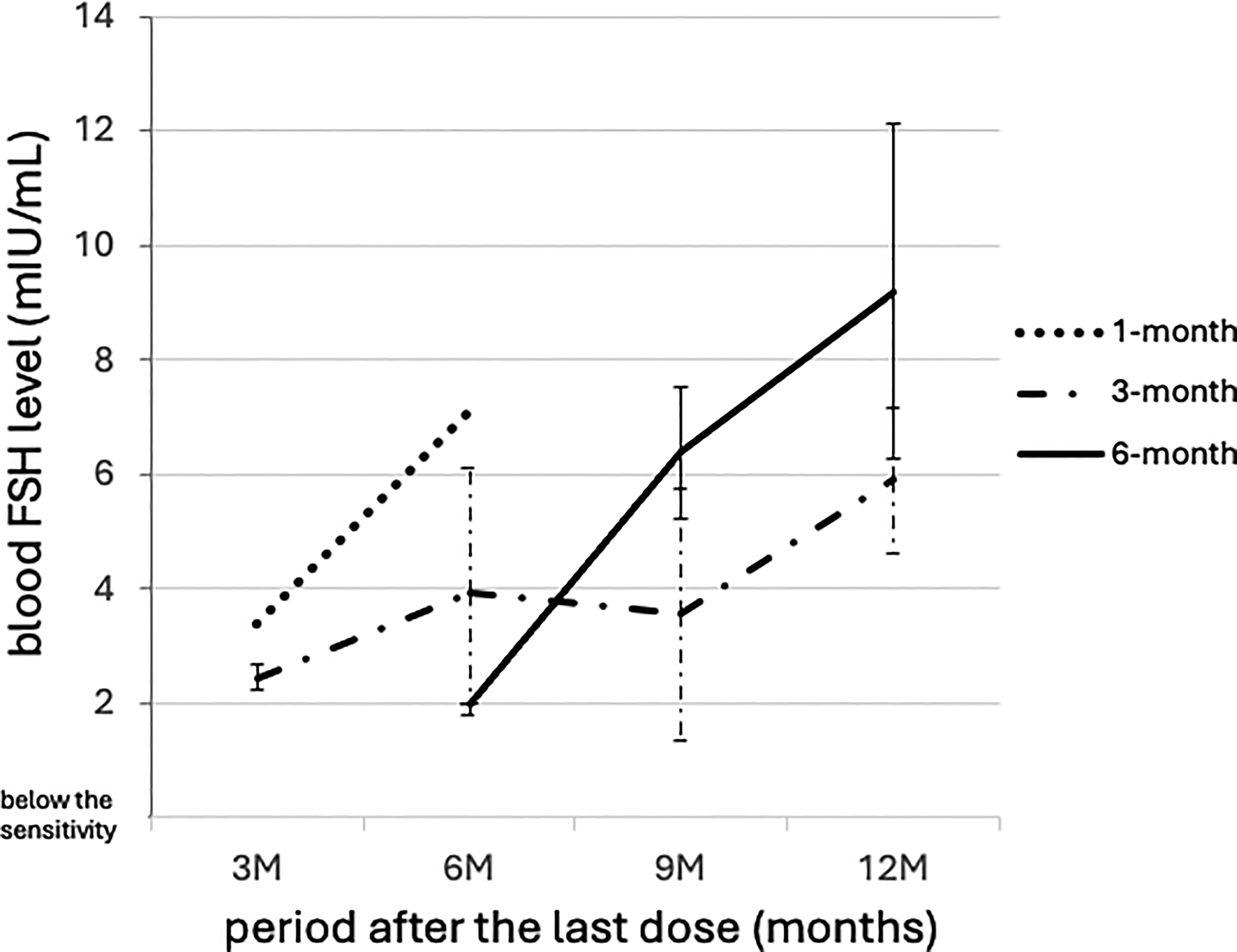
Blood FSH levels after each GnRHa formulation interruption. Blood tests were performed in 15 cycles in which menstrual resumption was delayed. Blood FSH levels increased approximately 3 months after the last dose of the 1-month formulation and approximately 9 months after the last dose of the 3-month formulation. The vertical lines accompanying each data point (error bars) represent the standard deviation (SD). Longer error bars signify greater variability in the data, whereas shorter bars indicate lower variability. FSH, follicle-stimulating hormone.
