
Abstract
Childhood cancer survivors (CCS) who completed treatment and are disease-free face long-term care transition challenges. This quality improvement (QI) study explored CCS needs and captured feedback for the Adult Survivors of Childhood Cancer Clinic (ASCC) program development. Participants were predominantly White and female; ages ranged from 1 to 17 years at diagnosis and 18 to 34 years at the time of the study. Surveys (n = 47) and interviews (n = 5) focused on the voice of the ASCC patient. REDCap facilitated descriptive survey analysis, while the rapid analysis of interviews identified high-level themes aligned with the survey findings. Nutrition and mental health needs were ranked equally as the top needs, and rapid interview analysis identified noteworthy gender-specific trends. Integrating the patient perspective helps ensure clinic programming is tailored to the patients it serves.
Keywords
Introduction
In 2020, of which the most recent U.S. data exist, there were approximately 496,000 childhood cancer survivors (CCS). 1 The National Cancer Institute defines CCS as individuals diagnosed with cancer before the age of 21 years and who have been followed up for at least 5 years after diagnosis. 2 These individuals face various challenges that evolve over their lifetime. Parents and caregivers meet survivors’ health care needs in the pediatric setting, 3 and as survivors enter adulthood, they increase ownership of their health habits and health care. One CCS challenge concerns transitioning from child- to adult-focused care. 4
Transition is the “purposeful, planned movement of adolescents and young adults with chronic physical and medical conditions from child-centered to adult-oriented health care systems and ensures that their care will remain both medically and developmentally appropriate.” 5 Guides are influential in health care system program development. One example is Got Transition, a general, noncancer-specific guide endorsed by the American Academy of Pediatrics to help providers support individuals from child-centered to adult-centered care. 6
The ideal transition model for the CCS population is unknown 7 ; nonetheless, it should be a gradual, structured, and organized process that involves collaboration between pediatric and adult clinicians, during which survivors are educated about their cancer history, future risks, and the need for long-term follow-up care (LTFUC).8,9 Moreover, the transition from pediatric- to adult-focused LTFUC should be adapted to the needs of each CCS. 8 Models of CCS care should be built to provide or seamlessly facilitate continuous survivor-focused care across the age continuum. A longitudinal relationship with a survivor-focused provider can help promote the values survivors report as important in transitioning to LTFUC. 9
Survivors negotiate a cascade of shifting concerns, and responsive models of care must possess the diversity of expertise to address physical and psychosocial concerns. 10 Ensuring access to specialized resources addressing survivor needs in an integrated care model improves CCS engagement in survivorship care across the pediatric–adult continuum. To ensure adequate expertise in the Adult Survivors of Childhood Cancer (ASCC) Clinic within a multisite cancer care system, this quality improvement (QI) study explored survivors’ needs and their preferred modes of engagement with programming. While both research and QI involve systematic inquiry, research is designed to produce generalizable knowledge, whereas QI focuses on applying evidence to improve processes within a specific local context. 11 Based on the findings, CCS were informed of the implementation of ASCC Clinic services and encouraged, through a successful transition, into the adult setting.
Patients and Methods
A multidisciplinary working group was established to conduct a qualitative needs assessment informing the development of an ASCC Clinic. This QI study did not meet the definition of research as per the Human Subject Protection Regulations; thus, it did not require Internal Review Board oversight. We followed the Belmont Report and ensured that subjects were fully informed about the nature of the project, so that they could make an informed decision to participate. The working group and program development were supported by local stakeholders, including the Levine Children’s Hospital Director of Supportive Medicine in the Pediatric Hematology and Oncology Department, Levine Cancer Institute (LCI), and the Department of Supportive Oncology (DSO) (Fig. 1). The DSO was established in 2017 and includes eight clinical, research, and education sections. One of the clinical sections is Adult Survivorship, with a team for adult care best described as a long-term follow-up clinic in a shared care model. This QI study took place in the DSO, where CCS were being introduced to their ASCC clinical care team as they plan for their transition to adult care. To qualify for this planning meeting, survivors had to be 5 years off treatment and no longer in high school.
