
Abstract
Purpose:
Previous literature suggests that age does not impact outcomes in women with triple-negative breast cancer (TNBC). Young women have a higher rate of achieving pathologic complete response (pCR); however, the impact of age on outcomes and the type of surgery performed following neoadjuvant chemotherapy (NAC) is not well studied.
Methods:
An institutional retrospective database review identified women with TNBC who underwent NAC followed by surgery from 03/2010 to 09/2019. Clinicopathologic, treatment, and outcome variables were compared between women aged <40 and ≥40 years at diagnosis. The association between type of surgery and outcomes was examined.
Results:
Among 515 women, 104 (20%) were aged <40 years and 411 (80%) were ≥40. Compared to women ≥40, younger women presented at a similar clinical stage; were more likely to have a high-penetrance gene mutation, a higher overall pCR rate, and undergo a mastectomy; and less likely to receive adjuvant radiotherapy (all p < 0.01). Median follow-up was 2.8 years (interquartile range 1.6–4.7). 5-year locoregional recurrence (LRR) and distant recurrence (DR) rates did not significantly differ between these 2 age groups (LRR/7.9% vs. 8.7%, p = 0.6; DR/15.2% vs. 18.4%, p = 0.6). On multivariable analysis, lymphovascular invasion and nodal positivity were significantly associated with a decrease in overall and breast-cancer-specific survival. Age <40 years was not associated with survival. Women who opted for bilateral mastectomy were more likely to achieve a pCR.
Conclusions:
Young age was not an independent predictor of recurrence and survival outcomes in women with TNBC treated with NAC. Further studies with ongoing advancement in NAC are crucial.
Triple-negative breast cancer (TNBC) represents a challenging subtype that lacks expression of the estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2). Accounting for 15%–20% of breast cancer cases, TNBC is known for its aggressive clinical behavior and poor overall prognosis.1–3 Young women diagnosed with breast cancer are disproportionately affected by the triple-negative subtype. 4 Additionally, younger women with TNBC are more likely to present with more aggressive tumor features, including larger tumor size, higher histological grade, and increased rates of nodal involvement. 5 Studies examining the relationship of young age to survival according to different breast cancer subtypes have demonstrated no clear increased risk of breast cancer mortality in young women with TNBC. 6
In operable TNBC, the preoperative delivery of chemotherapy has become the standard approach to reduce tumor burden and improve surgical outcomes. Neoadjuvant chemotherapy (NAC) offers valuable insight into treatment response and provides the opportunity to individualize additional treatment recommendations in the adjuvant setting. Additionally, NAC may shrink the tumor, potentially allowing for breast-conserving surgery (BCS) and axillary de-escalation.7–11 A pooled analysis of eight prospectively randomized neoadjuvant trials of all breast cancer subtypes has demonstrated that young women have a higher risk of relapse and death compared with women age 40–49 years and women age ≥50 years. Unlike young women with hormone receptor (HR) positive/HER2 negative tumors who sustained worse outcomes, women aged <40 years with TNBC were more likely to obtain a pathologic complete response (pCR) compared to their older counterparts, yet showed no difference in risk of relapse or death. 12
Understanding how outcomes in a real-world setting are influenced by the addition of NAC in young women with TNBC is critical for optimizing management strategies for this vulnerable population. In this study, we compared patient characteristics, treatment, and outcomes among women aged < 40 and ≥ 40 years who were diagnosed with TNBC and received NAC.
Methods
Upon obtaining Memorial Sloan Kettering Cancer Center (New York, NY, USA) institutional review board approval, women with clinical stage I–III TNBC who underwent NAC followed by surgery between March 2010 and September 2019 were identified from a prospectively maintained database. We included 515 patients who had HR-negative tumors, defined by the absence of ER and PR and the absence of HER2 overexpression by either immunohistochemistry or fluorescence in situ hybridization. Clinicopathologic, treatment, and outcome measures were abstracted from medical records and compared in women age < 40 years to those age ≥ 40 years. We also sought to analyze whether there was an association between the type of surgery performed (partial mastectomy, unilateral total mastectomy, and bilateral mastectomy with contralateral prophylactic mastectomy [CPM]) and outcomes.
Race was self-reported and categorized as Black, Other, or White. At our institution, all surgeons perform a sentinel lymph node biopsy with dual-tracer for patients who were node positive and who became clinically node negative following NAC. pCR was defined as the absence of residual invasive tumor in the breast and ipsilateral axillary lymph nodes (ypT0/is ypN0). Locoregional recurrence (LRR) was defined as recurrence of disease in the ipsilateral breast, chest wall, or regional nodal basins. Distant recurrence (DR) was defined as recurrent disease elsewhere in the body. Data on dates of disease status and disease status at last follow-up (no evidence of disease, alive with disease, died of disease, died of other causes) were collected.
