
Abstract
Purpose:
To explore the acceptability of the content and delivery of the age-specific cancer rehabilitation program Young Adults Taking Action (YATAC) from the perspective of young adult cancer survivors (YACSs).
Methods:
Nineteen YACSs (aged 18–39) participated. Program acceptability was explored through four focus groups. The Theoretical Framework of Acceptability guided data collection and analysis. Data from the focus groups were deductively analyzed using framework analysis.
Results:
The YACSs found the YATAC program acceptable and relevant to their needs. The participants reported enhanced physical self-efficacy, improved mood, greater acceptance of their condition, reduced loneliness, and increased confidence in managing daily life. Peer support, practical exercises, and tailored content were identified as particularly valuable. Referring to delivery acceptance, participants described the program format as engaging and supportive, though some found the intensive schedule burdensome. Few suggested removing content; instead, they recommended extending sessions and adding topics such as diet, fertility, and cognitive concerns. The participants also highlighted the need for clearer guidance on accessing resources after the program. Group discussions were generally beneficial; however, some participants expressed discomfort around discussing sensitive topics in mixed settings.
Conclusion:
The YATAC program was well received and perceived as beneficial by YACSs, particularly when sessions were practical, peer-supported, and individualized. The findings support the program’s continued development and refinement.
Implications for Cancer Survivors
: This study highlights the importance of peer interaction and personalized content and thoughtful delivery design in survivorship care for young adults. Future research should explore long-term and wider outcomes.
Introduction
Late effects and reduced participation in everyday life after cancer treatment among young adult cancer survivors (YACSs) aged 18–39 are major concerns for these individuals and for society.1–4 Globally, approximately one million young adults are diagnosed with cancer every year, with 1600 cases in Denmark.5–7 Due to advances in cancer detection and treatment, young adults with cancer have a high 5-year survival rate ranging from 83% to 86%. 8 However, they face a high risk of severe, multiple, and age-specific late effects, which may persist or emerge decades beyond treatment.4,9–12 In particular, this is due to the intensive, multimodal, and prolonged treatment that YACSs often undergo, combined with the disruption of key developmental milestones such as education, career, and family-building.13,14
Specifically, YACSs often experience simultaneous physical and psychological challenges, including fatigue, sexual health issues, fertility concerns, fear of recurrence, depression, and anxiety, which hinder their participation in education, work, leisure, and social life.4,15–20 In addition, studies show that YACSs lack confidence in managing life after treatment.21,22 The literature emphasizes the need for age-specific programs to enhance self-efficacy in managing late effects and everyday participation.4,21,23,24 Rehabilitation is an interdisciplinary approach that addresses complex problems by focusing on the dynamic interaction between biological, psychological, social, and existential factors. It aims to improve functioning and participation and has been shown to enhance self-efficacy and health-related quality of life.25–28 Nevertheless, age-specific rehabilitation programs for YACSs remain limited.4,24,29,30
To address the lack of rehabilitation programs tailored to the specific needs of YACSs, a comprehensive age-specific, goal-oriented, and peer-based rehabilitation program called Young Adults Taking Action (YATAC) was codeveloped with YACSs and other stakeholders. 31 Before a full-scale feasibility study can be conducted, it is crucial to assess the program’s preliminary acceptability to identify areas for refinement and enhance sustainable implementation. This study explored the acceptability of the content and delivery of the YATAC program from the perspective of YACSs.
Method
Research design
This qualitative feasibility study explored the acceptability of the YATAC program. The study design, including the intervention structure and the evaluation plan, is described in detail in a previously published protocol 32 and registered on clinicaltrials.gov (NCT05551286).
The study is reported in accordance with the COnsolidated criteria for REporting Qualitative research Checklist, 33 which guided both study design and reporting to enhance transparency and methodological rigor. A completed COREQ checklist is provided as Supplementary Data.
Theoretical framework
The Theoretical Framework of Acceptability (TFA) was applied to assess the acceptability of the program’s content and delivery. 34 Developed by Sekhon et al., 34 the TFA provides a comprehensive conceptual model for evaluating how individuals perceive health care interventions, based on their anticipated or experienced cognitive and emotional responses. The framework has been widely used in previous studies to guide data collection and analysis related to the acceptability of health care interventions.35–38
In the TFA, acceptability is conceptualized as a multifaceted construct that can be assessed both prospectively, before an individual engages with an intervention, and retrospectively, after the intervention has been experienced. It defines acceptability as the extent to which an individual who receives or delivers an intervention considers the intervention appropriate based on anticipated or experienced cognitive and emotional responses to the intervention. 34
The framework comprises seven interrelated constructs: affective attitude, burden, ethicality, intervention coherence, opportunity costs, perceived effectiveness, and self-efficacy. These constructs capture participants’ emotional reactions, perceived effort, moral alignment, understanding, trade-offs, expected outcomes, and confidence in engaging with the intervention. 34 The constructs are described in detail in Table 1.
