
Abstract
Objective:
Fatigue is a prevalent and debilitating problem in adolescents and young adults (AYAs) with cancer. AYAs with acute lymphoblastic leukemia (ALL) are at particular risk for fatigue. Other factors, such as pain, nausea, and negative mood, have also been identified as contributors to cancer-related fatigue in cross-sectional studies. Because these states rapidly fluctuate, they may also serve as important time-varying predictors of fatigue. The purpose of this study was to determine whether current pain, nausea, and negative mood predict subsequent fatigue in AYAs during maintenance therapy and whether these relationships are moderated by sociodemographic factors.
Methods:
Eighteen AYAs (Mage = 17.90) completed a baseline demographic questionnaire and once-daily diaries to assess current fatigue, pain, nausea, and negative mood over a 28-day period during maintenance treatment. Dynamic structural equation modeling was used to examine whether pain, nausea, or negative mood predicts next-day fatigue, and if specific demographic variables, age, biological sex, race, ethnicity, and insurance status (public vs. private) moderated these relationships.
Results:
Pain significantly predicted next-day fatigue in AYAs (Est. = 0.35, p < 0.001), and age was the only significant moderator of this relationship (Est. = −0.13, p < 0.001). Nausea and negative mood did not significantly predict next-day fatigue.
Conclusions:
Pain positively predicted next-day fatigue, and the effect of pain as a predictor of fatigue was found to decrease with age. Routine pain assessments that trigger timely, in-the-moment interventions may help alleviate current pain and reduce near-term fatigue in AYAs with ALL during maintenance treatment, especially among younger adolescents.
Introduction
Fatigue is one of the most prevalent and debilitating symptoms among adolescents and young adults (AYAs) undergoing cancer treatment, often persisting into survivorship.1–4 AYAs diagnosed with acute lymphoblastic leukemia (ALL) appear particularly vulnerable to fatigue, in part due to prolonged exposure to corticosteroids and extended treatment duration.1,5,6 Maintenance therapy, a relatively stable and prolonged phase of ALL treatment lasting 2–3 years, involves lower-intensity chemotherapy compared to earlier phases. 7 Despite this reduced intensity, many AYAs continue to report high levels of fatigue, suggesting that factors beyond acute treatment toxicity contribute to this persistent symptom burden.8–13
Emerging research highlights the importance of biopsychosocial mechanisms in the development and maintenance of cancer-related fatigue.14–17 Biological factors, such as hypothalamic–pituitary–adrenal axis dysfunction, circadian rhythm disruption, and chronic inflammation, have been identified to contribute to cancer-related fatigue. 18 Psychological factors, including negative mood (e.g., distress, depressive symptoms), pain, and nausea, have shown consistent associations with fatigue in cross-sectional and longitudinal studies.9,13,19–30 These symptoms often interact in dynamic and compounding ways, exacerbating fatigue during and after cancer treatment.13,19,26–31
Despite these findings, little is known about how these symptoms interact with fatigue on a day-to-day basis during the maintenance phase of treatment. This gap is critical as physical and emotional states can fluctuate rapidly and, in turn, influence subsequent functioning and health behaviors. Assessing these factors more frequently could help identify critical patterns and time points for delivering personalized, targeted supportive care interventions (just-in-time adaptive interventions). 32
Beyond biological and psychological influences, sociodemographic factors such as age, biological sex, race, ethnicity, and insurance status have been shown to impact fatigue,33–35 and therefore may moderate relationships between daily symptoms and fatigue. 8 Prior research has documented disparities in symptom burden and access to supportive care across these dimensions,36–38 suggesting that certain subgroups of AYAs may be more susceptible to fatigue-related impairments. Understanding these moderating effects is essential for identifying high-risk populations and tailoring interventions accordingly.