Categorical variables were summarized by frequency and percentages, while continuous variables were described using medians and interquartile ranges. A descriptive analysis with statistical comparisons was performed to evaluate associations of covariates by age and type of surgery. The Wilcoxon rank sum test was used to compare continuous variables, and the Fisher’s exact test or chi-squared test was used to compare categorical variables. LRR, DR, overall survival (OS), and breast-cancer-specific survival (BCSS) were estimated using the Kaplan-Meier method. Differences between the resulting survival curves were evaluated using the log-rank test. To account for the potential confounding effects of clinicopathologic features, we performed a multivariable analysis to determine associations of covariates with survival, including age as a forced predictor in a Cox regression model. All other covariates that were significant on the univariate Cox regression models at a type I error rate of 0.05 were included in the multivariable analysis. The final permissible type I error rate for multivariable analysis was set to 0.0125 after Bonferroni correction, given that we compared OS, BCSS, LRR, and DR. R 4.3 statistical software (R Foundation for Statistical Computing, Vienna, Austria) was used for all analyses.
Results
We identified a total of 515 women with stage I–III TNBC treated with NAC with a median follow-up time of 2.8 years (interquartile range 1.6–4.7). Twenty percent (n = 104) of women were age < 40 years, and 80% (n = 411) were age ≥ 40 years. Clinicopathologic characteristics according to age are shown in Table 1. Median patient age was 51 years (interquartile range 41–60). Women aged < 40 years were more likely to be of “Other” race than those ≥ 40 years (30% vs. 19%, p = 0.02). Fifteen women (2.9%) had inflammatory breast cancer (1 woman [1.0%] age < 40 years vs. 14 women [3.4%] age ≥ 40 years). Eight women (1.6%) had TNBC with metaplastic features (n = 0 [0%] in women age < 40 years vs. n = 8 [1.9%] in those age ≥ 40 years). Compared to women age ≥ 40 years, younger women presented at a similar clinical stage (of all patients, 6.4% were stage 1, 65% stage 2, and 29% stage 3) and had similar rates of lymphovascular invasion (LVI) (25%) and extracapsular extension in lymph node metastases (9.4%). Women age < 40 years were more likely to have high-penetrance gene mutations (35% vs. 14%, p < 0.001), receive a preoperative magnetic resonance imaging (MRI) (p = 0.03), and have an overall pCR (47% vs. 25%, p < 0.001) (Table 1).
Clinicopathologic Features Among Women with cT1-3 TNBC Treated with Neoadjuvant Chemotherapy who Underwent Surgery Between 2010 and 2019 According to Age
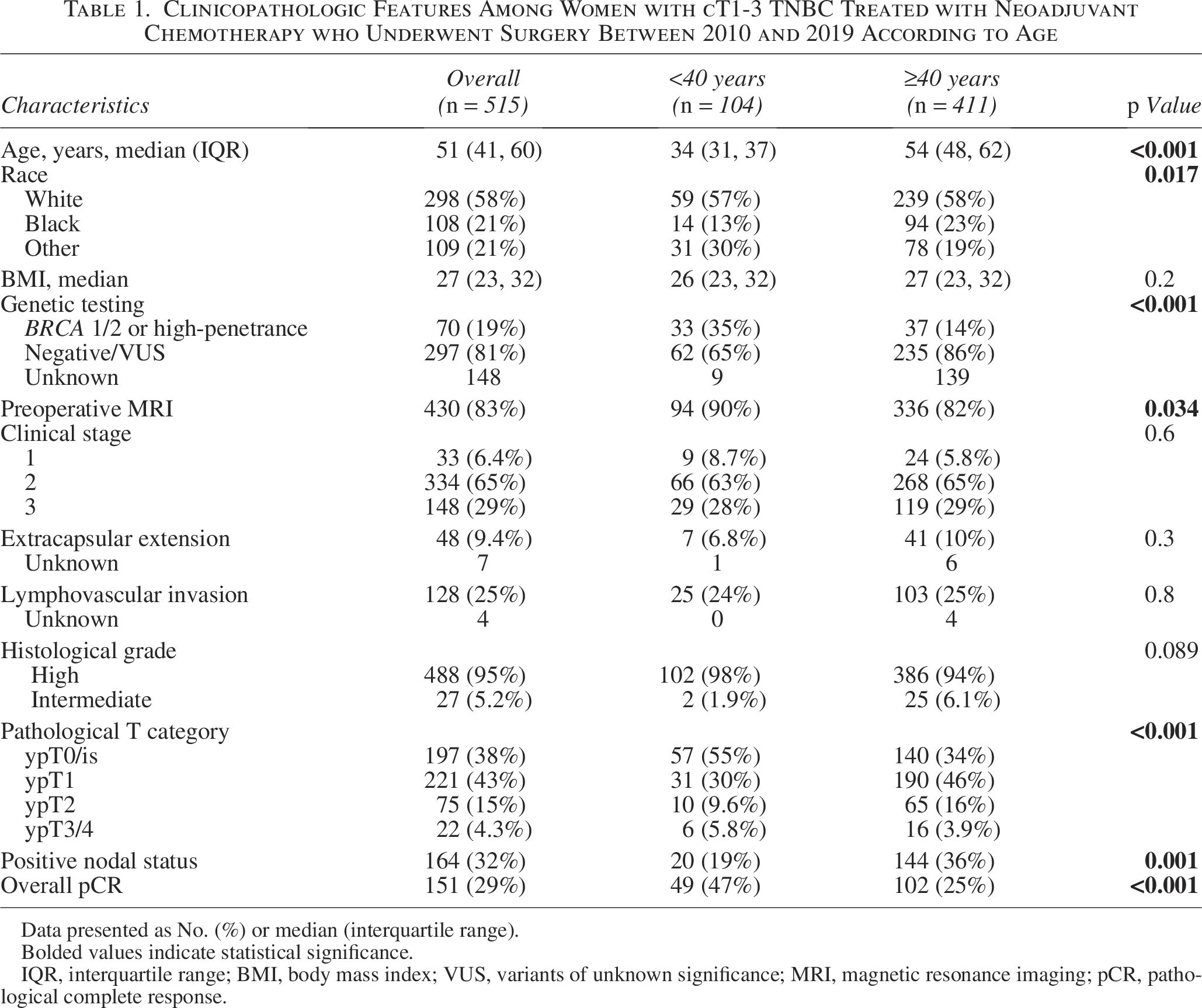
Data presented as No. (%) or median (interquartile range).