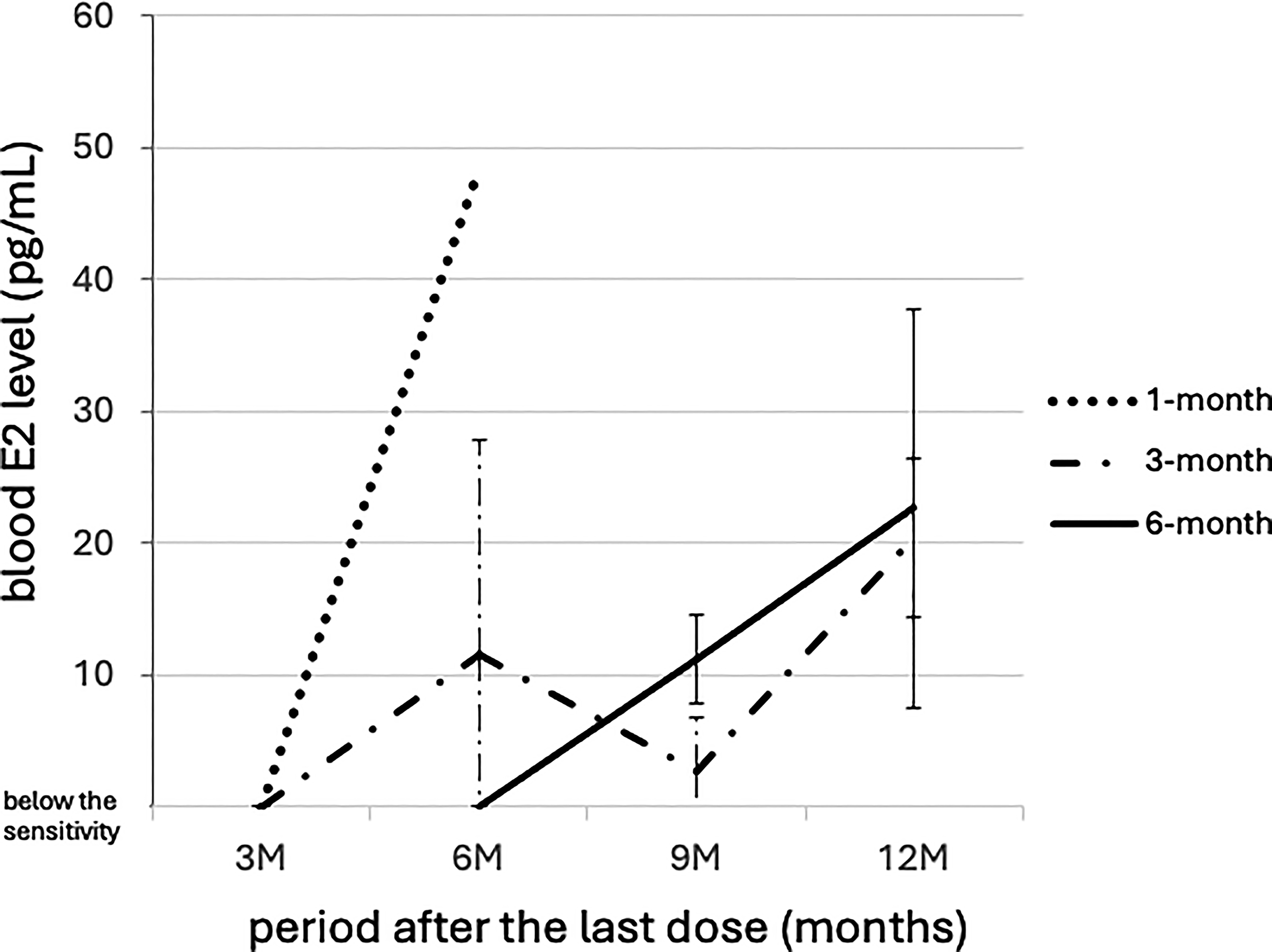
Blood E2 levels after each GnRHa formulation interruption. Blood tests were performed in 15 cycles in which menstrual resumption was delayed. Blood E2 levels were found to be close to the early follicular phase level approximately 3 months or more after the last dose of the 1-month formulation and approximately 12 months of the 3- and 6-month formulations.
