
Abstract
CHAT is a virtual navigation program designed to improve adolescent and young adult cancer survivors (AYAs) health insurance literacy. CHAT is feasible, acceptable, and preliminarily efficacious. We used state-of-the-science methods to identify CHAT’s core functions (i.e., effectiveness-driving features). We conducted 7 semistructured interviews with CHAT developers (e.g., health services researchers, psychologists) and implementers (e.g., AYA patient navigator). We used interview data to develop a preliminary list of core functions. We then used a member-checking exercise with interview participants and other CHAT team members to develop consensus on a final list of core functions and underlying theory of change.
Keywords
Introduction
Adolescent and young adult (AYA) cancer survivors—those diagnosed between the ages of 15 and 39—experience unique challenges across the cancer continuum. Being diagnosed during a dynamic time of life has consequences for the transition of young survivors into adulthood, including delayed career trajectories, impact on fertility and family-building, and long-term financial stresses.1–3 Many AYA cancer survivors have minimal experience navigating the complicated United States health care system with a serious illness, resulting in consequences, such as taking on debt or filing for bankruptcy, and reduced access to care. 4
Health insurance in the United States is a complex and fragmented mix of private and public systems with variation in out-of-pocket costs for equivalent services/medications. 5 Navigating the complex system requires substantial knowledge of health insurance systems and coverage AYA cancer survivors often report lacking. 4 Health insurance literacy (HIL), or the understanding of health insurance and the application of health insurance concepts, is critical to navigating the U.S. health care system, minimizing costs to patients, and lessening financial-related stress.
To bridge this gap and create a program targeted to AYA survivors, Kirchhoff and colleagues developed the CHAT (let’s CHAT about health insurance) intervention from the Health Insurance Navigation Tools (HINT) program originally designed for childhood cancer survivors by Park and colleagues.6–8 HINT and CHAT are four-session programs designed to provide psychoeducation with a focus on improving health insurance and cost-related literacy while overcoming related barriers faced by long-term survivors of childhood cancer (HINT) or AYA cancer patients (CHAT). CHAT’s feasibility was tested in a two-arm pilot randomized trial with 86 newly diagnosed AYA survivors from 3 hospitals in Utah. 9 The trial results supported the feasibility and acceptability of CHAT and demonstrated preliminary efficacy at improving the HIL of AYA survivors. 10 CHAT participants demonstrated a greater increase in HIL than usual care participants (5.4 vs. 2.4, respectively; p = 0.04), as well as greater increases related to confidence and knowledge of health insurance terminology (2.9 vs. 0.7, respectively, p = 0.01). 10
Identifying CHAT’S core functions is a critical step to clarify which features are collectively necessary and sufficient for improving insurance literacy among AYAs. Future adaptations using the core functions could extend CHAT’s benefits to new contexts or a broader range of populations, enhancing accessibility. Additionally, identifying core functions allows for CHAT to be combined with other interventions such as financial navigation. Here we report on the core functions of the CHAT intervention using state-of-the-science methods.
Materials and Methods
Interventions are comprised of intervention and implementation core functions. Implementation core functions are features required for an intervention’s proficient and consistent use in practice. 11 Intervention core functions relate to features of the intervention that drive its effectiveness in achieving desired outcomes. Once identified, core functions may be fulfilled using forms, the activities or strategies that are feasible, acceptable, and appropriate in new populations and contexts. 12 Identifying core functions allows adaptations to meet the needs of new contexts or populations without compromising the intervention’s originally demonstrated levels of effectiveness. 13 Our identification of CHAT’s core functions was guided by a refined version of the core functions approach developed by Alexis Kirk.13–15 This study was approved by the Wake Forest University School of Medicine Institutional Review Board (IRB00107846, approved 1/23/2024).
CHAT summary document and interview guide
We used a combination of published and internal documents provided by CHAT team members to develop a document describing the CHAT intervention.13–15
An interdisciplinary team of researchers with expertise in AYA cancer, implementation science, intervention development, and core functions identification methods developed the interview guide using guidance from Kirk et al. and the CHAT summary document.13–15 The interview guide can be found in the Supplementary Appendix.