Bolded values indicate statistical significance.
IQR, interquartile range; BMI, body mass index; VUS, variants of unknown significance; MRI, magnetic resonance imaging; pCR, pathological complete response.
Table 2 summarizes the treatment our study population received. There was no difference in the type of chemotherapy regimens received between groups, with nearly 87% of women receiving an ACT (adriamycin, cyclophosphamide, and taxol)-based regimen. Among young women who received NAC other than ACT, 5 (4.8%) received taxane-based chemotherapy, 2 (1.9%) received anthracycline-based chemotherapy, and 4 (3.8%) received bevacizumab with ACT. Of women age ≥ 40 years who received NAC other than ACT, 25 (6.1%) received taxane-based chemotherapy, 10 (2.4%) received anthracycline-based chemotherapy, 8 (1.9%) received bevacizumab with ACT, 8 (1.9%) received CMF (cyclophosphamide, methotrexate, and fluorouracil), and 3 received other regimens. Women age < 40 years were more likely to undergo a mastectomy (75% vs. 47%, p < 0.001), less likely to undergo an axillary lymph node dissection (ALND) (31% vs. 44%, p = 0.019), and less likely to receive adjuvant radiotherapy (70% vs. 84%, p < 0.001).
Treatment Among Women with cT1-3 Triple-Negative Breast Cancer Treated with Neoadjuvant Chemotherapy who Underwent Surgery Between 2010 and 2019 According to Age
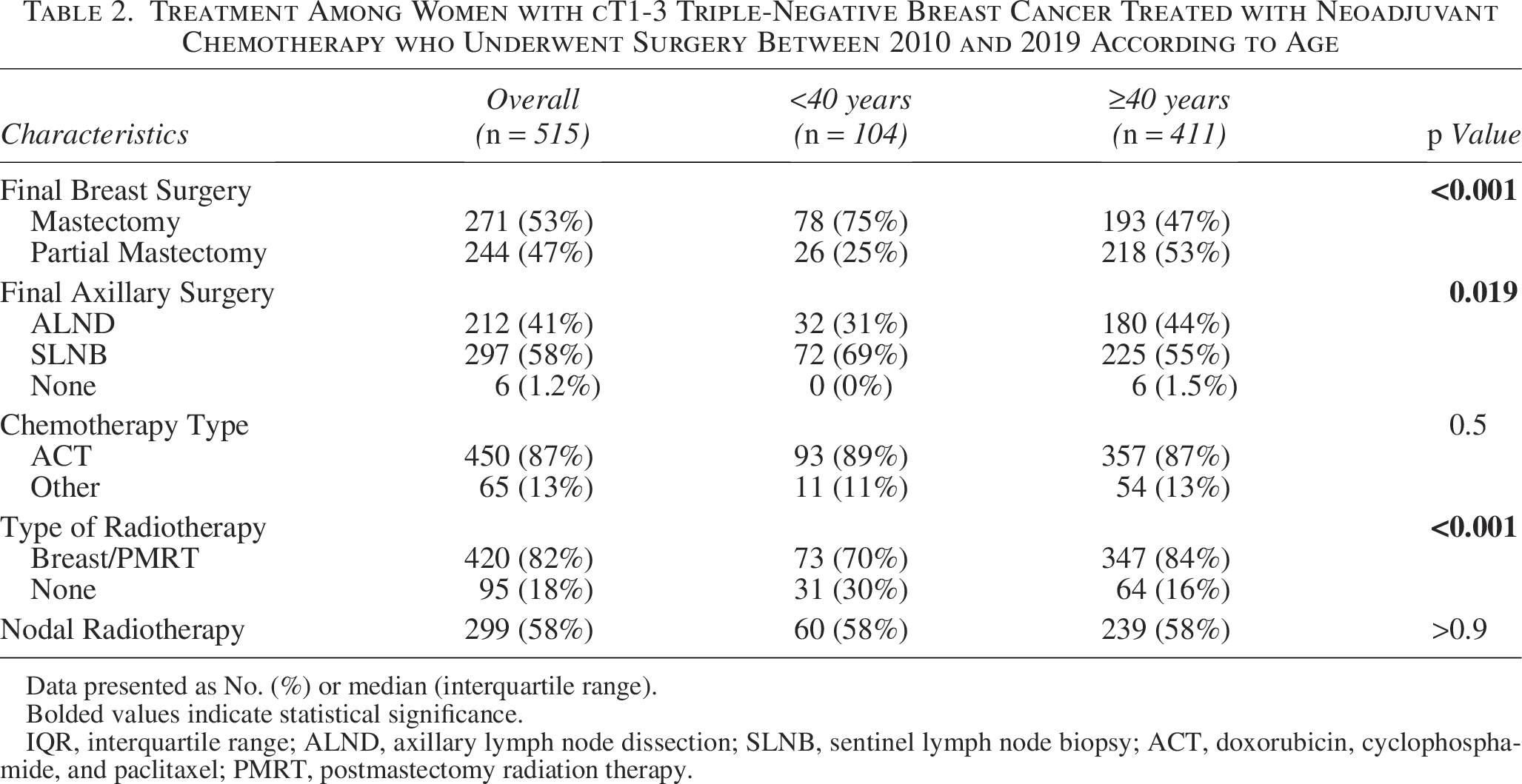
Data presented as No. (%) or median (interquartile range).