Multivariate analysis of the factors influencing the timing of resumption of menstruation showed that age, previous cyclophosphamide administration, serum AMH levels before chemotherapy, and duration of GnRHa administration were not significant factors, and only the use of the 6-month formulation for the last dose at the time of GnRHa interruption had a significant effect on the timing of resumption of menstruation (p = 0.04) (Table 2).
Analysis of Factors Affecting the Days until Menstruation Resumes (Multiple Regression Analysis)
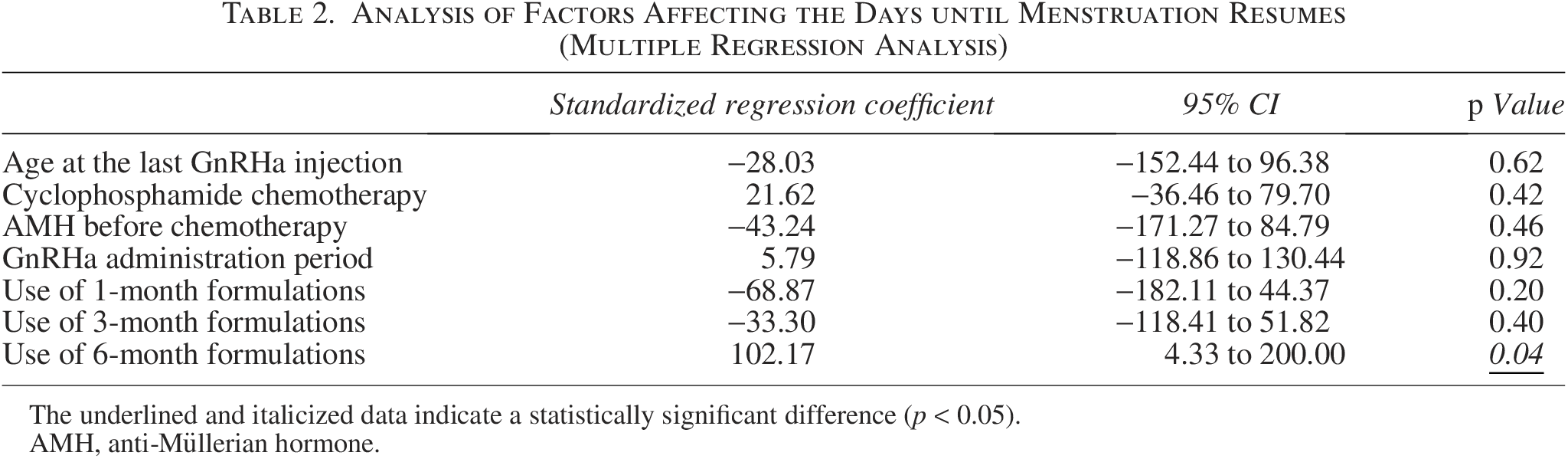
The underlined and italicized data indicate a statistically significant difference (p < 0.05).
AMH, anti-Müllerian hormone.