The present study seeks to address these gaps by examining whether daily experiences of pain, nausea, and negative mood predict next-day fatigue among AYAs receiving maintenance therapy for ALL. Furthermore, we investigate whether sociodemographic characteristics moderate these associations, with the goal of identifying high-risk subgroups and informing the development of personalized, targeted interventions for fatigue management during this critical phase of treatment.
Methods
Participants and procedures
This study involved secondary analysis of data from a study that analyzed the temporal associations between daily contextual factors and oral 6-mercaptopurine (6-MP) adherence among AYAs with ALL undergoing maintenance treatment. 39 Eligible participants were recruited during routine outpatient maintenance chemotherapy visits at a large pediatric cancer center in the Mid-Atlantic region of the United States. To participate in the primary study, AYAs had to meet the following criteria: (1) be between 14 and 25 years of age; (2) have a diagnosis of ALL; (3) be in the maintenance phase of treatment, with at least 1 month of maintenance chemotherapy completed and a minimum of 1 month remaining; (4) be prescribed daily oral 6-MP; (5) have proficiency in English; and (6) if under 18 years of age, have a caregiver (parent or legal guardian) available to provide informed consent. Exclusion criteria included the inability to complete study measures due to cognitive impairment, as determined by the medical team. Data collection procedures were conducted with approval from the Institutional Review Board at Children’s Hospital of Philadelphia.
After completing informed consent in the clinic, AYA participants completed a baseline demographic questionnaire via REDCap (Research Electronic Data Capture; Vanderbilt University). Then, for the next 28 days (the approximate time between monthly maintenance clinic visits), participants received a prompt at 4 PM Eastern Standard Time to complete a once-daily diary. Daily surveys were brief (<1 minute to complete) and consisted of nine items assessing current physical symptoms (pain, fatigue, nausea; three items), current mood (positive and negative affect; two items), recent family or social stressors (argument with parent, ease of communication with parent, loneliness; three items), and current motivation to take oral 6-MP (one item). If a participant did not start the survey questions within an hour after it was sent, one reminder was sent. For the present study, only data related to physical symptoms and mood were analyzed (i.e., five items total). Physical symptoms were rated on a scale of 0 (none) to 10 (worst), which were adapted items from two adult oncology ecological momentary assessment studies.39–41 Mood items were rated on a scale of 0 (not at all) to 3 (extremely), adapted from a physical activity ecological momentary assessment study.39,41
Diaries were sent via text message using Twilio/REDCap. Twilio is a third-party communication platform that integrates with REDCap to automatically send survey questions and responses to and from a REDCap database to a participant’s mobile phone via a text message. Participants text back their response to each survey question, and then their response is stored in the REDCap database.
Statistical analyses
Data screening procedures were performed using SPSS version 29 (IBM Corp., Armonk, NY, USA) and out-of-range values, skewness, kurtosis, means, and standard deviations (SDs) were evaluated using descriptive statistics. The data were within the range of minimum and maximum values for each measure, and the percentage of missing data overall was <5%. Demographic and descriptive variables were analyzed using frequencies. Dynamic structural equation modeling (DSEM) was conducted in Mplus Version 8.8 with Bayesian estimation to evaluate within-person associations between daily symptoms and next-day fatigue, and between-person moderation by demographic characteristics. 42 DSEM was selected for its capacity to model multilevel time-series data, simultaneously estimating within-person (Level 1) and between-person (Level 2) effects. 43
Bayesian estimation was used to generate standardized regression coefficients that incorporate parameter uncertainty and to handle missing data by estimating posterior distributions rather than relying on listwise deletion. 43 Models included random intercepts and autoregressive parameters to account for individual differences in symptom levels and temporal dependencies in the data. All predictors were mean-centered to isolate within-person effects. Model convergence was assessed using potential scale reduction values, with values <1.05 indicating acceptable convergence. Of note, a negative linear trend in fatigue levels was detected during data screening procedures and corrected for in analyses.