Bolded values indicate statistical significance.
IQR, interquartile range; ALND, axillary lymph node dissection; SLNB, sentinel lymph node biopsy; ACT, doxorubicin, cyclophosphamide, and paclitaxel; PMRT, postmastectomy radiation therapy.
Variables associated with type of surgery
Patient and treatment variables associated with the type of surgery were examined and are shown in Table 3. Patients were more likely to undergo bilateral mastectomy if they were younger (median age of 41 years compared to 54 years in those who received partial mastectomy and 55 years in those who received unilateral total mastectomy, p < 0.001) and of White race (p < 0.001). Factors associated with bilateral mastectomy included the presence of a BRCA or high-penetrance gene mutation and undergoing a preoperative MRI (both p < 0.001). Characteristics of more-aggressive tumor biology, including a higher clinical stage, extracapsular extension, LVI, higher pathological stage, positive nodal status, and lower overall pCR rate, were more likely to be seen in women who underwent unilateral total mastectomy than in those who received a partial mastectomy or a CPM. A significantly higher crude rate of recurrence and death was also seen in women who underwent unilateral total mastectomy (Table 3).
Clinicopathologic Characteristics and Outcomes Among Women with cT1-3 TNBC Treated with Neoadjuvant Chemotherapy According Type of Surgery Between 2010 and 2019
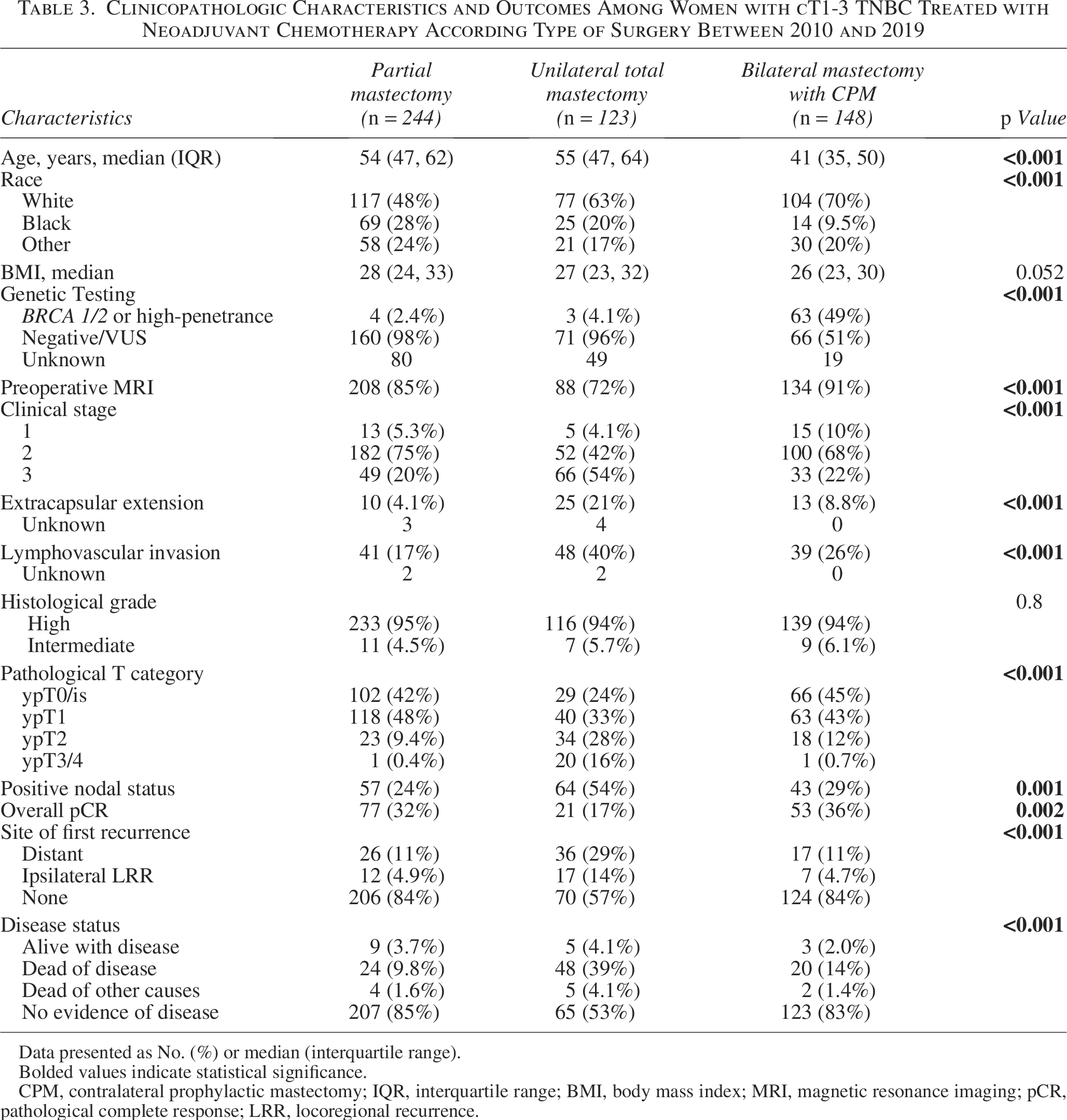
Data presented as No. (%) or median (interquartile range).