Core functions interviews
An exhaustive group of CHAT developers and implementers, including the CHAT principal investigator and coinvestigators, an AYA patient navigator, two research assistants, and two project managers, were recruited by email to provide their feedback on the summary document in structured interviews. Interviews sought to identify gaps in the summary document, features of CHAT, and the context in which it was implemented that influenced its effectiveness. Interviews were recorded and transcribed verbatim using ATLAS.ti 24.
AYA patient feedback
To supplement the primary data collection and account for AYAs’ perspectives, we utilized previously collected qualitative data from CHAT study exit interviews on the content and delivery of the CHAT intervention. The secondary qualitative dataset included 12 AYAs who participated in CHAT and in an exit interview. AYA patient feedback on CHAT content feedback was combined into a single document for analysis. More information about the CHAT intervention and exit interview sample characteristics is published in-depth elsewhere. 10
Analysis
Two coders coded interview and patient feedback data using a combination of a priori codes for identifying core functions (e.g., essential elements, forms) and inductive codes specific to the intervention (i.e., specific forms used to carry out core functions) and participant population (e.g., caregivers, tailoring to age). We co-coded one interview to refine the codebook, establish inter-coder reliability, and develop consensus through coding discrepancy resolution. 16 Once consensus was reached, the coders independently coded the remaining interviews. They then employed grounded theory methods used in previous core functions research to identify themes by comparing both within and across codes. 17
From this, we derived a preliminary set of core functions and original forms. The coders independently analyzed codes related to CHAT’s core functions and original forms and compared results, reconciling discrepancies in findings. The larger study team provided feedback on the preliminary list of core functions and original forms. We then conducted member checking to ascertain the accuracy of the derived core functions and forms during one virtual meeting and via email, receiving written and verbal feedback. We integrated feedback and shared revised versions until no new feedback was received and consensus was reached, which required three iterations.