Description of the Constructs in the Theoretical Framework of Acceptability (TFA)

An individual could be the person receiving or delivering the intervention.
In this study, the TFA guided both the development of the semistructured interview guide and the deductive analysis of the focus group data, which enabled a structured and theory-informed exploration of the participants’ experiences.
Setting and time frame
The study was conducted at REHPA, the Danish Knowledge Center for Rehabilitation and Palliative Care, in Nyborg, Denmark. REHPA is a publicly funded research clinic that offers free residential rehabilitation stays for individuals with life-threatening diseases. 39 The study was conducted between May and November 2022.
Participants and recruitment
The eligibility criteria were (1) aged 18–39 at the start of the program, (2) diagnosed with any type of cancer, (3) had completed primary/active cancer-directed treatment (cytotoxic chemotherapy, radiation therapy, and/or definitive surgical intervention; hormonal treatments or maintenance therapies were allowed), (4) independent in personal activities of daily living, (5) able to speak and understand Danish, (6) access to an internet-enabled device (e.g., smartphone or tablet), and (7) willing to provide written informed consent.
Participants were recruited between May and September 2022 through multiple channels. Information about the program was distributed to municipalities, relevant hospital departments, and the websites and social media platforms of REHPA and the nongovernmental organization Young Cancer at the Danish Cancer Society, and participants were referred to the program by their treating physician or a general practitioner.
The sampling strategy was purposive, aiming for diversity in gender, diagnosis, and time since treatment in order to capture a broad range of experiences. The recruitment goal was 20 participants, a fixed sample size based on REHPA’ capacity for each rehabilitation stay. Nineteen participants were ultimately included, which reflects full enrollment for the study period.
The program
The program aims to improve YACSs’ self-efficacy to manage everyday life and health-related quality of life. 31 It builds on the Social Cognitive Theory and John Dewey’s learning theory.40–42
The program includes 23 sessions delivered over the course of a five-day in-person residential stay and a two-day in-person residential follow-up stay ten weeks after the five-day stay. An online follow-up session was held five weeks after the five-day residential stay. 32 Details of the content, duration, delivery, and providers are in Table 2, in accordance with the Template for Intervention Description and Replication checklist. 43 All sessions were mandatory except for the work and education component, in which the participants chose either return-to-work or return-to-education sessions. 32 Each session followed Cole’s seven steps of group intervention: introduction, main activity, sharing, processing, generalization, application, and summary. 44