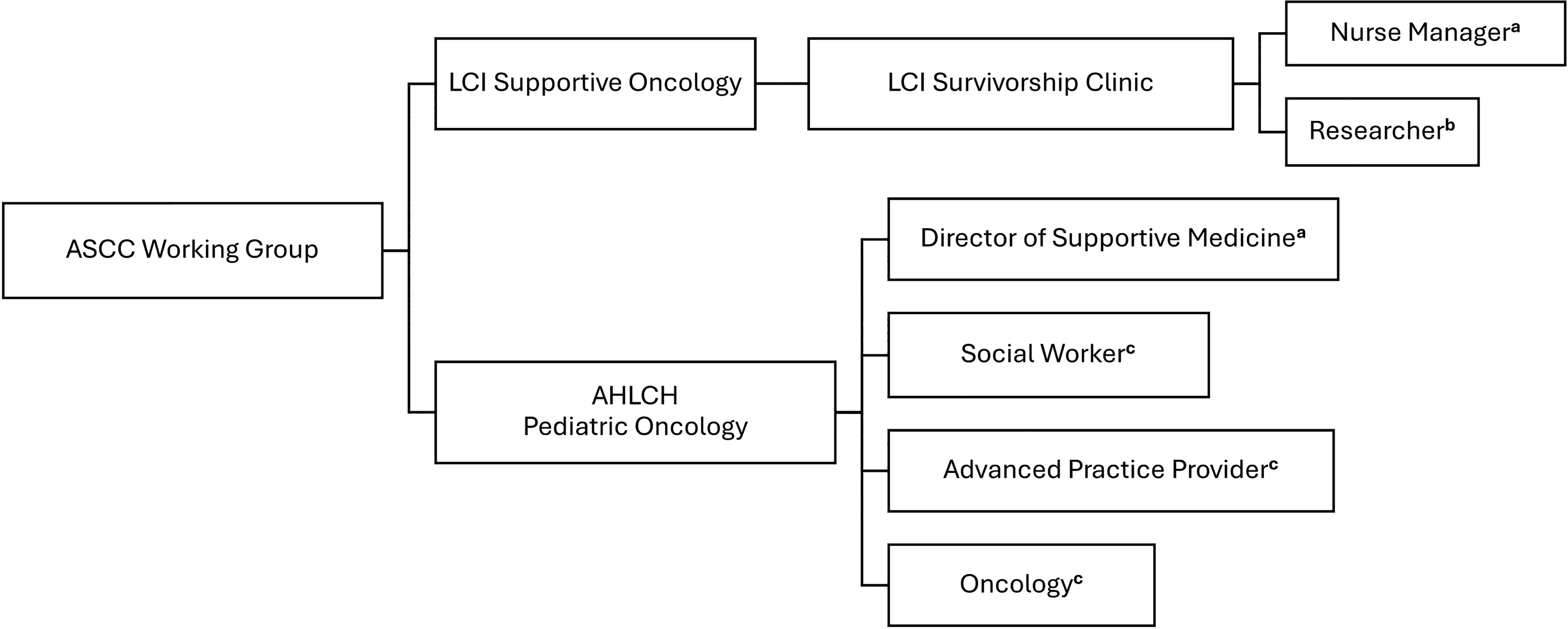
Structure of the Adult Survivors of Childhood Cancer (ASCC) working group.
A qualitative approach using purposive sampling and deductive analysis focused on the survivor’s voice. Two methods were employed: (1) a self-administered survey and (2) semi-structured interviews. The survey was an online open- and closed-ended survey formulated to identify needs, services desired, program format, information preferences, and demographics. Survivors from LCI’s Children’s Hospital Supportive Program, seen at LCI, participated in the survey and interviews. Patients who could not speak or understand English were excluded from recruitment. Consent was obtained at each methodological step.
Data collection
Self-administered surveys
Surveys were developed based on two sources of information: (1) the literature concerning qualitative research on survivors and their caregivers’ experiences when transitioning from child to adult services, research on models of care and transition for ASCCs, and input from the ASCC working group stakeholders. The survey was anonymous, except for those who volunteered to participate in the subsequent interviews. In that event, one data variable requested that survivors provide their contact details and consent to follow-up regarding their interview participation. Survey participation was either via a personal invitation from the clinician or via a QR code on a promotional flyer. Participants were invited to the survey if they participated in a transition meeting.
The survey was developed to capture the broad and detailed categories of ASCC preferences and views on transitioning to LTFUC (Supplementary Data S1). Part 1 focused on ASCC needs, and Part 2 consisted of the validated Cancer Worry Scale (CWS), Self-Management Skills Scale (SMSS), and Expectations Scale (ES). 12 The CWS is a 6-item questionnaire focused on worry about cancer-related issues, such as late effects. The SMSS is a 15-item questionnaire focused on the skills that adolescents need to manage their health care, and the ES is a 12-item questionnaire about the nature of adult LTFUC. As a combined set, these scales are reported to be reliable and valid (e.g., Person Separation Index ≥0.81; Cronbach’s α ≥ 0.81; test–retest reliability ≥0.85) to measure the constructs that CCS report as barriers and/or facilitators to the process of transitioning from pediatric to adult-oriented LTFUC. 12 Part 3 of the survey captured respondent demographics. The scale responses were formulated as yes/no, multiple-choice, open-ended for write-in responses or ranking responses based on importance.