At the within-person level (Level 1), cross-lagged effects were modeled by regressing next-day fatigue (t) on prior-day (t–1; lag 1) pain, nausea, and negative mood. Moderation analyses at the between-person level (Level 2) examined whether demographic characteristics influenced the strength of these within-person associations. See Figure 1 for the statistical model. Credibility intervals (CIs) are reported for all DSEM parameters and represent the range within which each parameter has a 95% probability of falling. 44 Estimates with 95% CIs that do not include zero were considered statistically significant.44,45
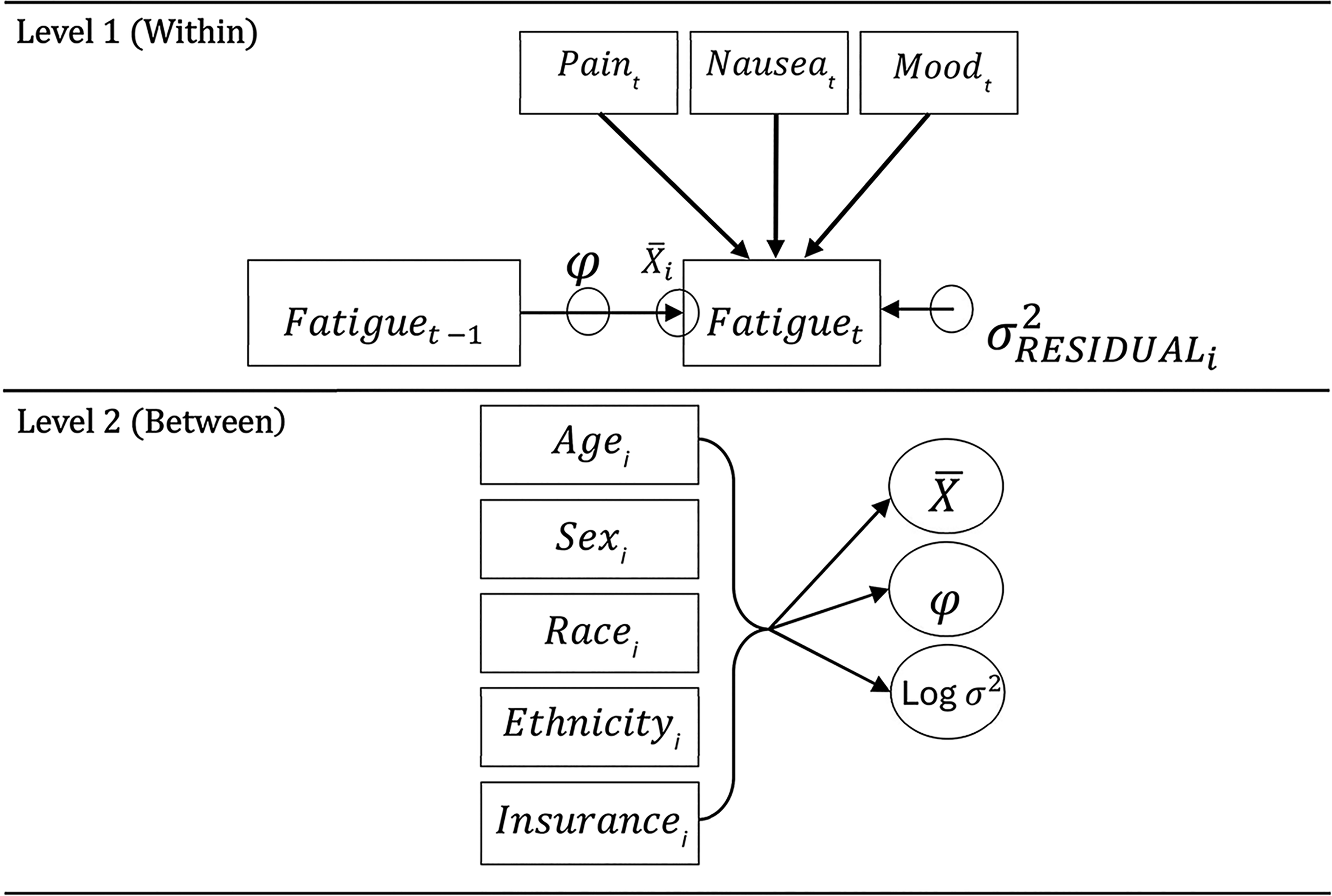
Statistical model. This figure illustrates within-person and between-person associations between daily pain and next-day fatigue. Age, biological sex, race, ethnicity, and insurance status were examined as moderators at the between-person level.