Description of the Content, Duration, and Delivery Form of Each Component of the Program at REHPA
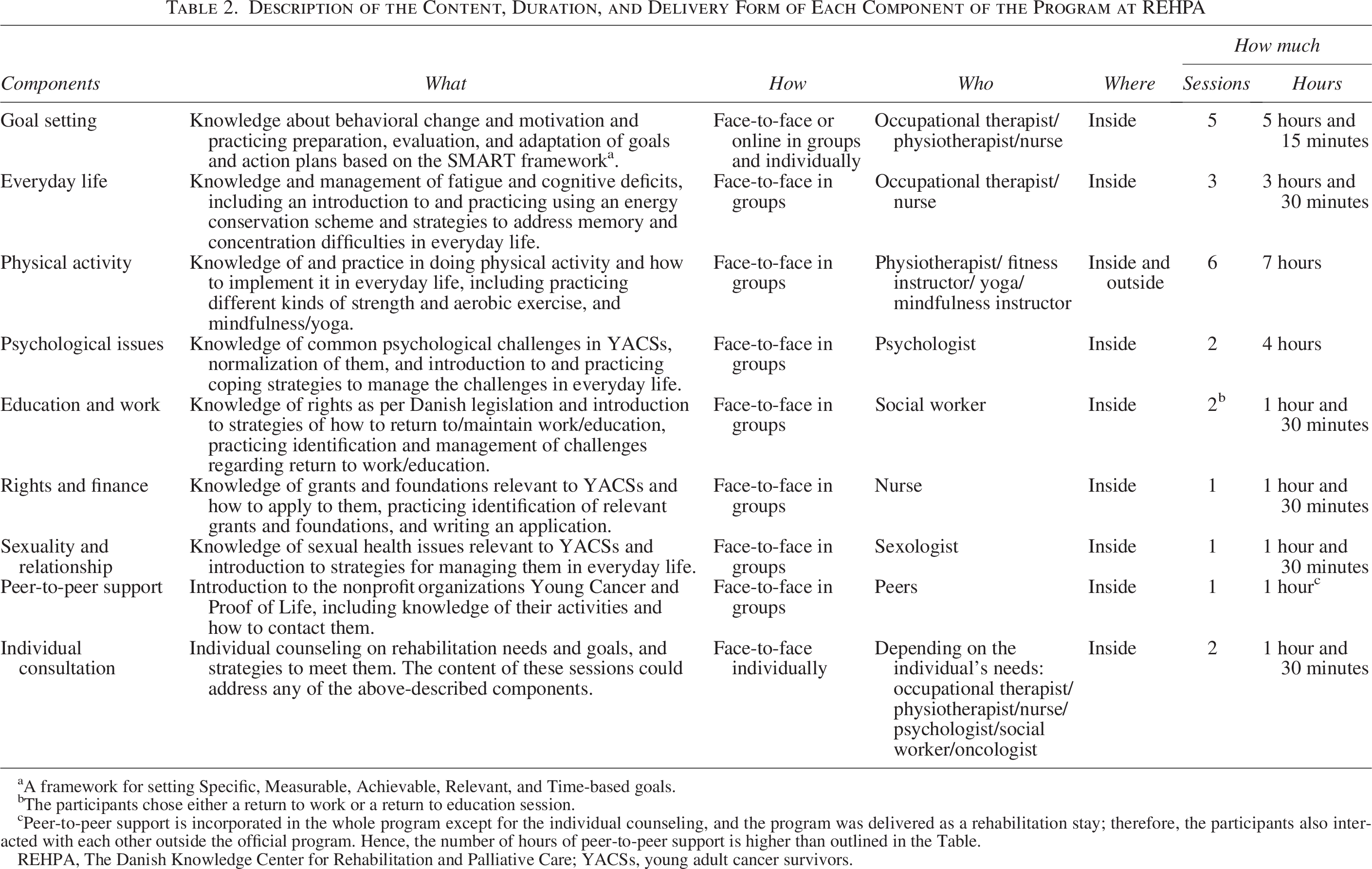
A framework for setting Specific, Measurable, Achievable, Relevant, and Time-based goals.
The participants chose either a return to work or a return to education session.
Peer-to-peer support is incorporated in the whole program except for the individual counseling, and the program was delivered as a rehabilitation stay; therefore, the participants also interacted with each other outside the official program. Hence, the number of hours of peer-to-peer support is higher than outlined in the Table.
REHPA, The Danish Knowledge Center for Rehabilitation and Palliative Care; YACSs, young adult cancer survivors.
Data collection
Demographic and clinical characteristics were collected using Research Electronic Data Capture (REDcap) and included age, gender, living arrangements, marital status, children, education, employment, cancer type, time since diagnosis, and treatment modalities. 45
Data on the program’s acceptability to YACS were collected through four focus groups, two conducted after the five-day residential stay and two after the two-day follow-up. The focus groups were chosen to enable rich, interactive discussions and diverse perspectives. 46 All 19 participants took part. Each focus group comprised 9 to 10 participants.
The focus groups took place in a quiet room at REHPA and were moderated by a female physiotherapist and PhD scholar trained in qualitative interviewing. A nonparticipant observer, either a female PhD scholar with a background in nursing or a male PhD scholar who is a physiotherapist, attended each focus group to ensure coverage of all topics and questions outlined in the interview guide and comprehensive note-taking and reflexivity. None of the members of the research team conducting the focus groups had any prior relationship with the participants.
All the focus groups followed the same semistructured interview guide, which was developed using the seven constructs of the TFA framework34,46 as outlined in Table 3. The interview guide was pilot tested prior to the focus groups. Before each focus group, the interviewer introduced herself, explained the purpose of the interview, outlined the data handling procedures, and encouraged the participants to speak openly. The interview setting was designed to encourage open and reflective dialogue to enable the participants to share their experiences in depth and build on each other’s responses. The first author facilitated the discussions by posing follow-up questions when appropriate, which allowed the participants to shape the conversation and emphasize topics they considered meaningful. All the focus groups were audio-recorded, transcribed verbatim, and pseudonymized to protect the identity of the participants. The transcripts were not returned to the participants for review. On average, the focus groups lasted 57 minutes (range: 53–60 minutes).