Survey data collection was managed using the REDCap electronic data capture tools hosted at Atrium Health Wake Forest Baptist (Charlotte, NC, USA).13,14 REDCap is a secure, web-based software platform that supports data capture for research.
Semi-structured interviews
Upon survey completion, individuals were contacted by phone or email and invited to participate in a virtual semi-structured interview. Phone and email details were captured in the survey, which requested consent to follow up. The interview guide (Supplementary Data S2) was developed from the survey data, with the aim of obtaining more in-depth, qualitative information on the key survey findings. Five individuals agreed to participate in the interview, which lasted between 40 and 90 minutes. A researcher (D.M.B.) trained and experienced in qualitative research wrote the interview guide and conducted the interviews. The ASCC working group provided input on the interview guide before it was implemented.
Analysis
Survey analysis was managed using the REDCap electronic data capture tools hosted at Atrium Health Wake Forest Baptist (Charlotte, NC, USA).13,14 The REDCap report functions were used to extract data for descriptive analysis. 15 Interview recordings were transcribed using the Microsoft Teams transcription feature for rapid analysis. The rapid analysis supported the timely dissemination of qualitative findings for ongoing implementation. 16 The interviews were analyzed (D.M.B.) to capture high-level themes related to the specific priority needs identified in the survey descriptive analysis. ASCC working group members reviewed and gave input to the interview data analysis.
Results
Of the approximately 93 participants approached, 47 CCS, ages 1–17 years at diagnosis and 18–34 years at the time of the study, responded to the survey (a response rate of 50.5%). Five agreed to be interviewed (a response rate of 10.6%). Participants were predominantly White and female (Table 1), with one respondent identifying as having multiple races and ethnicities. The survey results identified the greatest needs and priority needs. A rapid analysis of the interviews identified gender-specific noteworthy trends.
Demographic Characteristics Of Childhood Cancer Survivors

Interview participants reported more than one race or ethnicity.
SD, standard deviation; No., number of participants.
Survey needs
In the survey, participants were asked what their greatest needs were at the time they completed it. The top three survey-reported needs (Fig. 2a) were as follows: 1) nutrition (n = 18, 38%), participants needed to know about their nutritional needs; 2) mental health (n = 17, 36%), they needed help or to find someone who could help them deal with their feelings; and 3) physical activity (n = 16, 34%), they needed to know about their physical activity needs. Participants were then asked to rate the top five of their reported needs in order of priority, and 14 ASCC ranked nutrition (n = 7, 50%) and mental health (n = 7, 50%) (Fig. 2b) equally. Additional survey needs reported are presented in Supplementary Data S3.
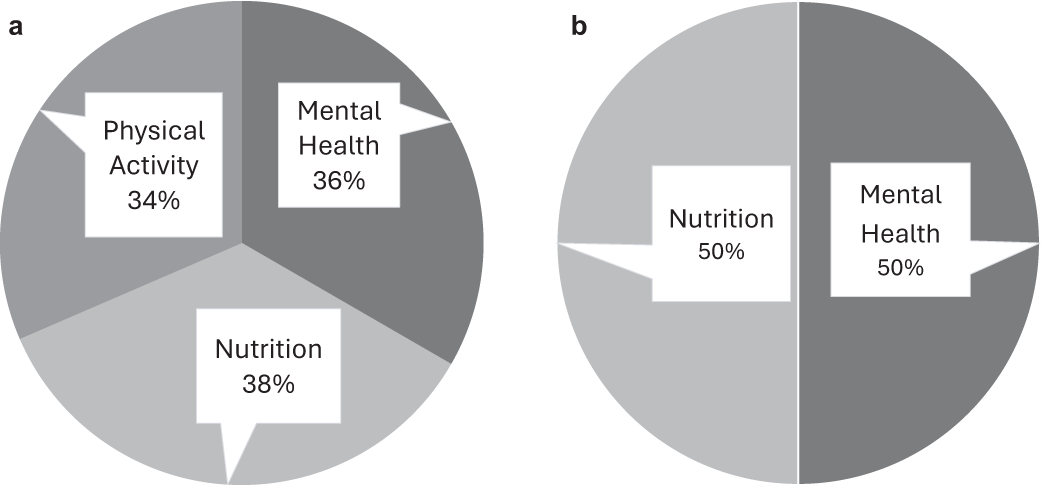
Adult Survivors of Childhood Cancer Survey Reported Needs at The Time of the Survey (Right Now).