Results
Demographic characteristics and mean scores for daily diary items are presented in Table 1. The sample included 18 AYAs with ALL, with a mean age of 17.9 years (SD = 2.3). Most participants were male (77.8%) and identified as white (66.7%), while the remaining participants identified as Black (11.1%), Asian (5.6%), or another/unspecified race (16.7%). Most of the sample was non-Hispanic (72.2%). Mean survey completion rate of the sample over the 28-day period was 88.9% (SD = 16.3%).
Demographic Characteristics
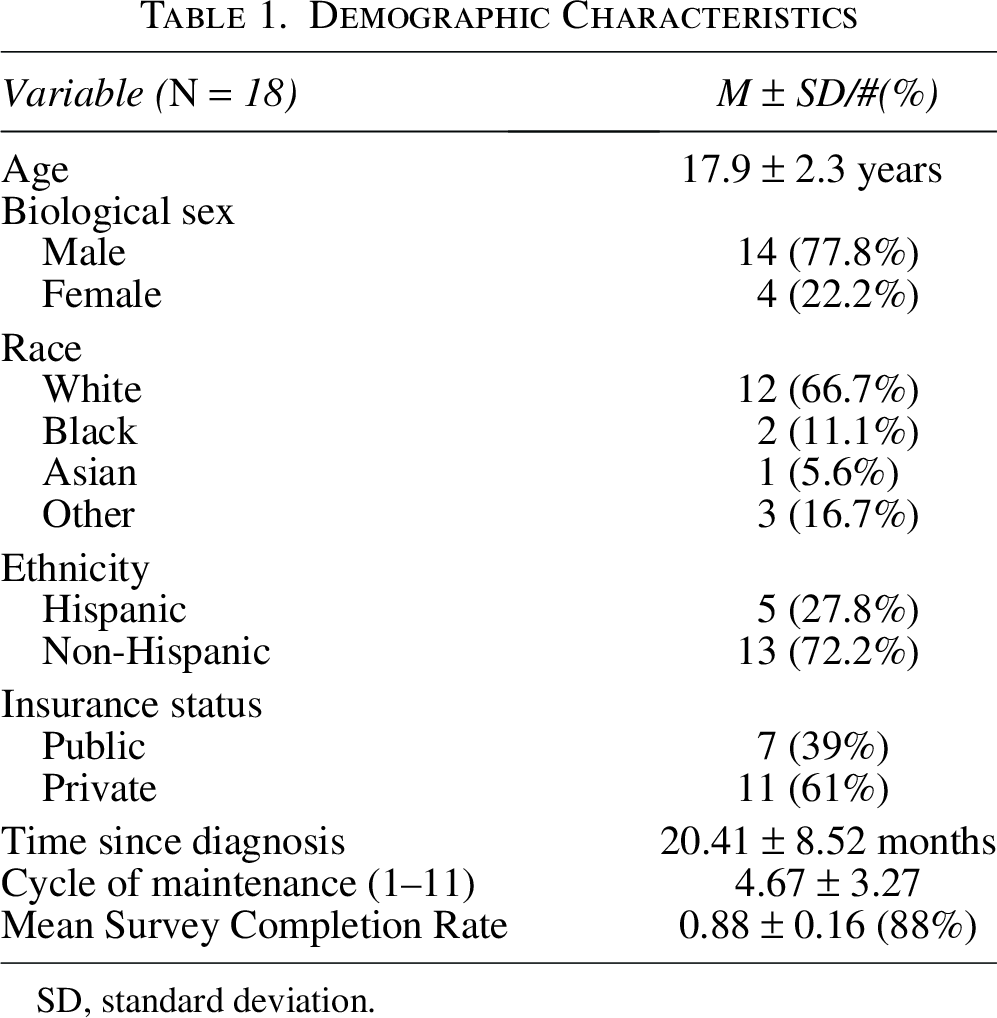
SD, standard deviation.