The Semi-Structured Interview Guide
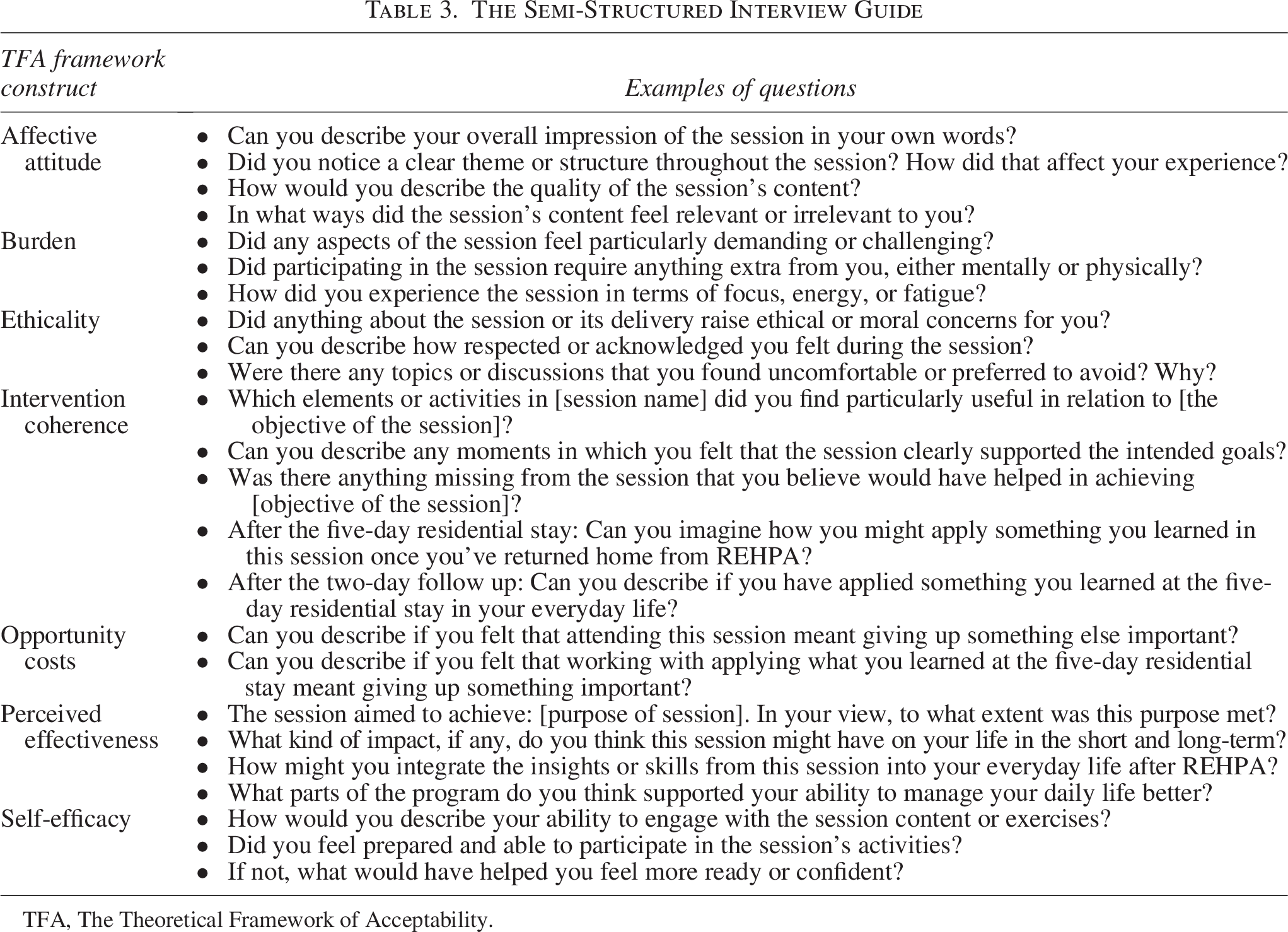
TFA, The Theoretical Framework of Acceptability.
Data analysis
The data were analyzed using the Framework Analysis approach, guided by the TFA constructs,34,47 which informed the identification and organization of the study’s main themes. The analysis followed the five systematic steps of Framework Analysis: (1) Familiarization, (2) Developing a coding framework, (3) Indexing, (4) Charting, and (5) Mapping and interpretation. 47 The first and last authors independently conducted steps 1–4. During the familiarization step, they listened to the audio recordings and read the transcripts several times to gain an overall understanding of the data (Step 1). Next, they independently coded each transcript and applied an initial coding framework based on the seven TFA constructs (Steps 2 and 3). The data were then charted by grouping coded segments under the relevant TFA constructs, and potential quotes that vividly represented the constructs were noted (Step 4). The two authors cross-compared their results and discussed their coding, resolving any discrepancies through discussion until consensus was reached. In the final step (Step 5), the first and last authors collaboratively explored patterns and relationships within and across the TFA constructs to generate overarching interpretations and selected illustrative quotes to support their findings. The results were then reviewed and discussed with the wider author group to ensure credibility and consistency. Data saturation was considered achieved after the fourth focus group, as no new themes or insights emerged.
Participant validation (member checking) was not undertaken, as the findings were grounded in a clearly structured theoretical framework, and as cross-researcher triangulation was prioritized for credibility.
Ethics approval
This study was conducted in accordance with the Declaration of Helsinki and approved by the Danish Data Protection Agency (22/28502). The Regional Ethics Committee of Southern Denmark determined that ethical approval was not required (20222000-50). All participants provided written informed consent. The data were securely stored on a password-protected server at Odense University Hospital, and confidentiality was maintained through pseudonymization.