To enhance our confidence in interpreting the results, SAB, an implementation methodologist and theoretician, conducted a web search of extant theories that included key constructs identified during analysis (e.g., autonomy, connectedness to information).
Results
Core function interview participants (n = 7) represented participation in all stages of the CHAT study, from conceptualization to development to intervention delivery. CHAT participant feedback was integrated into the core function interview analysis. Member checking included 11 CHAT team members, including all of those who participated in the interviews, as well as individuals on the larger study team (e.g., study coordinators).
We identified seven core functions, including four implementation and three intervention core functions; member-checking exercise participants identified 3–12 forms per core function (Tables 1–2). No discordance in core functions was observed between the CHAT study team and study participants. Collectively, the effectiveness underlying CHAT’s core functions can be explained by Self-Determination Theory, as the interventions promoted participants to enhance their autonomy, competence, and relatedness to the information presented. 18
CHAT Implementation Core Functions
CHAT Intervention Core Functions
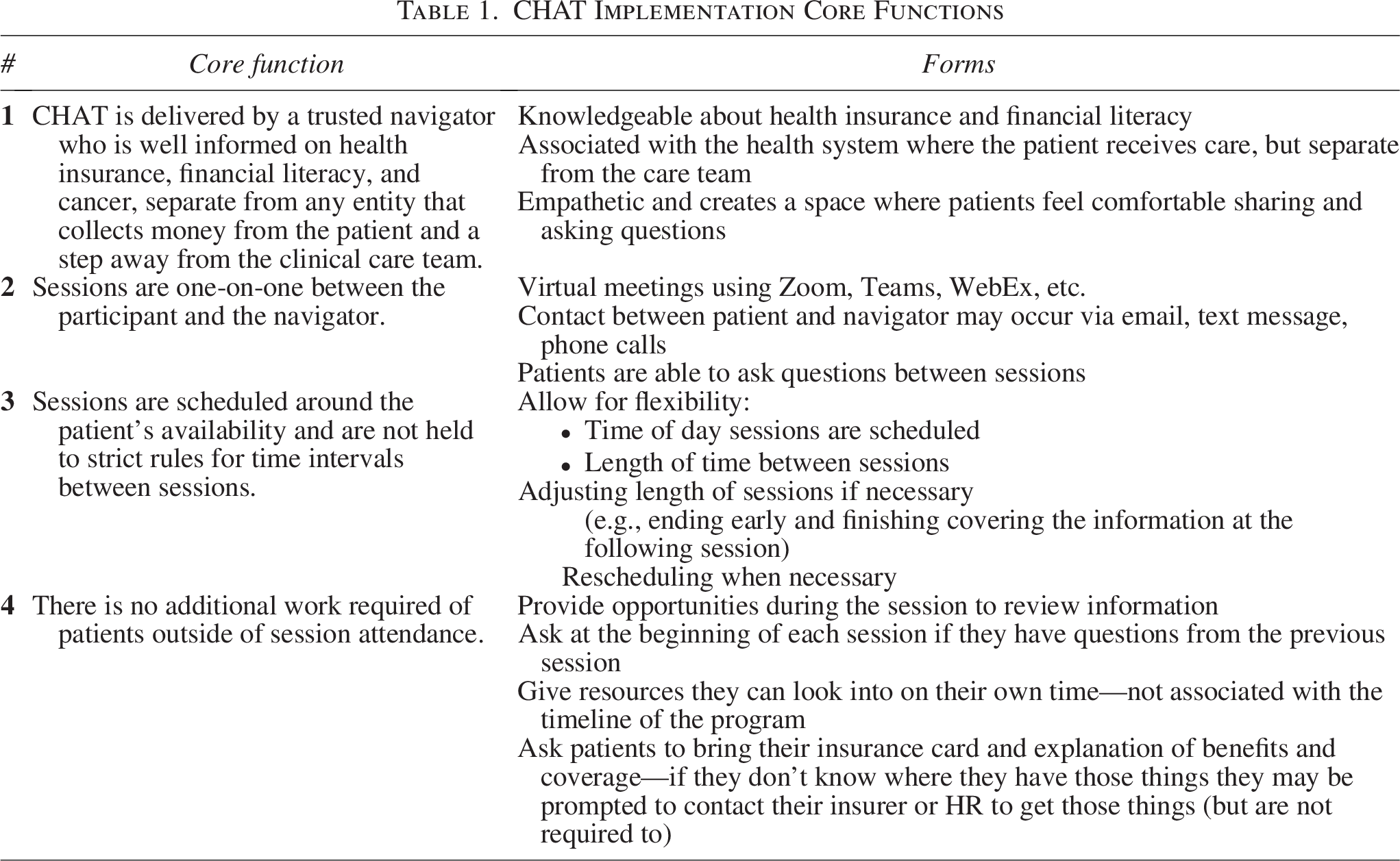
Implementation core functions (Table 1)
CHAT was designed for acceptability and feasibility from the perspective of implementers and patients. This was achieved through a skilled navigator in an accessible format.
CHAT is delivered by a trusted navigator who is well-informed on health insurance, financial literacy, and cancer, separate from any entity that collects money from the patient and a step away from the clinical care team. Sessions are one-on-one between the participant and the navigator. Sessions are scheduled around the patient’s availability and are not held to strict rules for time intervals between sessions. There is no additional work required of patients outside of session attendance.