Bolded values indicate statistical significance.
CPM, contralateral prophylactic mastectomy; IQR, interquartile range; BMI, body mass index; MRI, magnetic resonance imaging; pCR, pathological complete response; LRR, locoregional recurrence.
Recurrence and survival outcomes
Overall, there were 36 LRR and 79 DR events; no difference in site of first recurrence was noted in women age < 40 years compared to those age ≥ 40 years (p = 0.7) (Table 4). The 5-year LRR rate was 7.9% (95% confidence interval [CI] 1.4–14%) in women age < 40 years compared to 8.7% (95% CI 5.5–12%) in women age ≥ 40 years and did not significantly differ between groups (p = 0.6) (Fig. 1A). The 5-year DR rate was not different in women age < 40 years compared to those age ≥ 40 years (15.2% [95% CI 7.4–22.4%] vs. 18.4% [95% CI 14–22.5%], p = 0.6) (Fig. 1B). On multivariable analysis, when adjusting for tumor characteristics and treatment, factors associated with the development of DR included LVI and positive nodal status, although LVI did not remain significant after Bonferonni correction (Table 5). Achieving a pCR was significantly associated with improved DR (hazard ratio [HR] 0.22, 95% CI 0.08–0.64, p = 0.006). Age and type of surgery were not significantly associated with DR.
Locoregional and Distant Recurrence Rates and Clinical Outcomes Among Women with cT1-3 TNBC Treated with Neoadjuvant Chemotherapy who Underwent Surgery Between 2010 and 2019 According to Age
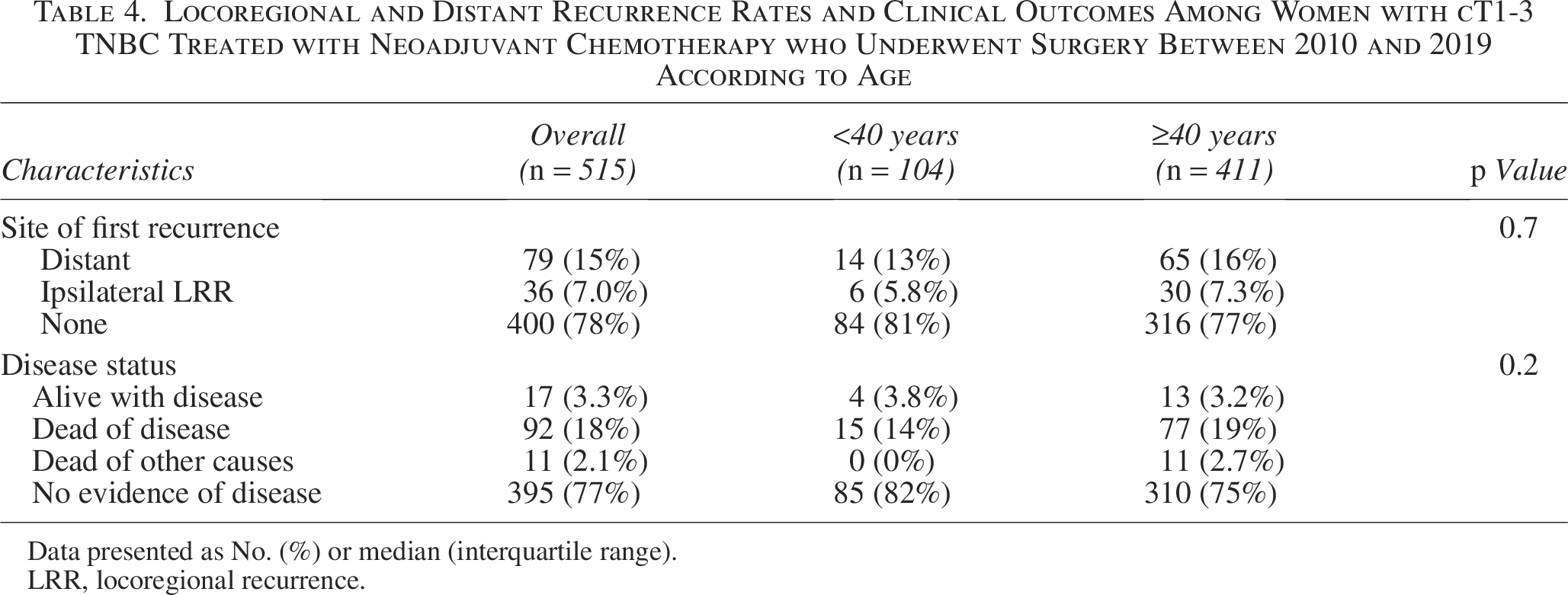
Data presented as No. (%) or median (interquartile range).