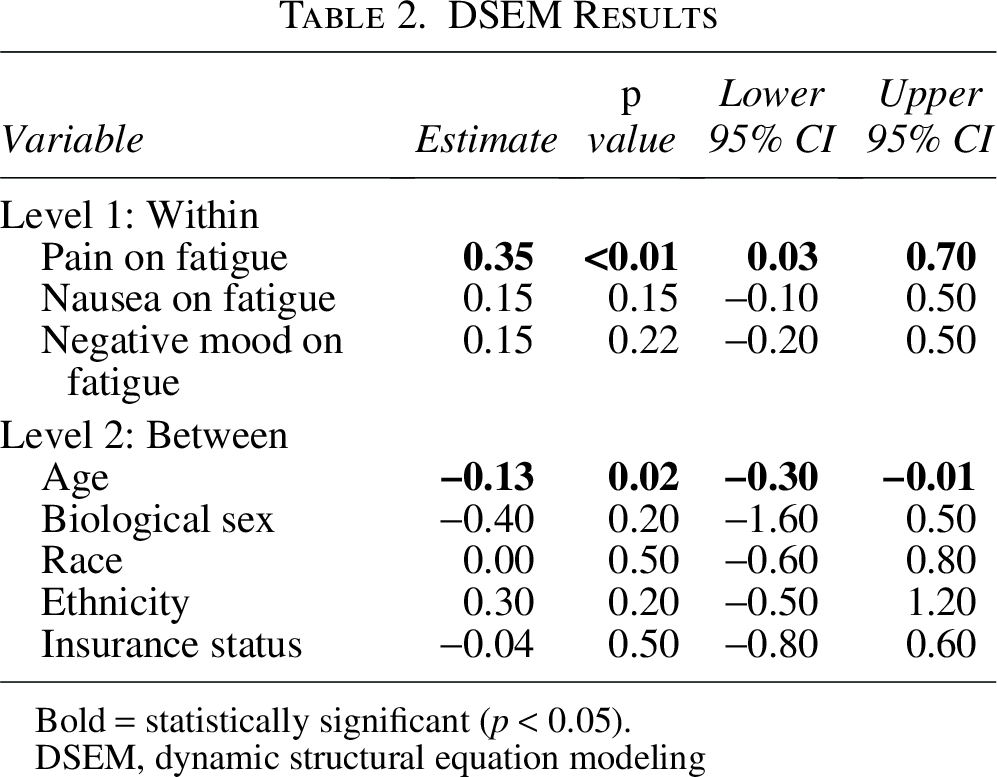
DSEM analyses revealed that pain significantly predicted next-day fatigue ratings in AYAs (see Table 2 for all DSEM results). Specifically, greater pain intensity ratings were associated with greater fatigue ratings the following day (Est. = 0.35, p < 0.01; 95% CI = 0.03 to 0.70). Nausea (Est. = 0.15, p = 0.15; 95% CI = −0.10 to 0.50) and negative mood (Est. = 0.15, p = 0.22; 95% CI = −0.20 to 0.50) did not significantly predict next-day fatigue. Age was found to moderate the relationship between pain and fatigue, such that the impact of pain on fatigue decreases as age increases (Est. = −0.13, p = 0.02; 95% CI = −0.30 to −0.01). Biological sex (Est. = −0.40, p = 0.20; 95% CI = −1.60 to 0.50), race (Est. = −0.00, p = 0.50; 95% CI = −0.60 to 0.80), ethnicity (Est. = 0.30, p = 0.20; 95% CI = −0.50 to 1.20), and insurance status (Est. = −0.04, p = 0.50; 95% CI = −0.80 to 0.60) did not moderate the relationship between pain and fatigue. A visual representation of daily fluctuations in pain and fatigue ratings is provided in Figure 2.