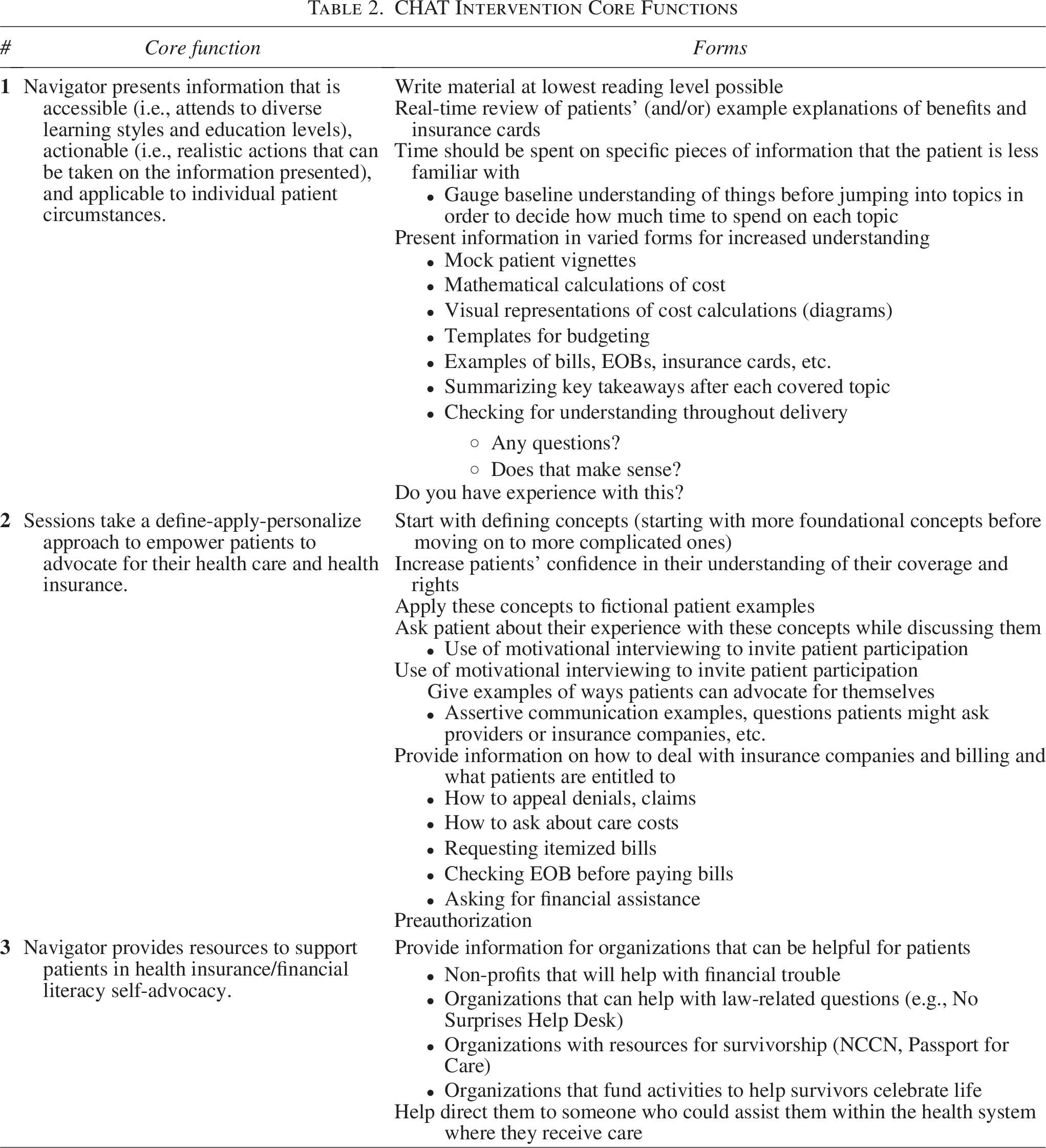
Intervention core functions (Table 2)
CHAT fostered autonomy, competence, and relatedness to the information presented. This was achieved by providing education and guidance to build participants’ self-efficacy in managing their health insurance, while also encouraging self-advocacy to address insurance- and financial-related barriers to care.
19
Navigator presents information that is accessible (i.e., attends to diverse learning styles and education levels), actionable (i.e., realistic actions that can be taken on the information presented), and applicable to individual patient circumstances. Sessions take a define-apply-personalize approach to empower patients to advocate for their health care and health insurance. Navigator provides resources to support patients in health insurance/financial literacy self-advocacy.
Discussion
Identifying the core functions of evidence-based interventions for AYAs with cancer is crucial for adapting these approaches to other populations and contexts. Utilizing state-of-the-science methods identification of core functions has the potential to increase reach and accessibility of financial hardship interventions. We identified seven core functions of CHAT’s preliminary efficacy that included ensuring the material was applicable and built participant self-advocacy. Our findings also highlight key implementation core functions related to the high levels of feasibility and acceptability of CHAT, including sessions being scheduled around patients’ availability and delivered one-on-one by a trusted navigator with adequate health insurance knowledge who was not directly involved with their care or collecting payments from the patient.