LRR, locoregional recurrence.
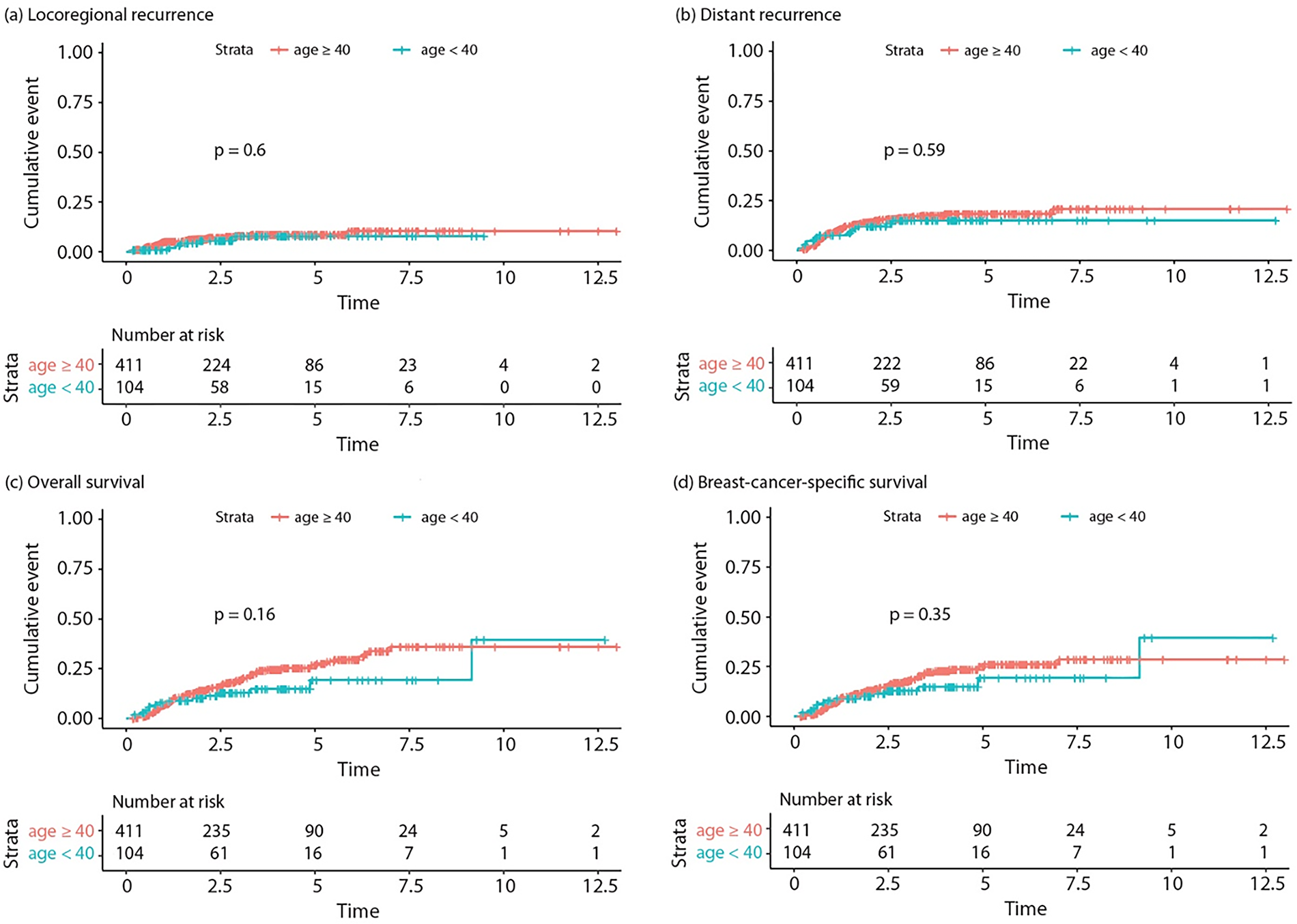
Survival plots comparing women age < 40 years to those age ≥ 40 years with triple-negative breast cancer treated with neoadjuvant chemotherapy;
Multivariable Cox Regression Analysis of The Association Between Age and OS and BCSS, Adjusted for Potential Confounders, Among Women with cT1-3 TNBC Treated with Neoadjuvant Chemotherapy who Underwent Surgery Between 2010 and 2019
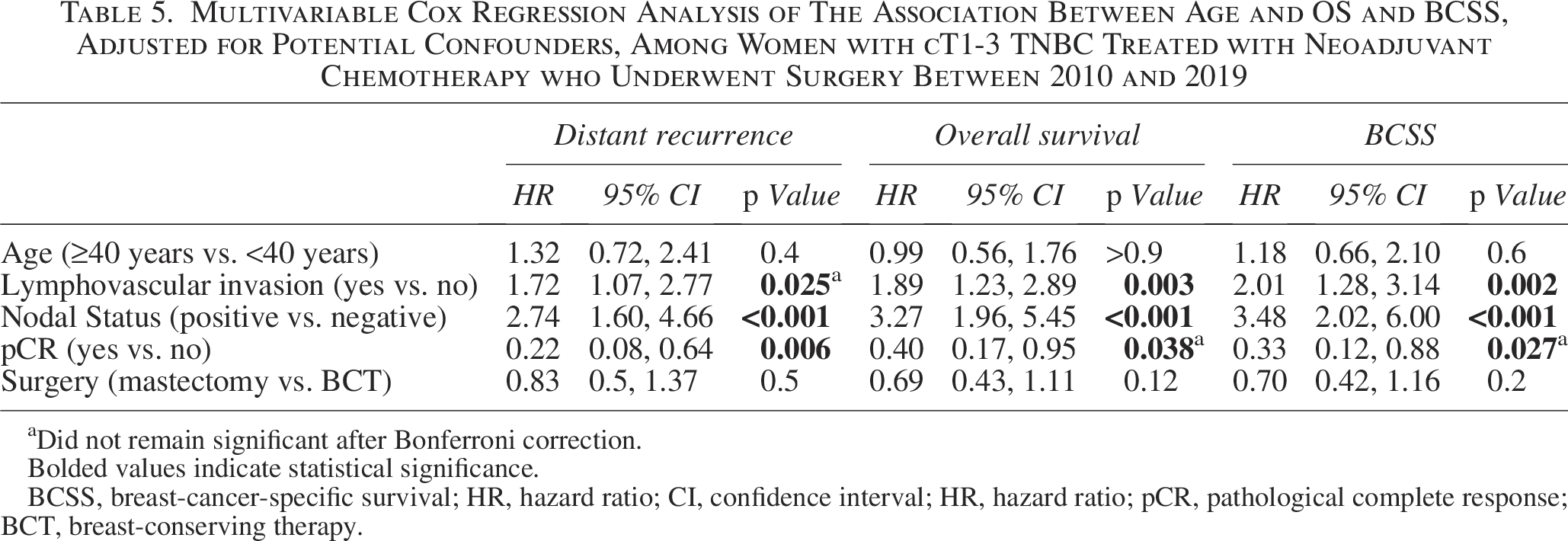
Did not remain significant after Bonferroni correction.
Bolded values indicate statistical significance.
BCSS, breast-cancer-specific survival; HR, hazard ratio; CI, confidence interval; HR, hazard ratio; pCR, pathological complete response; BCT, breast-conserving therapy.
There was no difference in survival outcomes according to age; 92 (18%) women died due to breast cancer at the end of the study (Table 4). On multivariable analysis, LVI, positive nodal status, and having residual disease were significantly associated with OS and BCSS (Table 5). Having residual disease, however, did not remain significant after Bonferroni correction. Age and type of surgery were not significantly associated with survival outcomes. When age was not forced into the multivariable model, there were no associations between the presence of a high-penetrance gene mutation and recurrence or survival outcomes (data not shown). The 5-year death rates were 19.3% (95% CI 7.3–29.8%) in women age < 40 years and 26.8% (95% CI 21.1–32.0%) in women age ≥ 40 years and