Results
Twenty-five YACSs were referred, but five did not meet the inclusion criteria, and one canceled shortly before the rehabilitation stay. Hence, the final sample consisted of 19 YACSs, the majority of whom were women with breast cancer. The demographic and cancer-related clinical characteristics of the participants are presented in Table 4.
Demographic and Cancer Related Clinical Characteristics for the Included Young Adult Cancer Survivors (n = 19)
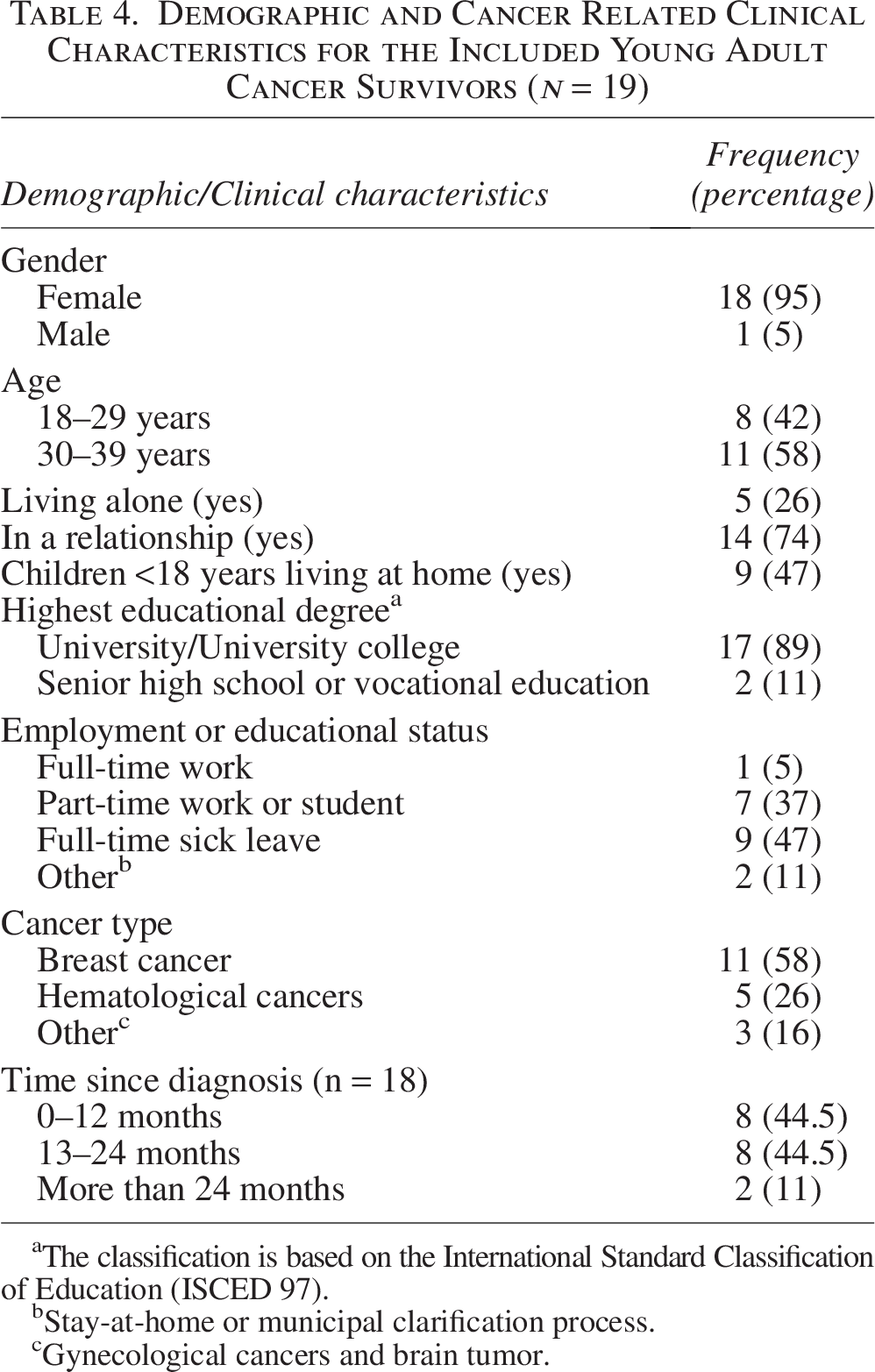
The classification is based on the International Standard Classification of Education (ISCED 97).
Stay-at-home or municipal clarification process.
Gynecological cancers and brain tumor.
Affective attitude
Overall, the participants expressed a very positive view of the program. Some prospectively thought that specific sessions might not be relevant or beneficial to them. However, they found that these sessions provided valuable knowledge and practical tools for addressing their challenges (Table 5, Quotes 1 and 2).