Interview rapid analysis
The interview analysis generated gender-specific trends. Males shared that they appreciated the reinforcement of nutritional information at their survivorship visit and did not seek mental health support. Male participants offered that “whenever I go to the survivorship visits, I feel like it does genuinely help with nutrition” (Participant #2) and “it’s [mental health support] something I have to kind of like push aside and in order tothink about like my treatment” (Participant #1). Females found it challenging to maintain a nutritious diet despite survivorship visits during and immediately following college. They also expressed feelings of anxiety and guilt surrounding their cancer experience and found help through therapy. Female participants shared that it’s hard to maintain a specific diet in college (Participants #3 and #4), and one expressed that spending time with a psychologist “healed me a lot mentally and also just emotionally” (Participant #3).
Discussion
In this study, we conducted open- and closed-ended surveys and semi-structured interviews to identify the needs of survivors as they transition to LTFUC. Based on these data, the ASCC Clinic program at LCI’s DSO was established to include specialized services to address these identified issues. Analysis revealed overarching needs concerning nutrition, mental health, and physical activity.
Our participants align with a recent patient-centered study focusing on adolescent and young adults (AYAs), which also reported that the majority of its participants identified as White and female. 17 And, like another CCS study 18 in the Netherlands, our analysis revealed that participants reported multiple needs. Our survey showed that nutrition, mental health, and physical activity were the most frequently reported needs, with nutrition and mental health receiving the highest priority. This demonstrates that survivors know that lifestyle factors, such as nutrition and mental health, are essential to their well-being and future health. They acknowledge ongoing needs for information reinforcement across this period of life as social factors and resources change (i.e., they move out independently and have jobs with variable salaries and insurance coverage).
Interviews highlighted that male participants were less likely to seek out mental health, while female participants struggled the most with their nutritional needs posttreatment. Similar to our programming informed by the survey and interviews, mental health was a top element in the AYA patient-centered model of care developed by Figueroa Gray et al., who recognize the importance of repeated support over time. 17 Other research showing similar concerns about nutrition has proposed a “stepped care model,” in which CCS can progress through levels of evidence-based interventions as outcomes are assessed. 19 With nutrition and dietary interventions already recognized as key factors in secondary prevention, specific nutritional programming can represent useful tools 20 for survivors transitioning through to LTFUC and emerging adulthood.
Based on these results, the services added to the ASCC Clinic program include a social worker for mental health concerns and an exercise specialist to support physical activity. The ASCC Clinic already provided nutrition services during this QI study. In the DSO shared care model, we emphasize a clear transition plan and targeted CCS services to ensure the ongoing reinforcement of healthy behaviors during this development time.
This study has strengths and limitations. A strength was the multidisciplinary working group stakeholders (Fig. 1) who identified survivors to meet the study recruitment goals. This population can be hard to reach, 21 and recruitment help was vital to our success. Limitations include the predominance of White and female participants. Our data may not capture the full range of experiences and needs across different communities, potentially missing crucial insights from under-represented minorities. To resolve this, we learned that recruitment should involve a multifaceted approach, including the consideration of social media engagement, which can support future recruitment efforts. 22 Lastly, the interview findings are limited because the participants represent only a small portion of clinic patients, and the data were analyzed by a single researcher (D.M.B.).
Further implementation work is needed to explore how nutrition, mental health, and physical activity services impact CCS’s quality of life and continued involvement in LTFUC and the ASCC Clinic. This future work would be informed by evaluation metrics demonstrating improved service utilization, measured by an increase in referrals to a dietitian, and further supported by patient-reported outcome assessments, such as the Patient Health Questionnaire, a quick assessment tool for capturing depressive symptoms.
Conclusions
Our data demonstrate that survivors have multiple needs as they transition to LTFUC, and they prioritize nutrition and mental health as their top two survivorship care needs. Furthermore, it is noteworthy that males did not seek mental health help, while females did, and that males valued the reinforcement of nutritional information, while females struggled with nutrition in the context of college. We found no similar studies demonstrating this gender-specific trend. Combining survey and interview data is an innovative approach that supports patient voice representation to prioritize age-appropriate ASCC Clinic programming. Additionally, this methodology can be adjusted to guide future projects that serve other populations and cancer centers, including those with regional diversity and multiple locations. As survivors move through different developmental stages, their needs will change. A clear transition plan for survivors ensures the ongoing reinforcement of healthy behaviors during this development time. The implications of these results inform targeted program development to address nutritional, mental health, and physical activity needs explicitly through specialized services.
Authors’ Contributions
D.M.B.: Conceptualization, methodology, visualization, data curation, writing—original draft preparation. S.Y.: Validation, resources, writing—reviewing and editing. J.P.: Conceptualization, validation, resources, writing—reviewing and editing.
Footnotes
Acknowledgments
The authors would like to thank all the patients and caregivers and Jacqueline Edwards, our RN Clinical Coordinator, who helped to support this quality improvement study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This program development work was supported by funding from The Leon Levine Foundation.
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.