Of the five cycles in the 1-month formulation group, Case A (black arrow in Fig. 1), who had 83 days between the last dose and the resumption of menstruation, used only the 1-month formulation for the 6 months until the last dose. In contrast, Case B (white arrow in Fig. 1), in which menstrual resumption was largely delayed, with 295 days between the last dose and the resumption of menstruation, also used only the 1-month formulation for approximately 2.5 years until the last dose. However, it was discontinued due to the side effect of alopecia; then, TAM alone was continued for 5 years until the end of the study period, and menstruation resumed during TAM administration. This was the only case in the 1-month formulation group that was taking TAM when menstruation resumed. In the other three cycles, the 3-month formulation was used in the 6 months before the last dose, or the 6-month formulation was used in the 12 months before the last dose.
These results confirm that in the 1-month formulation group, menstrual resumption was significantly delayed when any of the following three factors was present: (1) the use of the 3-month formulation in the 6 months before the last dose of GnRHa, (2) the use of the 6-month formulation in the 12 months before the last dose, or (3) the use of TAM when menstruation resumed (p = 0.04) (Fig. 4).
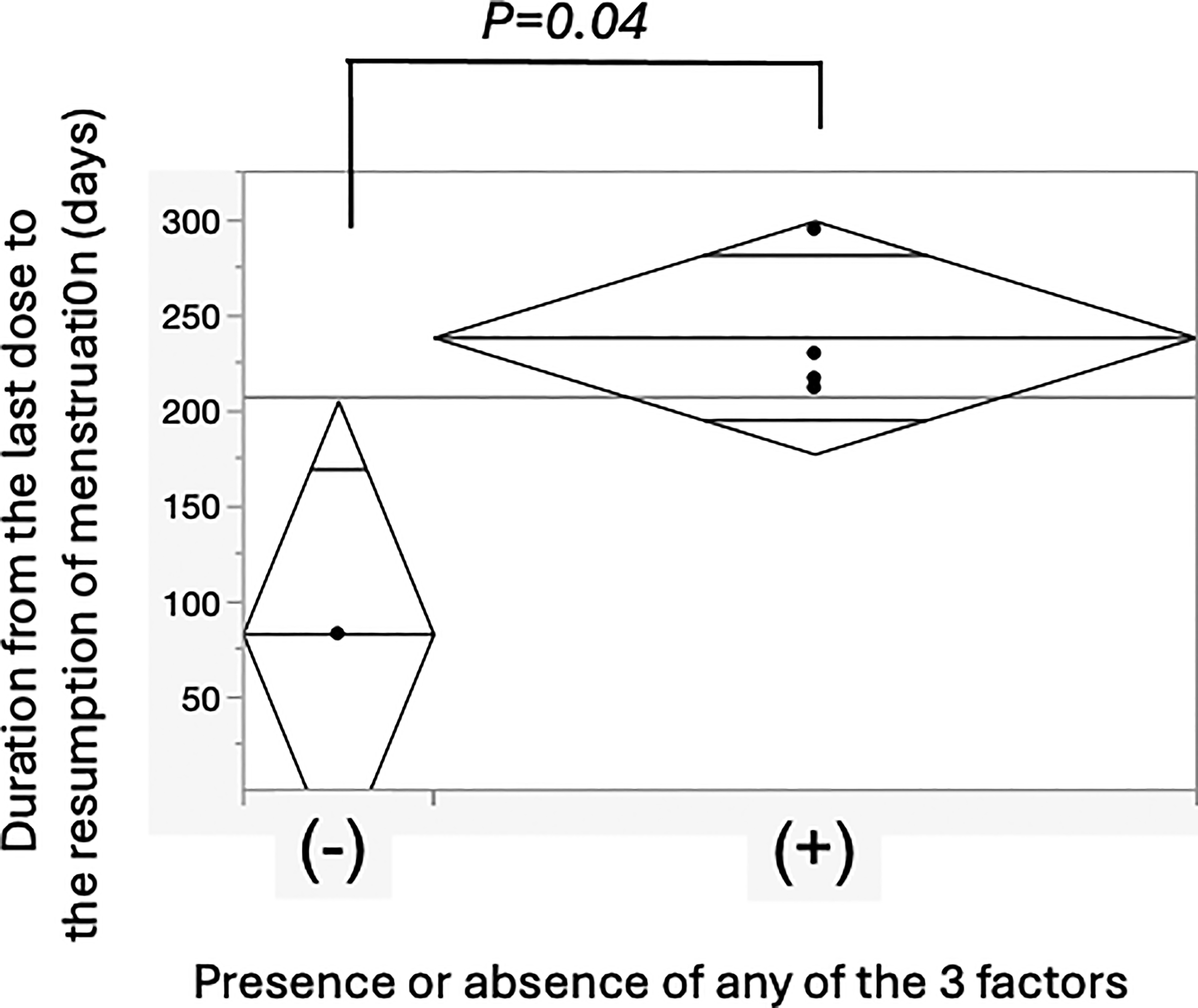
The days from the last dose to the menstruation resumption in the presence or absence of the three factors affecting the resumption in the 1-month formulation group. In the 1-month formulation group, menstrual resumption was significantly influenced by the presence or absence of the following three factors: (1) the use of a 3-month formulation in the 6 months before the last dose of GnRHa, (2) the use of a 6-month formulation in the 12 months before the last dose, or (3) the use of TAM when menstruation resumes. The width of the diamond represents the precision of the estimate based on the sample size. A larger sample size results in a wider width, whereas a smaller sample size results in a narrower width. The central line within the diamond represents the mean of the respective group. The upper and lower bounds of the diamond indicate the 95% confidence interval of the mean for that group, showing the range within which the population mean is expected to lie.