did not differ between groups (p = 0.16) (Fig. 1C). Breast-cancer-specific mortality also did not differ between women aged < 40 years and those aged ≥ 40 years (5-year breast-cancer-specific mortality rates were 19.3% [95% CI 7.3–29.8%] vs. 25.2% [95% CI 19.6–30.4%], p = 0.35) (Fig. 1D).
Discussion
To better understand age-dependent differences in the treatment and outcomes for women with TNBC treated with modern NAC, we compared 104 young women, defined as younger than 40 years, to 411 women age ≥ 40 years. In women with TNBC breast cancer who received NAC, age was not an independent predictor of recurrence or survival outcomes. These findings are consistent with prior studies evaluating outcomes of young women with TNBC.6,12
The literature has often highlighted the more-aggressive nature of TNBC in younger women.13–15 The treatment paradigm of TNBC, particularly those with stage II and III TNBC, has shifted from upfront surgery to a preference for administering NAC. Despite presenting at equivalent clinical stages than their older counterparts, young age has been shown to be a determining factor in the achievement of a pCR following NAC.11,12,16,17 In a retrospective cohort study of 287 women with TNBC treated with NAC between 2007 and 2013, Villarreal-Garza et al. showed that women age ≤ 40 years were more likely to have a pCR, defined as ypT0/is and ypN0, than those age > 40 years (56.4% vs. 41.0%, p = 0.02). 17 Comparatively, younger women in our study were more likely to obtain an overall pCR following NAC.