The accessibility and applicability of the information presented, the focus on building self-advocacy skills, and the personalized yet self-contained nature of the sessions were central in the intervention’s design. These concepts underlie Self-Determination Theory, with autonomy, competence, and relatedness ensuring the participants feel confident in their ability to put knowledge and skills learned during the program to use. 19 Identifying a theory of change clarifies how core functions, in combination, produce implementation and intervention outcomes. This helps explain underlying assumptions that led to the outcomes and the driver(s) of success. Identification of a theory of change also provides a framework for adaptation of the intervention to new contexts.
Recent literature has begun to focus on HIL as an important modifiable component of cancer-related financial hardship.6,20 There is an association between low HIL and financial hardship outcomes such as lower COmprehensive Score for financial Toxicity scores, borrowing money/going into debt, inability to pay for housing or food, and skipping a procedure due to cost or coverage concerns.4,21,22 This highlights the importance of interventions aimed at enhancing health insurance knowledge and empowering patients to advocate for themselves when dealing with health care and insurance agencies. CHAT provides patients with these tools; therefore, cancer centers and other treatment facilities can implement CHAT as a potential strategy to improve patient financial hardship.
Identification of the core functions facilitates future adaptations of CHAT and facilitates implementation by providing a list of elements that must be preserved, and that may be adapted to enhance implementation and/or effectiveness in a new context or population. The next step after identifying the core functions is to use evidence-based adaptation methods, such as Making Optimal Decisions for Intervention Flexibility during Implementation, to adapt the program to new contexts. 23 Using the identified core functions, currently, CHAT is being blended with a financial navigation intervention, LIFT (Lessening the Impact of Financial Toxicity), for which we previously identified the core functions. 15 The purpose of this process is to develop a comprehensive program that can both build self-advocacy by educating AYAs about health insurance while providing direct assistance through financial navigation, accounting for the multilevel factors contributing to financial hardship.
The findings of this study should be interpreted in the context of certain strengths and limitations. Importantly, we assessed CHAT core functions retrospectively; ideally, intervention developers would have stated an a priori theory of change underlying intervention forms and intended outcomes. While our theory-based approach posits specific mechanisms underlying the relationship between core functions and these outcomes, we do not yet have experimental data on the causal relationship between the core functions and key implementation and intervention outcomes. Additionally, evidence from a radomized controlled trial (RCT) of CHAT’s causal influence on outcomes is not yet available. If the trial results from a RCT of CHAT do not demonstrate causal influence on outcomes, core functions may not produce the intervention’s intended outcomes.
Conclusions
Through qualitative interviews with the CHAT study team and patient feedback, seven core functions were identified. The findings of this study utilize emerging intervention adaptation methods to describe tangible starting points for future adaptation of CHAT. Core functions serve as a scaffold for future adaptations to new contexts, including community oncology clinics. Identifying CHAT’s core functions allows for rapid adaptation in the ever-changing U.S. health policy landscape, expanding the reach of much-needed health insurance education for AYA survivors.
Authors’ Contributions
Conceptualization: J.M.S., S.A.B. Methodology: C.R.W., A.R.W., S.A.B. Validation: C.R.W., A.R.W., A.C.K., G.K.P., K.Mv.T.B., P.L.V.L., S.B.W., J.M.S., S.A.B., A.C. Formal analysis: C.R.W., A.R.W. Investigation: C.R.W. Data curation: C.R.W., P.L.V.L. Writing—original draft: C.R.W., A.R.W. Writing—review and editing: C.R.W., A.R.W., A.C.K., G.K.P., E.R.P., K.Mv.T.B., P.L.V.L., S.C.B., E.H., S.B.W., J.M.S., S.A.B., A.C. Supervision: A.C.K., G.K.P., E.R.P., J.M.S., S.A.B. Project administration: C.R.W., S.C.B. Funding acquisition: A.C.K., S.B.W., J.M.S., S.A.B.
Footnotes
Acknowledgment
The authors would like to thank the CHAT study team members who participated in interviews and provided feedback on the CHAT core functions.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Funding Information: Research reported in this publication was supported by the National Cancer Institute of the National Institutes of Health under award number R01CA282653 (PIs: John Salsman & Sarah A. Birken). Austin R. Waters was supported by the National Cancer Institute under award number T32CA092203. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.