Of the 24 cycles included in this study, clinical pregnancy (confirmed gestational sac) occurred in 18 cycles (75%), and ongoing pregnancy (confirmed fetal heartbeat) occurred in 15 cycles (63%). Subsequently, delivery occurred in 12 cycles (50%). Of the 12 cases that resulted in birth, 1 was a natural pregnancy, and 11 were pregnancies achieved through assisted reproductive technology (9 pregnancies resulted from embryos that had been cryopreserved for fertility preservation, and 2 pregnancies resulted from embryos obtained through oocyte retrieval performed during hormone therapy discontinuation); all were full-term births. One case had a small-for-gestational-age infant due to gestational diabetes (gestational age, 39 weeks, birth weight, 2417 g), and one case had a large-for-gestational-age infant (based on the Japanese standards) of unknown cause (gestational age, 39 weeks; birth weight, 3643 g); however, all births showed good baby growth. The duration from treatment discontinuation to delivery was 645 ± 136 days, and the duration from menstrual resumption to delivery was 381 ± 119 days.
Discussion
In premenopausal BC patients undergoing fertility preservation and seeking pregnancy after the interruption of endocrine therapy including GnRHa, the number of days between the last dose of GnRHa and the resumption of menstruation varied widely among individuals, and even in patients who had used a 1-month or 3-month formulation for the last dose, amenorrhea continued for >6 months.
The safety of interrupting endocrine therapy to achieve pregnancy and childbirth in premenopausal BC patients has long been controversial, but the POSITIVE trial was recently reported. 11 The study included 18 to 30 months of adjuvant endocrine therapy, followed by up to 2 years of interruption of endocrine therapy, with a recurrence rate comparable to the control group of up to 3 years after interruption. The delay in the resumption of menstruation due to the GnRHa formulation should be avoided, as it is desirable to aim for an early pregnancy and childbirth during the 2-year interruption period.