Achieving a pCR is associated with improved long-term outcomes in breast cancer patients.7,11,18 Interestingly, despite the higher likelihood of achieving pCR in younger women, our study found no significant difference in LRR, DR, OS, or BCSS compared to those aged ≥ 40 years. This suggests that the improved response rates observed in younger patients do not necessarily translate into differential long-term outcomes when aggressive modern treatments are employed. Similarly, Villarreal-Garza et al. showed that age ≤ 40 years was not associated with a difference in disease-free survival (odds ratio [OR] 0.9, 95% CI 0.5–1.7, p = 0.768) or OS (OR 1.1, 95% CI 0.5–2.2, p = 0.876) among the triple-negative subset despite a higher reported rate of pCR. 17 The German Breast Group pooled eight NAC trials that included 1645 women with TNBC and also showed that pCR determined prognosis, but not age. Among women age < 40 years with TNBC, the pCR rate was 39.3%, but there was no difference in OS when compared to women age 40–49 years (HR: 1.03, 95% CI: 0.76–1.39, p = 0.855) or age ≥ 50 years (HR: 0.88, 95% CI: 0.66–1.18, p = 0.399) who had pCR rates of 37.0% and 25.2%, respectively. While age did not determine prognosis, achieving a pCR was associated with improved local recurrence-free survival, distant disease-free survival, disease-free survival, and OS. 12 Similarly, we showed that achieving a pCR translates to improved DR, OS, and BCSS, although this association did not remain significant for OS and BCSS after multiple comparison correction.
NAC offers patients the opportunity to reduce tumor stage, allowing them to be candidates for BCS. Despite higher rates of pCR in young women, they are less likely to opt for BCS. In our study, 75% of younger women in our study underwent a mastectomy, of whom 63 (60.6%) underwent bilateral mastectomy with CPM, even though the majority (55%) achieved a breast pCR. Verdial et al. also demonstrated this trend by reviewing 1383 women with breast cancer of any subtype and found that 72% (467/649) became eligible for BCS after being deemed ineligible at presentation. Young women age ≤ 40 years were less likely to choose BCS after becoming BCS-eligible following NAC (45% vs. 65% in those 41–60 years and 81% of those age ≥ 61 years, p < 0.001). 19 The tendency toward more-aggressive surgery for younger women is multifactorial. Young women may choose a mastectomy because of personal preference, presence of a genetic mutation, family history, desire to avoid radiation early in life, and, possibly, socioeconomic factors. This difference underscores the importance of personalized counseling and shared decision-making in the treatment planning for young women with TNBC. However, the occurrence of pCR is only known after surgery is complete and does not play a role in preoperative decision-making for most women. Although post-NAC MRI can be used as a surrogate for complete response,20,21 that may or may not factor into patient-provider decision-making regarding surgical choice. Patient-provider discussions can emphasize our findings that the type of surgery is not associated with OS or BCSS, but rather tumor biology.
Conversely, de-escalation of axillary surgery following NAC is more successful in younger women. In our study women aged < 40 years were more likely to avoid an ALND than their older counterparts. Several prospective trials have established the safety of axillary de-escalation for breast cancer patients who received NAC.22–26 We can appreciate the success of NAC by comparing rates of ALND to a previous study at our institution that demonstrated 51% of women age < 40 years with TNBC underwent an ALND regardless of the timing of chemotherapy. 5 Verdial et al. reviewed a larger group of women who received NAC who had any breast cancer subtype and reported a significantly higher rate of ALND avoidance in young women (55%) who initially presented with cN1 disease, compared to 38% and 37% in the age 41–60 years group and age ≥ 61 years group, respectively (p = 0.001). 19
We were also interested in understanding the characteristics and outcomes of women with TNBC who underwent NAC based on the type of surgery they underwent. Women who opted for bilateral mastectomy with CPM were more likely to be White, have a high-penetrance gene mutation, present with lower clinical stages, less likely to have high-risk features (i.e., extracapsular extension, LVI, nodal metastases), and more likely to achieve a pCR in comparison to those who underwent BCS or total mastectomy. This observation was also seen in previous studies that examined all breast cancer subtypes, 27 and emphasizes the lost opportunity in BCS, particularly in view of recent advances in chemotherapy regimens and improvements in pCR rates for TNBC.
Our study is limited by its retrospective nature. Additionally, the KEYNOTE-522 trial demonstrated benefit with the addition of immunotherapy to NAC, which was standardized following our study time period. 28 Future studies addressing the additional benefits of immunotherapy in young women will provide additional information regarding potential improvements in outcomes. To the best of our knowledge, however, our study is the largest to evaluate treatment and outcomes in young women with TNBC treated with NAC, although longer follow-up beyond our median follow-up of 2.8 years is needed. From a clinical perspective, our findings suggest that young women with TNBC can be counseled about their prognosis with reassurance that, with modern NAC regimens, their outcomes can be on par with those of older women. This can provide significant psychological support, as well as inform decision-making processes regarding treatment strategies.
Conclusions
The effectiveness of NAC in achieving pCR and the equivalence of breast cancer outcomes in young women with TNBC compared with older patients highlights opportunities to provide reassurance when counseling patients about the equivalent options of BCS and mastectomy. Continued research with ongoing advancements in neoadjuvant therapy will be crucial in understanding this challenging patient group.
Authors’ Contributions
All authors contributed to the study conception and design. Material preparation and data collection were performed by R.M.-U. and K.F. Data analysis was performed by R.M.-U., M.L.G., and V.S. The first draft of the article was written by R.M.-U. and all authors commented on previous versions of the article. All authors read and approved the final article.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The preparation of this study was supported in part by NIH/NCI Cancer Center Support Grant P30 CA008748 to Memorial Sloan Kettering Cancer Center.