Participant Quotes Aligned with Theoretical Framework of Acceptability Framework Constructs
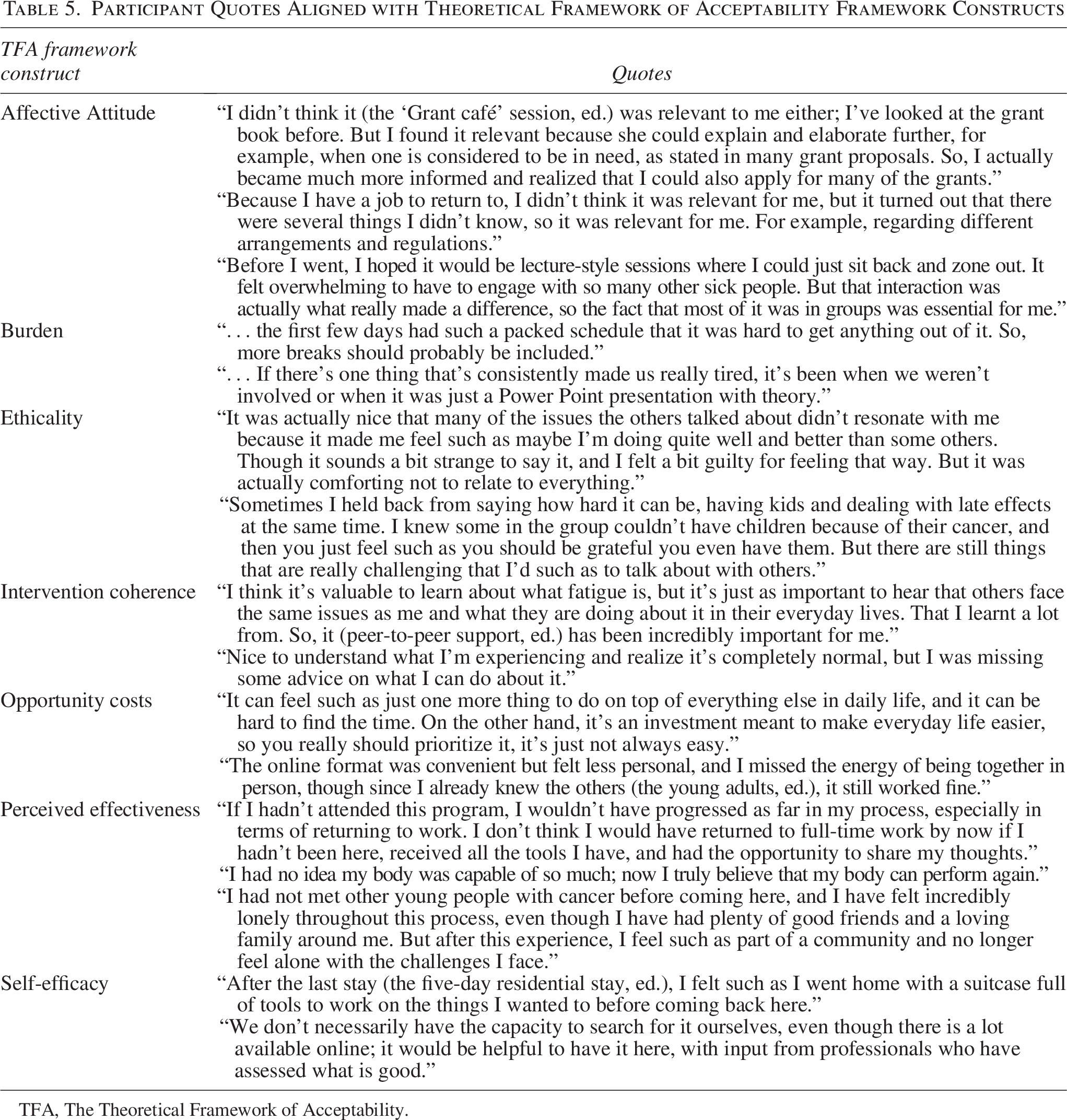
TFA, The Theoretical Framework of Acceptability.
In general, the participants found the content of the sessions relevant and in line with their needs. How the content was delivered was mentioned as essential for how acceptable they found the sessions. The participants highlighted that the providers’ capacity to engage beyond the formal presentation significantly impacted their perception of the sessions. Furthermore, there was broad agreement that it enhanced the relevance and relatability of the content of the sessions when participants’ specific situations, challenges, and personal experiences were used as a starting point. This approach also facilitated better retention of the presented knowledge and theory.
All participants agreed that peer-to-peer support through group sessions was very rewarding and meaningful. Some participants expressed initial concerns about the group sessions, either because they identified as introverted or because they feared that they could not manage being around many other sick individuals (Table 5, Quote 3).