In recent years, many BC patients have undergone fertility preservation before chemotherapy or endocrine therapy. This study also included BC patients who underwent fertility preservation, and as mentioned above, a good pregnancy rate was obtained. If frozen embryos are available, pregnancy is possible with frozen embryo transfer under hormone replacement, even if the resumption of menstruation is delayed. However, in the case of frozen embryo transfer, it is desirable that menstruation and ovulation be restored, if possible, because there is almost a consensus that the perinatal prognosis is better if the transfer is performed in a natural cycle than in a hormone replacement cycle. 12
In the gynecological field, when only the 1-month formulation is used for conditions such as uterine fibroids or endometriosis, menstruation usually resumes about 2–3 months after the last injection. In contrast, in our present study, even with the 1-month formulation, the mean time to menstrual recovery exceeded 6 months after the final administration (Table 1), which is substantially longer than expected.
A previous study 13 examining menstrual recovery after long-term chemotherapy and endocrine therapy in premenopausal BC patients reported a mean time to menstrual recovery of 7.3 ± 2.8 months after the GnRHa formulation. At that time, only the 1- and 3-month depot preparations were in clinical use, but the specific formulation employed was not indicated. Furthermore, the study indicated that the menstrual recovery rate was 42.1% for those aged 40 years or younger and 9.2% for those aged 41 years or older, suggesting a tendency for the time to menstrual recovery to be longer in older patients. However, in our present study, no significant difference was found regarding age as a factor affecting menstrual resumption (Table 2).
To identify the cause of delayed menstrual resumption beyond expectations after GnRHa formulation use, an additional investigation of all GnRHa formulations administered suggested that the use of long-term depot formulations, such as 3- and 6-month formulations, may delay the resumption of menstruation (Fig. 1).
It was also suggested that TAM continued alone after the interruption of GnRHa treatment may delay the resumption of menstruation (Fig. 4). The reason for the delayed resumption of menstruation in patients using TAM is that TAM acts on the hypothalamus as an estrogen agonist even under low-estrogen conditions during GnRHa treatment and may suppress the luteinizing hormone surge by suppressing hypothalamic GnRH secretion from the hypothalamus through negative feedback, 14 and that this suppressive effect of TAM on GnRH secretion may continue even after the GnRHa is discontinued. 15 Therefore, we hypothesized that the presence or absence of TAM administration also affected the timing of menstrual resumption.
No consistent trend was observed for the 3- and 6-month formulations, and more cases need to be accumulated in the future. Nevertheless, we assume that in BC patients who try to conceive after interrupting endocrine therapy, it may be easier to estimate the timing of resumption of menstruation by avoiding these long-term depot formulations for several months or more in advance.
Because the number of premenopausal BC patients who discontinue endocrine therapy to achieve pregnancy and childbirth has been increasing in recent years, there is a need for gynecologists and BC doctors to work together to optimize endocrine therapy, restore menstruation and ovulation as soon as possible, and achieve pregnancy and childbirth within the shortest possible interruption period.
Conclusion
In BC patients who may seek pregnancy after interrupting endocrine therapy using GnRHa, 3- and 6-month GnRHa formulations may delay menstruation resumption beyond their anticipated effective period, and should be replaced with a 1-month formulation more than 6 months before the interruption, to achieve pregnancy and childbirth as soon as possible during the interruption.
Authors’ Contributions
H.S., S.K., K.S., and S.M. contributed to project planning. K.T., H.H., and Y.T. contributed to article writing/editing.
Footnotes
Acknowledgments
There were five breast clinics and hospitals that cooperated with this survey. Dr. Hiroshi Matsumoto, Dr. Yoko Yamada (Saitama Cancer Center), Dr. Manabu Arai, Dr. Koji Fujimoto, Dr. Takashi Hojo, Dr. Kenji Kurono (Saitama Medical Center, Saitama Medical University), Dr. Akihiko Osaki, Dr. Hiroko Shimada, Dr. Asami Nukui (International Medical Center, Saitama Medical University), Dr. Takeshi Murata (National Cancer Center), Dr. Risa Goto (Kumamoto University). The authors would like to express our gratitude to all the doctors. This work was supported by the MHLW Research for the Promotion of Cancer Control Program Grant in Japan Number JPMH23EA1016.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.