Daily fluctuations in pain and fatigue ratings among AYAs with ALL. This figure displays day-to-day fluctuations in pain and fatigue among AYAs with ALL during maintenance therapy across the 28-day study period.
DSEM Results
Bold = statistically significant (p < 0.05).
DSEM, dynamic structural equation modeling
Discussion
The present study utilized intensive longitudinal data to conduct secondary analysis of the daily associations between pain, nausea, mood, and cancer-related fatigue in AYAs with ALL during maintenance therapy. Consistent with prior cross-sectional and longitudinal research, we found daily increases in pain significantly predicted higher levels of fatigue the following day, underscoring the robust and temporally proximal relationship between pain and fatigue in this population.20–23,25,26 In contrast, nausea and negative mood did not significantly predict next-day fatigue, indicating that pain may play a more immediate or influential role in driving daily fatigue fluctuations during maintenance therapy. Importantly, age moderated the pain–fatigue relationship, with younger AYAs showing a stronger association between these symptoms than their older peers, suggesting that developmental factors may shape vulnerability to symptom burden during maintenance therapy.
Findings of the current study contribute to a growing body of literature emphasizing the biopsychosocial underpinnings of cancer-related fatigue. While maintenance therapy is less intensive than earlier phases, our results suggest that daily fluctuations in pain may be a key driver of fatigue, independent of treatment intensity. This supports the notion that fatigue is not solely a consequence of chemotherapy toxicity, but is driven by complex and dynamic biopsychosocial processes that sustain symptom burden over time.14,15 The absence of significant associations between fatigue and nausea or negative mood may be due to the low average levels of these symptoms in our sample, or it may suggest that their effects on fatigue are more immediate or cumulative rather than delayed.
Importantly, age was found to moderate the pain–fatigue relationship, with younger AYAs exhibiting a stronger association between these symptoms during maintenance therapy than their older peers. This finding aligns with recent studies of survivors of childhood cancer showing that pain and fatigue frequently co-occur and that younger individuals may be particularly vulnerable. For example, Schulte et al. (2021) reported that chronic pain and fatigue often co-occur among younger survivors, 46 highlighting how developmental factors can shape symptom trajectories. Similarly, Vanrusselt et al. (2023) identified age-dependent variations in the pain–fatigue association, 47 suggesting that developmental factors influence both symptom expression and coping capacity. Together, these findings support a biopsychosocial framework in which biological factors, psychological processes, and developmental stage interact to influence fatigue in AYAs with ALL. Younger adolescents may have fewer adaptive coping strategies, heightened emotional reactivity, or less experience managing chronic symptoms, which could amplify the impact of pain on fatigue.48–50 These results underscore the importance of tailoring symptom management interventions by developmental stage, such as incorporating age-appropriate pain coping strategies into fatigue management protocols for younger AYAs. Furthermore, routine assessment of pain that triggers prompt and personalized intervention may help reduce fatigue, particularly in younger adolescents, by addressing this key driver of symptom burden during maintenance treatment.
Contrary to our expectations, other sociodemographic factors (biological sex, race, ethnicity, and insurance status) did not significantly moderate the pain–fatigue relationship. While prior research has highlighted disparities in cancer symptom burden and access to supportive care,36–38 our null findings may be attributable to the small sample size and limited variability across these demographic factors in the current study. Future research with larger, more diverse samples is needed to further examine potential sociodemographic moderators and their role in shaping symptom trajectories.