Burden
The participants described the 5-day residential stay as intense, which left some feeling fatigued and made it difficult for them to concentrate and engage in some sessions (Table 5, Quote 4). Conversely, the participants were unable to identify any elements or content that seemed less relevant or could be removed to allow for more breaks. Instead, they expressed a desire for additional time, particularly during the sessions “Psychological issues” and “Education and Work,” to delve deeper into their individual situations and receive personalized guidance.
The participants reported that too much theory and lack of active involvement as participants in sessions was burdensome and fatiguing (Table 5, Quote 5). For example, they found the “Fatigue—what can I do?” session very theory-heavy and challenging. However, when they engaged directly with the energy conservation techniques in the subsequent workshop, the material became more relatable and personalized, which renewed their engagement. They also described that it was very useful to gain knowledge about the distinction between tiredness, fatigue, and exhaustion, and how these interact.
Ethicality
Although peer-to-peer support was generally viewed as a beneficial element and as acceptable, it also challenged the morals of some participants (Table 5, Quote 6). Some participants with children felt uncomfortable discussing parenting challenges in group sessions, knowing that others in the group had faced reduced fertility or infertility due to their cancer (Table 5, Quote 7). Hence, several participants suggested holding a separate session for YACSs with children to discuss issues related to this.
Intervention coherence
The participants reported that they understood how providing them with knowledge, strategies, practical exercises to manage everyday life, and peer-to-peer support contributed to the overall program aim. They exemplified this by pointing out that they had received and worked with tools that supported them in managing some of their challenges. In particular, they mentioned the goal-setting form as extremely tangible and easy to use, and useful to take home and apply in everyday life. The same applied to the energy conservation forms in the session “How can I distribute my energy?”
The participants reported that being introduced to relevant knowledge that supported them in addressing everyday challenges was important to enhance their lives. Specifically, they found information on managing fatigue and cognitive deficits, understanding their rights under Danish legislation, recognizing common psychological challenges, and addressing sexual health issues to be particularly useful. Some participants also noted that knowledge in combination with sharing experiences with other YACSs was important to them to cope with their challenges (Table 5, Quote 8). Furthermore, they expressed a desire for additional activities and opportunities to apply the knowledge in practical, real-world contexts, thereby making it more relevant and actionable for their specific situations (Table 5, Quote 9).
Opportunity costs
None of the participants expressed that the program required them to sacrifice any benefits, profits, or values. However, there was broad consensus that integrating rehabilitation into a daily routine already filled with practical tasks, family obligations, work or studies, and leisure activities can be challenging (Table 5, Quote 10).
Some participants noted that the online component, the follow-up sessions on “Goals and direction,” made balancing work, studies, and everyday life easier. Nonetheless, they felt that the online format was less personal and more distant, lacking the immediacy and atmosphere of in-person sessions (Table 5, Quote 11).
Perceived effectiveness.
Generally, the participants described that the program helped them to manage different challenges in their daily lives, which improved their lives (Table 5, Quote 12). Several participants reported experiencing a sense of mastery, both during sessions and between the stays, in terms of their physical abilities and managing everyday life. For example, several participants described increased self-efficacy regarding their physical abilities after the session “SilentFit” (Table 5, Quote 13). Furthermore, the participants reported better mood, acceptance of their situation, and a reduced feeling of loneliness after the program (Table 5, Quote 14).
Some participants considered that expanding the program to include knowledge about diet and fertility issues and a cognitive and memory assessment had enhance the program’s effectiveness.
Self-efficacy
Overall, the participants said that they were able to complete the sessions and the required work between the two stays (Table 5, Quote 15). However, they emphasized that the lack of specific information on where to access additional knowledge, tools, or resources limited their ability to actively apply what they had learned to their daily lives. For instance, many found “MediYoga” relevant but lacked specific information and guidance on where they could practice it in their local community (Table 5, Quote 16).
Discussion
This study explored the acceptability of the YATAC program among YACSs, using the TFA framework. Overall, the content and the delivery of the program were perceived as acceptable, and the participants identified elements related to all seven TFA constructs. However, some constructs were more prominently reflected in the participant feedback than others.
The participants expressed highly positive affective attitudes toward the program, reporting that its content was well aligned with their needs. This is perhaps unsurprising, given that the program was codeveloped with YACSs to enhance relevance and engagement.31,48 Many participants shared characteristics with the codesign group (e.g., well-educated women with breast cancer), which may have enhanced its relevance. 31 Nevertheless, these findings are noteworthy, as young adults are typically less inclined than older adults to engage with interventions that do not align with their values and preferences.49,50 When individuals perceive external pressure to adopt approaches that do not align with their needs, they may reject the intervention’s message and disengage from participation.49,50
As in previous studies, the participants highly valued the peer-to-peer support component.51–53 However, the group format raised ethical concerns; some withheld personal experiences to avoid upsetting others, particularly on sensitive topics such as parenting, an issue linked to guilt and isolation in the literature.54,55 This highlights the potential benefit of optional or subgroup-specific sessions. Peer exposure has previously been found to sometimes provoke anxiety; 55 however, this was not evident here. On the contrary, some participants felt reassured by hearing about others’ greater challenges and gaining a different perspective on their own situations.