Results of this study should be considered within the context of several limitations. First, our sample size may have limited the ability to detect smaller effect sizes, particularly in moderation analyses. Second, although daily diaries minimize recall bias and capture real-time symptom changes, the reliance on self-reported data may introduce subjective bias. Third, the 28-day monitoring period may not fully capture longer-term symptom variability or fluctuations occurring across the maintenance phase of treatment. Fourth, the single-site design and demographic composition of the sample limit generalizability to broader populations of AYAs with ALL or other cancers. Fifth, this study focused specifically on pain, nausea, and negative mood, without assessing other potentially relevant biopsychosocial factors, such as sleep quality, physical activity, and anxiety, that have been shown to influence fatigue.14,15 Sixth, unmeasured confounding variables, such as treatment intensity and toxicity, which have been shown to impact pain among pediatric cancer survivors, 51 were not controlled for and should be addressed in future research. Finally, while this study provides valuable insights into temporal associations between symptoms and fatigue, its observational design limits causal inference. Although a longitudinal study with a longer follow-up period may help clarify temporal relationships, experimental or quasi-experimental designs, such as testing whether interventions targeting pain also reduce fatigue, may help establish causality.
The findings from this study have several important clinical implications for managing fatigue among AYAs with ALL during maintenance therapy. First, given that pain emerged as a significant time-varying predictor of fatigue in the current study, routine and systematic assessment of pain symptoms should be integrated into standard care. Ecological momentary assessment methods may be particularly valuable, and digital tools such as text messaging or mobile apps (i.e., Pain Squad+TM app, a gamified and freely available multidimensional pain assessment and management tool),52–54 could offer efficient ways to capture pain in real time and support the delivery of personalized, just-in-time adaptive. 32 These approaches could prompt AYAs to use evidence-based pain coping strategies, such as distraction, gentle physical activity (i.e., stretching, walking, yoga, light exercise), and/or relaxation techniques (i.e., diaphragmatic breathing, progressive muscle relaxation, mindfulness), which may subsequently alleviate fatigue by targeting shared underlying mechanisms such as stress, muscle tension, and sleep disruption. These targeted and scalable interventions may have cascading benefits for AYAs, ultimately reducing pain, mitigating fatigue, and improving quality of life. Second, the stronger pain–fatigue link observed in younger adolescents highlights the necessity of developmentally tailored approaches. Clinicians should consider incorporating age-appropriate pain coping skills training and fatigue self-management education that address the unique emotional and cognitive needs of younger AYAs. Providing additional psychosocial support and teaching adaptive coping strategies may enhance resilience and symptom control in this vulnerable subgroup. Finally, health care clinicians should adopt a proactive, multidisciplinary approach to symptom management that includes regular monitoring (potentially facilitated through digital health), early intervention, and ongoing education about the interplay of symptoms.38,55
In summary, this study identified daily pain as a significant and temporally predictive factor contributing to fatigue among AYAs undergoing maintenance therapy for ALL, especially among younger adolescents. Future research should aim to replicate these findings in larger, more diverse samples and explore real-time, individualized interventions that account for dynamic symptom interactions. Such efforts are critical for advancing supportive care strategies that improve quality of life and long-term outcomes in this vulnerable population.
Authors’ Contributions
K.L.K. contributed to conceptualization, literature review, data analysis, writing, reviewing, and editing. A.L.H.P. contributed to reviewing and editing. A.M.P. contributed to conceptualization, study design, methodology, data collection, writing, reviewing, and editing.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Mattie Miracle Cancer Foundation (Pilot Grant: “Real-Time Medication Adherence Assessments among Adolescents and Young Adults with Leukemia”) and the National Cancer Institute (Grant 1K08CA241335-01). Funding was awarded to the senior author, Alexandra Psihogios.