The participants also demonstrated a clear understanding of the intervention’s coherence and purpose. They particularly valued the use of goal setting to help improve the management of everyday challenges. This was somewhat unexpected, as previous studies have described goal setting as a difficult aspect of rehabilitation, even in programs tailored to young adults with cancer.53,56 Interestingly, several studies suggest that the primary barrier to effective goal setting lies not with the patients, whose perspective was explored in this study, but with the health care professionals, who may struggle to adapt their clinical routines and communication style. 56
The opportunity costs were not directly reported; however, the participants acknowledged that balancing the program with everyday demands could be challenging. Many YACSs juggle work, education, and caregiving responsibilities alongside their rehabilitation needs—a challenge documented in existing literature. 57 To facilitate integration into daily life, online delivery formats were recommended. Such formats have previously been found acceptable and feasible for YACSs.30,58 Nevertheless, evidence suggests that face-to-face peer support may be more effective in enhancing self-efficacy, perceived control, and cancer-related knowledge compared with online peer support. 59
The participants perceived the YATAC program as effective, reporting increased confidence in managing daily activities and reduced feelings of loneliness—outcomes that are aligned with the program’s theoretical foundation and with prior research.53,60,61 Interactive sessions were preferred, whereas theory-heavy content felt burdensome. The participants also recommended adding cognitive assessments and information on diet and fertility—areas previously identified as important.62–64 Although diet was excluded during the coproduction process, the current findings suggest that it should be considered in future versions. 31
Although the participants generally felt confident in engaging with the program, they expressed a need for clearer guidance on accessing additional resources. This may reflect fatigue, cognitive challenges, or lower health literacy, which is common among young adults and linked to difficulties with navigating complex health care systems. 65 However, as health literacy was not assessed, these interpretations should be treated with caution.
Strength and limitations
This study’s strength lies in its participant-focused approach and use of a structured framework to explore the acceptability of the YATAC program to YACSs. Including all participants in the focus groups ensured diverse insights, and data saturation was achieved through a transparent, validated analysis. The limitations include underrepresentation of men, ethnic minorities, and varied cancer types. Although the results are not generalizable, their consistency supports the validity of the findings.
Conclusion
The YATAC program was deemed acceptable by the YACSs, who reported enhanced physical self-efficacy, improved mood, greater acceptance of their condition, reduced feelings of loneliness, and increased self-efficacy in managing everyday life. The program was perceived as particularly effective when the sessions were practical, peer-supported, and tailored to individual needs. The participants suggested improvements such as longer sessions; the inclusion of additional topics such as diet, fertility, and cognitive concerns; and clearer guidance on accessing relevant resources. The findings provide valuable insights for future program development, including the refinement of context—mechanism–outcome configurations and the design of broader interventions. Further research is needed to assess the program’s long-term impact and its applicability across more diverse and representative populations.
Authors’ Contributions
Conceptualization of the research project: M.A., M.S.P., M.A.H., and K.l.C.; Methodology and data collection: M.A., D.S.J., M.S.P., and K.l.C.; Formal analysis: M.A. and K.l.C.; Writing—original draft preparation: M.A.; Writing—review and editing: M.A., M.S.P., M.A.H., and K.l.C.; Supervision: M.S.P., M.A.H., and K.l.C.; Project administration: M.A.; All authors have read and agreed to the published version of the article.
Footnotes
Acknowledgment
The authors are grateful to the YACSs who participated in the program and to REHPA for hosting the program. The authors extend the thanks to the professionals who delivered the program and the staff who assisted with its operation. Special thanks to Birthe Kargaard, Christina Wendelboe, Christina Strandsberg, and Signe Hulsbæk. The authors would also like to express the gratitude to Mod!Kræft at Zealand University Hospital, Roskilde; Kræftværket at Rigshospitalet, Copenhagen University Hospital; Livskræften at Odense University Hospital; Frirumm1 at Aarhus University Hospital; and the patient organization Young Cancer at the Danish Cancer Society for helping with recruitment. The authors would like to thank Anne Therese Karlsson and Jens-Jakob Kjer Møller for their assistance with the focus groups. Finally, the authors acknowledge OPEN, Open Patient data Explorative Network, Odense University Hospital, Region of Southern Denmark, for their support and services related to OPEN REDCap.
Author Disclosure Statement
The authors have no relevant financial or nonfinancial interests to disclose.
Funding Information
M.A. received a PhD grant from the Region of Southern Denmark (19/37135). In addition, the study is funded by REHPA, which receives financial support from the Danish Government.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.